
The Financial Burden of Surgery for Congenital Malformations—The Austrian Perspective

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
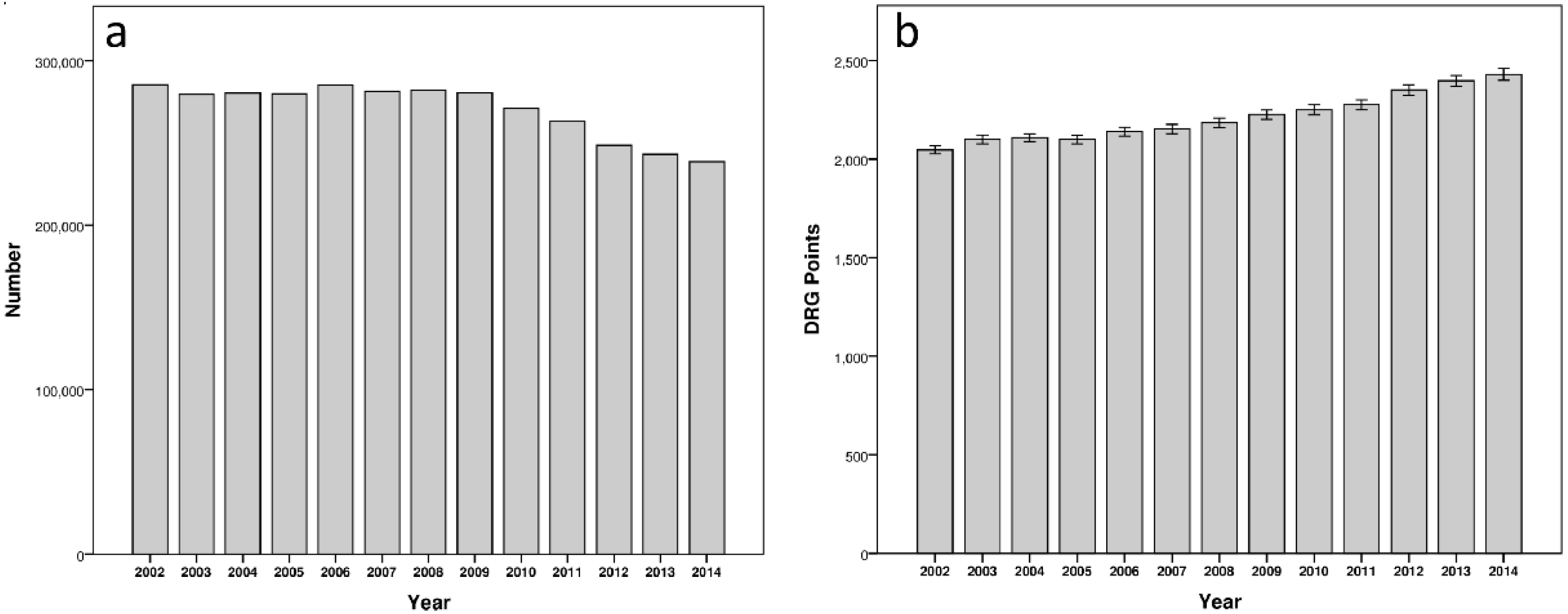
3.1. Total Hospitalizations
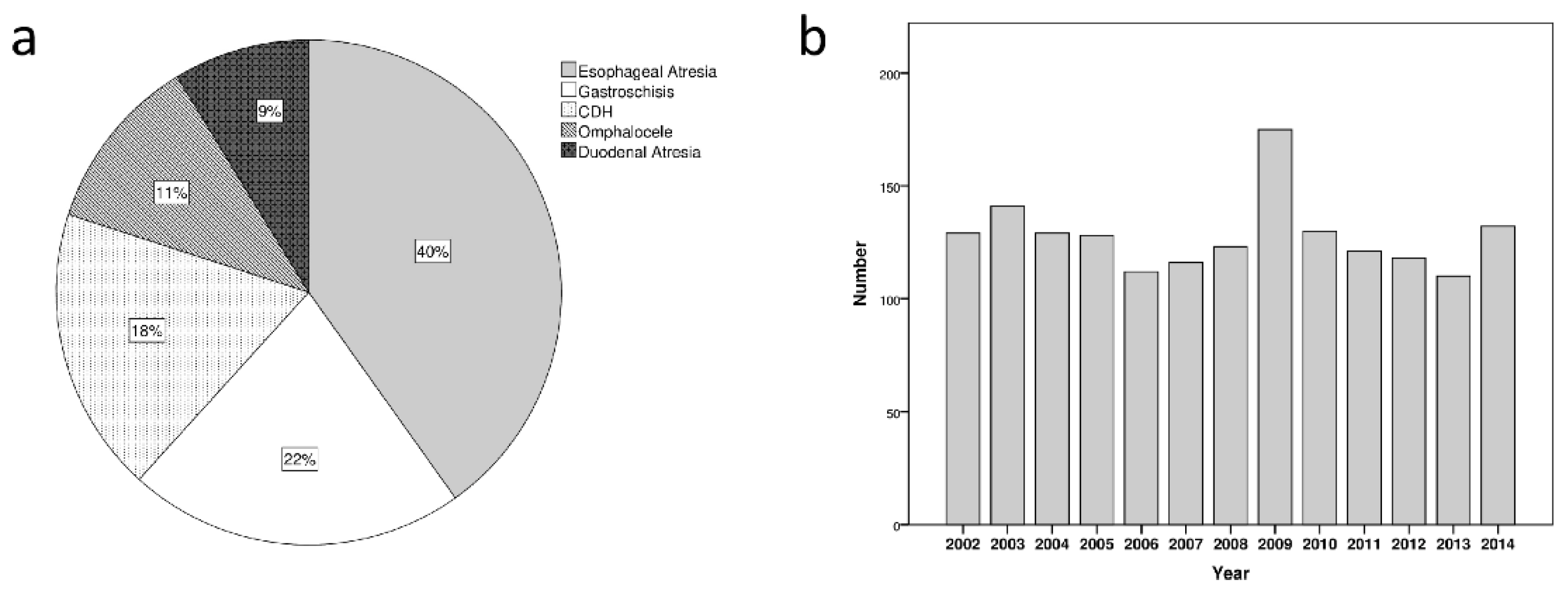
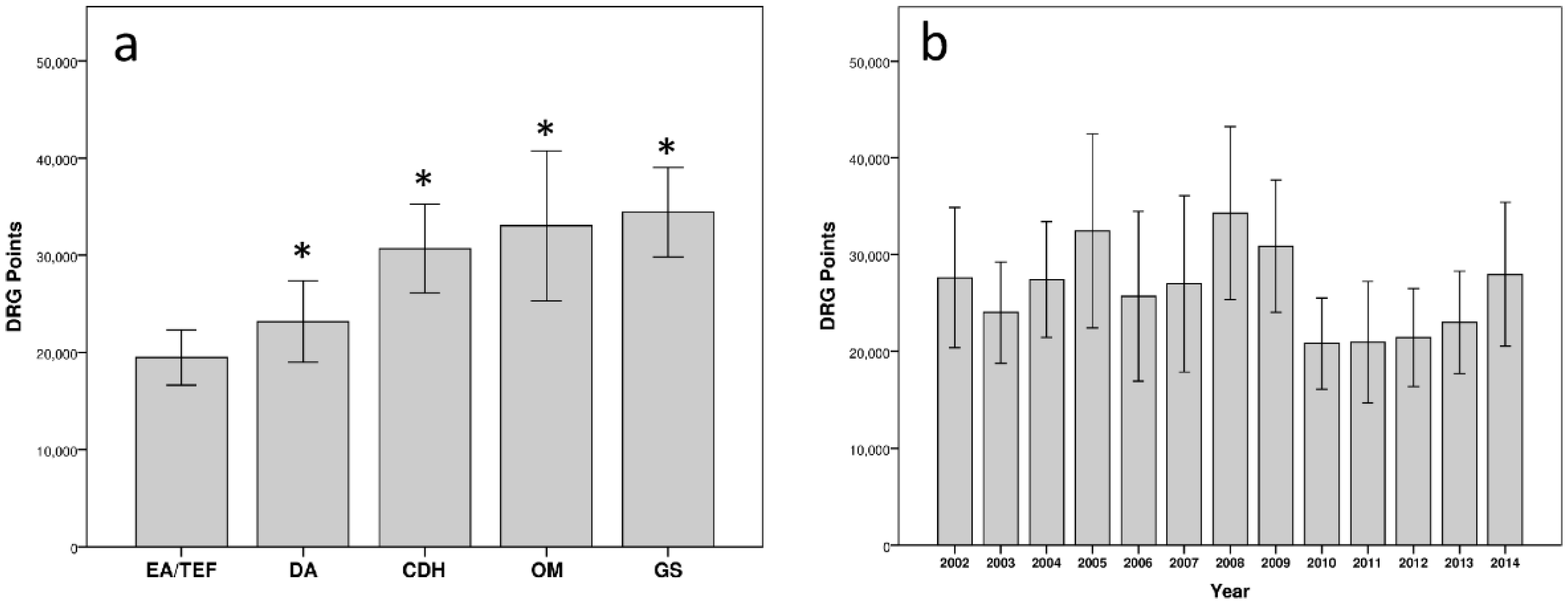
3.2. Congenital Malformations and Comparison to Other Hospitalizations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Apfeld, J.C.; Kastenberg, Z.J.; Gibbons, A.T.; Phibbs, C.S.; Lee, H.C.; Sylvester, K.G. The disproportionate cost of operation and congenital anomalies in infancy. Surgery 2019, 165, 1234–1242. [Google Scholar] [CrossRef]
- Arth, A.C.; Tinker, S.C.; Simeone, R.M.; Ailes, E.C.; Cragan, J.D.; Grosse, S.D. Inpatient Hospitalization Costs Associated with Birth Defects Among Persons of All Ages—United States, 2013. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Higashi, H.; Barendregt, J.J.; Kassebaum, N.J.; Weiser, T.G.; Bickler, S.W.; Vos, T. The burden of selected congenital anomalies amenable to surgery in low and middle-income regions: Cleft lip and palate, congenital heart anomalies and neural tube defects. Arch. Dis. Child. 