
Age of Onset and Its Related Factors in Cocaine or Methamphetamine Use in Adults from the United States: Results from NHANES 2005–2018


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. NHANES Data Extracted
2.2.1. Drug Use Questionnaire
2.2.2. Demographic Characteristics
2.3. Statistical Analyses
3. Results
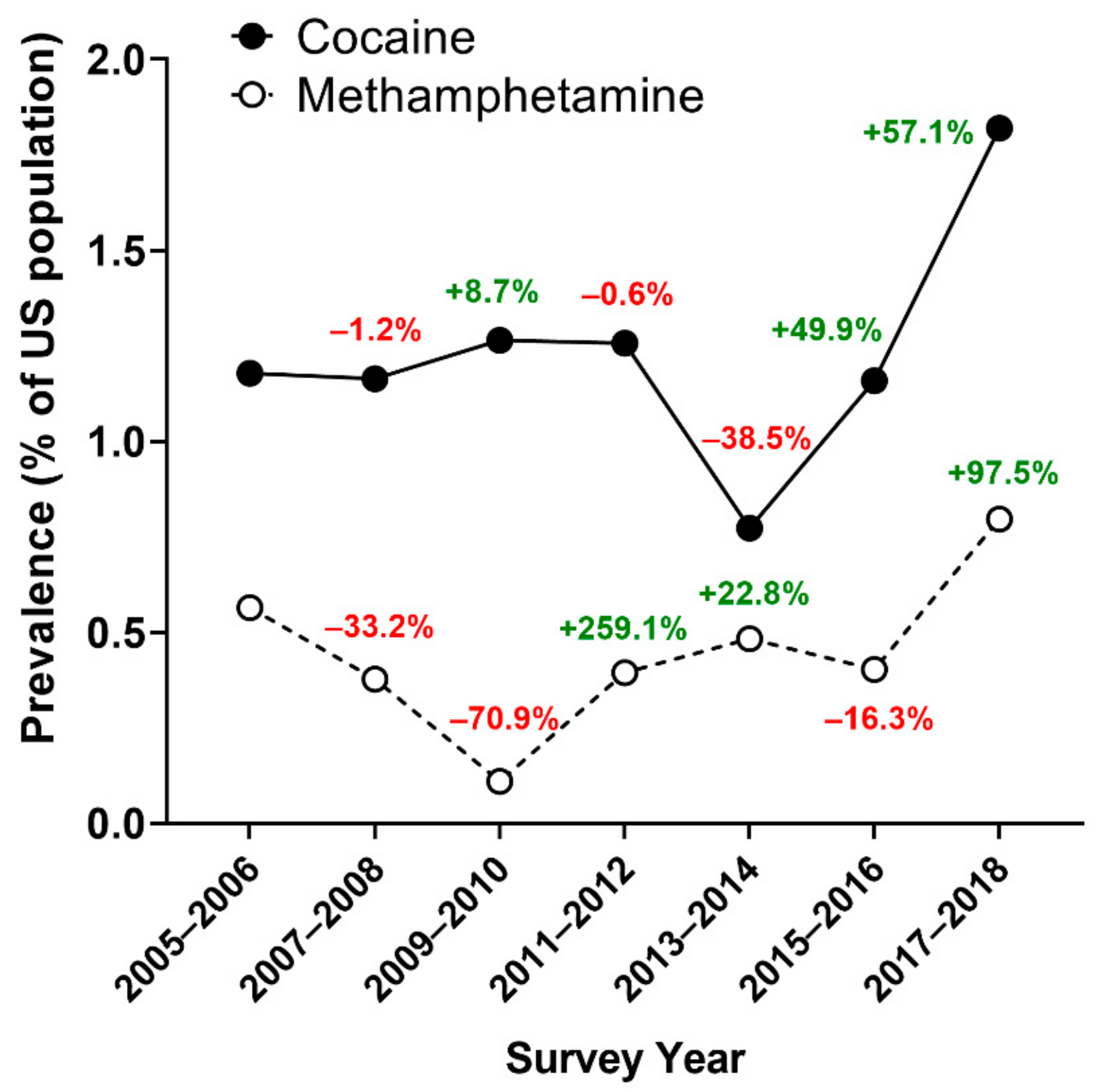
3.1. Prevalence and Frequencies of Past-Month Cocaine or Methamphetamine Use
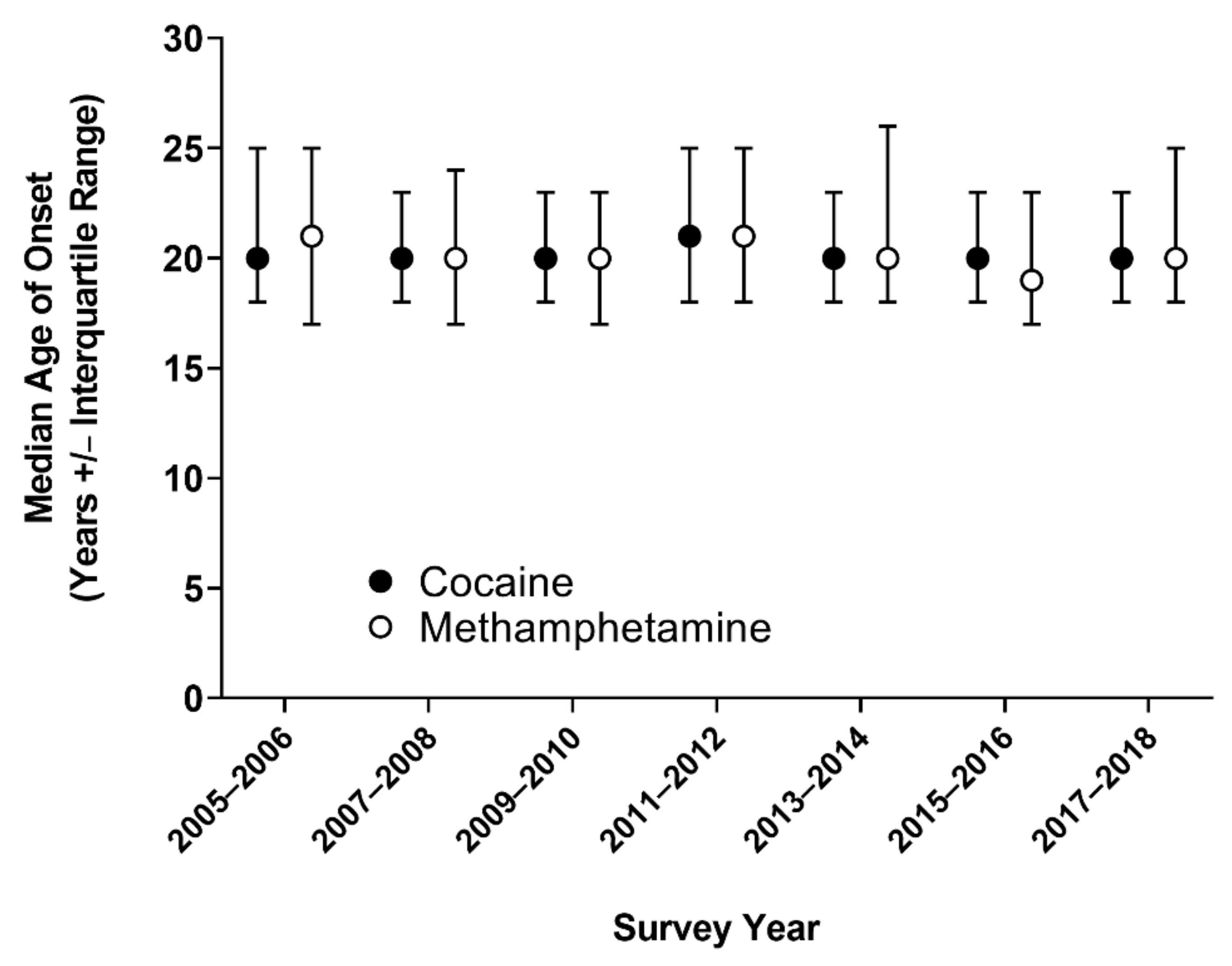
3.2. Trends in Age of Onset of Cocaine and Methamphetamine Use
3.3. Factors Associated with Age of Onset of Cocaine and Methamphetamine Use
3.3.1. Demographic and Other Drug Use Characteristics
3.3.2. Age of Onset of Cocaine Use
3.3.3. Age of Onset of Methamphetamine Use
4. Discussion
4.1. Cocaine and Methamphetamine Use Has Increased from 2005 to 2018
4.2. Factors Associated with Age of Onset of Cocaine or Methamphetamine Use
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNODC. World Drug Report 2021—Executive Summary: Policy Implications; United Nations Publication: Vienna, Austria, 2021; ISBN 9789211483611. [Google Scholar]
- SAMHSA. Results from the 2019 National Survey on Drug Use and Health; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2020. [Google Scholar]
- UNODC. World Drug Report Drug Market Trends: Cocaine Amphetamine-Type Stimulants; United Nations Publication: Vienna, Austria, 2021; ISBN 9789211483611. [Google Scholar]
- Hedegaard, H.; Miniño, A.M.; Warner, M. Drug Overdose Deaths in the United States, 1999–2018. NCHS Data Brief, no 356. Cent. Dis. Contol Prev. 2020, 1–8. [Google Scholar]
- French, M.T.; Maclean, J.C. Underage alcohol use, delinquency, and criminal activity. Health Econ. 2006, 15, 1261–1281. [Google Scholar] [CrossRef]
