
Economic Evaluation of Long-Term Survivorship Care for Cancer Patients in OECD Countries: A Systematic Review for Decision-Makers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Overview of Included Studies
3.2. Studies of Long-Term Survivorship Care by Cancer Type
3.2.1. Colorectal Cancer
3.2.2. Breast Cancer
3.2.3. Skin Cancer
3.2.4. Cervical Cancer
3.2.5. Head and Neck Cancer
3.2.6. Hodgkin’s Disease
3.2.7. Testicular Cancer
3.2.8. Others
3.3. Quality Assessment
3.4. Usefulness of Economic Evaluation Studies to Decision-Makers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Section and Topic | Item # | Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstract checklist (Table A2). | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | 1 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | 1 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | 2 |
| Information sources | 6 | Specify all databases, registers, websites, organizations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | 2 |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | 2, Table A3, Appendix B |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently and, if applicable, details of automation tools used in the process. | 2, Appendix B |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators and, if applicable, details of automation tools used in the process. | 2, Appendix B |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | 2, Appendix B and Appendix C |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | 2, Appendix B and Appendix C | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | 3, Table A6 and Table A7, Appendix D |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | NA |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis. | 2–3 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | 2–3, Table A5, Appendix C | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | 2–3, Table A5, Appendix C | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity and software package(s) used. | 2–3 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results. | NA | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | NA | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | 3, Table A6 and Table A7, Appendix D |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | NA |
| RESULTS | |||
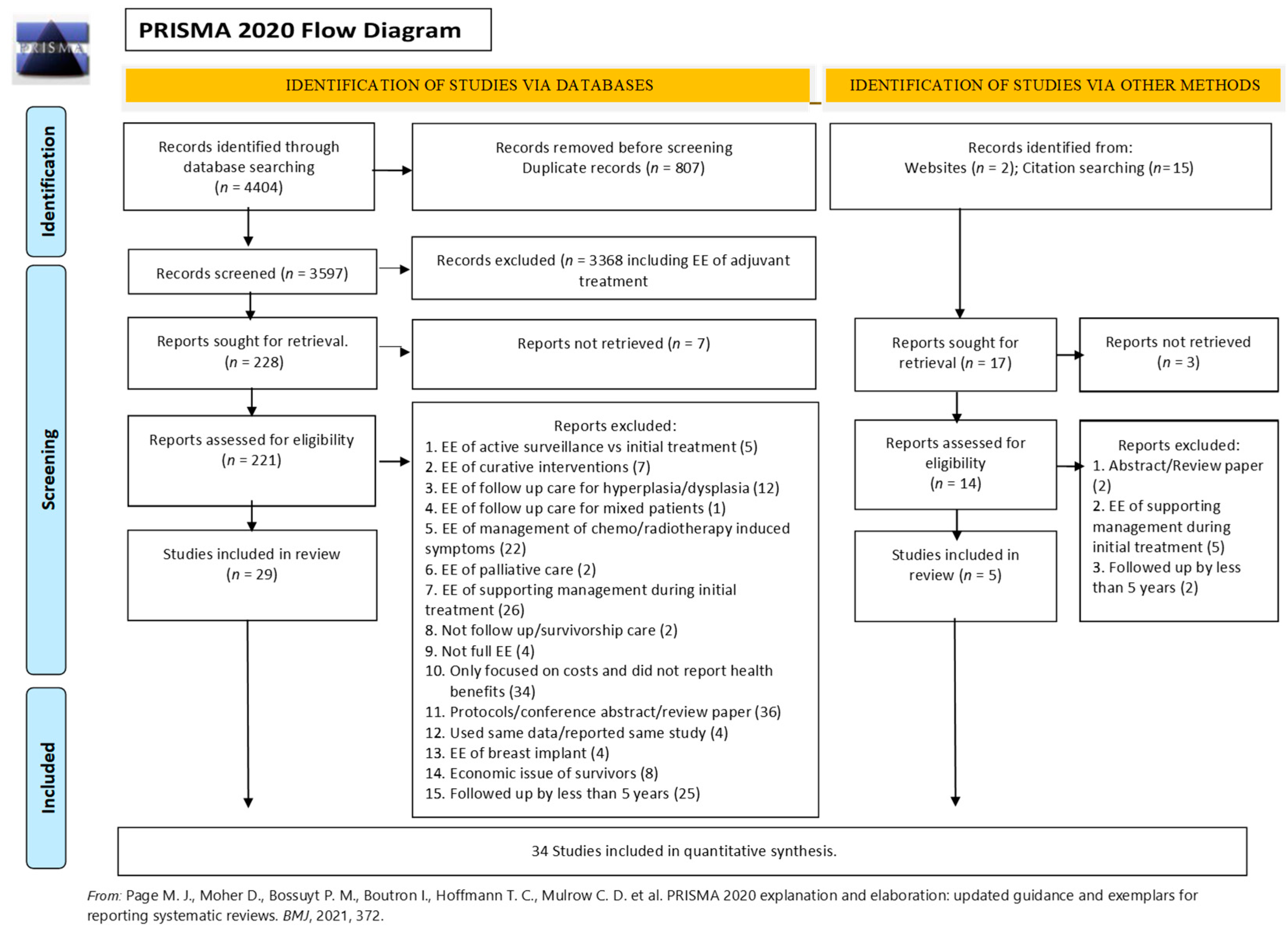
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram (see Figure 1). | 3–11, Table A5, Appendix C and Table A7, Appendix D |
| 16b | Cite studies that met many but not all inclusion criteria (‘near-misses’) and explain why they were excluded. | Table A4, Appendix B | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | 3–11, Appendix C and Appendix D |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Appendix D |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | 3–11, Table A5, Appendix C |
| Results of syntheses | 20a | For each synthesis, briefly summarize the characteristics and risk of bias among contributing studies. | 8–11 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | 8–11 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Appendix C and Appendix D | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | 9–11, Table A5, Appendix C | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | Table A7, Appendix D |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Table A7, Appendix D |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | 11–12 |
| 23b | Discuss any limitations of the evidence included in the review. | 11–12 | |
| 23c | Discuss any limitations of the review processes used. | 11–12 | |
| 23d | Discuss implications of the results for practice, policy and future research. | 11–12 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | 2 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | 2 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | 2 | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | NA |
| Competing interests | 26 | Declare any competing interests of review authors. | 12 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Appendix A, Appendix B, Appendix C and Appendix D |
| Section and Topic | Item # | Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | 1 |
| BACKGROUND | |||
| Objectives | 2 | Provide an explicit statement of the main objective(s) or question(s) the review addresses. | 1 |
| METHODS | |||
| Eligibility criteria | 3 | Specify the inclusion and exclusion criteria for the review. | 1 |
| Information sources | 4 | Specify the information sources (e.g., databases, registers) used to identify studies and the date when each was last searched. | 1 |
| Risk of bias | 5 | Specify the methods used to assess risk of bias in the included studies. | 1 |
| Synthesis of results | 6 | Specify the methods used to present and synthesize results. | 1 |
| RESULTS | |||
| Included studies | 7 | Give the total number of included studies and participants and summarize relevant characteristics of studies. | 1 |
| Synthesis of results | 8 | Present results for main outcomes, preferably indicating the number of included studies and participants for each. If meta-analysis was performed, report the summary estimate and confidence/credible interval. If comparing groups, indicate the direction of the effect (i.e., which group is favored). | 1 |
| DISCUSSION | |||
| Limitations of evidence | 9 | Provide a brief summary of the limitations of the evidence included in the review (e.g., study risk of bias, inconsistency and imprecision). | 1 |
| Interpretation | 10 | Provide a general interpretation of the results and important implications. | 1 |
| OTHER | |||
| Funding | 11 | Specify the primary source of funding for the review. | NA |
| Registration | 12 | Provide the register name and registration number. | 1 |
Appendix B
| Search Terms | Numbers | |
|---|---|---|
| ||
| 1. | “economic evaluation*” or “economic analys*” or “cost*” or expenditure or “out of pocket” or “cost of illness*” or “health care cost*” or “direct service cost*” or “drug cost*” or “hospital cost*” | 883,278 |
| 2 | “Costs and Cost Analysis” [MeSH Terms] OR “Economics” [MeSH Terms] OR “Economics” [MeSH Subheading] OR “Cost of Illness” [MeSH Terms] OR “Cost Sharing” [MeSH Terms] OR “Cost Savings” [MeSH Terms] OR “technology, high cost” [MeSH Terms] OR “Cost Control” [MeSH Terms] OR “Cost-Benefit Analysis” [MeSH Terms] OR “Cost Allocation” [MeSH Terms] OR “Health Care Costs” [MeSH Terms] OR “Direct Service Costs” [MeSH Terms] OR “Hospital Costs” [MeSH Terms] OR “Employer Health Costs” [MeSH Terms] OR “Drug Costs” [MeSH Terms] OR “Health Expenditures” [MeSH Terms] | 742,199 |
| 3 | 1 OR 2 | 1,328,609 |
| 4 | “follow-up” or “secondary prevent*” or “after treatment” or “after chemo*” or “after radiation” or “after care” or “after cur*” or “post treatment” or “post chemo*” or “post radiotherapy” or “survivorship care” or “long-term strateg*” | 1,568,415 |
| 5 | “Neoplasms” [MeSH Terms] | 3,378,598 |
| 6 | (cancer* or carcinoma* or histiocytosis or leukemia or lymphoma* or medulloblastoma* or neoplasm* or nephroblastoma* or neuroblastoma* or oncolog* or osteosarcoma* or retinoblastoma* or sarcoma* or tumor* or neoplasm*).ti,ab. | 3,448,803 |
| 7 | 5 OR 6 | 4,370,095 |
| 8 | (Australia or Austria or Belgium or Canada or Chile or Colombia or Czech Republic or Denmark or Estonia or Finland or France or Germany or Greece or Hungary or Iceland or Ireland or Israel or Italy or Japan or Korea or Latvia or Lithuania or Luxembourg or Mexico or Netherlands or “New Zealand” or Norway or Poland or Portugal or Slovak Republic or Slovenia or Spain or Sweden or Turkey or “United Kingdom” or England or United States).ti,ab. | 1,153,236 |
| 9 | 3 and 4 and 7 and 8 | 1499 |
| 10 | Filters: 2000–2020 and English | 1277 |
| ||
