
Use of Virtual Reality-Based Therapy in Patients with Urinary Incontinence: A Systematic Review with Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selections
- P—Population: adult individuals with urinary incontinence
- Intervention: virtual reality
- C—Comparison: no intervention or all other treatments
- Outcomes:
- ○
- Assessment of muscle function (“maximal contraction”, “Vaginal manometry”, “vaginal dynamometer”, “perineometer”, “electromyography”, “EMG”)
- ○
- Symptoms of UI (“urine loss”, “Pad test”, “bladder diary”)
- ○
- Quality of life (“International Consultation on Incontinence Questionnaire-UI”, “ICIQ-UI SF”, “International Consultation on Incontinence Questionnaire Overactive Bladder”, “ICIQ-OAB”, “International Consultation on Incontinence Questionnaire Overactive Bladder Quality of Life Module”, “ICIQ-OABqol”).
2.3. Outcome Measures
- Maximal voluntary contraction (MVC): The attempt to recruit as many fibers in a muscle as possible for the purpose of developing force. MVC of the pelvic floor can be assessed by vaginal palpation, dynamometers and manometers.
- Pelvic floor manometry/perineometer: Measurement of resting pressure or pressure rise generated during contraction of the PFM using a manometer connected to a sensor, which is inserted into the vagina, rectum or urethra. Pelvic floor manometric tools measure pressure in mmHg, hPa or cmH2O.
- Pelvic floor dynamometry: Measurement of PFM resting and contractile forces using strain gauges mounted on a speculum (a dynamometer), which is inserted into the vagina. Dynamometry measures force in Newton units (N = 1 kg × m/s2).
- EMG Electromyographic diagnosis: Made by evaluating the state of the muscle by recording and analyzing the electrical activity generated by the muscle. Surface electromyography: electrodes placed on the skin of the perineum or inside the urethra, vagina or rectum [14].
- Symptoms of UI (urine loss):
- Bladder diary: includes fluid intake, pad usage, number incontinence episodes, and the degree of incontinence.
- Pad testing: quantification of the amount of urine lost over the duration of testing by measuring the increase in weight of the perineal pads used (weighted pre- and post-testing) [14].
- Quality of life:
- The International Consultation on Incontinence Questionnaire Short Form (ICIQ-SF) is a short, new questionnaire (five questions) proposed by the World Health Organization with the aim of providing a clinically easy-to-use set of modules covering all aspects of the assessment of urinary incontinence severity and its impact on QoL. ICIQ-SF has a maximum score of 21; the higher the score, the more severe is the UI [31].
- The “International Consultation on Incontinence Questionnaire Overactive Bladder” (ICIQ-OAB) is a questionnaire for evaluating overactive bladder and related impact on quality of life (QoL) and outcome of treatment. It consists of 4 questions and an overall score ranging from 0 to 16, with greater values indicating increased symptom severity [32].
- The International Consultation on Incontinence Questionnaire Overactive Bladder Quality of Life Module (ICIQ-OABqol) explores in detail the impact of an overactive bladder on patients’ lives. It consists of 26 questions (overall score ranging from 25 to 160), with greater values indicating increased impact on quality of life [32].