- Anthony, J.C.; Petronis, K.R. Early-onset drug use and risk of later drug problems. Drug Alcohol Depend. 1995, 40, 9–15. [Google Scholar] [CrossRef]
- Robins, L.N.; Przybeck, T.R. Etiology of drug abuse. Implications for prevention. NIDA Res. Monogr. 1985, 56, 1–283. [Google Scholar]
- Grant, B.F.; Dawson, D.A. Age of onset of drug use and its association with DSM-IV drug abuse and dependence: Results from the national longitudinal alcohol epidemiologic survey. J. Subst. Abus. 1998, 10, 163–173. [Google Scholar] [CrossRef]
- Dawson, D.A.; Goldstein, R.; Chou, S.P.; Ruan, W.J.; Grant, B.F. Age at First Drink and the First Incidence of Adult-Onset DSM-IV Alcohol Use Disorders. Alcohol. Clin. Exp. Res. 2008, 32, 2149–2160. [Google Scholar] [CrossRef] [PubMed]
- King, K.M.; Chassin, L. A Prospective Study of the Effects of Age of Initiation of Alcohol and Drug Use on Young Adult Substance Dependence*. J. Stud. Alcohol Drugs 2007, 68, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Storr, C.L.; Anthony, J.C. Early-onset drug use and risk for drug dependence problems. Addict. Behav. 2009, 34, 319–322. [Google Scholar] [CrossRef] [Green Version]
- Palmer, R.; Young, S.; Hopfer, C.; Corley, R.; Stallings, M.; Crowley, T.; Hewitt, J. Developmental epidemiology of drug use and abuse in adolescence and young adulthood: Evidence of generalized risk. Drug Alcohol Depend. 2009, 102, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Grant, J.D.; Scherrer, J.; Lynskey, M.T.; Lyons, M.; Eisen, S.A.; Tsuang, M.T.; True, W.R.; Bucholz, K.K. Adolescent alcohol use is a risk factor for adult alcohol and drug dependence: Evidence from a twin