2015, 100, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Richter, T.; Nestler-Parr, S.; Babela, R.; Khan, Z.M.; Tesoro, T.; Molsen, E.; Hughes, D.A.; International Society for Pharmacoeconomic; Outcomes Research Rare Disease Special Interest Group. Rare Disease Terminology and Definitions—A Systematic Global Review: Report of the ISPOR Rare Disease Special Interest Group. Value Health 2015, 18, 906–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannizzo, S.; Lorenzoni, V.; Palla, I.; Pirri, S.; Trieste, L.; Triulzi, I.; Turchetti, G. Rare diseases under different levels of economic analysis: Current activities, challenges and perspectives. RMD Open 2018, 4, e000794. [Google Scholar] [CrossRef] [PubMed]
- Arnold, H.E.; Baxter, K.J.; Short, H.L.; Travers, C.; Bhatia, A.; Durham, M.M.; Raval, M.V. Short-term and family-reported long-term outcomes of simple versus complicated gastroschisis. J. Surg. Res. 2018, 224, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.W.Y.; Yan, B.P.; Fong, T.M.C.; Fung, A.K.P.; Cheng, F.W.T. Long-term health-related burden of adult congenital heart diseases in Hong Kong. J. Med. Econ. 2019, 22, 814–817. [Google Scholar] [CrossRef]
