
Effects of Endurance Training Intensity on Pulmonary Diffusing Capacity at Rest and after Maximal Aerobic Exercise in Young Athletes


 , , , ,
, , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
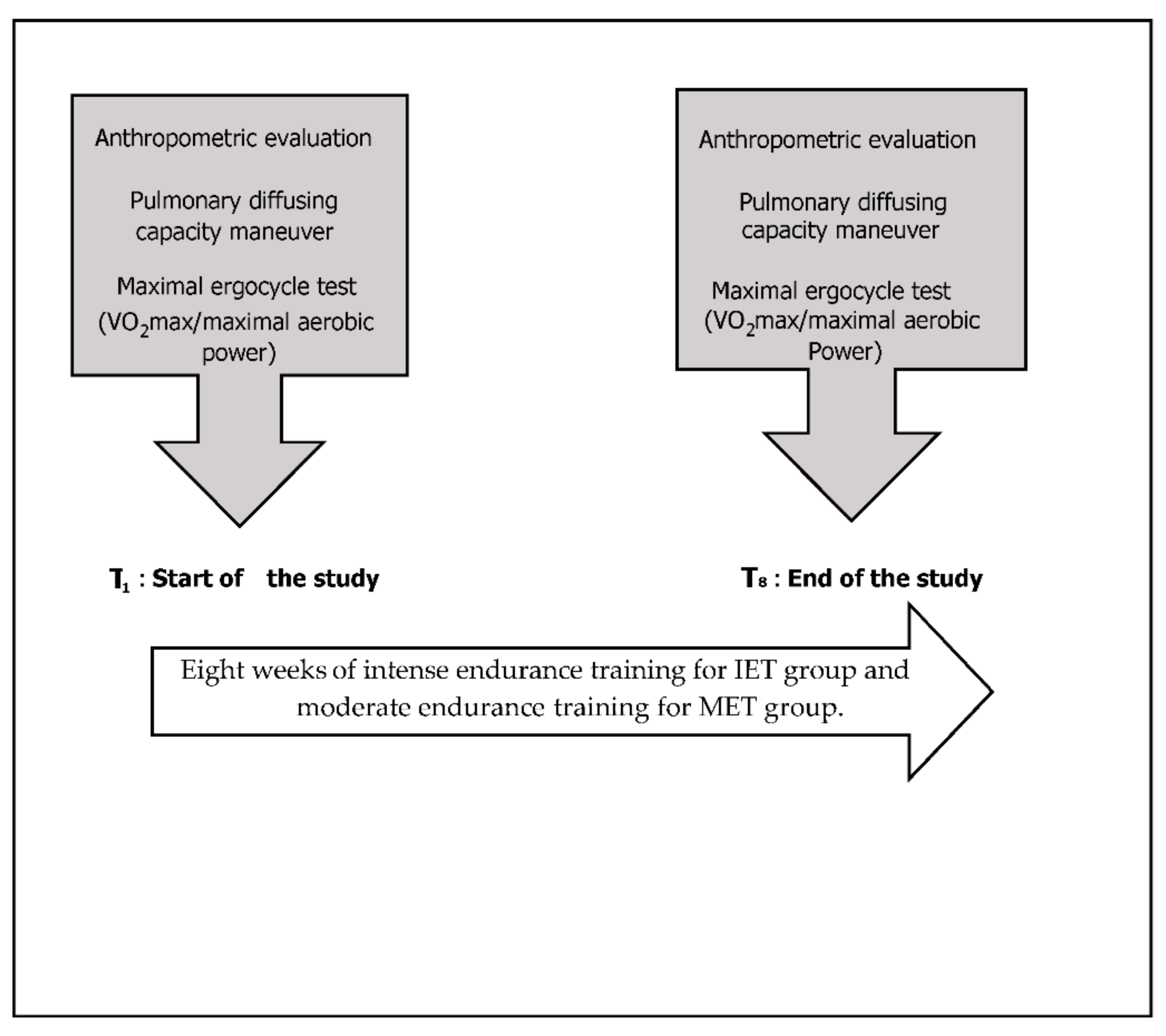
2.2. Procedures
2.3. Exercise Training Program
2.4. Statistical Analyses
3. Results
3.1. Time-Related Effects
3.1.1. At Rest
3.1.2. After Maximal Exercise
3.2. Group Effects
3.2.1. At Rest
3.2.2. After Maximal Exercise
3.3. Group × Time Interactions
3.3.1. At Rest
3.3.2. After Maximal Exercise
4. Discussion
4.1. Effects of Endurance Training on Performance
4.2. Effects of Endurance Training on Lung Function
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, B.J.; Carlson, A.R.; Miller, A.D.; Johnson, B.D. Exercise-induced interstitial pulmonary edema at sea-level in young and old healthy humans. Respir. Physiol. Neurobiol. 2014, 191, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Owens, G.R.; Rogers, R.M.; Pennock, B.E.; Levin, D. The Diffusing Capacity as a Predictor of Arterial Oxygen Desaturation during Exercise in Patients with Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 1984, 310, 1218–1221. [Google Scholar] [CrossRef]
- Brunelli, A.; Xiumeé, F.; Refai, M.; Salati, M.; Marasco, R.; Sciarra, V.; Sabbatini, A. Evaluation of Expiratory Volume, Diffusion Capacity, and Exercise Tolerance Following Major Lung Resection: A Prospective Follow Up Analysis. Chest 2007, 131, 141–147. [Google Scholar] [CrossRef]
- Flaherty, J.M.; Smoliga, J.M.; Zavorsky, G.S. The effect of increased physical activity on pulmonary diffusing capacity in unfit women. Exp. Physiol. 2014, 99, 562–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandigout, S.; Lecoq, A.M.; Courteix, D.; Guenon, P.; Obert, P. Effect of gender in response to an aerobic training pro-gramme in prepubertal children. Acta Paediatr. 2001, 90, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Tedjasaputra, V.; Melissa, M.; Bouwsema, M.M.; Stickland, M.K. Effect of aerobic fitness on capillary blood volume and dif-fusing membrane capacity responses to exercise. J. Physiol. 2016, 594, 4359–4370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manier, G.; Moinard, J.; Stoicheff, H. Pulmonary diffusing capacity after maximal exercise. J. Appl. Physiol. 1993, 75, 2580–2585. [Google Scholar] [CrossRef]
- Zavorsky, G.S.; Quiron, K.B.; Massarelli, P.S.; Lands, L.C. The Relationship between Single-Breath Diffusion Capacity of the Lung for Nitric Oxide and Carbon Monoxide during Various Exercise Intensities. Chest 2004, 125, 1019–1027. [Google Scholar] [CrossRef] [Green Version]
- Nourry, C.; Deruelle, F.; Guinhouya, C.; Baquet, G.; Fabre, C.; Bart, F.; Berthoin, S.; Mucci, P. High-intensity intermittent running training improves pulmonary function and alters exercise breathing pattern in children. Graefe Arch. Clin. Exp. Ophthalmol. 2005, 94, 415–423. [Google Scholar] [CrossRef]