design. Psychol. Med. 2005, 36, 109–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poudel, A.; Gautam, S. Age of onset of substance use and psychosocial problems among individuals with substance use disorders. BMC Psychiatry 2017, 17, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butelman, E.R.; Chen, C.Y.; Conybeare, R.A.; Brown, K.G.; Fry, R.S.; Kimani, R.; da Rosa, J.C.; Ott, J.; Kreek, M.J. Are trait impulsivity and exposure to cannabis or alcohol associated with the age of trajectory of cocaine use? A gender-specific dimensional analysis in humans with cocaine dependence diagnosis. Exp. Clin. Psychopharmacol. 2020, 28, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Blanco, C.; Flórez-Salamanca, L.; Secades-Villa, R.; Wang, S.; Hasin, D.S. Predictors of initiation of nicotine, alcohol, cannabis, and cocaine use: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Am. J. Addict. 2018, 27, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, C.A.; Obando, D.; Trujillo, A. An examination of the association between early initiation of substance use and interrelated multilevel risk and protective factors among adolescents. PLoS ONE 2019, 14, e0225384. [Google Scholar] [CrossRef] [Green Version]
- Haug, S.; Núñez, C.L.; Becker, J.; Gmel, G.; Schaub, M.P. Predictors of onset of cannabis and other drug use in male young adults: Results from a longitudinal study. BMC Public Health 2014, 14, 1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Human Services; Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey Questionnaire; Department of Health and Human Services: Hyattsville, MD, USA, 2021. Available online: https://www.cdc.gov/nchs/nhanes/ (accessed on 19 November 2021).