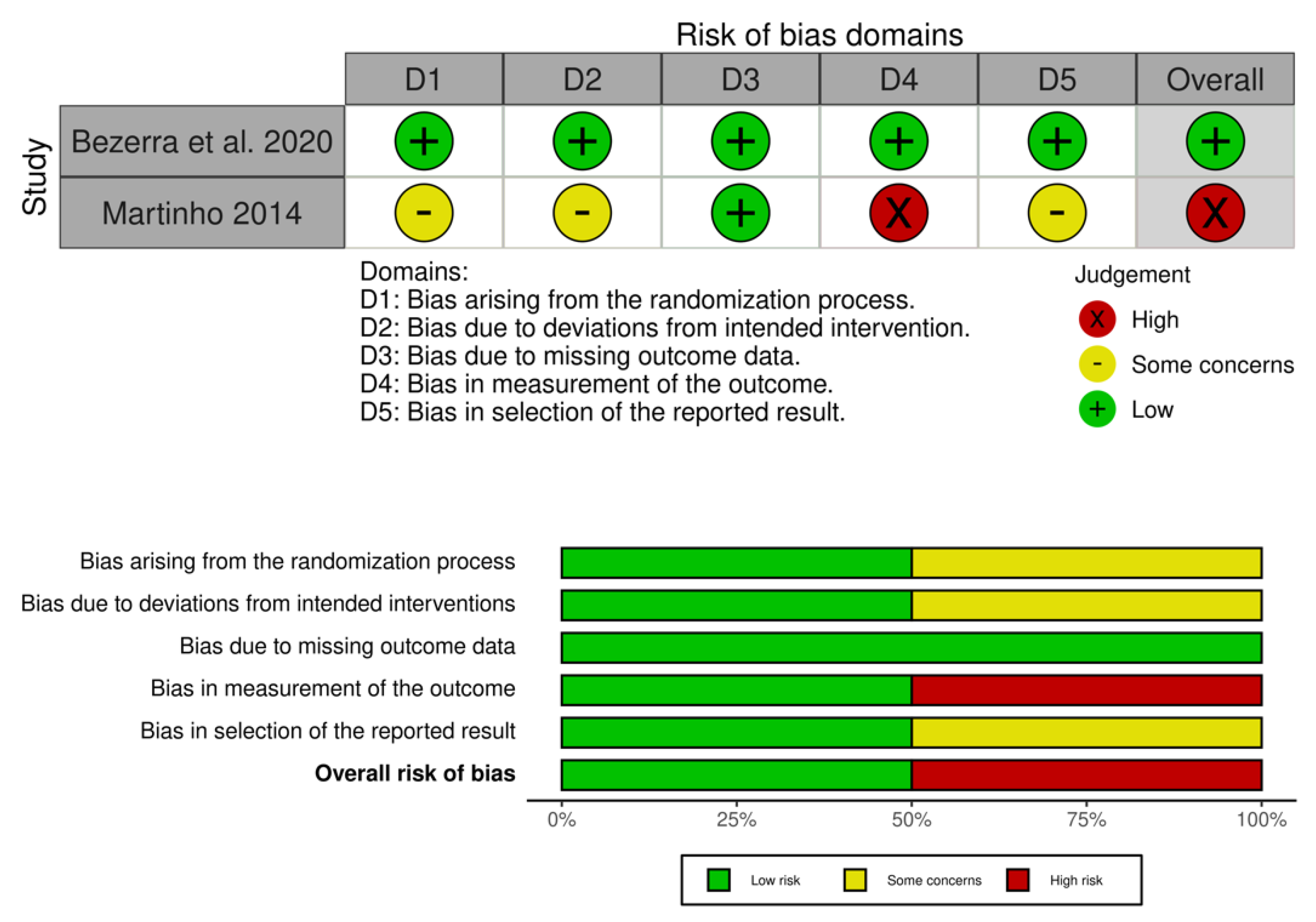
2.4. Assessment of Risk of Bias in Included Studies
2.5. Data Extraction, Management and Synthesis
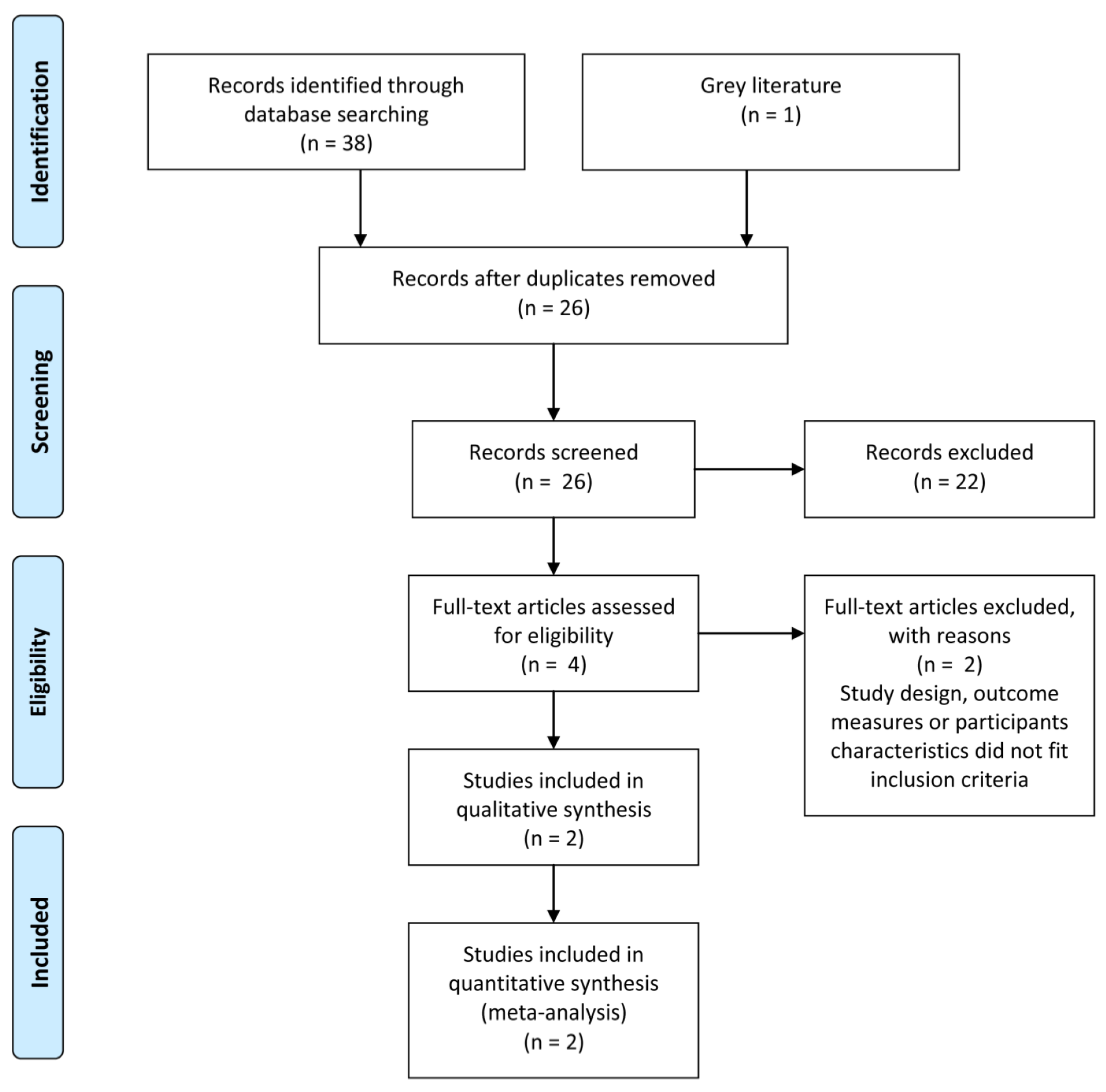
3. Results
3.1. Included Studies
3.2. Excluded Studies
3.3. Methodological Quality
3.4. Effects of Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrams, P.; Andersson, K.E.; Apostolidis, A.; Birder, L.; Bliss, D.; Brubaker, L.; Cardozo, L.; Castro-Diaz, D.; O’Connell, P.R.; Cottenden, A.; et al. 6th International Consultation on Incontinence. Recommendations of the International Scientific Committee: Evaluation and Treatment of Urinary Incontinence, Pelvic Organ Prolapse and Faecal Incontinence. Neurourol. Urodyn. 2018, 37, 2271–2272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griebling, T.L. Worldwide Prevalence Estimates of Lower Urinary Tract Symptoms, Overactive Bladder, Urinary Incontinence, and Bladder Outlet Obstruction. Bju Int. 2011, 108, 1138–1139. [Google Scholar] [CrossRef] [PubMed]
- Buckley, B.S.; Lapitan, M.C.M. Prevalence of Urinary Incontinence in Men, Women, and Children-Current Evidence: Findings of the Fourth International Consultation on Incontinence REPLY. Urology 2010, 76, 271. [Google Scholar] [CrossRef]
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint Report on the Terminology for Female Pelvic Floor Dysfunction. Neurourol. Urodyn. 2010, 29, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Dumoulin, C.; Cacciari, L.P.; Hay-Smith, E.J.C. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst. Rev. 2018, 10, CD005654. [Google Scholar] [CrossRef]
- Tran, L.T.; Puckett, Y. Urinary Incontinence; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Stewart, W.F.; Hirsh, A.G.; Kirchner, H.L.; Clarke, D.N.; Litchtenfeld, M.J.; Minassian, V.A. Urinary Incontinence Incidence: Quantitative Meta-Analysis of Factors that Explain Variation. J. Urol. 2014, 191, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.M.; Hundley, A.F.; Fulton, R.G.; Myers, E.R. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obs. Gynecol. 2009, 114, 1278–1283. [Google Scholar] [CrossRef]
- Siddiqui, N.Y.; Levin, P.J.; Phadtare, A.; Pietrobon, R.; Ammarell, N. Perceptions about female urinary incontinence: A systematic review. Int. Urogynecol. J. 2014, 25, 863–871. [Google Scholar] [CrossRef]