- Paterson, D.H. Respiratory and cardiovascular aspects of intermittent exercise with regard to ice hockey. Can. J. Appl. Sport Sci. 1979, 4, 22–28. [Google Scholar]
- Dridi, R.; Glenet, S.; Tabka, Z.; Amri, M.; Guénard, H. Effects of a Basketball Activity on Lung Capillary Blood Volume and Membrane Diffusing Capacity, Measured by NO/CO Transfer in Children. J. Sports Sci. Med. 2006, 5, 431–439. [Google Scholar]
- Kaufmann, D.A.; Swenson, E.W. Pulmonary changes during marathon training: A longitudinal study. Respiration 1981, 41, 217–223. [Google Scholar] [CrossRef]
- Stickland, M.K.; Welsh, R.C.; Petersen, S.R.; Tyberg, J.V.; Anderson, W.D.; Jones, R.L.; Taylor, D.A.; Bouffard, M.; Haykowsky, M.J. Does fitness level modulate the cardiovascular hemodynamic response to exercise? J. Appl. Physiol. 2006, 100, 1895–1901. [Google Scholar] [CrossRef] [Green Version]
- De Bisschop, C.; Martinot, J.B.; Leurquin-Sterk, G.; Faoro, V.; Guénard, H.; Naeije, R. Improvement in lung diffusion by en-dothelin A receptor blockade at high altitude. J. Appl. Physiol. 2012, 112, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Lavin, K.M.; Straub, A.M.; Uhranowsky, K.A.; Smoliga, J.M.; Zavorsky, G.S. Alveolar-Membrane Diffusing Capacity Limits Performance in Boston Marathon Qualifiers. PLoS ONE 2012, 7, e44513. [Google Scholar] [CrossRef] [Green Version]
- Al Dandachi, G.; Londner, C.; Caumont-Prim, A.; Plantier, L.; Chevalier-Bidaud, B.; Toussaint, J.-F.; Desgorces, F.-D.; Delclaux, C. Ageing and endurance training effects on quantity and quality of pulmonary vascular bed in healthy men. Respir. Res. 2014, 15, 8. [Google Scholar] [CrossRef] [Green Version]
- Dridi, R.; Dridi, N.; Zouita, A.B.M.; Muller, P.; Tabka, Z.; Guénard, H.; Laher, I.; Hackney, A.C.; Zouhal, H. Pulmonary diffusing capacity measured by NO/CO transfer in Tunisian boys. Pediatr. Pulmonol. 2020, 55, 2754–2761. [Google Scholar] [CrossRef] [PubMed]
- Clanton, T.L.; Dixon, G.F.; Drake, J.; Gadek, J.E. Effects of swim training on lung volumes and inspiratory muscle condi-tioning. J. Appl. Physiol. 1987, 62, 39–46. [Google Scholar] [CrossRef]
- Cooper, D.M.; Weiler-Ravell, D. Gas Exchange Response to Exercise in Children1,2. Am. Rev. Respir. Dis. 1984, 129, S47–S48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zavorsky, G.S.; Hsia, C.C.; Hughes, J.M.B.; Borland, C.D.; Guénard, H.; van der Lee, I.; Steenbruggen, I.; Naeije, R.; Cao, J.; Dinh-Xuan, A.T. Standardisation and application of the single-breath determination of nitric oxide uptake in the lung. Eur. Respir. J. 2017, 49, 1600962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guenard, H.; Varene, N.; Vaida, P. Determination of lung capillary blood volume and membrane diffusing capacity in man by the measurements of NO and CO transfer. Respir. Physiol. 1987, 70, 113–120. [Google Scholar] [CrossRef]
