Trends and Stabilization up to 2022 in Overweight and Obesity in Switzerland, Comparison to France, UK, US and Australia

Abstract
:1. Introduction
2. Methods and Procedures
3. Results and Discussion
3.1. Observed Prevalence of Overweight and Obesity in Switzerland from 1992 to 2007
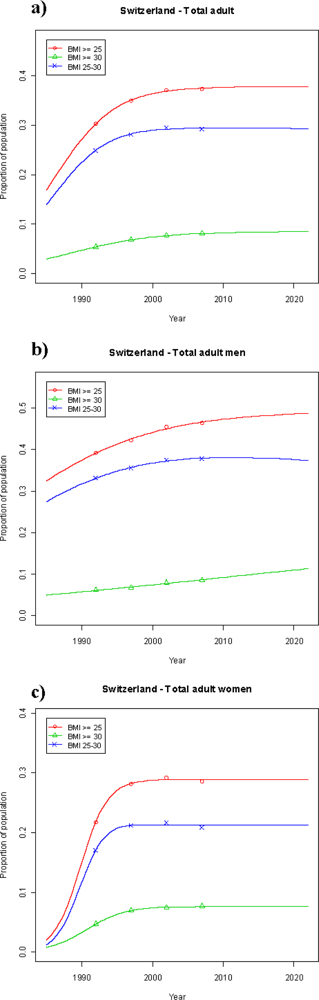
3.2. Projected Prevalence of Overweight and Obesity in Switzerland from 2007 to 2022
3.3. Projected Prevalence of Overweight and Obesity from 2007 to 2022 in Other Countries
4. Discussion
Acknowledgments
References and Notes
- Abelson, P; Kennedy, D. The obesity epidemic. Science 2004, 304, 1413. [Google Scholar]
- Larson, N; Story, M. The adolescent obesity epidemic: why, how long, and what to do about it. Adolesc. Med. State Art Rev 2008, 19, 357–79. [Google Scholar]
- Haslam, D; James, P. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar]
- Guh, DP; Zhang, W; Bansback, N; Amarsi, Z; Birmingham, CL; Anis, AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar]
- Young People’s Health in Context. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2001/2002 Survey; Currie, C; Roberts, C; Morgan, A; Smith, R; Settertobulte, W; Samdal, O; Rasmussen, VB (Eds.) WHO Regional Office for Europe: Copenhagen, Denmark.
- Kosti, RI; Panagiotakos, DB. The epidemic of obesity in children and adolescents in the world. Cent. Eur. J. Public Health 2006, 14, 151–159. [Google Scholar]
- Schmid, A; Schneider, H; Golay, A; Keller, U. Economic burden of obesity and its comorbidities in Switzerland. Soz. Präventivmed 2005, 50, 87–94. [Google Scholar]
- Schweizerische Gesundheitsbefragung 2007. Standardtabellen über Übergewicht, Information received from Galati-Petrecca, M., Bundesamt für Statistik, CH-2010 Neuchâtel, Switzerland, October 2008.
- Sassi, F; Devaux, M; Cecchini, M; Rusticelli, E. The obesity epidemic: Analysis of past and projected future trends in selected OECD countries. OECD Health Working Papers No 45, OECD: F-75775 Paris, CEDEX 16; France, March 2009.
- Eichholzer, M; Lüthy, J; Gutzwiller, F. Epidemiologie des Übergewichts in der Schweiz: Resultate der Schweizerischen Gesundheitsbefragung 1992/93. Schweiz. Med. Wochenschr 1999, 12, 353–361. [Google Scholar]
- Eichholzer, M; Bisig, B; Gutzwiller, F; Lüthy, J. Aktuelle Ernährungsprobleme in der Schweiz. Resultate der Schweizerischen Gesundheitsbefragung 1997. Mitt. Lebensm. Hyg 2000, 91, 251–273. [Google Scholar]
- Fry, J; Finley, W. The prevalence and costs of obesity in the EU. Proc. Nutr. Soc 2005, 64, 359–362. [Google Scholar]
- Haslam, DW; James, WP. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar]
- Ogden, CL; Carroll, MD; Curtin, LR; McDowell, MA; Tabak, CJ; Flegal, KM. Prevalence of overweight and obesity in the United States, 1999−2004. JAMA 2006, 295, 1549–1555. [Google Scholar]
- Hossain, P; Kawar, B; El Nahas, M. Obesity and diabetes in the developing world—a growing challenge. N. Engl. J. Med 2007, 356, 213–215. [Google Scholar]
- Lobstein, T; Millstone, E; PorGrow Research Team. Context for the PorGrow study: Europe’s obesity crisis. Obes. Rev 2007, 8, 7–16. [Google Scholar]
- Wang, Y; Beydoun, M; Caballero, B; Kumanyika, SK. Will all americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity 2008, 16, 2323–2330. [Google Scholar]
- Huang, ES; Basu, A; O’Grady, M; Capretta, JC. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care 2009, 32, 2225–2229. [Google Scholar]
- Homer, J; Milstein, B; Dietz, W. Obesity population dynamics: exploring historical growth and plausible futures in the U.S. In proceeding of 24th International Conference of the System Dynamics Society, Nijmegen, the Netherlands, 2006.