- Apfeld, J.C.; Kastenberg, Z.J.; Sylvester, K.G.; Lee, H.C. The Effect of Level of Care on Gastroschisis Outcomes. J. Pediatr. 2017, 190, 79–84.e1. [Google Scholar] [CrossRef]
- Johnson, J.T.; Wilkes, J.F.; Menon, S.C.; Tani, L.Y.; Weng, H.Y.; Marino, B.S.; Pinto, N.M. Admission to dedicated pediatric cardiac intensive care units is associated with decreased resource use in neonatal cardiac surgery. J. Thorac. Cardiovasc. Surg. 2018, 155, 2606–2614.e5. [Google Scholar] [CrossRef]
- Ronnekleiv-Kelly, S.M.; Soares, K.C.; Ejaz, A.; Pawlik, T.M. Management of choledochal cysts. Curr. Opin. Gastroenterol. 2016, 32, 225–231. [Google Scholar] [CrossRef]
- Somme, S.; Shahi, N.; McLeod, L.; Torok, M.; McManus, B.; Ziegler, M.M. Neonatal surgery in low- vs. high-volume institutions: A KID inpatient database outcomes and cost study after repair of congenital diaphragmatic hernia, esophageal atresia, and gastroschisis. Pediatr. Surg. Int. 2019, 35, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Hagenbichler, E. The Austrian DRG System, 1st ed.; Federal Ministry of Health: Wien, Austria, 2010.