- Forster, R.E. Diffusion of Gases across the Alveolar Membrane. In Handbook of Physiology: The Respiratory System IV; American Physiological Society: Bethesda, MD, USA, 1987; pp. 71–88. [Google Scholar]
- Krawiec, J.A.; Forster, R.E.; Gottliebsen, T.W.; Fish, D. Rate of CO uptake by human red blood cells. Fed. Proc. 1983, 42, 993. [Google Scholar]
- Stam, H.; Hrachovina, V.; Stijnen, T.; Versprille, A. Diffusing capacity dependent on lung volume and age in normal subjects. J. Appl. Physiol. 1994, 76, 2356–2363. [Google Scholar] [CrossRef]
- Glénet, S.N.; De Bisschop, C.M.; Dridi, R.; Guénard, H.J. Membrane conductance in trained and untrained subjects using either steady state or single breath measurements of NO transfer. Nitric Oxide 2006, 15, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Tabata, I.; Nishimura, K.; Kouzaki, M.; Hirai, Y.; Ogita, F.; Miyachi, M.; Yamamoto, K. Effects of moderate-intensity endur-ance and high-intensity intermittent training on anaerobic capacity and VO2max. Med. Sci. Sports Exerc. 1996, 10, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Seiler, S.; Jøranson, K.; Olesen, B.V.; Hetlelid, K.J. Adaptations to aerobic interval training: Interactive effects of exercise intensity and total work duration. Scand. J. Med. Sci. Sports 2011, 23, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsia, C.C.W. Signals and mechanisms of compensatory lung growth. J. Appl. Physiol. 2004, 97, 1992–1998. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.; Xia, F.C.; Wagner, P.D.; Breen, E.C. Exercise-induced VEGF transcriptional activation in brain, lung and skeletal muscle. Respir. Physiol. Neurobiol. 2010, 170, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Birukova, A.A.; Moldobaeva, N.; Xing, J.; Birukov, K.G. Magnitude-dependent effects of cyclic stretch on HGF- and VEGF-induced pulmonary endothelial remodeling and barrier regulation. Am. J. Physiol. Cell. Mol. Physiol. 2008, 295, L612–L623. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, B.O.; Koch, G. Effect of Physical Training on Hemodynamic Response during Submaximal and Maximal Exercise in 11–13-Year Old Boys. Acta Physiol. Scand. 1973, 87, 27–39. [Google Scholar] [CrossRef]
- Jones, A.M.; Carter, H. The Effect of Endurance Training on Parameters of Aerobic Fitness. Sports Med. 2000, 29, 373–386. [Google Scholar] [CrossRef]
- Groves, L.; Brade, S.; Wright, S.P. Pushing it to the limit: Enhanced diffusing membrane capacity facilitates greater pulmonary diffusing capacity in athletes during exercise. J. Physiol. 2016, 594, 7171–7172. [Google Scholar] [CrossRef] [PubMed]
- Jarstad, E.; Mamen, A. The performance and aerobic endurance effects of high-intensity versus moderate-intensity continuous running. Appl. Physiol. Nutr. Metab. 2019, 44, 990–996. [Google Scholar] [CrossRef]