- SAMHSA. Results from the 2017 National Survey on Drug Use and Health; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018. [Google Scholar]
- Patrick, M.E.; Wightman, P.; Schoeni, R.F.; Schulenberg, J. Socioeconomic Status and Substance Use Among Young Adults: A Comparison Across Constructs and Drugs. J. Stud. Alcohol Drugs 2012, 73, 772–782. [Google Scholar] [CrossRef] [Green Version]
- Guerin, A.A.; Drummond, K.D.; Bonomo, Y.; Lawrence, A.J.; Rossell, S.L.; Kim, J.H. Assessing methamphetamine-related cue reactivity in people with methamphetamine use disorder relative to controls. Addict. Behav. 2021, 123, 107075. [Google Scholar] [CrossRef] [PubMed]
- Crummy, E.A.; O’Neal, T.J.; Baskin, B.M.; Ferguson, S.M. One Is Not Enough: Understanding and Modeling Polysubstance Use. Front. Neurosci. 2020, 14, 569. [Google Scholar] [CrossRef] [PubMed]
- Zuckermann, A.M.; Williams, G.C.; Battista, K.; Jiang, Y.; de Groh, M.; Leatherdale, S.T. Prevalence and correlates of youth poly-substance use in the COMPASS study. Addict. Behav. 2020, 107, 106400. [Google Scholar] [CrossRef]
- Golub, A.; Bennett, A.S.; Elliott, L. Beyond America’s War on Drugs: Developing Public Policy to Navigate the Prevailing Pharmacological Revolution. AIMS Public Health 2015, 2, 142–160. [Google Scholar] [CrossRef]
- Alcover, K.C.; Thompson, C.L. Patterns of Mean Age at Drug Use Initiation Among Adolescents and Emerging Adults. JAMA Pediatr. 2020, 174, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Schulenberg, J.E.; Patrick, M.E.; Johnston, L.D.; O’Malley, P.M.; Bachman, J.G.; Miech, R.A. Monitoring the Future National Survey Results on Drug Use, 1975–2020: Volume II, College Students and Adults Ages 19–60; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2021. [Google Scholar]
- AIHW. National Drug Strategy Household Survey 2019; Australian Institute of Health and Welfare: Canberra, Australia, 2020. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2021: Trends and Developments; Publications Office of the European Union: Luxemburg, 2021. [Google Scholar]
- Sowell, E.R.; Thompson, P.; Tessner, K.D.; Toga, A.W. Mapping Continued Brain Growth and Gray Matter Density Reduction in Dorsal Frontal Cortex: Inverse Relationships during Postadolescent Brain Maturation. J. Neurosci. 2001, 21, 8819–8829. [Google Scholar] [CrossRef]
- Sowell, E.R.; Thompson, P.; Holmes, C.J.; Jernigan, T.L.; Toga, A.W. In vivo evidence for post-adolescent brain maturation in frontal and striatal regions. Nat. Neurosci. 1999, 2, 859–861. [Google Scholar] [CrossRef]
- Humensky, J. Are adolescents with high socioeconomic status more likely to engage in alcohol and illicit drug use in early adulthood? Subst. Abus. Treat. Prev. Policy 2010, 5, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keeler, T.E.; Hu, T.-W.; Barnett, P.G.; Manning, W.G.; Sung, H.-Y. Do cigarette producers price-discriminate by state? An empirical analysis of local cigarette pricing and taxation. J. Health Econ. 1996, 15, 499–512. [Google Scholar] [CrossRef]
- Farrell, S.; Manning, W.G.; Finch, M.D. Alcohol dependence and the price of alcoholic beverages. J. Health Econ. 2003, 22, 117–147. [Google Scholar] [CrossRef]
- Yang, L.H.; Wong, L.Y.; Grivel, M.M.; Hasin, D.S. Stigma and substance use disorders. Curr. Opin. Psychiatry 2017, 30, 378–388. [Google Scholar] [CrossRef]