- Ferreira, C.R. The burden of rare diseases. Am. J. Med. Genet. A 2019, 179, 885–892. [Google Scholar] [CrossRef]
- Austin, C.P.; Cutillo, C.M.; Lau, L.P.L.; Jonker, A.H.; Rath, A.; Julkowska, D.; Thomson, D.; Terry, S.F.; de Montleau, B.; Ardigo, D.; et al. Future of Rare Diseases Research 2017–2027: An IRDiRC Perspective. Clin. Transl. Sci. 2018, 11, 21–27. [Google Scholar] [CrossRef]
- Dingemann, C.; Eaton, S.; Aksnes, G.; Bagolan, P.; Cross, K.M.; De Coppi, P.; Fruithof, J.; Gamba, P.; Husby, S.; Koivusalo, A.; et al. ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: Diagnostics, Preoperative, Operative, and Postoperative Management. Eur. J. Pediatr. Surg. 2020, 30, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Groft, S.C.; Posada de la Paz, M. Preparing for the Future of Rare Diseases. Adv. Exp. Med. Biol. 2017, 1031, 641–648. [Google Scholar] [CrossRef]
- Mazzucato, M.; Visona Dalla Pozza, L.; Manea, S.; Minichiello, C.; Facchin, P. A population-based registry as a source of health indicators for rare diseases: The ten-year experience of the Veneto Region’s rare diseases registry. Orphanet J. Rare Dis. 2014, 9, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradnock, T.J.; Marven, S.; Owen, A.; Johnson, P.; Kurinczuk, J.J.; Spark, P.; Draper, E.S.; Knight, M.; Baps, C. Gastroschisis: One year outcomes from national cohort study. BMJ 2011, 343, d6749. [Google Scholar] [CrossRef] [Green Version]
- Shetty, S.; Kennea, N.; Desai, P.; Giuliani, S.; Richards, J. Length of stay and cost analysis of neonates undergoing surgery at a tertiary neonatal unit in England. Ann. R. Coll. Surg. Engl. 2016, 98, 56–60. [Google Scholar] [CrossRef] [Green Version]
- Jsselstijn, H.; Gischler, S.J.; Wijnen, R.M.H.; Tibboel, D. Assessment and significance of long-term outcomes in pediatric surgery. Semin. Pediatr. Surg. 2017, 26, 281–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmedding, A.; Wittekind, B.; Salzmann-Manrique, E.; Schloesser, R.; Rolle, U. Decentralized surgery of abdominal wall defects in Germany. Pediatr. Surg. Int. 2020, 36, 569–578. [Google Scholar] [CrossRef] [Green Version]
- Dubrovsky, G.; Sacks, G.D.; Friedlander, S.; Lee, S. Understanding the relationship between hospital volume and patient outcomes for infants with gastroschisis. J. Pediatr. Surg. 2017, 52, 1977–1980. [Google Scholar] [CrossRef] [PubMed]
- Youssef, F.; Cheong, L.H.; Emil, S.; The Canadian Pediatric Surgery Network. Gastroschisis outcomes in North America: A comparison of Canada and the United States. J. Pediatr. Surg. 2016, 51, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Aite, L.; Zaccara, A.; Cuttini, M.; Mirante, N.; Nahom, A.; Bagolan, P. Lack of institutional pathways for referral: Results of a survey among pediatric surgeons on prenatal consultation for congenital anomalies. Prenat. Diagn. 2013, 33, 904–907. [Google Scholar] [CrossRef] [PubMed]
