
The Association between Exposure to Residential Indoor Volatile Organic Compounds and Measures of Central Arterial Stiffness in Healthy Middle-Aged Men and Women

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Home Stage—24-h Central Ambulatory Monitoring and VOC Measurements
2.3. Clinic Stage—Pulse Wave Velocity and Anthropometric Measurements
2.4. Statistical Analysis
3. Results
3.1. Air Quality and Residential Characteristics
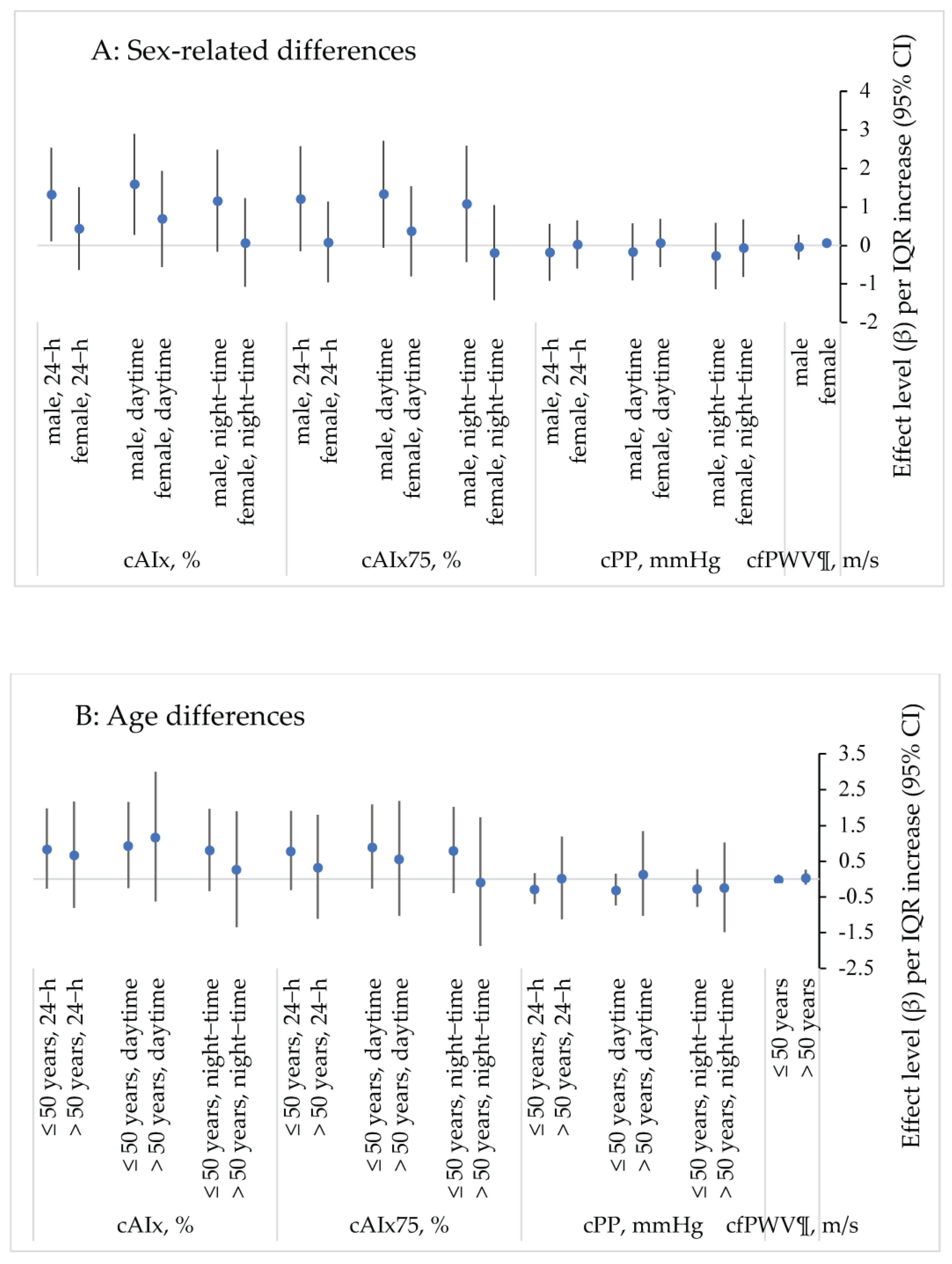
3.2. Associations with Subclinical Measures of Arterial Stiffness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ran, J.; Qiu, H.; Sun, S.; Yang, A.; Tian, L. Are ambient volatile organic compounds environmental stressors for heart failure? Environ. Pollut. 2018, 242, 1810–1816. [Google Scholar] [CrossRef] [PubMed]
- Everson, F.; De Boever, P.; Nawrot, T.S.; Goswami, N.; Mthethwa, M.; Webster, I.; Martens, D.S.; Mashele, N.; Charania, S.; Kamau, F.; et al. Personal NO2 and Volatile Organic Compounds Exposure Levels are Associated with Markers of Cardiovascular Risk in Women in the Cape Town Region of South Africa. Int. J. Environ. Res. Public Health 2019, 16, 2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamopoulos, D.; Vyssoulis, G.; Karpanou, E.; Kyvelou, S.-M.; Argacha, J.-F.; Cokkinos, D.; Stefanadis, C.; Borne, P.V.D. Environmental determinants of blood pressure, arterial stiffness, and central hemodynamics. J. Hypertens. 2010, 28, 903–909. [Google Scholar] [CrossRef]
- Ran, J.; Kioumourtzoglou, M.-A.; Sun, S.; Han, L.; Zhao, S.; Zhu, W.; Li, J.; Tian, L. Source-Specific Volatile Organic Compounds and Emergency Hospital Admissions for Cardiorespiratory Diseases. Int. J. Environ. Res. Public Health 2020, 17, 6210. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.-T. An overview of health hazards of volatile organic compounds regulated as indoor air pollutants. Rev. Environ. Health 2019, 34, 81–89. [Google Scholar] [CrossRef] [PubMed]
- US EPA. Volatile Organic Compound’ Impact of Indoor Air Quality. Available online: https://www.epa.gov/indoor-air-quality-iaq/volatile-organic-compounds-impact-indoor-air-quality (accessed on 16 July 2021).
- Rumchev, K.; Spickett, J.; Bulsara, M.; Phillips, M.; Stick, S. Association of domestic exposure to volatile organic compounds with asthma in young children. Thorax 2004, 59, 746–751. [Google Scholar] [CrossRef] [Green Version]
- The Reference Values for Arterial Stiffness Collaboration, Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: ‘establishing normal and reference values’. Eur. Heart J. 2010, 31, 2338–2350. [CrossRef]