| (“economic evaluation*” or “economic analys*” or “cost* utility” or “cost analysis” or “cost effective*” or “cost benefit” or “cost minimization” or “cost minimization” or expenditure or “out of pocket” or “cost of illness*” or “health care cost*” or “direct service cost*” or “drug cost*” or “hospital cost*”) AND (“Follow-up” or “secondary prevent*” or “after treatment” or “after chemo*” or “after radiation” or “after care” or “after cur*” or “post treatment” or “post chemo*” or “post radiotherapy” or “survivorship care” or “long-term strateg*” or “short-term strateg*”) AND (Cancer* or carcinoma* or histiocytosis or leukemia or lymphoma* or medulloblastoma* or neoplasm* or nephroblastoma* or neuroblastoma* or oncolog* or osteosarcoma* or retinoblastoma* or sarcoma* or tumor* or neoplasm*) AND (Australia or Austria or Belgium or Canada or Chile or Colombia or Czech Republic or Denmark or Estonia or Finland or France or Germany or Greece or Hungary or Iceland or Ireland or Israel or Italy or Japan or Korea or Latvia or Lithuania or Luxembourg or Mexico or Netherlands or “New Zealand” or Norway or Poland or Portugal or Slovak Republic or Slovenia or Spain or Sweden or Turkey or “United Kingdom” or England or United States)Filters: 2000–2020 and English | 2107 | |
| ||
| (“economic evaluation*” or “economic analys*” or “cost* utility” or “cost analysis” or “cost effective*” or “cost benefit” or “cost minimization” or “cost minimization” or expenditure or “out of pocket” or “cost of illness*” or “health care cost*” or “direct service cost*” or “drug cost*” or “hospital cost*”) AND (“follow-up” or “secondary prevent*” or “after treatment” or “after chemo*” or “after radiation” or “after care” or “after cur*” or “post treatment” or “post chemo*” or “post radiotherapy” or “survivorship care” or “long-term strateg*” or “short-term strateg*”) AND (cancer* or carcinoma* or histiocytosis or leukemia or lymphoma* or medulloblastoma* or neoplasm* or nephroblastoma* or neuroblastoma* or oncolog* or osteosarcoma* or retinoblastoma* or sarcoma* or tumor* or neoplasm*) AND (Australia or Austria or Belgium or Canada or Chile or Colombia or Czech Republic or Denmark or Estonia or Finland or France or Germany or Greece or Hungary or Iceland or Ireland or Israel or Italy or Japan or Korea or Latvia or Lithuania or Luxembourg or Mexico or Netherlands or “New Zealand” or Norway or Poland or Portugal or Slovak Republic or Slovenia or Spain or Sweden or Turkey or “United Kingdom” or England or United States)Filters: 2000–2020 and English | 204 | |
| ||
| (“Follow-up” or “secondary prevent*” or “after treatment” or “after chemo*” or “after radiation” or “after care” or “after cur*” or “post treatment” or “post chemo*” or “post radiotherapy” or “survivorship care” or “long-term strateg*” or “short-term strateg*”) AND (Cancer* or carcinoma* or histiocytosis or leukemia or lymphoma* or medulloblastoma* or neoplasm* or nephroblastoma* or neuroblastoma* or oncolog* or osteosarcoma* or retinoblastoma* or sarcoma* or tumor* or neoplasm*) AND (Australia or Austria or Belgium or Canada or Chile or Colombia or Czech Republic or Denmark or Estonia or Finland or France or Germany or Greece or Hungary or Iceland or Ireland or Israel or Italy or Japan or Korea or Latvia or Lithuania or Luxembourg or Mexico or Netherlands or “New Zealand” or Norway or Poland or Portugal or Slovak Republic or Slovenia or Spain or Sweden or Turkey or “United Kingdom” or England or United States)Filters: English | 750 | |
| ||
| (“follow-up” or “secondary prevent*” or “after treatment” or “after chemo*” or “after radiation” or “after care” or “after cur*” or “post treatment” or “post chemo*” or “post radiotherapy” or “survivorship care” or “long-term strateg*” or “short-term strateg*”) AND (cancer* or carcinoma* or histiocytosis or leukemia or lymphoma* or medulloblastoma* or neoplasm* or nephroblastoma* or neuroblastoma* or oncolog* or osteosarcoma* or retinoblastoma* or sarcoma* or tumor* or neoplasm*) AND (Australia or Austria or Belgium or Canada or Chile or Colombia or Czech Republic or Denmark or Estonia or Finland or France or Germany or Greece or Hungary or Iceland or Ireland or Israel or Italy or Japan or Korea or Latvia or Lithuania or Luxembourg or Mexico or Netherlands or “New Zealand” or Norway or Poland or Portugal or Slovak Republic or Slovenia or Spain or Sweden or Turkey or “United Kingdom” or England or United States)Filters: English | 67 | |
| 17 | |
- −
- Any long-term strategy or any long-term follow-up care or survivorship care (≥5 years after initial treatment) as care used in a supportive role to improve quality of life as well as diagnostic strategy to detect recurrence. Types of care that were included in the review were:
- ○
- Management and/or screening for certain issues such as curable recurrence
- ○
- Diets, including the use of dietary supplements
- ○
- Exercise
- ○
- Counseling
- ○
- E-health technologies: web-based or app-based e-health interventions
- −
- Fertility treatments
- −
- Any study setting (e.g., hospital- or community-based)
- −
- Any form of recruitment
- Studies that either estimated the impact of survivorship care, comparing it to no survivorship care, or compared different long-term care strategies for cancer survivors in OECD countries
- Economic evaluations: costing studies, cost-effectiveness analyses, cost–utility analyses, cost–consequences analyses and cost minimization analyses were included if they reported both the costs and benefits expected for both usual care and the comparator(s)
- Research articles published in English language
- Research limited to human studies
- Full publication or manuscript available for review
- Economic evaluation of active surveillance vs. initial treatment (5)
- Economic evaluation of curative interventions (7)
- Economic evaluation of follow-up care for hyperplasia/dysplasia (12)
- Economic evaluation of follow-up care for mixed patients (1)
- Economic evaluation of management of chemo/radiotherapy-induced symptoms (22)
- Economic evaluation of palliative care (2)
- Economic evaluation of supporting management during initial treatment (31)
- Not follow-up/survivorship care (2)
- Not economic study (4)
- Only focused on costs and did not report health benefits (34)
- Protocols/conference abstract/review papers (38)
- Used same data/reported same study (4)
- Economic evaluation of breast implant (4)
- Economic issue of survivors (8)
- Followed up for less than 5 years (27)
| # | Study Author and Publication Year | Follow-Up Period |
|---|---|---|
| Colorectal cancer | ||
| 1 | Augestad et al. [54] | 24 months |
| 2 | Verberne et al. [55] | 3 years |
| Breast cancer | ||
| 3 | Beaver et al. [56] | 24 months |
| 4 | Benning et al. [57] | 12 months |
| 5 | Burm et al. [58] | 9–15 months |
| 6 | Coyle et al. [59] | 24 months |
| 7 | Kimman et al. [60] | 1 year |
| 8 | Oltra et al. [61] | 3 years |
| 9 | Wojcinski et al. [62] | 12 months |
| Ovarian, uterine cancer | ||
| 10 | Armstrong et al. [63] | 2 years |
| 11 | Dixon et al. [64] | 12 months |
| Head and neck cancer | ||
| 12 | Ham et al. [65] | 3.5 months |
| Others | ||
| 13 | Bongers et al. [66] | Mean (SD) = 31.6 (9.8) months |
| 14 | Greuter et al. [67] | 3 and 6 months |
| 15 | Heinzel et al. [68] | Unclear |
| 16 | Jeyarajah et al. [69] | Mixed 3 and/or 5 years |
| 17 | Kampshoff et al. [70] | 12 weeks |
| 18 | Kent et al. [71] | Up to 5 years |
| 19 | Lizée et al. [72] | 2 years |
| 20 | Moore et al. [73] | 12 months |
| 21 | Nam et al. [74] | Unclear |
| 22 | Polinder et al. [75] | 12 months |
| 23 | Pollack et al. [76] | 366–1095 days |
| 24 | Shih et al. [77] | 6 months |
| 25 | van der Spek et al. [78] | 6 months |
| 26 | van Dongen et al. [79] | 12 months |
| 27 | van Loon et al. [80] | Up to 5 years |
- 16.