- Radziminska, A.; Straczynska, A.; Weber-Rajek, M.; Styczynska, H.; Strojek, K.; Piekorz, Z. The impact of pelvic floor muscle training on the quality of life of women with urinary incontinence: A systematic literature review. Clin. Interv. Aging 2018, 13, 957–965. [Google Scholar] [CrossRef] [Green Version]
- Preda, A.; Moreira, S. Stress Urinary Incontinence and Female Sexual Dysfunction: The Role of Pelvic Floor Rehabilitation. Acta Med. Port. 2019, 32, 721–726. [Google Scholar] [CrossRef]
- Ostle, Z. Assessment, diagnosis and treatment of urinary incontinence in women. Br. J. Nurs. 2016, 25, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kegel, A.H. Progressive resistance exercise in the functional restoration of the perineal muscles. Am. J. Obs. Gynecol. 1948, 56, 238–248. [Google Scholar] [CrossRef]
- Bo, K.; Frawley, H.C.; Haylen, B.T.; Abramov, Y.; Almeida, F.G.; Berghmans, B.; Bortolini, M.; Dumoulin, C.; Gomes, M.; McClurg, D.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction. Int. Urogynecol. J. 2017, 28, 191–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peschers, U.M.; Vodusek, D.B.; Fanger, G.; Schaer, G.N.; DeLancey, J.O.L.; Schuessler, B. Pelvic muscle activity in nulliparous volunteers. Neurourol. Urodyn. 2001, 20, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Hayes, W. Evidence-Based Physical Therapy for the Pelvic Floor-Bridging Science and Clinical Practice; Cambridge Press: Cambridge, UK, 2008. [Google Scholar]
- Garcia-Sanchez, E.; Avila-Gandia, V.; Lopez-Roman, J.; Martinez-Rodriguez, A.; Rubio-Arias, J.A. What Pelvic Floor Muscle Training Load is Optimal in Minimizing Urine Loss in Women with Stress Urinary Incontinence? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4358. [Google Scholar] [CrossRef] [Green Version]
- Boni, A.; Cochetti, G.; Del Zingaro, M.; Paladini, A.; Turco, M.; Rossi de Vermandois, J.A.; Mearini, E. Uroflow stop test with electromyography: A novel index of urinary continence recovery after RARP. Int. Urol. Nephrol. 2019, 51, 609–615. [Google Scholar] [CrossRef]
- Milios, J.E.; Ackland, T.R.; Green, D.J. Pelvic floor muscle training in radical prostatectomy: A randomized controlled trial of the impacts on pelvic floor muscle function and urinary incontinence. BMC Urol. 2019, 19, 116. [Google Scholar] [CrossRef]
- Rutkowska, A.; Rutkowski, S.; Szczepanska-Gieracha, J. The use of total immersion in the rehabilitation process. Med. Rehabil. 2020, 24, 27–30. [Google Scholar] [CrossRef]