- Mitchell, G.F. Effects of central arterial aging on the structure and function of the peripheral vasculature: Implications for end-organ damage. J. Appl. Physiol. (1985) 2008, 105, 1652–1660. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, G.F.; Guo, C.-Y.; Benjamin, E.J.; Larson, M.G.; Keyes, M.J.; Vita, J.A.; Vasan, R.S.; Levy, D. Cross-sectional correlates of increased aortic stiffness in the community: The Framingham Heart Study. Circulation 2007, 115, 2628–2636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Rourke, M.F.; Hashimoto, J. Mechanical Factors in Arterial Aging. J. Am. Coll. Cardiol. 2007, 50, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Zieman, S.J.; Melenovsky, V.; Kass, D.A. Mechanisms, Pathophysiology, and Therapy of Arterial Stiffness. Arter. Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, G.F.; Parise, H.; Benjamin, E.J.; Larson, M.G.; Keyes, M.J.; Vita, J.A.; Vasan, R.S.; Levy, D. Changes in Arterial Stiffness and Wave Reflection With Advancing Age in Healthy Men and Women: The Framingham Heart Study. Hypertension 2004, 43, 1239–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenters, V.; Uiterwaal, C.S.; Beelen, R.; Bots, M.L.; Fischer, P.; Brunekreef, B.; Hoek, G. Long-Term Exposure to Air Pollution and Vascular Damage in Young Adults. Epidemiology 2010, 21, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, J.; Carter, E.; Schauer, J.J.; Ezzati, M.; Daskalopoulou, S.S.; Valois, M.F.; Shan, M.; Yang, X. Household air pollution and measures of blood pressure, arterial stiffness and central haemodynamics. Heart 2018, 104, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Brasche, S.; Bischof, W. Daily time spent indoors in German homes--baseline data for the assessment of indoor exposure of German occupants. Int. J. Hyg. Environ. Health 2005, 208, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Leech, J.A.; Nelson, W.C.; Burnett, R.T.; Aaron, S.; Raizenne, M.E. It’s about time: A comparison of Canadian and American time-activity patterns. J. Expo. Anal. Environ. Epidemiol. 2002, 12, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Hormigos-Jimenez, S.; Padilla-Marcos, M.A.; Meiss, A.; Gonzalez-Lezcano, R.A.; Feijó-MuÑoz, J. Experimental validation of the age-of-the-air CFD analysis: A case study. Sci. Technol. Built Environ. 2018, 24, 994–1003. [Google Scholar] [CrossRef]
- Gilbey, S.E.; Reid, C.M.; Huxley, R.R.; Soares, M.J.; Zhao, Y.; Rumchev, K. Associations Between Sub-Clinical Markers of Cardiometabolic Risk and Exposure to Residential Indoor Air Pollutants in Healthy Adults in Perth, Western Australia: A Study Protocol. Int. J. Environ. Res. Public Health 2019, 16, 3548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, E.; Parati, G.; Stergiou, G.; Asmar, R.; Beilin, L.; Bilo, G.; Clement, D.; de la Sierra, A.; de Leeuw, P.; Dolan, E.; et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J. Hypertens. 2013, 31, 1731–1768. [Google Scholar] [CrossRef] [Green Version]