- Record the first author’s last name and initials
- 17.
- Record the journal name
- 18.
- Record the year of publication
- 19.
- Record the volume and page numbers
- 20.
- Setting
- 21.
- Type of cancer
- 22.
- Patient population (age if available)
- 23.
- Intervention
- 24.
- Comparator
- 25.
- Type of economic evaluation
- 26.
- Study design
- 27.
- Discount rate
- 28.
- Perspective
- 29.
- Costs included
- 30.
- Time horizon/study period
- 31.
- Outcome measures
- 32.
- Baseline analysis
- 33.
- Sensitivity analysis
- 34.
- Main results
- 35.
- Additional comments (a threshold value, etc.)
Appendix C
| Author (Publication Year) | Setting | Type of Cancer | Intervention | Comparator | EE Type | Study Design | Discount Rate | Perspective | Costs Included | Time Horizon Study Period | Outcome Measures | Sensitivity Analysis | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Staib et al., (2000) | Germany | Colorectal | Intensive follow-up | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Personnel, infrastructure and test costs | 10 years | Cost per followed cancer patient | Not conducted |
| 2 | Bleeker et al., (2001) | The Netherlands | Colonic | Mixed follow-up | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Tests and examination costs | 43 months | Cost of follow-up diagnostic event per curative resected recurrence | Not conducted |
| 3 | Borie et al., (2004) | France | Colorectal | Standard follow-up | Simplified follow-up | CUA | Markov Model | NA | Not reported (health system) | The costs of the examination carried out | 5-7 years | Δcost/ΔQALY | OW |
| 4 | Renehan et al., (2004) | UK | Colorectal | Intensive follow-up | Usual follow-up | CEA | 5-year trail model | Benefits 1.5% and costs 6% | Health service perspective | Direct, indirect and overhead costs | 5 years | Δcost/ΔLY | OW, SA |
| 5 | Macafee et al., (2008) | UK | Colorectal | Intensive follow-up | Usual follow-up | CEA | Retrospective data used for 5-year projection | Costs 3.5% | Hospital perspective | Direct hospital costs | 5 years | Cost of follow-up and cost of resectable recurrence | SA |
| 6 | Di Cristofaro et al., (2012) | Italy | Colorectal | Multiple surveillance protocols | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Costs for follow-up tests | 5 years | The costs and the percentage of recurrence following the various surveillance protocols Recurrence rate | Not conducted |
| 7 | Mant et al., (2017) | UK | Colorectal | CT and CEA follow-up | Minimal follow-up | CUA | Randomized controlled trial and a pre-trial economic model | Costs and benefits 3.5% | The perspective of the UK NHS | Costs for visits and tests | 8 years | Δcost/ΔQALY | SA, TA |
| 8 | Grogan et al., (2002) | Australia | Breast | 13 follow-up schedules | Minimal follow-up | Costing study | Retrospective data audit used to establish an empirical model | NA | Not reported (health system) | Costs for visits and tests | 70 months | Cost of follow-up per detection of salvageable event per patient | Not conducted |
| 9 | Kokko et al., (2005) | Finland | Breast | Routine follow-up | Unclear | Costing study | Randomized controlled trial | No | The hospital perspective | Costs for visits and tests | 4 years | Cost of follow-up per patient Cost per detected recurrence | Not conducted |
| 10 | Robertson et al., (2011) | UK | Breast | Mammography | No surveillance | CUA | Markov modeling | Costs and benefits 3.5% | The UK NHS | Costs incurred by the NHS | Lifetime | Δcost/ΔQALY | OW, MW, TA |
| 11 | Lu et al., (2012) | The Netherlands | Breast | 3 alternate strategies | Guideline follow-up | CEA | An extended and validated simulation model | NA | Not reported (health system) | Costs for follow-up tests Percentage of small tumors identified by tests | Lifetime | Detection rate of small tumors (2 cm or smaller) and associated costs for each strategy Additional costs associated with an increase of 1% in the number of early breast cancers detected | Not conducted |
| 12 | Bessen et al., (2015) | Australia | Breast | Intensive follow-up | Simplified follow-up | CUA | Retrospective data audit and discrete event simulation model | NA | Not reported (health system) | Costs for tests | 5 years | Cost per QALY gained; Δcost/ΔQALY | SA, PSA |
| 13 | Draeger et al., (2020) | The Netherlands | Breast | Unclear | Unclear | CEA | Quasi-experimental pre/post study | NA | Not reported (health system) | Costs for diagnostic procedures, clinical follow-up visits | 5 years | Potential savings of follow-up | Predefined follow-up sensitivity analysis |
| 14 | Hengge et al., (2007) | Germany | Melanoma | Intensive follow-up | Guideline follow-up | CUA | Markov model | NA | Not reported (health system) | Actual costs for materials, scans, human resources and overhead costs | 5 years | Costs per detected metastasis and cost per QALY gained | Not conducted |
| 15 | Leiter et al., (2009) | Germany | Melanoma | Technical | None | CEA | Retrospective data audit | NA | Not reported (health system) | Cost for each technical follow-up investigation | 5 years | Costs for the detection of one recurrence | Not conducted |
| 16 | Podlipnik et al., (2019) | Spain | Malignant melanoma | CT | Contrast brain MRI | CEA | Decision tree | Not applied | Healthcare system | Costs for visits and tests | 5 years | Cost-effectiveness ratio per patient | OW, SA |
| 17 | Forni et al., (2007) | Italy | Cervical | Simplified follow-up | Usual follow-up | CEA | Retrospective data audit | NA | Not reported (health system) | The costs of the examination carried out | 5 years | The number of recurrences, cost of per recurrence per patient | Not conducted |
| 18 | Baena-Cañada et al., (2013) | UK | Cervical | Primary care follow-up | Specialist-led follow-up | CMA | Retrospective data audit | NA | Not reported (health system) | Costs for visits and complementary tests | 5 years | Cost of the follow-up, events, HRQL and satisfaction | Not conducted |
| 19 | Auguste et al., (2014) | UK | Cervical | MRI with or without CT | Clinical follow-up | CUA | Markov model | Costs 3.5% | Healthcare system | Costs for tests | 5 years | Δcost/ΔQALY | OW, SA, PSA |
| 20 | Shah et al., (2015) | Australia | Head, neck + nasopharyngeal | PET-CT scan | No PET-CT scan | CEA | Quasi-experimental pre/post study | Costs 5% | Hospital perspective | Direct costs | 5 years | Cost of follow-up strategies The proportion of radically treatable recurrences | Not conducted |
| 21 | Meregaglia et al., (2018) | Italy and Switzerland | Head and neck | Intensive follow-up | Symptom-driven surveillance | CUA | Markov model | Costs and benefits 3% | Healthcare system | Costs for hospital admissions, specialist visits, radiological exams, laboratory tests and outpatient treatment | Lifetime | Δcost/ΔQALY Δcost/ΔLYG | OW, TW, PSA |
| 22 | Dryver et al., (2003) | Canada | Hodgkin’s disease | CXR, CT, blood count | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Costs for visits and tests | 1–120 months | the cost per true relapse | Not conducted |
| 23 | Guadagnolo et al., (2006) | USA | Hodgkin’s disease | Routine annual CT | Non-CT modalities | CUA | Markov model | Costs and benefits 3% | Modified societal perspective | Visits and blood tests | Lifetime | Δcost/ΔQALY and Δcost/ΔLY | SA, OW |
| 24 | Clasen et al., (2009) | Germany | Seminoma | Technical | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Cost for each technical follow-up investigation | 10 years | Cost per relapse detected | Not conducted |
| 25 | Charytonowicz et al., (2019) | USA | TGCT | mRNA testing | CT-based follow-up | Costing study | Markov model | Costa and benefits 5% | Healthcare system | Costs for visits and tests | 10 years | The sensitivity of each tests The cost of follow-up care | OW |
| 26 | Gilbert et al., (2000) | Canada | Lung | Specialist outpatient | Non-specialist follow-up | CEA | Retrospective data audit | NA | Not reported (health system) | Personnel, infrastructure and test costs | 1 to 107 months | Cost per recurrence detected by a surgeon or FP and 5 years survival rate | Not conducted |
| 27 | Dion et al., (2010) | Canada | Renal | Clinical guidelines | Usual follow-up | CEA | Retrospective data audit | NA | Not reported (health system) | Costs for visits and tests | 5 years | The total cost of follow-up per patient and per patient month The cost per recurrence | Not conducted |