- Jacobson, L. Welcome to the virtual world. In On the Cutting Edge of Technology; Swadley, R., Ed.; Sams Publishing: Carmel, IN, USA, 1993; pp. 69–79. [Google Scholar]
- Kristiansen, L.; Magnussen, L.H.; Wilhelmsen, K.T.; Maeland, S.; Nordahl, S.H.G.; Clendaniel, R.; Hovland, A.; Juul-Kristensen, B. Efficacy of intergrating vestibular rehabilitation and cognitive behaviour therapy in persons with persistent dizziness in primary care- a study protocol for a randomised controlled trial. Trials 2019, 20, 575. [Google Scholar] [CrossRef] [Green Version]
- Rutkowski, S.; Kiper, P.; Cacciante, L.; Cieslik, B.; Mazurek, J.; Turolla, A.; Szczepanska-Gieracha, J. Use of virtual reality-based training in different fields of rehabilitation: A systematic review and meta-analysis. J. Rehabil. Med. 2020, 52, jrm00121. [Google Scholar] [CrossRef]
- Rutkowski, S.; Rutkowska, A.; Jastrzebski, D.; Racheniuk, H.; Pawelczyk, W.; Szczegielniak, J. Effect of Virtual Reality-Based Rehabilitation on Physical Fitness in Patients with Chronic Obstructive Pulmonary Disease. J. Hum. Kinet. 2019, 69, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnechere, B.; Jansen, B.; Omelina, L.; Van Sint Jan, S. The use of commercial video games in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Jastrzebski, D.; Zebrowska, A.; Rutkowski, S.; Rutkowska, A.; Warzecha, J.; Ziaja, B.; Palka, A.; Czyzewska, B.; Czyzewski, D.; Ziora, D. Pulmonary Rehabilitation with a Stabilometric Platform after Thoracic Surgery: A Preliminary Report. J. Hum. Kinet. 2018, 65, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, V.; de Bruin, E.D.; Dumoulin, C. Virtual Reality Rehabilitation as a Treatment Approach for Older Women With Mixed Urinary Incontinence: A Feasibility Study. Neurourol. Urodyn. 2015, 34, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Martinho, N.M.; Silva, V.R.; Marques, J.; Carvalho, L.C.; Iunes, D.H.; Botelho, S. The effects of training by virtual reality or gym ball on pelvic floor muscle strength in postmenopausal women: A randomized controlled trial. Braz. J. Phys. 2016, 20, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ Br. Med. J. 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Hajebrahimi, S.; Corcos, J.; Lemieux, M.C. International consultation on incontinence questionnaire short form: Comparison of physician versus patient completion and immediate and delayed self-administration. Urology 2004, 63, 1076–1078. [Google Scholar] [CrossRef]