- Pardy, C.; D’Antonio, F.; Khalil, A.; Giuliani, S. Prenatal detection of esophageal atresia: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2019, 98, 689–699. [Google Scholar] [CrossRef] [Green Version]
- Monaco, L.; Crimi, M.; Wang, C.M. The challenge for a European network of biobanks for rare diseases taken up by RD-Connect. Pathobiology 2014, 81, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Moliner, A.M.; Waligora, J. The European Union Policy in the Field of Rare Diseases. Adv. Exp. Med. Biol. 2017, 1031, 561–587. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Year | Other Diagnoses | EA/TEF | DA | CDH | OM | GS | Total Malformations | Total Admissions |
|---|---|---|---|---|---|---|---|---|
| 2002 | 285,326 | 48 | 12 | 17 | 21 | 31 | 129 | 285,455 |
| 2003 | 279,458 | 51 | 22 | 24 | 11 | 33 | 141 | 279,599 |
| 2004 | 280,181 | 48 | 9 | 27 | 16 | 29 | 129 | 280,310 |
| 2005 | 279,759 | 49 | 9 | 23 | 20 | 27 | 128 | 279,887 |
| 2006 | 285,162 | 56 | 10 | 18 | 6 | 22 | 112 | 285,274 |
| 2007 | 281,191 | 54 | 9 | 17 | 14 | 22 | 116 | 281,307 |
| 2008 | 281,938 | 51 | 4 | 29 | 13 | 26 | 123 | 282,061 |
| 2009 | 280,322 | 63 | 19 | 41 | 21 | 31 | 175 | 280,497 |
| 2010 | 270,862 | 59 | 10 | 21 | 6 | 34 | 130 | 270,992 |
| 2011 | 263,109 | 53 | 6 | 26 | 10 | 26 | 121 | 263,230 |
| 2012 | 248,401 | 51 | 12 | 16 | 14 | 25 | 118 | 248,519 |
| 2013 | 242,951 | 45 | 10 | 21 | 18 | 16 | 110 | 243,061 |
| 2014 | 238,301 | 40 | 13 | 24 | 18 | 37 | 132 | 238,433 |
| 3,516,961 | 668 | 145 | 304 | 188 | 359 | 1664 | 3,518,625 |
| DRG Points [Mean ± SD] | Factor | |
|---|---|---|
| Other Hospitalizations | 2205 ± 6245 | 1 |
| EA/TEF | 19,454 ± 36,761 | 8.82 |
| DA | 23,161 ± 25,395 | 10.50 |
| CDH | 30,668 ± 39,915 | 13.91 |
| OM | 33,015 ± 52,983 | 14.97 |
| GS | 34,426 ± 43,663 | 15.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasparella, P.; Singer, G.; Kienesberger, B.; Arneitz, C.; Fülöp, G.; Castellani, C.; Till, H.; Schalamon, J. The Financial Burden of Surgery for Congenital Malformations—The Austrian Perspective. Int. J. Environ. Res. Public Health 2021, 18, 11166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111166
Gasparella P, Singer G, Kienesberger B, Arneitz C, Fülöp G, Castellani C, Till H, Schalamon J. The Financial Burden of Surgery for Congenital Malformations—The Austrian Perspective. International Journal of Environmental Research and Public Health. 2021; 18(21):11166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111166
Chicago/Turabian StyleGasparella, Paolo, Georg Singer, Bernhard Kienesberger, Christoph Arneitz, Gerhard Fülöp, Christoph Castellani, Holger Till, and Johannes Schalamon. 2021. "The Financial Burden of Surgery for Congenital Malformations—The Austrian Perspective" International Journal of Environmental Research and Public Health 18, no. 21: 11166. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111166