| 28 | C. R. Rettenmaier et al., (2010) | USA | Uterine | Imaging | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Costs for tests and visits | 20 years | The cost per patient recurrence | Not conducted |
| 29 | N. Rettenmaier et al., (2010) | USA | Ovarian and primary peritoneal | Imaging | None | Costing study | Retrospective data audit | NA | Not reported (health system) | Costs for tests and visits | 16 years | The cost per patient recurrence | Not conducted |
| 30 | Imran et al., (2019) | Canada | Thyroid | Primary care follow- up | Tertiary care follow-up | CEA | Retrospective data audit | NA | Not reported | Costs for visits and tests Travel costs | 62 months | Cost of follow-up care and travel cost per patients Rates of recurrence and cancer-related mortality | Not conducted |
| 31 | Dansk et al., (2016) | Sweden | Bladder | Flexible cystoscopy with WLFC and BLFC | Flexible cystoscopy with WLFC only | CCA | Mixed: decision tree and Markov model | Costs 3% | Hospital and other purchaser perspectives | Costs for visits and tests | 5 years | Cost of follow-up strategy Detection rate, hospital bed days and number of procedures | SA |
| 32 | Pearce et al., (2016) | Ireland | Prostate | Guideline follow-up | Current guideline | CMA | Markov model | Costs 5% | Healthcare payer | Costs for visits | 10 years | The average cost of follow-up per survivor | OW, PSA |
| 33 | Gao et al., (2017) | Australia | Hem. malignancy | 12-month intervention | None | CEA | Markov model | Costs and benefits 3% | Health sector perspective | Costs for individual fitness activities, dietician time, project manager/physiotherapist time | Lifetime | Δcost/Δhealth- adjusted life years (HALYs) gained | OW, SA |
| 34 | Ehrhardt et al., (2020) | USA | Childhood cancer | 1-, 2-, 3-, 5- and 10-year interval screening | No screening | CUA | Microsimulation model | Costs and benefits 3% | Not reported (societal perspective) | Medical costs and indirect patient costs, such as lost work time | Lifetime | Δcost/ΔQALY | OW, TW |
Appendix D
| Number of ITEM | Description of ITEM | Summary of Criterion |
|---|---|---|
| Item 1 | Identify the study as an economic evaluation or use more specific terms such as “cost-effectiveness analysis”, and describe the interventions compared. | Title identifies an economic evaluation |
| Item 2 | Provide a structured summary of objectives, perspective, setting, methods (including study design and inputs), results (including base case and uncertainty analyses) and conclusions. | Structured summary was presented in abstract |
| Item 3 | Provide an explicit statement of the broader context for the study. Present the study question and its relevance for health policy or practice decisions. | Background and objectives were provided |
| Item 4 | Describe characteristics of the base case population and subgroups analyzed, including why they were chosen. | Target population and subgroups were reported |
| Item 5 | State relevant aspects of the system(s) in which the decision(s) need(s) to be made. | Setting and location were reported |
| Item 6 | Describe the perspective of the study and relate this to the costs being evaluated. | Study perspective was reported |
| Item 7 | Describe the interventions or strategies being compared and state why they were chosen. | Comparator(s) was/were reported |
| Item 8 | State the time horizon(s) over which costs and consequences are being evaluated and say why appropriate. | Time horizon was reported |
| Item 9 | Report the choice of discount rate(s) used for costs and outcomes and say why appropriate. | Discount rate was used |
| Item 10 | Describe what outcomes were used as the measure(s) of benefit in the evaluation and their relevance for the type of analysis performed. | Choice of health outcomes was reported |
| Item 11 | a. Single study-based estimates: Describe fully the design features of the single effectiveness study and why the single study was a sufficient source of clinical effectiveness data. b. Synthesis-based estimates: Describe fully the methods used for identification of included studies and synthesis of clinical effectiveness data. | a. Measurement of effectiveness (single study-based) b. Measurement of effectiveness (synthesis-based) was reported |
| Item 12 | If applicable, describe the population and methods used to elicit preferences for outcomes. | Measurement and valuation of preference-based outcomes |
| Item 13 | a. Single study-based economic evaluation: Describe approaches used to estimate resource use associated with the alternative interventions. Describe primary or secondary research methods for valuing each resource item in terms of its unit cost. Describe any adjustments made to approximate to opportunity costs. b. Model-based economic evaluation: Describe approaches and data sources used to estimate resource use associated with model health states. Describe primary or secondary research methods for valuing each resource item in terms of its unit cost. Describe any adjustments made to approximate to opportunity costs. | a. Estimating resources and costs—single study-based b. Estimating resources and costs—model-based |
| Item 14 | Report the dates of the estimated resource quantities and unit costs. Describe methods for adjusting estimated unit costs to the year of reported costs if necessary. Describe methods for converting costs into a common currency base and the exchange rate. | Currency, price date and conversion were reported |
| Item 15 | Describe and give reasons for the specific type of decision-analytical model used. Providing a figure to show model structure is strongly recommended. | Choice of model was reported |
| Item 16 | Describe all structural or other assumptions underpinning the decision-analytical model. | Assumptions were described |
| Item 17 | Describe all analytical methods supporting the evaluation. This could include methods for dealing with skewed, missing, or censored data; extrapolation methods; methods for pooling data; approaches to validate or make adjustments (such as half cycle corrections) to a model; and methods for handling population heterogeneity and uncertainty. | Analytic methods were described |
| Item 18 | Report the values, ranges, references and, if used, probability distributions for all parameters. Report reasons or sources for distributions used to represent uncertainty where appropriate. Providing a table to show the input values is strongly recommended. | Study parameters were reported |
| Item 19 | For each intervention, report mean values for the main categories of estimated costs and outcomes of interest, as well as mean differences between the comparator groups. If applicable, report incremental cost-effectiveness ratios. | Incremental cost and outcomes were reported |
| Item 20 | a. Single study-based economic evaluation: Describe the effects of sampling uncertainty for the estimated incremental cost and incremental effectiveness parameters, together with the impact of methodological assumptions (such as discount rate, study perspective). b. Model-based economic evaluation: Describe the effects on the results of uncertainty for all input parameters, and uncertainty related to the structure of the model and assumptions. | a. Characterizing uncertainty (single study-based) b. Characterizing uncertainty (model-based) was reported |
| Item 21 | If applicable, report differences in costs, outcomes, or cost-effectiveness that can be explained by variations between subgroups of patients with different baseline characteristics or other observed variability in effects that are not reducible by more information. | Characterizing heterogeneity was reported |
| Item 22 | Summarize key study findings and describe how they support the conclusions reached. Discuss limitations and the generalizability of the findings and how the findings fit with current knowledge. | Study findings, limitations, generalizability and current knowledge were mentioned |
| Item 23 | Describe how the study was funded and the role of the funder in the identification, design, conduct, and reporting of the analysis. Describe other nonmonetary sources of support. | Source of funding was mentioned |
| Item 24 | Describe any potential for conflict of interest of study contributors in accordance with journal policy. In the absence of a journal policy, we recommend authors comply with International Committee of Medical Journal Editors recommendations. | Conflicts of interest were presented |
| Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Item 12 | Item 13 | Item 14 | Item 15 | Item 16 | Item 17 | Item 18 | Item 19 | Item 20 | Item 21 | Item 22 | Item 23 | Item 24 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Summary of criterion | Compliance with the CHEERS checklist | Title identifies an economic evaluation | Structured summary was presented in abstract | Background and objectives were provided | Target population and subgroups were reported | Setting and location were reported | Study perspective was reported | Comparator(s) was/were reported | Time horizon was reported | Discount rate was used | Choice of health outcomes was reported | a. Measurement of effectiveness (single study-based)b. Measurement of effectiveness (synthesis-based) was reported | Measurement and valuation of preference-based outcomes | a. Estimating resources and costs (single study-based)b. Estimating resources and costs (model-based) | Currency, price date and conversion were reported | Choice of model was reported | Assumptions were described | Analytic methods were described | Study parameters were reported | Incremental cost and outcomes were reported | a. Characterizing uncertainty (single study-based)b. Characterizing uncertainty (model based) was reported | Characterizing heterogeneity was reported | Study findings, limitations, generalizability and current knowledge were mentioned | Source of funding was mentioned | No conflicts of interest were presented | |
| Colorectal cancer | ||||||||||||||||||||||||||
| 1 | Staib et al., (2000) | 50% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 0 | 1 | NA | 1 | 1 | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 0.5 i | 0 | 0 |
| 2 | Bleeker et al., (2001) | 48% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 0 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 0.5 i | 1 | 0 |
| 3 | Borie et al., (2004) | 65% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 0.5 c | 1 | 0 | 1 | 0.5 e | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 |
| 4 | Renehan et al., (2004) | 83% | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 c | 1 | 0.5 e | NA | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 |
| 5 | Macafee et al., (2008) | 63% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | 0.5 c | 1 | 0.5 e | NA | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| 6 | Di Cristofaro et al., (2012) | 60% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 0 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 1 | 0 | 1 | 1 | 0.5 i | 0 | 0 |
| 7 | Mant et al., (2017) | 85% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 c | 1 | 0.5 e | 1 | 1 | 1 | 0.5 f | 1 | 1 | 1 | 1 | 0.5 h | 0 | 1 | 1 | 1 |
| Breast cancer | ||||||||||||||||||||||||||
| 8 | Grogan et al., (2002) | 46% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | 0 | 1 | 0.5 e | NA | 1 | 1 | 0.5 f | 0 | 0 | 0 | 0 | 0 | 0 | 0.5 i | 1 | 0 |
| 9 | Kokko et al., (2005) | 60% | 0.5 a | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| 10 | Robertson et al., (2011) | 92% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| 11 | Lu et al., (2012) | 65% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0.5 e | NA | 1 | 1 | 1 | 0 | 0.5 g | 1 | 0 | 1 | 0 | 1 | 0 | 1 |
| 12 | Bessen et al., (2015) | 71% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | 0 | 1 | 0.5 e | NA | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 |
| 13 | Draeger et al., (2020) | 68% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 1 | 1 | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 1 | 0 | 0 | 1 | 1 | 1 |
| Skin cancer | ||||||||||||||||||||||||||
| 14 | Hengge et al., (2007) | 52% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | 0 | 1 | 0.5 e | NA | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| 15 | Leiter et al., (2009) | 58% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 0 | 1 | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 1 | 1 | 0 | 1 | 0 |
| 16 | Podlipnik et al., (2019) | 71% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | 0.5 d | 1 | 0.5 e | NA | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 |
| Cervical cancer | ||||||||||||||||||||||||||
| 17 | Forni et al., (2007) | 53% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| 18 | Baena-Cañada et al., (2013) | 60% | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 0.5 c | NA | 1 | 0.5 e | 1 | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| 19 | Auguste et al., (2014) | 94% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Head and neck cancer | ||||||||||||||||||||||||||
| 20 | Shah et al., (2015) | 66% | 0.5 a | 0.5 b | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 e | NA | 1 | 1 | NA | 1 | NA | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| 21 | Meregaglia et al., (2018) | 90% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | 0.5 c | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Hodgkin’s disease | ||||||||||||||||||||||||||
| 22 | Dryver et al., (2003) | 48% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 0 | 1 | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| 23 | Guadagnolo et al., (2006) | 88% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 |
| Testicular cancer | ||||||||||||||||||||||||||
| 24 | Clasen et al., (2009) | 48% | 0.5 a | 0 | 1 | 1 | 1 | 0 | 0 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 1 | 1 | 0 | 0 |
| 25 | Charytonowicz et al., (2019) | 79% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 e | NA | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 |
| Others | ||||||||||||||||||||||||||
| 26 | Gilbert et al., (2000) | 48% | 0 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| 27 | Dion et al., (2010) | 63% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| 28 | C. R. Rettenmaier et al., (2010) | 45% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 0 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| 29 | N. Rettenmaier et al., (2010) | 50% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 0 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| 30 | Imran et al., (2019) | 55% | 0.5 a | 0.5 b | 1 | 1 | 1 | 0 | 1 | 0.5 c | NA | 1 | 0.5 e | NA | 1 | 1 | NA | NA | NA | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| 31 | Dansk et al., (2016) | 90% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 c | 1 | 0.5 e | NA | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 32 | Pearce et al., (2016) | 98% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 33 | Gao et al., (2017) | 94% | 1 | 0.5 b | 1 | 1 | 1 | 1 | 1 | 0.5 c | 0.5 c | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 34 | Ehrhardt et al., (2020) | 90% | 1 | 0.5 b | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- AIHW, “Cancer data in Australia,” Australian Institute of Health and Welfare, Canberra, Australia. 2021. Available online: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/contents/cancer-survival-data-visualisation (accessed on 23 July 2021).
- OECD, “Health Care Quality Indicators: Cancer Care,” Organisation for Economic Co-operation and Development Online. 2021. Available online: https://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_LTCR (accessed on 26 July 2021).
- Shapiro, C.L. Cancer Survivorship. N. Engl. J. Med. 2018, 379, 2438–2450. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar]
- Graves, N. Make economics your friend. J. Hosp. Infect. 2018, 100, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Frew, E.; Breheny, K. Health economics methods for public health resource allocation: A qualitative interview study of decision makers from an English local authority. Health Economics. Policy Law 2020, 15, 128–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Q.; Graves, N.; Pacella, R.E. Economic evaluations of guideline-based care for chronic wounds: A systematic review. Appl. Health Econ. Health Policy 2018, 16, 633–651. [Google Scholar] [CrossRef]
- McCreanor, V.; Graves, N.; Barnett, A.G.; Parsonage, W.; Merlo, G. A systematic review and critical analysis of cost-effectiveness studies for coronary artery disease treatment. F1000Research 2018, 7, 77. [Google Scholar] [CrossRef]
- Gubler-Gut, B.E.; Pöhlmann, J.; Flatz, A.; Schwenkglenks, M.; Rohrmann, S. Cost-effectiveness of physical activity interventions in cancer survivors of developed countries: A systematic review. J. Cancer Surviv. 2021, 15, 961–975. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Marzorati, C.; Riva, S.; Pravettoni, G. Who is a cancer survivor? A systematic review of published definitions. J. Cancer Educ. 2017, 32, 228–237. [Google Scholar] [CrossRef]