- González-Mohíno, F.; González-Ravé, J.M.; Juárez, D.; Fernández, F.A.; Castellanos, R.B.; Newton, R.U. Effects of Continuous and Interval Training on Running Economy, Maximal Aerobic Speed and Gait Kinematics in Recreational Runners. J. Strength Cond. Res. 2016, 30, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Cox, H.M. Exercise training programs and cardiorespiratory adaptation. Clin. Sports Med. 1991, 10, 19–32. [Google Scholar] [CrossRef]
- Reuschlein, P.S.; Reddan, W.G.; Burpee, J.; Gee, J.B.; Rankin, J. Effect of physical training on the pulmonary diffusing capacity during submaximal work. J. Appl. Physiol. 1968, 24, 152–158. [Google Scholar] [CrossRef]
- Hanson, J.S. Physical Training and the Pulmonary Diffusing Capacity. Dis. Chest 1969, 56, 488–493. [Google Scholar] [CrossRef]
- Dempsey, J.A.; Gledhill, N.; Reddan, W.G.; Forster, H.V.; Hanson, P.G.; Claremont, A.D. Pulmonary adaptation to exercise: Effects of exercise type and duration, chronic hypoxia and physical training. Ann. N. Y. Acad. Sci. 1977, 301, 243–261. [Google Scholar] [CrossRef]
- Tsoukias, N.M.; Wilson, A.F.; George, S.C. Effect of alveolar volume and sequential filling on the diffusing capacity of the lungs: I. Theory. Respir. Physiol. 2000, 120, 231–249. [Google Scholar] [CrossRef]
- Hsia, C.C.W.; McBrayer, D.G.; Ramanathan, M. Reference values of pulmonary diffusing capacity during exercise by a re-breathing technique. Am. J. Respir Crit. Care Med. 1995, 152, 658–665. [Google Scholar] [CrossRef]
- Bachofen, H.; Schurch, S.; Urbinelli, M.; Weibel, E.R. Relations among alveolar surface tension, surface area, volume, and recoil pressure. J. Appl. Physiol. 1987, 62, 1878–1887. [Google Scholar] [CrossRef]
- Olfert, I.M.; Balouch, J.; Kleinsasser, A.; Knapp, A.; Wagner, H.; Wagner, P.D.; Hopkins, S.R. Does gender affect human pulmonary gas exchange during exercise? J. Physiol. 2004, 557, 529–541. [Google Scholar] [CrossRef] [Green Version]
- Hsia, C.C.W. Recruitment of lung diffusing capacity: Update of concept and application. Chest 2002, 122, 1774–1783. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, W.A.; Jaryszak, E.M.; Peterson, A.J.; Presson, R.G.; Wagner, W.W. Heterogeneous capillary recruitment among adjoining alveoli. J. Appl. Physiol. 2003, 95, 469–476. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, S.R.; Barker, R.C.; Brutsaert, T.D.; Gavin, T.P.; Entin, P.; Olfert, I.M.; Veisel, S.; Wagner, P.D. Pulmonary gas ex-change during exercise in women: Effects of exercise type and work increment. J. Appl. Phys. 2000, 89, 721–730. [Google Scholar]
- Chang, D.V.; Tiller, C.J.; Kisling, J.A.; Case, J.; Mund, J.A.; Haneline, L.S.; Ingram, D.A.; Tepper, R.S. Membrane and capillary components of lung diffusion and pro-angiogenic cells in infants. Eur. Respir. J. 2013, 43, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Tamhane, R.M.; Johnson, R.L.; Hsia, C.C. Pulmonary Membrane Diffusing Capacity and Capillary Blood Volume Measured During Exercise from Nitric Oxide Uptake. Chest 2001, 120, 1850–1856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coffman, K.; Carlson, A.R.; Miller, A.D.; Johnson, B.D.; Taylor, B.J. The effect of aging and cardiorespiratory fitness on the lung diffusing capacity response to exercise in healthy humans. J. Appl. Physiol. 