- Parati, G.; Stergiou, G.; O’Brien, E.; Asmar, R.; Beilin, L.; Bilo, G.; Clement, D.; de la Sierra, A.; de Leeuw, P.; Dolan, E.; et al. European Society of Hypertension practice guidelines for ambulatory blood pressure monitoring. J. Hypertens. 2014, 32, 1359–1366. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Rangel, A.; Sharpe, T.; Musau, F.; McGill, G. Field evaluation of a low-cost indoor air quality monitor to quantify exposure to pollutants in residential environments. J. Sens. Sens. Syst. 2018, 7, 373–388. [Google Scholar] [CrossRef] [Green Version]
- Rumchev, K.B.; Spickett, J.T.; Bulsara, M.K.; Phillips, M.R.; Stick, S.M. Domestic exposure to formaldehyde significantly increases the risk of asthma in young children. Eur. Respir. J. 2002, 20, 403–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, R.R.; Wilkinson, B.I.; Schiffrin, L.E.; Avolio, P.A.; Chirinos, A.J.; Cockcroft, R.J.; Heffernan, S.K.; Lakatta, G.E.; McEniery, M.C.; Mitchell, F.G.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butlin, M.; Qasem, A. Large Artery Stiffness Assessment Using SphygmoCor Technology. Pulse (Basel) 2017, 4, 180–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljungman, P.L.S.; Li, W.; Rice, M.B.; Wilker, E.H.; Schwartz, J.; Gold, D.R.; Koutrakis, P.; Benjamin, E.J.; Vasan, R.S.; Mitchell, G.F.; et al. Long- and short-term air pollution exposure and measures of arterial stiffness in the Framingham Heart Study. Environ. Int. 2018, 121, 139–147. [Google Scholar] [CrossRef]
- Scheers, H.; Nawrot, T.S.; Nemery, B.; Casas, L. Changing places to study short-term effects of air pollution on cardiovascular health: A panel study. Environ. Health Glob. Access Sci. Source 2018, 17, 80. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Vlachopoulos, C.; Aznaouridis, K.; O’Rourke, M.F.; Safar, M.E.; Baou, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: A systematic review and meta-analysis. Eur. Heart J. 2010, 31, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, H.; Yamashina, A. Non-Invasive Vascular Function Tests: Their Pathophysiological Background and Clinical Application. Circ. J. 2010, 74, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Zanoli, L.; Lentini, P.; Granata, A.; Gaudio, A.; Fatuzzo, P.; Serafino, L.; Rastelli, S.; Fiore, V.; D’Anca, A.; Signorelli, S.S.; et al. A systematic review of arterial stiffness, wave reflection and air pollution. Mol. Med. Rep. 2017, 15, 3425–3429. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N. Type 2 diabetes-related sex differences in cardiovascular risk: Reasons, ramifications, and clinical realities. Eur. Heart J. 2020, 41, 1354–1356. [Google Scholar] [CrossRef]