- Cutler, DM; Glaeser, EL; Shapiro, JM. Why have Americans become more obese? J. Econ. Perspect 2003, 17, 93–118. [Google Scholar]
- Hill, JO; Peters, JC. Environmental contributions to the obesity epidemic. Science 1998, 280, 1371–1374. [Google Scholar]
- Christakis, NA; Fowler, JH. The spread of obesity in a large social network over 32 years. N. Engl. J. Med 2007, 357, 370–379. [Google Scholar]
- Marques-Vidal, P; Bochud, M; Mooser, V; Paccaud, F; Waeber, G; Vollenweider, P. Prevalence of obesity and abdominal obesity in the Lausanne population. BMC Public Health 2008, 8, 330. [Google Scholar]
- Helmert, U; Strube, H. The development of obesity in Germany in the period from 1985 until 2000. Gesundheitswesen 2004, 66, 409–415. [Google Scholar]
- Faeh, D; Braun, J; Bopp, M. Underestimation of obesity prevalence in Switzerland: comparison of two methods for correction of self-report. Swiss Med. Wkly 2009, 139, 752–756. [Google Scholar]



{kind=link}
{kind=link}
| Nat. survey | Total adult population (age > 15) | Overweight & obesity BMI ≥ 25 | Overweight BMI 25 – 29.9 | Obesity BMI ≥ 30 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | male | total | female | male | total | female | male | total | female | male | total | |
| total number | total number | total number | % | % | % | % | % | % | % | % | % | |
| 1992/93 | 2 947 789 | 2 735 471 | 5 683 260 | 21.8 | 39.2 | 30.3 | 17.1 | 33.1 | 24.9 | 4.7 | 6.1 | 5.4 |
| 1997 | 3 052 211 | 2 827 975 | 5 880 186 | 28.2 | 42.2 | 34.9 | 21.2 | 35.5 | 28.1 | 7.0 | 6.7 | 6.8 |
| 2002 | 3 108 453 | 2 909 185 | 6 017 638 | 29.3 | 45.4 | 37.1 | 21.8 | 37.5 | 29.4 | 7.5 | 7.9 | 7.7 |
| 2007 | 3 164 763 | 3 021 948 | 6 186 711 | 28.6 | 46.4 | 37.3 | 20.9 | 37.8 | 29.2 | 7.7 | 8.6 | 8.1 |
| Total population (age 15–24) | Overweight & obesity BMI ≥ 25 | Overweight BMI 25 – 29.9 | Obesity BMI ≥ 30 | |||||||||
| female | male | total | female | male | total | female | male | total | female | male | total | |
| total number | total number | total number | % | % | % | % | % | % | % | % | % | |
| 1992/93 | 423 107 | 432 646 | 855 752 | 6.8 | 12.9 | 9.8 | 6.1 | 11.8 | 8.9 | 0.7 | 1.1 | 0.9 |
| 1997 | 400 874 | 406 866 | 807 739 | 9.4 | 11.9 | 10.5 | 8.4 | 10.8 | 9.6 | 0.8 | 1.1 | 0.9 |
| 2002 | 414 663 | 430 144 | 844 807 | 7.9 | 14.3 | 11.2 | 5.4 | 12.7 | 9.1 | 2.5 | 1.6 | 2.1 |
| 2007 | 458 298 | 486 648 | 944 947 | 7.7 | 15.4 | 11.7 | 6.0 | 13.6 | 9.9 | 1.7 | 1.8 | 1.8 |
| Country | Population | Age (y) | Outlier excluded | n | A | B | C | Pred. 2022 |