- Tsai, A.C.; Kiang, M.V.; Barnett, M.L.; Beletsky, L.; Keyes, K.M.; McGinty, E.E.; Smith, L.R.; Strathdee, S.A.; Wakeman, S.E.; Venkataramani, A.S. Stigma as a fundamental hindrance to the United States opioid overdose crisis response. PLoS Med. 2019, 16, e1002969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, P.; Harney, A.; Lee, N.K.; Pennay, A. Treatment utilization and barriers to treatment: Results of a survey of dependent methamphetamine users. Subst. Abus. Treat. Prev. Policy 2011, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Cruickshank, C.C.; Dyer, K. A review of the clinical pharmacology of methamphetamine. Addiction 2009, 104, 1085–1099. [Google Scholar] [CrossRef]
- Coe, M.A.; Phipps, R.A.J.; Cone, E.J.; Walsh, S.L. Bioavailability and Pharmacokinetics of Oral Cocaine in Humans. J. Anal. Toxicol. 2018, 42, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Thurstone, C.; Salomonsen-Sautel, S.; Mikulich-Gilbertson, S.K.; Hartman, C.A.; Sakai, J.T.; Hoffenberg, A.S.; McQueen, M.B.; Min, S.-J.; Crowley, T.J.; Corley, R.P.; et al. Prevalence and predictors of injection drug use and risky sexual behaviors among adolescents in substance treatment. Am. J. Addict. 2013, 22, 558–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, A.; Darke, S.; Ross, J.; Teesson, M. The effect of persistence of cocaine use on 12-month outcomes for the treatment of heroin dependence. Drug Alcohol Depend. 2006, 81, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Staiger, P.K.; Long, C.M.; Carr, V.; Marlatt, G.A.; Richardson, B. Overlooked and underestimated? Problematic alcohol use in clients recovering from drug dependence. Addiction 2012, 108, 1188–1193. [Google Scholar] [CrossRef] [Green Version]
- Dillon, F.R.; Turner, C.W.; Robbins, M.S.; Szapocznik, J. Concordance among biological, interview, and self-report measures of drug use among African American and Hispanic adolescents referred for drug abuse treatment. Psychol. Addict. Behav. 2005, 19, 404–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napper, L.E.; Fisher, D.G.; Johnson, M.E.; Wood, M.M. The reliability and validity of drug users’ self reports of amphetamine use among primarily heroin and cocaine users. Addict. Behav. 2010, 35, 350–354. [Google Scholar] [CrossRef] [Green Version]
- Kjellsson, G.; Clarke, P.; Gerdtham, U.-G. Forgetting to remember or remembering to forget: A study of the recall period length in health care survey questions. J. Health Econ. 2014, 35, 34–46. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Survey Year | Cocaine—n | Methamphetamine—n |
|---|---|---|
| 2005–2006 | 2,218,308 | 1,062,015 |
| 2007–2008 | 2,364,077 | 765,305 |
| 2009–2010 | 2,620,742 | 227,261 |
| 2011–2012 | 2,651,675 | 830,829 |
| 2013–2014 | 1,653,094 | 1,033,882 |
| 2015–2016 | 2,513,407 | 874,046 |
| 2017–2018 | 3,969,027 | 1,735,796 |
| Cocaine (n = 3975) | Methamphetamine (n = 1606) | |
|---|---|---|
| Average age—years (±SD) | 40.33 (±11.41) | 40.50 (±10.88) |
| Sex—no. (%) | ||
| Male | 2494 (62.7) | 1026 (63.9) |
| Female | 1481 (37.3) | 580 (36.1) |
| Average age of onset of use—years (±SD) | 21.62 (±5.77) | 22.25 (±6.98) |
| Other drug use—no. (%) | ||
| Regular tobacco use | 1871 (47.1) | 815 (50.7) |
| Regular cannabis use | 1869 (47.0) | 846 (52.7) |
| Lifetime heroin use | 548 (13.8) | 301 (18.7) |
| Lifetime cocaine use | 3975 (100) | 1469 (91.5) |
| Lifetime methamphetamine use | 1469 (37.0) | 1606 (100) |
| Lifetime IV use—no. (%) | 472 (11.9) | 332 (20.7) |