- Khuseyinova, N.; Schnabel, R.; Ullmann, A.; Zeller, T.; Gori, T.; Espinola-Klein, C.; Lackner, K.; Blankenberg, S.; Munzel, T.; Wild, P. Determinants of arterial stiffness in pre- and postmenopausal women. Eur. Heart J. 2013, 34 (Suppl. 1), P1597. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Arden Pope, C., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.T.; Park, E.K.; Lee, S.G.; Baek, S.H.; Kim, S.H.; Lee, J.H.; Lee, J.W. SAT0145 Increased Carotid Arterial Stiffness in Women with Rheumatoid Arthritis Assessed by Echo-Tracking Ultrasonography. Ann. Rheum. Dis. 2014, 73 (Suppl. 2), 643. [Google Scholar] [CrossRef]
- Petra, C.; Albu, A.; Pamfil, C.; Tămaş, M.; Vesa, Ş.; Rednic, S. The relationship between epicardial adipose tissue and arterial stiffness in patients with rheumatoid arthritis. Med. Ultrason. 2019, 21, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Brook, D.R.; Brook, R.J.; Urch, R.B.; Vincent, R.R.; Rajagopalan, R.S.; Silverman, R.F. Inhalation of Fine Particulate Air Pollution and Ozone Causes Acute Arterial Vasoconstriction in Healthy Adults. Circ. J. Am. Heart Assoc. 2002, 105, 1534–1536. [Google Scholar]
- McEniery, C.; Cockcroft, J. Does Arterial Stiffness Predict Atherosclerotic Coronary Events? Adv. Cardiol. 2007, 44, 160–172. [Google Scholar]
- Münzel, T.; Gori, T.; Al-Kindi, S.; Deanfield, J.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef] [Green Version]
- Kelly, P.R.; Millasseau, C.S.; Ritter, M.J.; Chowienczyk, J.P. Vasoactive Drugs Influence Aortic Augmentation Index Independently of Pulse-Wave Velocity in Healthy Men. Hypertens. J. Am. Heart Assoc. 2001, 37, 1429–1433. [Google Scholar] [CrossRef] [Green Version]
- Curto, A.; Ranzani, O.; Milà, C.; Sanchez, M.; Marshall, J.D.; Kulkarni, B.; Bhogadi, S.; Kinra, S.; Wellenius, G.A.; Tonne, C. Lack of association between particulate air pollution and blood glucose levels and diabetic status in peri-urban India. Environ. Int. 2019, 131, 105033. [Google Scholar] [CrossRef]
- Li, W.; Dorans, K.S.; Wilker, E.H.; Rice, M.B.; Kloog, I.; Schwartz, J.D.; Koutrakis, P.; Coull, B.A.; Gold, D.R.; Meigs, J.B.; et al. Ambient air pollution, adipokines, and glucose homeostasis: The Framingham Heart Study. Environ. Int. 2018, 111, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Mečiarová, Ľ.; Vilčeková, S.; Burdová, E.K.; Kiselák, J. Factors Effecting the Total Volatile Organic Compound (TVOC) Concentrations in Slovak Households. Int. J. Environ. Res. Public Health 2017, 14, 1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, M.; Galbally, I.E.; Molloy, S.B.; Selleck, P.W.; Keywood, M.D.; Lawson, S.J.; Powell, J.C.; Gillett, R.W.; Dunne, E. Factors controlling volatile organic compounds in dwellings in Melbourne, Australia. Indoor Air 2016, 26, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.H.; Jones, P.; Brook, R.; Bard, R.; Oliver, K.; Williams, R. Associations between personal exposures to VOCs and alterations in cardiovascular physiology: Detroit Exposure and Aerosol Research Study (DEARS). Atmos. Environ. 2015, 104, 246–255. [Google Scholar] [CrossRef]