2017, 122, 1425–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalande, S.; Yerly, P.; Faoro, V.; Naeije, R. Pulmonary vascular distensibility predicts aerobic capacity in healthy individuals. J. Physiol. 2012, 590, 4279–4288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faoro, V.; Deboeck, G.; Vicenzi, M.; Gaston, A.-F.; Simaga, B.; Doucende, G.; Hapkova, I.; Roca, E.; Subirats, E.; Durand, F.; et al. Pulmonary Vascular Function and Aerobic Exercise Capacity at Moderate Altitude. Med. Sci. Sports Exerc. 2017, 49, 2131–2138. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| IET Group (n = 8) | MET Group p-Value (n = 8) | ||
|---|---|---|---|
| Age (years) | 17.0 ± 1.0 | 17.1 ± 0.6 0.76 | |
| Weight (kg) | 64 ± 2 | 65 ± 2 0.46 | |
| Height (cm) | 172 ± 7 | 172 ± 4 1 | |
| VO2max (mL·kg−1 min−1) | 47.2 ± 1.4 | 47.5 ± 1.2 0.67 | |
| Maximum Work Load (w) | 245 ± 30 | 250 ± 37 0.77 | |
| Heart Rate (beats/min) | rest | 63 ± 2 | 64 ± 2 0.35 |
| max | 197 ± 2 | 196 ± 2 0.32 | |
| Intense Endurance Training Group (IET) | Moderate Endurance Training Group (MET) | |
|---|---|---|
| Weeks 1 to 4 | Weekly Training Program | |
| Monday | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: moderate intensity 70–80% of HRmax Active recovery = 2–3 min | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: low intensity (aerobic exercises) ≈60% of HRmax Active recovery = 2–3 min |
| Tuesday | Recovery | Recovery |
| Wednesday | Recovery | Recovery |
| Thursday | Warm-up/Drills: 30 min Running 400 m/600 m/800 m: heavy endurance training 85–95% of HRmax Active recovery = 2–3 min | Warm-up/Drills: 30 minRunning 400 m/600 m/800 m: moderate endurance training 70–80% of HRmaxActive recovery = 2–3 min |
| Friday | Recovery | Recovery |
| Saturday | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: moderate intensity 70–80% of HRmax Active recovery = 2–3 min | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: low to moderate intensity ≈60–70 of HRmax Active recovery = 2–3 min |
| Sunday | Recovery | Recovery |
| Weeks 5 to 8 | Weekly Training Program | |
| Monday | Warm-up/Drills: 30 min Running 400 m/600 m/800 m: moderate to heavy endurance training 70–95% of HRmax | Warm-up/Drills: 30 min Running 400 m/600 m/800 m: low intensity ≈ 60% of HRmax |
| Tuesday | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m): moderate endurance training 70–80% of HRmax Active recovery = 2–3 min | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: low endurance training ≈ 60% of HRmax Active recovery = 2–3 min |
| Wednesday | Recovery | Recovery |