- Donovan, J.; Abrams, P.; Peters, T.; Kay, H.; Reynard, J.; Chapple, C.; de la Rosette, J.; Kondo, A. The ICS-‘BPH’ study: The psychometric validity and reliability of the ICSmale questionnaire. BJU 1996, 77, 554–562. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, L.O.; de Oliveira, M.C.E.; da Silva Filho, E.M.; Vicente da Silva, H.K.; Menezes de Oliveira, G.F.; da Silveira Goncalves, A.K.; Pegado, R.; Micussi, M. Impact of Pelvic Floor Muscle Training Isolated and Associated with Game Therapy on Mixed Urinary Incontinence: A Randomized Controlled Trial. Games Health J. 2021, 10, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Martinho, N. O Treinamento Por Meio De Realidade Virtual Melhora A Funcionalidade Dos Músculos Do Assoalho Pélvico De Mulheres Na Pós-Menopausa? 2014. Available online: https://bdtd.unifal-mg.edu.br:8443/bitstream/tede/588/5/Disserta%C3%A7%C3%A3o%20de%20Natalia%20Miguel%20Martinho.pdf (accessed on 10 June 2021).
- Botelho, S.; Martinho, N.M.; Silva, V.R.; Marques, J.; Carvalho, L.C.; Riccetto, C. Virtual reality: A proposal for pelvic floor muscle training. Int. Urogynecol. J. 2015, 26, 1709–1712. [Google Scholar] [CrossRef]
- Oliveira, M.C.E.; Bezerra, L.O.; Melo Angelo, P.H.; de Oliveira, M.C.; Silva-Filho, E.; Ribeiro, T.S.; Pegado, R.; Micussi, M. Game therapy a new approach to treat women facing mixed urinary incontinence: A study protocol. Neurourol. Urodyn. 2020, 39, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Ferreira, M.; Azevedo, M.J.; Firmino-Machado, J.; Santos, P.C. Pelvic floor muscle training protocol for stress urinary incontinence in women: A systematic review. Rev. Assoc. Med. Bras. 2017, 63, 642–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aukee, P.; Immonen, P.; Penttinen, J.; Laippala, P.; Airaksinen, O. Increase in pelvic floor muscle activity after 12 weeks’ training: A randomized prospective pilot study. Urology 2002, 60, 1020–1023. [Google Scholar] [CrossRef]
- Glavind, K.; Nohr, S.B.; Walter, S. Biofeedback and physiotherapy versus physiotherapy alone in the treatment of genuine stress urinary incontinence. Int. Urogynecol. J. Pelvic Floor Dysfunct. 1996, 7, 339–343. [Google Scholar] [CrossRef]
- Urinary Incontinence and Pelvic Organ Prolapse in Women: Management; NICE: London, UK, 2019.