{kind=link}
| Men | Women | |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Demographics | ||
| Age (years) | 50.7 ± 10.7 | 53.2 ± 9.3 |
| n (%) | 39 (35.1) | 72 (64.9) |
| SES, n (%) | ||
| Low | 8 (7.2) | |
| Medium | 15 (13.5) | |
| High | 88 (79.3) | |
| Do you suffer from any chronic conditions? n (%) | ||
| None | 83 (74.8) | |
| Asthma, thyroid etc. | 28 (25.2) | |
| Medications, n (%) | ||
| None | 49 (44.1) | |
| Vitamin supplements | 27 (24.3) | |
| Prescription medication § | 23 (20.7) | |
| Combination of vitamins and prescription § | 12 (10.8) | |
| Physical measurements | ||
| Height (cm) | 178.8 ± 8.6 | 163.2 ± 6.4 |
| Weight (kg) | 82.7 ± 10.8 | 65.0 ± 10.4 |
| BMI (kg/m2) | 25.8 ± 2.8 | 24.4 ± 3.5 |
| Waist measurement (cm) | 92.8 ± 8.7 | 80.0 ± 10.6 |
| Hip–waist ratio | 0.92 ± 0.06 | 0.81 ± 0.06 |
| Male | Female | p-Value | |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| cSBP †, mmHg | |||
| 24-h | 111.8 ± 10.7 | 105.9 ± 8.7 | 0.005 |
| Daytime | 118.0 ± 11.6 | 110.7 ± 8.4 | ≤0.001 |
| Night-time | 101.7 ± 12.3 | 95.9 ± 10.2 | 0.011 |
| Cdbp †, mmHg | |||
| 24-h | 74.5 ± 7.6 | 68.6 ± 6.7 | ≤0.001 |
| Daytime | 79.7 ± 8.1 | 73.8 ± 6.7 | ≤0.001 |
| Night-time | 63.4 ± 9.2 | 58.5 ± 7.6 | 0.003 |
| HR †, bpm | 68.0 ± 8.3 | 72.0 ± 7.0 | 0.016 |
| CAIx †, % | |||
| 24-h | 32.16 ± 9.08 | 41.63 ± 8.03 | ≤0.001 |
| Daytime | 31.11 ± 10.05 | 39.77 ± 9.41 | ≤0.001 |
| Night-time | 34.61 ± 9.23 | 45.34 ± 8.70 | ≤0.001 |
| cAIx75 †, % | |||
| 24-h | 28.34 ± 9.70 | 39.56 ± 7.80 | ≤0.001 |
| Daytime | 29.24 ± 9.79 | 39.69 ± 8.79 | ≤0.001 |
| Night-time | 26.58 ± 10.72 | 39.69 ± 9.47 | ≤0.001 |
| cPP †, mmHg | |||
| 24-h | 38.34 ± 6.18 | 37.07 ± 5.14 | 0.257 |
| Daytime | 38.29 ± 6.59 | 36.94 ± 5.22 | 0.246 |
| Night-time | 38.26 ± 6.29 | 37.46 ± 5.74 | 0.502 |
| cfPWV ‡, m/s | 7.1 ± 1.4 | 6.9 ± 1.1 | 0.081 |
| Mean ± SD | Min–Max | |
|---|---|---|
| Temperature, °C | 23.6 ± 3.0 | 17.0–29.6 |
| RH, % | 49.2 ± 8.2 | 26.6–72.2 |
| VOC, ppb | 406.6 ± 272.0 | 97.6–1888.4 |
| Characteristic | n (%) |
|---|---|
| Type of home | |
| Stand-alone dwelling | 96 (86.5) |
| Group dwelling | 15 (13.5) |
| Age of the home | |
| <10 years | 26 (23.4) |
| >10 years | 83 (74.8) |
| Number of occupants | |
| ≤2 | 43 (38.7) |
| ≥3 | 66 (59.4) |
| Garage attached | |
| Yes | 60 (54.1) |
| No | 49 (44.1) |
| Type of cooking appliances | |
| Gas | 25 (22.5) |
| Electric | 20 (18.0) |
| Both | 63 (56.8) |
| Use of cooking extractor fan | |