| Thursday | Warm-up/Drills: 30 min Running 800 m/1000 m/1500 m: 85–95% of HRmax Active recovery = 2–3 min | Warm-up/Drills: 30 min Running 800 m/1000 m/1500 m: 70–80% of HRmax Active recovery = 2–3 min |
| Friday | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: moderate to heavy intensity 70–95% of HRmax Active recovery = 2–3 min | Warm-up/Drills: 30 min Running 600 m/800 m/1000 m/1500 m: low intensity ≈ 60% of HRmax Active recovery = 2–3 min |
| Saturday | Recovery | Recovery |
| Sunday | Recovery | Recovery |
| Mean ± SD | p (Paired t Test) | ICC | ICC: CI 95% | CV (%) | ||
|---|---|---|---|---|---|---|
| VI (L) | ||||||
| Rest | 1st trial | 5.18 ± 0.18 | 0.48 | 0.92 | 0.78–0.97 | 1.73 |
| 2nd trial | 5.17 ± 0.15 | |||||
| Exercise | 1st trial | 5.45 ± 0.24 | 0.07 | 0.89 | 0.68–0.96 | 2.65 |
| 2nd trial | 5.38 ± 0.22 | |||||
| VA (L) | ||||||
| Rest | 1st trial | 7.48 ± 0.33 | 0.14 | 0.89 | 0.69–0.96 | 2.63 |
| 2nd trial | 7.40 ± 0.29 | |||||
| Exercise | 1st trial | 7.56 ± 0.35 | 0.69 | 0.96 | 0.89–0.99 | 1.76 |
| 2nd trial | 7.54 ± 0.34 | |||||
| DLNO (mL·min−1·mmHg−1) | ||||||
| Rest | 1st trial | 196.78 ± 1.32 | 0.13 | 0.80 | 0.41–0.93 | 1.62 |
| 2nd trial | 196.29 ± 1.63 | |||||
| Exercise | 1st trial | 256.46 ± 5.97 | 0.08 | 0.91 | 0.75–0.97 | 1.34 |
| 2nd trial | 254.28 ± 6.07 | |||||
| DLCO (mL·min−1·mmHg−1) | ||||||
| Rest | 1st trial | 47.84 ± 0.79 | 0.71 | 0.84 | 0.54–0.94 | 1.23 |
| 2nd trial | 47.46 ± 0.58 | |||||
| Exercise | 1st trial | 53.92 ± 2.41 | 0.92 | 0.94 | 0.83–0.98 | 2.07 |
| 2nd trial | 53.89 ± 2.32 | |||||
| DM (mL·min−1·mmHg−1) | ||||||
| Rest | 1st trial | 97.43 ± 2.84 | 0.56 | 0.96 | 0.86–0.98 | 1.24 |
| 2nd trial | 97.25 ± 3.05 | |||||
| Exercise | 1st trial | 131.35 ± 2.57 | 0.11 | 0.96 | 0.89–0.99 | 0.81 |
| 2nd trial | 130.89 ± 2.96 | |||||
| VC (mL) | ||||||
| Rest | 1st trial | 130.79 ± 6.68 | 0.38 | 0.94 | 0.84–0.98 | 2.38 |
| 2nd trial | 131.50 ± 6.92 | |||||
| Exercise | 1st trial | 159.36 ± 1.24 | 0.87 | 0.82 | 0.48–0.94 | 0.86 |
| 2nd trial | 159.41 ± 2.14 | |||||
| Parameter | IET Group (Mean ± SD) | MET Group (Mean ± SD) | Variance Analysis/Effects | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | Time | Group × Time | ||||||||||
| Pre | Post | ES | Pre | Post | ES | p | ES | p | ES | p | ES | |
| VI (L) | 5.17 ± 0.22 | 5.43 ± 0.32 | 0.94 | 5.26 ± 0.27 | 5.22 ± 0.08 | 0.2 | 0.526 | 0.015 | 0.214 | 0.055 | 0.091 | 0.099 |
| DM (mL/min/mmHg) | 96.06 ± 3.90 | 108.85 ± 3.69 | 3.36 | 99.69 ± 2.87 | 101.84 ± 4.11 | 0.61 | 0.203 | 0.057 | 0.000 | 0.541 | 0.000 | 0.374 |
| TLNO (mL/min/mmHg) | 189.21 ± 3.63 | 213.16 ± 8.98 | 2.72 | 197.08 ± 1.83 | 200.24 ± 2.62 | 1.4 | 0.003 | 0.279 | 0.000 | 0.567 | 0.000 | 0.388 |
| TLCO (mL/min/mmHg) | 46.88 ± 1.46 | 53.43 ± 3.18 | 2.36 | 47.89 ± 3.93 | 47.84 ± 1.23 | 0.02 | 0.000 | 0.411 | 0.000 | 0.407 | 0.000 | 0.404 |
| Vc (mL) | 131.68 ± 10.17 | 150.05 ± 3.39 | 2.42 | 130.96 ± 7.75 | 130.51 ± 14.51 | 0.08 | 0.009 | 0.221 | 0.016 | 0.190 | 0.009 | 0.222 |