- Denlinger, C.S.; Carlson, R.W.; Are, M.; Baker, K.S.; Davis, E.; Edge, S.B.; Friedman, D.L.; Goldman, M.; Jones, L.; King, A. Survivorship: Introduction and definition. J. Natl. Compr. Canc. Netw. 2014, 12, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bessen, T.; Keefe, D.M.; Karnon, J. Does one size fit all? Cost utility analyses of alternative mammographic follow-up schedules, by risk of recurrence. Int. J. Technol. Assess. Health Care Jan. 2015, 31, 281–288. [Google Scholar] [CrossRef]
- Bessen, T.; Karnon, J. A patient-level calibration framework for evaluating surveillance strategies: A case study of mammographic follow-up after early breast cancer. Value Health 2014, 17, 669–678. [Google Scholar] [CrossRef] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated health economic evaluation reporting standards (CHEERS) statement. Cost Eff. Res. Alloc. 2013, 11, 6. [Google Scholar] [CrossRef] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)—Explanation and Elaboration: A Report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013, 16, e1–e5. [Google Scholar] [CrossRef] [Green Version]
- Bleeker, W.A.; Mulder, N.H.; Hermans, J.; Otter, R.; Plukker, J.T. Value and cost of follow-up after adjuvant treatment of patients with Dukes’ C colonic cancer. Br. J. Surg. 2001, 88, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Di Cristofaro, L.; Scarpa, M.; Angriman, I.; Perissinotto, E.; Ruffolo, C.; Frego, M.; Erroi, F. Cost-effectiveness analysis of postoperative surveillance protocols following radical surgery for colorectal cancer. Acta Chir. Belg. 2012, 112, 24–32. [Google Scholar] [CrossRef]
- Staib, L.; Link, K.H.; Beger, H.G. Follow-up in colorectal cancer: Cost-effectiveness analysis of established and novel concepts. Langenbeck’s Arch. Surg. 2000, 385, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Borie, F.; Combescure, C.; Daurès, J.-P.; Trétarre, B.; Millat, B. Cost-effectiveness of two follow-up strategies for curative resection of colorectal cancer: Comparative study using a Markov model. World. J. Surg. 2004, 28, 563–569. [Google Scholar] [CrossRef]
- Macafee, D.A.; Whynes, D.K.; Scholefield, J.H. Risk-stratified intensive follow up for treated colorectal cancer - realistic and cost saving? Colorectal Dis. 2008, 10, 222–230. [Google Scholar] [CrossRef]
- Mant, D.; Gray, A.; Pugh, S.; Campbell, H.; George, S.; Fuller, A.; Shinkins, B.; Corkhill, A.; Mellor, J.; Dixon, E.; et al. A randomised controlled trial to assess the cost-effectiveness of intensive versus no scheduled follow-up in patients who have undergone resection for colorectal cancer with curative intent. Health Technol. Assess. 2017, 21, 1–86. [Google Scholar] [CrossRef] [Green Version]
- Renehan, A.G.; O’Dwyer, S.T.; Whynes, D.K. Cost effectiveness analysis of intensive versus conventional follow up after curative resection for colorectal cancer. BMJ 2004, 328, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Téhard, B.; Detournay, B.; Borget, I.; Roze, S.; De Pouvourville, G. Value of a QALY for France: A New Approach to Propose Acceptable Reference Values. Value Health 2020, 23, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Grogan, M.; Rangan, A.; Gebski, V.; Boyages, J. The value of follow-up of patients with early breast cancer treated with conservative surgery and radiation therapy. Breast 2002, 11, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Kokko, R.; Hakama, M.; Holli, K. Follow-up cost of breast cancer patients with localized disease after primary treatment: A randomized trial. Breast Cancer Res. Treat. 2005, 93, 255–260. [Google Scholar] [CrossRef]
- Robertson, C.; Arcot Ragupathy, S.K.; Boachie, C.; Dixon, J.M.; Fraser, C.; Hernández, R.; Heys, S.; Jack, W.; Kerr, G.R.; Lawrence, G.; et al. The clinical effectiveness and cost-effectiveness of different surveillance mammography regimens after the treatment for pri-mary breast cancer: Systematic reviews registry database analyses and economic evaluation. Health Technol. Assess. 2011, 15, 1–322. [Google Scholar] [CrossRef]
- Lu, W.; Greuter, M.J.; Schaapveld, M.; Vermeulen, K.M.; Wiggers, T.; de Bock, G.H. Safety and cost-effectiveness of shortening hospital follow-up after breast cancer treatment. Br. J. Surg. 2012, 99, 1227–1233. [Google Scholar] [CrossRef] [Green Version]
- Hengge, U.R.; Wallerand, A.; Stutzki, A.; Kockel, N. Cost-effectiveness of reduced follow-up in malignant melanoma. J. Dtsch. Derm. Ges. 2007, 5, 898–907. [Google Scholar] [CrossRef]
- Leiter, U.; Marghoob, A.A.; Lasithiotakis, K.; Eigentler, T.K.; Meier, F.; Meisner, C.; Garbe, C. Costs of the detection of metastases and follow-up examinations in cutaneous melanoma. Melanoma Res. 2009, 19, 50–57. [Google Scholar] [CrossRef]
- Podlipnik, S.; Moreno-Ramírez, D.; Carrera, C.; Barreiro, A.; Manubens, E.; Ferrandiz-Pulido, L.; Sánchez, M.; Vidal-Sicart, S.; Malvehy, J.; Puig, S. Cost-effectiveness analysis of imaging strategy for an intensive follow-up of patients with American Joint Committee on Cancer stage IIB, IIC and III malignant melanoma. Br. J. Derm. 2019, 180, 1190–1197. [Google Scholar] [CrossRef]
- Forni, F.; Ferrandina, G.; Deodato, F.; Macchia, G.; Morganti, A.G.; Smaniotto, D.; Luzi, S.; D’Agostino, G.; Valentini, V.; Cellini, N. Squamous cell carcinoma antigen in follow-up of cervical cancer treated with radiotherapy: Evaluation of cost-effectiveness. Int. J. Radiat Oncol. Biol. Phys. 2007, 69, 1145–1149. [Google Scholar] [CrossRef]
- Baena-Cañada, J.M.; Ramírez-Daffós, P.; Cortés-Carmona, C.; Rosado-Varela, P.; Nieto-Vera, J.; Benítez-Rodríguez, E. Follow-up of long-term survivors of breast cancer in primary care versus specialist attention. Fam Pr. 2013, 30, 525–532. [Google Scholar] [CrossRef] [Green Version]
- Auguste, P.; Barton, P.; Meads, C.; Davenport, C.; Małysiak, S.; Kowalska, M.; Zapalska, A.; Guest, P.; Martin-Hirsch, P.; Borowiack, E.; et al. Evaluating PET-CT in routine surveillance and follow-up after treatment for cervical cancer: A cost-effectiveness analysis. BJOG 2014, 121, 464–476. [Google Scholar] [CrossRef]
- Meads, C.; Davenport, C.; Małysiak, S.; Kowalska, M.; Zapalska, A.; Guest, P.; Martin-Hirsch, P.; Borowiack, E.; Auguste, P.; Barton, P. Evaluating PET-CT in the detection and management of recurrent cervical cancer: Systematic reviews of diagnostic accuracy and subjective elicitation. Int. J. Gynaecol. Obs. 2014, 121, 398–407. [Google Scholar] [CrossRef] [Green Version]
- Shah, K.; Te Marvelde, L.; Collins, M.; De Abreu Lourenco, R.; D’Costa, I.; Coleman, A.; Fua, T.; Liu, C.; Rischin, D.; Lau, E.; et al. Safety and cost analysis of an (18)FDG-PET-CT response based follow-up strategy for head and neck cancers treated with primary radiation or chemoradiation. Oral Oncol. 2015, 51, 529–535. [Google Scholar] [CrossRef]
- Meregaglia, M.; Cairns, J.; Licitra, L.; Bossi, P. The use of intensive radiological assessments in routine surveillance after treatment for head and neck cancer: An economic evaluation. Eur. J. Cancer 2018, 93, 89–98. [Google Scholar] [CrossRef]
- Dryver, E.T.; Jernström, H.; Tompkins, K.; Buckstein, R.; Imrie, K.R. Follow-up of patients with Hodgkin’s disease following curative treatment: The routine CT scan is of little value. Br. J. Cancer 2003, 89, 482–486. [Google Scholar] [CrossRef] [Green Version]
- Guadagnolo, B.A.; Punglia, R.S.; Kuntz, K.M.; Mauch, P.M.; Ng, A.K. Cost-effectiveness analysis of computerized tomography in the routine follow-up of patients after primary treatment for Hodgkin’s disease. J. Clin. Oncol. 2006, 24, 4116–4122. [Google Scholar] [CrossRef] [PubMed]
- Clasen, J.; Schmidberger, H.; Souchon, R.; Weissbach, L.; Hartmann, M.; Hartmann, J.T.; Hehr, T.; Bamberg, M. What is the value of routine follow-up in stage I seminoma after paraaortic radiotherapy? An analysis of the German Testicular Cancer Study Group (GTCSG) in 675 prospectively followed patients. Strahlenther. Onkol. 2009, 185, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Charytonowicz, D.; Aubrey, H.; Bell, C.; Ferret, M.; Tsui, K.; Atfield, R.; Coleman, N.; Murray, M.J.; Wilson, E.C.F. Cost Analysis of Noninvasive Blood-Based MicroRNA Testing Versus CT Scans for Follow-up in Patients With Testicular Germ-Cell Tumors. Clin. Genitourin. Cancer 2019, 17, e733–e744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, S.; Reid, K.R.; Lam, M.Y.; Petsikas, D. Who should follow up lung cancer patients after operation? Ann. Thorac. Surg. 2000, 69, 1696–1700. [Google Scholar] [CrossRef]