- Dantas, L.O.; Carvalho, C.; Santos, B.L.J.; Ferreira, C.H.J.; Bo, K.; Driusso, P. Mobile health technologies for the management of urinary incontinence: A systematic review of online stores in Brazil. Braz. J. Phys. 2021, 25, 387–395. [Google Scholar] [CrossRef]
- Dufour, S.; Fedorkow, D.; Kun, J.; Deng, S.X.; Fang, Q. Exploring the Impact of a Mobile Health Solution for Postpartum Pelvic Floor Muscle Training: Pilot Randomized Controlled Feasibility Study. JMIR Mhealth Uhealth 2019, 7, e12587. [Google Scholar] [CrossRef]
- Araujo, C.C.; Marques, A.A.; Juliato, C.R.T. The Adherence of Home Pelvic Floor Muscles Training Using a Mobile Device Application for Women with Urinary Incontinence: A Randomized Controlled Trial. Female Pelvic Med. Reconstr. Surg. 2020, 26, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Ong, T.A.; Khong, S.Y.; Ng, K.L.; Ting, J.R.; Kamal, N.; Yeoh, W.S.; Yap, N.Y.; Razack, A.H. Using the Vibrance Kegel Device With Pelvic Floor Muscle Exercise for Stress Urinary Incontinence: A Randomized Controlled Pilot Study. Urology 2015, 86, 487–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczepanska-Gieracha, J.; Cieslik, B.; Rutkowski, S.; Kiper, P.; Turolla, A. What can virtual reality offer to stroke patients? A narrative review of the literature. NeuroRehabilitation 2020, 47, 109–120. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Study design: RCT, quasi RCT, CCT, non-RCT, pilot study, clinical control prospective study | Study design: case report, review, study protocol, case series, clinical trial, feasibility study |
| Population: adults and children with urinary incontinence, stress urinary incontinence, mixed urinary incontinence, urgency urinary incontinence. | Population: patients with schizophrenia, anorexia, autism, depression, cancers, anxiety, neurological disorders, healthy subjects without UI symptoms |
| Intervention: virtual reality immersive and non-immersive interventions | Intervention: robotics, smartphone applications |
| Comparison: all other treatments (non-VR) or no treatments | Lack of control group, equal intervention |
| Outcome: assessment of muscle function, Symptoms of UI, Quality of life | Outcome: all outcomes not related to urinary incontinence |
| Reference | Participants/Age Range (yy) | Type of UI | VR Type | Treatments | Treatment Duration | Outcome Measures | Main Findings |
|---|---|---|---|---|---|---|---|
| Bezerra et al. 2021 [36] | 32 women/45–75 yy | MUI | Wii Fit Plus | PFMT + GT (EG) (n = 16) PFMT (CG) (n = 16) | 8 weeks | Manometry, QoL-ICIQ-SF, 1 h pad-test | PFMT associated with GT did not show better improvements than PFMT isolated in PFM quality of life, pressure and urinary loss. Both interventions proved to be effective for the treatment of women with MUI. |
| Martinho 2014 [37] | 47 women/53–69 yy | MUI | Wii Fit Plus | PFMT + VR (n = 27) PFMT (n = 20) | 5 weeks | ICIQ UI-SF, ICIQ-OAB, Dynamometry, DP | PFMT through virtual reality equates to PFMT through kinesiotherapy regarding the improvement of pelvic floor muscle strength, voiding symptoms, anterior wall prolapse and quality of life, proving to be effective for postmenopausal women. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rutkowska, A.; Salvalaggio, S.; Rutkowski, S.; Turolla, A. Use of Virtual Reality-Based Therapy in Patients with Urinary Incontinence: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106155
Rutkowska A, Salvalaggio S, Rutkowski S, Turolla A. Use of Virtual Reality-Based Therapy in Patients with Urinary Incontinence: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(10):6155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106155
Chicago/Turabian StyleRutkowska, Anna, Silvia Salvalaggio, Sebastian Rutkowski, and Andrea Turolla. 2022. "Use of Virtual Reality-Based Therapy in Patients with Urinary Incontinence: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 10: 6155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106155