| VA (L) | 7.40 ± 0.04 | 7.52 ± 0.15 | 1.09 | 7.46 ± 0.37 | 7.42 ± 0.45 | 0.1 | 0.857 | 0.001 | 0.724 | 0.005 | 0.449 | 0.021 |
| Resting HR (bpm) | 63.5 ± 1.7 | 62 ± 1.8 | 0.84 | 64.5 ± 2.3 | 63.8 ± 0.9 | 0.35 | 0.03 | 0.16 | 0.09 | 0.10 | 0.48 | 0.09 |
| Parameter | IET Group (Mean ± SD) | MET Group (Mean ± SD) | Variance Analysis/Effects | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | Time | Group × Time | ||||||||||
| Pre | Post | ES | Pre | Post | ES | p | ES | p | ES | p | ES | |
| VI (L) | 5.41 ± 0.43 | 5.49 ± 0.22 | 0.23 | 5.36 ± 0.29 | 5.41 ± 0.2 | 0.2 | 0.537 | 0.014 | 0.553 | 0.013 | 0.889 | 0.001 |
| DM (mL/min/mmHg) | 131.3 ± 3.21 | 140.09 ± 1.00 | 3.69 | 131.4 ± 1.96 | 132.56 ± 6.63 | 0.24 | 0.011 | 0.211 | 0.001 | 0.324 | 0.009 | 0.220 |
| TLNO (mL/min/mmHg) | 256.39 ± 8.59 | 276.91 ± 6.59 | 2.68 | 256.54 ± 1.59 | 261.04 ± 7.79 | 8 | 0.003 | 0.281 | 0.000 | 0.498 | 0.002 | 0.289 |
| TLCO (mL/min/mmHg) | 53.71 ± 0.85 | 59.03 ± 0.80 | 6.45 | 54.14 ± 3.41 | 54 ± 5.21 | 0.03 | 0.049 | 0.131 | 0.028 | 0.160 | 0.022 | 0.174 |
| Vc (mL) | 159.09 ± 0.63 | 179.31 ± 7.23 | 3.94 | 159.15 ± 0.58 | 160.48 ± 8.81 | 0.21 | 0.000 | 0.435 | 0.000 | 0.504 | 0.000 | 0.439 |
| VA (L) | 7.49 ± 0.38 | 7.96 ± 0.30 | 1.37 | 7.50 ± 0.27 | 7.53 ± 0.47 | 0.05 | 0.125 | 0.082 | 0.068 | 0.114 | 0.104 | 0.091 |
| HRmax (bpm) | 196.7 ± 2.1 | 189.7 ± 1.2 | 3.1 | 195.7 ± 1.7 | 196.1 ± 2.3 | 0.19 | 0.000 | 0.36 | 0.000 | 0.46 | 0.000 | 0.52 |
| VO2max (mL/kg/min) | 47.2 ± 1.39 | 49.7 ± 0.66 | 2.22 | 47.5 ± 1.23 | 47.7 ± 0.91 | 0.12 | 0.03 | 0.15 | 0.003 | 0.28 | 0.006 | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dridi, R.; Dridi, N.; Govindasamy, K.; Gmada, N.; Aouadi, R.; Guénard, H.; Laher, I.; Saeidi, A.; Suzuki, K.; Hackney, A.C.; et al. Effects of Endurance Training Intensity on Pulmonary Diffusing Capacity at Rest and after Maximal Aerobic Exercise in Young Athletes. Int. J. Environ. Res. Public Health 2021, 18, 12359. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312359
Dridi R, Dridi N, Govindasamy K, Gmada N, Aouadi R, Guénard H, Laher I, Saeidi A, Suzuki K, Hackney AC, et al. Effects of Endurance Training Intensity on Pulmonary Diffusing Capacity at Rest and after Maximal Aerobic Exercise in Young Athletes. International Journal of Environmental Research and Public Health. 2021; 18(23):12359. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312359
Chicago/Turabian StyleDridi, Rim, Nadia Dridi, Karuppasamy Govindasamy, Nabil Gmada, Ridha Aouadi, Hervé Guénard, Ismail Laher, Ayoub Saeidi, Katsuhiko Suzuki, Anthony C. Hackney, and et al. 2021. "Effects of Endurance Training Intensity on Pulmonary Diffusing Capacity at Rest and after Maximal Aerobic Exercise in Young Athletes" International Journal of Environmental Research and Public Health 18, no. 23: 12359. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182312359