| B | 95% CI for B | se B | β | R2 | ΔR2 | ||
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Block 1 | 0.094 | 0.093 ** | |||||
| Constant | 16.663 | 15.013 | 18.313 | 0.841 | |||
| Survey Cycle | −0.217 | −0.392 | −0.041 | 0.089 | −0.054 * | ||
| Age | 0.155 | 0.132 | 0.177 | 0.011 | 0.304 ** | ||
| Block 2 | 0.156 | 0.151 ** | |||||
| Constant | 18.327 | 16.253 | 20.401 | 1.057 | |||
| Survey Cycle | −0.119 | −0.290 | 0.052 | 0.087 | −0.030 | ||
| Age | 0.159 | 0.137 | 0.181 | 0.011 | 0.312 ** | ||
| Sex (ref = male) | −0.239 | −0.746 | 0.268 | 0.258 | −0.020 | ||
| Education (ref = less than 9th grade) | −0.018 | −0.269 | 0.233 | 0.128 | −0.003 | ||
| Income (ref = $0 to $4999) | −0.117 | −0.176 | −0.057 | 0.030 | −0.091 ** | ||
| Regular Tobacco Use (ref = no regular use) | 0.889 | 0.364 | 1.415 | 0.268 | 0.076 ** | ||
| Regular Cannabis Use (ref = no regular use) | −1.159 | −1.684 | −0.634 | 0.268 | −0.095 ** | ||
| Lifetime Heroin Use (ref = no lifetime use) | −0.543 | −1.162 | 0.077 | 0.316 | −0.041 | ||
| Lifetime Methamphetamine Use (ref = no lifetime use) | −1.540 | −2.043 | −1.038 | 0.256 | −0.134 ** | ||
| Lifetime IV Use (ref = no lifetime use) | −1.386 | −2.162 | −0.610 | 0.396 | −0.086 ** | ||
| B | 95% CI for B | se B | β | R2 | ΔR2 | ||
|---|---|---|---|---|---|---|---|
| LL | UL | ||||||
| Block 1 | 0.089 | 0.087 *** | |||||
| Constant | 12.331 | 9.258 | 15.404 | 1.566 | |||
| Survey Cycle Year | 0.263 | −0.062 | 0.588 | 0.165 | 0.053 | ||
| Age | 0.193 | 0.150 | 0.236 | 0.022 | 0.291 *** | ||
| Block 2 | 0.147 | 0.136 *** | |||||
| Constant | 12.834 | 8.297 | 17.371 | 2.311 | |||
| Survey Cycle | 0.341 | 0.022 | 0.659 | 0.162 | 0.068 * | ||
| Age | 0.215 | 0.172 | 0.258 | 0.022 | 0.323 *** | ||
| Sex (ref = male) | −0.239 | −0.746 | 0.268 | 0.258 | −0.020 | ||
| Education (ref = less than 9th grade) | 0.070 | −0.418 | 0.559 | 0.249 | 0.010 | ||
| Income (ref = $0 to $4999) | −0.220 | −0.333 | −0.107 | 0.058 | −0.133 *** | ||
| Regular Tobacco Use (ref = no regular use) | 1.919 | 0.950 | 2.888 | 0.494 | 0.132 *** | ||
| Regular Cannabis Use (ref = no regular use) | −1.311 | −2.263 | −0.360 | 0.485 | −0.090 ** | ||
| Lifetime Heroin Use (ref = no lifetime use) | 1.124 | −0.126 | 2.374 | 0.637 | 0.066 | ||
| Lifetime Cocaine Use (ref = no lifetime use) | 0.835 | −1.017 | 2.687 | 0.944 | 0.029 | ||
| Lifetime IV Use (ref = no lifetime use) | −1.614 | −2.875 | −0.353 | 0.642 | −0.095 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerin, A.A.; Kim, J.H. Age of Onset and Its Related Factors in Cocaine or Methamphetamine Use in Adults from the United States: Results from NHANES 2005–2018. Int. J. Environ. Res. Public Health 2021, 18, 12259. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212259
Guerin AA, Kim JH. Age of Onset and Its Related Factors in Cocaine or Methamphetamine Use in Adults from the United States: Results from NHANES 2005–2018. International Journal of Environmental Research and Public Health. 2021; 18(22):12259. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212259
Chicago/Turabian StyleGuerin, Alexandre Arthur, and Jee Hyun Kim. 2021. "Age of Onset and Its Related Factors in Cocaine or Methamphetamine Use in Adults from the United States: Results from NHANES 2005–2018" International Journal of Environmental Research and Public Health 18, no. 22: 12259. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212259