- Dion, M.; Martínez, C.H.; Williams, A.K.; Chalasani, V.; Nott, L.; Pautler, S.E. Cost analysis of two follow-up strategies for localized kidney cancer: A Canadian cohort comparison. Can. Urol. Assoc. J. 2010, 4, 322. [Google Scholar] [CrossRef]
- Rettenmaier, C.R.; Rettenmaier, N.B.; Wojciechowski, T.; Abaid, L.N.; Brown, J.V., III; Micha, J.P.; Goldstein, B.H. The utility of routine follow-up procedures in the surveillance of uterine cancer: A 20-year institutional review. Oncology 2010, 79, 262–268. [Google Scholar] [CrossRef]
- Rettenmaier, N.; Rettenmaier, C.; Wojciechowski, T.; Abaid, L.; Brown, J., III; Micha, J.; Goldstein, B. The utility and cost of routine follow-up procedures in the surveillance of ovarian and primary peritoneal carcinoma: A 16-year institutional review. Br. J. Cancer 2010, 103, 1657–1662. [Google Scholar] [CrossRef] [PubMed]
- Imran, S.A.; Chu, K.; Rajaraman, M.; Rajaraman, D.; Ghosh, S.; De Brabandere, S.; Kaiser, S.M.; Van Uum, S. Primary versus Tertiary Care Follow-Up of Low-Risk Differentiated Thyroid Cancer: Real-World Comparison of Outcomes and Costs for Patients and Health Care Systems. Eur. Thyroid. J. 2019, 8, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Dansk, V.; Malmström, P.U.; Bläckberg, M.; Malmenäs, M. Hexaminolevulinate hydrochloride blue-light flexible cystoscopy in the detection and follow-up of nonmuscle-invasive bladder cancer: Cost consequences during outpatient surveillance in Sweden. Future Oncol. 2016, 12, 1025–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, A.M.; Ryan, F.; Drummond, F.J.; Thomas, A.A.; Timmons, A.; Sharp, L. Comparing the costs of three prostate cancer follow-up strategies: A cost minimisation analysis. Supportive Care Cancer 2016, 24, 879–886. [Google Scholar] [CrossRef]
- Gao, L.; Moodie, M.; Brown, V.; Avery, S. Cost-effectiveness of a lifestyle modification program in long-term survivors of hemopoietic stem cell transplantation. Clin. Transplant. 2017, 31, e13049–e13059. [Google Scholar] [CrossRef]
- Ehrhardt, M.J.; Ward, Z.J.; Liu, Q.; Chaudhry, A.; Nohria, A.; Border, W.; Fulbright, J.M.; Mulrooney, D.A.; Oeffinger, K.C.; Nathan, P.C. Cost-Effectiveness of the International Late Effects of Childhood Cancer Guideline Harmonization Group Screening Guidelines to Prevent Heart Failure in Survivors of Childhood Cancer. J. Clin. Oncol. 2020, 33, 3851–3862. [Google Scholar] [CrossRef] [PubMed]
- Mulrooney, D.A.; Hyun, G.; Ness, K.K.; Ehrhardt, M.J.; Yasui, Y.; Duprez, D.; Howell, R.M.; Leisenring, W.M.; Constine, L.S.; Tonorezos, E. Major cardiac events for adult survivors of childhood cancer diagnosed between 1970 and 1999: Report from the Childhood Cancer Survivor Study cohort. BMJ 2020, 368, 16794. [Google Scholar] [CrossRef] [Green Version]
- Draeger, T.; Voelkel, V.; Groothuis-Oudshoorn, C.G.M.; Lavric, M.; Veltman, J.; Dassen, A.; Boersma, L.J.; Witteveen, A.; Sonke, G.S.; Koffijberg, H.; et al. Applying Risk-Based Follow-Up Strategies on the Dutch Breast Cancer Population: Consequences for Care and Costs. Value Health 2020, 23, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Augestad, K.M.; Norum, J.; Dehof, S.; Aspevik, R.; Ringberg, U.; Nestvold, T.; Vonen, B.; Skrøvseth, S.O.; Lindsetmo, R.O. Cost-effectiveness and quality of life in surgeon versus general practitioner-organised colon cancer surveillance: A randomised controlled trial. BMJ Open 2013, 3, e002391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verberne, C.J.; Wiggers, T.; Grossmann, I.; de Bock, G.H.; Vermeulen, K.M. Cost-effectiveness of a carcinoembryonic antigen (CEA) based follow-up programme for colorectal cancer (the CEA Watch trial). Colorectal. Dis. 2016, 18, O91–O96. [Google Scholar] [CrossRef] [PubMed]
- Beaver, K.; Hollingworth, W.; McDonald, R.; Dunn, G.; Tysver-Robinson, D.; Thomson, L.; Hindley, A.C.; Susnerwala, S.S.; Luker, K. Economic evaluation of a randomized clinical trial of hospital versus telephone follow-up after treatment for breast cancer. Br. J. Surg. 2009, 96, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Benning, T.M.; Kimman, M.L.; Dirksen, C.D.; Boersma, L.J.; Dellaert, B.G.C. Combining individual-level discrete choice experiment estimates and costs to inform health care management decisions about customized care: The case of follow-up strategies after breast cancer treatment. Value Health 2012, 15, 680–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burm, R.; Thewes, B.; Rodwell, L.; Kievit, W.; Speckens, A.; van de Wal, M.; Prins, J. Long-term efficacy and cost-effectiveness of blended cognitive behavior therapy for high fear of recurrence in breast, prostate and colorectal Cancer survivors: Follow-up of the SWORD randomized controlled trial. BMC Cancer 2019, 19, 462. [Google Scholar] [CrossRef] [PubMed]
- Coyle, D.; Grunfeld, E.; Coyle, K.; Pond, G.; Julian, J.A.; Levine, M.N. Cost effectiveness of a survivorship care plan for breast cancer survivors. J. Oncol. Pr. 2014, 10, e86–e92. [Google Scholar] [CrossRef]
- Kimman, M.L.; Dirksen, C.D.; Voogd, A.C.; Falger, P.; Gijsen, B.C.M.; Thuring, M.; Lenssen, A.; van der Ent, F.; Verkeyn, J.; Haekens, C.; et al. Economic evaluation of four follow-up strategies after curative treatment for breast cancer: Results of an RCT. Eur. J. Cancer 2011, 47, 1175–1185. [Google Scholar] [CrossRef]
- Oltra, A.; Santaballa, A.; Munárriz, B.; Pastor, M.; Montalar, J. Cost-benefit analysis of a follow-up program in patients with breast cancer: A randomized prospective study. Breast. J. 2007, 13, 571–574. [Google Scholar] [CrossRef]
- Wojcinski, S.; Farrokh, A.; Hille, U.; Hirschauer, E.; Schmidt, W.; Hillemanns, P.; Degenhardt, F. Optimizing breast cancer follow-up: Diagnostic value and costs of additional routine breast ultrasound. Ultrasound Med. Biol. 2011, 37, 198–206. [Google Scholar] [CrossRef]
- Armstrong, A.; Otvos, B.; Singh, S.; Debernardo, R. Evaluation of the cost of CA-125 measurement, physical exam, and imaging in the diagnosis of recurrent ovarian cancer. Gynecol. Oncol. 2013, 131, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Dixon, P.; Beaver, K.; Williamson, S.; Sutton, C.; Martin-Hirsch, P.; Hollingworth, W. Cost-Consequence Analysis Alongside a Randomised Controlled Trial of Hospital Versus Telephone Follow-Up after Treatment for Endometrial Cancer. Appl. Health Econ. Health Policy 2018, 16, 415–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ham, J.C.; Driessen, C.M.; Hendriks, M.P.; Fiets, E.; Kreike, B.; Hoeben, A.; Slingerland, M.; van Opstal, C.C.; Kullberg, B.J.; Jonker, M.A.; et al. Prophylactic antibiotics reduce hospitalisations and cost in locally advanced head and neck cancer patients treated with chemoradiotherapy: A randomised phase 2 study. Eur. J. Cancer 2019, 113, 32–40. [Google Scholar] [CrossRef]
- Bongers, V.; Hobbelink, M.G.; van Rijk, P.P.; Hordijk, G.J. Cost-effectiveness of dual-head 18F-fluorodeoxyglucose PET for the detection of recurrent laryngeal cancer. Cancer Biother. Radiopharm. 2002, 17, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Greuter, M.J.; Schouten, C.S.; Castelijns, J.A.; de Graaf, P.; Comans, E.F.; Hoekstra, O.S.; de Bree, R.; Coupé, V.M. Cost-effectiveness of response evaluation after chemoradiation in patients with advanced oropharyngeal cancer using 18 F-FDG-PET-CT and/or diffusion-weighted MRI. BMC Cancer 2017, 17, 256. [Google Scholar] [CrossRef] [Green Version]
- Heinzel, A.; Müller, D.; Yekta-Michael, S.S.; Ceccon, G.; Langen, K.-J.; Mottaghy, F.M.; Wiesmann, M.; Kocher, M.; Hattingen, E.; Galldiks, N. O-(2-18F-fluoroethyl)-L-tyrosine PET for evaluation of brain metastasis recurrence after radiotherapy: An effectiveness and cost-effectiveness analysis. Neuro-Oncol. 2017, 19, 1271–1278. [Google Scholar] [CrossRef]
- Jeyarajah, S.; Adams, K.; Higgins, L.; Ryan, S.; Leather, A.; Papagrigoriadis, S. Prospective evaluation of a colorectal cancer nurse follow-up clinic. Colorectal. Dis. 2011, 13, 31–38. [Google Scholar] [CrossRef]
- Kampshoff, C.S.; van Dongen, J.M.; van Mechelen, W.; Schep, G.; Vreugdenhil, A.; Twisk, J.W.R.; Bosmans, J.E.; Brug, J.; Chinapaw, M.J.M.; Buffart, L.M. Long-term effectiveness and cost-effectiveness of high versus low-to-moderate intensity resistance and endurance exercise interventions among cancer survivors. J. Cancer Surviv. 2018, 12, 417–429. [Google Scholar] [CrossRef] [Green Version]