| Always/usually | 97 (87.4) |
| Never | 12 (10.9) |
| Distance to a major roadway | |
| ≤300 m | 53 (47.7) |
| ≥300 m | 53 (47.7) |
| Cleaning frequency | |
| Several times per week | 77 (69.4) |
| Irregularly | 31 (27.9) |
| Type of floor coverings | |
| Carpet, linoleum | 29 (26.1) |
| Stone, concrete | 30 (27.0) |
| Wood | 50 (45.0) |
| cAIx, % | cAIx75, % | cPP, mmHg | cfPWV §, m/s | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 24-h | Daytime | Night-Time | 24-h | Daytime | Night-Time | 24-h | Daytime | Night-Time | |||
| Model 1 | β estimate | 0.69 | 0.88 | 0.53 | 0.55 | 0.64 | 0.51 | −0.15 | −0.14 | −0.20 | −0.01 |
| 95% CI | −0.15, 1.53 | −0.04, 1.79 | −0.39, 1.45 | −0.34, 1.43 | −0.27, 1.56 | −0.54, 1.56 | −0.65, 0.36 | −0.66, 0.39 | −0.74, 0.35 | −0.14, 0.11 | |
| p-value | 0.107 | 0.061 | 0.257 | 0.227 | 0.165 | 0.340 | 0.562 | 0.606 | 0.474 | 0.823 | |
| Model 2 | β estimate | 1.04 | 1.23 | 0.91 | 0.90 | 1.01 | 0.87 | −0.17 | −0.17 | −0.21 L33 | 0.04 |
| 95% CI | 0.25, 1.84 | 0.32, 2.14 | 0.08, 1.75 | 0.10, 1.70 | 0.14, 1.89 | −0.05, 1.79 | −0.62, 0.28 | −0.63, 0.29 | −0.73, 0.31 | −0.08, 0.16 | |
| p-value | 0.011 | 0.009 | 0.033 | 0.028 | 0.023 | 0.064 | 0.455 | 0.457 | 0.428 | 0.560 | |
| Model 3 | β estimate | 1.09 | 1.33 | 0.88 | 0.93 | 1.11 | 0.80 | −0.17 | −0.17 | −0.22 | 0.03 |
| 95% CI | 0.29, 1.90 | 0.42, 2.24 | 0.03, 1.72 | 0.12, 1.74 | 0.24, 1.98 | −0.13, 1.73 | −0.63, 0.28 | −0.64, 0.30 | −0.74, 0.31 | −0.09, 0.15 | |
| p-value | 0.008 | 0.005 | 0.042 | 0.025 | 0.013 | 0.090 | 0.454 | 0.472 | 0.417 | 0.593 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilbey, S.E.; Reid, C.M.; Huxley, R.R.; Soares, M.J.; Zhao, Y.; Rumchev, K.B. The Association between Exposure to Residential Indoor Volatile Organic Compounds and Measures of Central Arterial Stiffness in Healthy Middle-Aged Men and Women. Int. J. Environ. Res. Public Health 2022, 19, 981. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020981
Gilbey SE, Reid CM, Huxley RR, Soares MJ, Zhao Y, Rumchev KB. The Association between Exposure to Residential Indoor Volatile Organic Compounds and Measures of Central Arterial Stiffness in Healthy Middle-Aged Men and Women. International Journal of Environmental Research and Public Health. 2022; 19(2):981. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020981
Chicago/Turabian StyleGilbey, Suzanne E., Christopher M. Reid, Rachel R. Huxley, Mario J. Soares, Yun Zhao, and Krassi B. Rumchev. 2022. "The Association between Exposure to Residential Indoor Volatile Organic Compounds and Measures of Central Arterial Stiffness in Healthy Middle-Aged Men and Women" International Journal of Environmental Research and Public Health 19, no. 2: 981. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020981