- Kent, M.S.; Korn, P.; Port, J.L.; Lee, P.C.; Altorki, N.K.; Korst, R.J. Cost effectiveness of chest computed tomography after lung cancer resection: A decision analysis model. Ann. Thorac. Surg. 2005, 80, 1215–1222, discussion 1222-3. [Google Scholar] [CrossRef]
- Lizée, T.; Basch, E.; Trémolières, P.; Voog, E.; Domont, J.; Peyraga, G.; Urban, T.; Bennouna, J.; Septans, A.L.; Balavoine, M.; et al. Cost-Effectiveness of Web-Based Patient-Reported Outcome Surveillance in Patients With Lung Cancer. J. Thorac. Oncol. 2019, 14, 1012–1020. [Google Scholar] [CrossRef]
- Moore, S.; Corner, J.; Haviland, J.; Wells, M.; Salmon, E.; Normand, C.; Brada, M.; O’Brien, M.; Smith, I. Nurse led follow up and conventional medical follow up in management of patients with lung cancer: Randomised trial. BMJ 2002, 325, 1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, R.K.; Redelmeier, D.A.; Spiess, P.E.; Sampson, H.A.; Fradet, Y.; Jewett, M.A. Comparison of molecular and conventional strategies for followup of superficial bladder cancer using decision analysis. J. Urol. 2000, 163, 752–757. [Google Scholar] [CrossRef]
- Polinder, S.; Verschuur, E.M.L.; Siersema, P.D.; Kuipers, E.J.; Steyerberg, E.W. Cost comparison study of two different follow-up protocols after surgery for oesophageal cancer. Eur. J. Cancer 2009, 45, 2110–2115. [Google Scholar] [CrossRef]
- Pollack, C.E.; Frick, K.D.; Herbert, R.J.; Blackford, A.L.; Neville, B.A.; Wolff, A.C.; Carducci, M.A.; Earle, C.C.; Snyder, C.F. It’s who you know: Patient-sharing, quality, and costs of cancer survivorship care. J. Cancer Surviv. 2014, 8, 156–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, S.T.F.; Butow, P.; Bowe, S.J.; Thewes, B.; Turner, J.; Gilchrist, J.; Mihalopoulos, C. Cost-effectiveness of an intervention to reduce fear of cancer recurrence: The Conquerfear randomized controlled trial. Psycho-Oncol. 2019, 28, 1071–1079. [Google Scholar] [CrossRef]
- van der Spek, N.; Jansen, F.; Holtmaat, K.; Vos, J.; Breitbart, W.; van Uden-Kraan, C.F.; Tollenaar, R.A.E.M.; Cuijpers, P.; Coupé, V.M.H.; Verdonck-de Leeuw, I.M. Cost-utility analysis of meaning-centered group psychotherapy for cancer survivors. Psycho-Oncol. 2018, 27, 1772–1779. [Google Scholar] [CrossRef]
- van Dongen, J.M.; Persoon, S.; Jongeneel, G.; Bosmans, J.E.; Kersten, M.J.; Brug, J.; Nollet, F.; Chinapaw, M.J.M.; Buffart, L.M. Long-term effectiveness and cost-effectiveness of an 18-week supervised exercise program in patients treated with autologous stem cell transplantation: Results from the EXIST study. J. Cancer Surviv. 2019, 13, 558–569. [Google Scholar] [CrossRef] [Green Version]
- van Loon, J.; Grutters, J.P.; Wanders, R.; Boersma, L.; Dingemans, A.M.; Bootsma, G.; Geraedts, W.; Pitz, C.; Simons, J.; Brans, B.; et al. 18FDG-PET-CT in the follow-up of non-small cell lung cancer patients after radical radiotherapy with or without chemotherapy: An economic evaluation. Eur. J. Cancer 2010, 46, 110–119. [Google Scholar] [CrossRef]

| Descriptive Variable | Number of Studies |
|---|---|
| Study design | |
| Retrospective data audit | 13 |
| Markov model | 9 |
| Other models | 6 |
| Randomized control trial | 1 |
| Decision tree model | 1 |
| Discrete event simulation model | 1 |
| Mixed: decision tree + Markov model | 1 |
| Quasi-experimental pre/post-study | 2 |
| Study Location | |
| UK | 6 |
| USA | 5 |
| Germany | 4 |
| Australia | 4 |
| Canada | 4 |
| Italy | 3 * |
| Netherlands | 3 |
| Sweden | 1 |
| France | 1 |
| Finland | 1 |
| Ireland | 1 |
| Spain | 1 |
| Switzerland | 1 * |
| Type of cancer | |
| Colorectal | 7 |
| Breast | 6 |
| Cutaneous melanoma | 3 |
| Cervical | 3 |
| Head and neck | 2 |
| Hodgkin’s disease | 2 |
| Testicular cancer | 2 |
| Prostate | 1 |
| Hematological malignancy | 1 |
| Bladder | 1 |
| Lung | 1 |
| Ovarian | 1 |
| Renal | 1 |
| Thyroid | 1 |
| Uterine | 1 |
| Not mentioned (childhood cancer) | 1 |
| Publication year (CHEERS checklist became available after 2013) | |
| Before 2013 | 20 |
| After 2013 | 14 |
| Study | Reasons | Level of Usefulness (Strong/Moderate/Limited) | ||||||
|---|---|---|---|---|---|---|---|---|
| Model-Based Design | Applied Model Calibration | Direct and Indirect Costs Included | Quality of Life Measure | Outcome Presented as ICER | Full Sensitivity Analysis (More than Two Combination of OW, MW, PSA, TA and SA) | Policy Suggestion/Direction | ||
| Colorectal cancer | ||||||||
| Staib et al. [20] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Bleeker et al. [18] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Borie et al. [21] | Yes | No | No (direct only) | Yes | Yes | No (only OW) | Yes | Limited |
| Renehan et al. [24] | Yes | No | Yes | No | Yes | Yes (OW + SA) | Yes | Moderate |
| Macafee et al. [22] | Yes | No | No (direct only) | No | No | No (only SA) | No | Limited |
| Di Cristofaro et al. [19] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Mant et al. [23] | Yes | No | No (direct only) | Yes | Yes | Yes (SA + TA) | No | Limited |
| Breast cancer | ||||||||
| Grogan et al. [26] | Yes | No | No (direct only) | No | No | Not conducted | No | Limited |
| Kokko et al. [27] | No | Na | No (direct only) | No | No | NA | No | Limited |
| Robertson et al. [28] | Yes | No | No (direct only) | Yes | Yes | Yes (OW + MW + TA) | No | Limited |
| Lu et al. [29] | Yes | No | No (direct only) | No | No | Not conducted | No | Limited |
| Bessen et al. [14] | Yes | Yes | No (direct only) | Yes | Yes | Yes (SA + PSA) | No | Moderate |
| Draeger et al. [53] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Skin cancer | ||||||||
| Hengge et al. [30] | Yes | No | No (direct only) | Yes | No | Not conducted | Yes | Limited |
| Leiter et al. [31] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Podlipnik et al. [32] | Yes | No | No (direct only) | No | No | Yes (OW + SA) | No | Limited |
| Cervical cancer | ||||||||
| Forni et al. [33] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Baena-Cañada et al. [34] | No | NA | No (direct only) | Yes | No | NA | No | Limited |
| Auguste et al. [35] | Yes | No | No (direct only) | Yes | Yes | Yes (OW + SA + PSA) | Yes | Moderate |
| Head and neck cancer | ||||||||
| Shah et al. [37] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Meregaglia et al. [38] | Yes | No | No (direct only) | Yes | Yes | Yes (OW + TW + PSA) | No | Limited |
| Hodgkin’s disease | ||||||||
| Dryver et al. [39] | No | NA | No (direct only) | No | No | NA | Yes | Limited |
| Guadagnolo et al. [40] | Yes | No | No (direct only) | Yes | Yes | Yes (OW + SA) | Yes | Moderate |
| Testicular cancer | ||||||||
| Clasen et al. [41] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Charytonowicz et al. [42] | Yes | No | No (direct only) | No | No | No (only OW) | Yes | Limited |
| Others | ||||||||
| Gilbert et al. [43] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Dion et al. [44] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Rettenmaier et al. [45] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Rettenmaier et al. [46] | No | NA | No (direct only) | No | No | NA | No | Limited |
| Imran et al. [47] | No | NA | No (direct only) | No | No | NA | Yes | Limited |
| Dansk et al. [48] | Yes | No | No (direct only) | No | No | No (only SA) | Yes | Limited |
| Pearce et al. [49] | Yes | No | No (direct only) | No | No | Yes (OW + PSA) | Yes | Limited |
| Gao et al. [50] | Yes | No | Yes | Yes | Yes | Yes (OW + PSA) | No | Moderate |
| Ehrhardt et al. [51] | Yes | Yes | Yes | Yes | Yes | Yes (OW + TW) | Yes | Strong |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brain, D.; Jadambaa, A. Economic Evaluation of Long-Term Survivorship Care for Cancer Patients in OECD Countries: A Systematic Review for Decision-Makers. Int. J. Environ. Res. Public Health 2021, 18, 11558. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111558
Brain D, Jadambaa A. Economic Evaluation of Long-Term Survivorship Care for Cancer Patients in OECD Countries: A Systematic Review for Decision-Makers. International Journal of Environmental Research and Public Health. 2021; 18(21):11558. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111558
Chicago/Turabian StyleBrain, David, and Amarzaya Jadambaa. 2021. "Economic Evaluation of Long-Term Survivorship Care for Cancer Patients in OECD Countries: A Systematic Review for Decision-Makers" International Journal of Environmental Research and Public Health 18, no. 21: 11558. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111558