|---|---|---|---|---|---|---|---|---|
| Australia | Total | >15 | 4 | 0.7535 | 125.1 | −0.0629 | 66.6% | |
| Men | >15 | 4 | 0.9926 | 102.0 | −0.0512 | 80.5% | ||
| Women | >15 | 4 | 0.5769 | 151.0 | −0.0759 | 53.5% | ||
| France | Total | >15 | 1996,0.349 | 11 | 0.5494 | 72.3 | −0.0364 | 42.4% |
| Men | >15 | 1996,0.426 | 11 | 0.4775 | 155.3 | −0.0785 | 46.2% | |
| Women | >15 | 1996,0.283 | 11 | 1 | 45.1 | −0.0221 | 36.5% | |
| Switzerland | Total | >15 | 4 | 0.3774 | 459.9 | −0.2316 | 37.7% | |
| Men | >15 | 4 | 0.4936 | 195.3 | −0.0987 | 48.7% | ||
| Women | >15 | 4 | 0.2890 | 1050.6 | −0.5280 | 28.9% | ||
| Switzerland | Total | 15–24 | 4 | 0.1385 | 108.1 | −0.0547 | 12.8% | |
| Men | 15–24 | 4 | 1 | 36.4 | −0.0173 | 18.8% | ||
| Women | 15–24 | 4 | 1 | 9.7 | −0.0036 | 8.5% | ||
| UK | Total | >15 | 2002,0.503 | 13 | 0.6197 | 317.1 | −0.1598 | 61.8% |
| Men | >15 | 2002,0.532 | 14 | 0.6610 | 385.6 | −0.1943 | 66.1% | |
| Women | >15 | 2002,0.479 | 14 | 0.5983 | 249.7 | −0.1259 | 59.3% | |
| US NHIS | Total | >15 | 9 | 0.6321 | 264.4 | −0.1332 | 62.8% | |
| Men | >15 | 9 | 0.7023 | 336.6 | −0.1696 | 70.1% | ||
| Women | >15 | 9 | 0.5968 | 177.4 | −0.0894 | 57.7% | ||
| Country | Population | Age (y) | Outlier excluded | n | A | B | C | Pred. 2022 |
|---|---|---|---|---|---|---|---|---|
| Australia | Total | >15 | 4 | 0.2778 | 193.8 | −0.0970 | 25.4% | |
| Men | >15 | 4 | 0.6587 | 138.8 | −0.0688 | 38.4% | ||
| Women | >15 | 4 | 0.2063 | 254.5 | −0.1278 | 20.2% | ||
| France | Total | >15 | 1996,0.091 | 11 | 1 | 83.3 | −0.0404 | 16.9% |
| Men | >15 | 1996,0.089 | 11 | 1 | 83.0 | −0.0403 | 16.9% | |
| Women | >15 | 1996,0.093 | 11 | 1 | 83.8 | −0.0407 | 17.0% | |
| Switzerland | Total | >15 | 4 | 0.0847 | 340.2 | −0.1711 | 8.4% | |
| Men | >15 | 4 | 0.1800 | 81.1 | −0.0404 | 11.3% | ||
| Women | >15 | 4 | 0.0768 | 737.0 | −0.3702 | 7.7% | ||
| Switzerland | Total | 15–24 | 4 | 1 | 108.5 | −0.0521 | 4.3% | |
| Men | 15–24 | 4 | 1 | 81.3 | −0.0385 | 3.2% | ||
| Women | 15–24 | 4 | 0.0212 | 707.2 | −0.3543 | 2.1% | ||
| UK | Total | >15 | 2002,0.186 | 14 | 0.3245 | 183.6 | −0.0920 | 30.0% |
| Men | >15 | 15 | 0.2780 | 228.3 | −0.1145 | 26.8% | ||
| Women | >15 | 2002,0.192 | 14 | 0.4630 | 119.1 | −0.0594 | 34.7% | |
| US NHIS | Total | >15 | 9 | 0.3082 | 238.8 | −0.1198 | 29.9% | |
| Men | >15 | 9 | 0.2910 | 293.7 | −0.1474 | 28.7% | ||
| Women | >15 | 9 | 0.3253 | 202.1 | −0.1014 | 30.9% | ||
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Schneider, H.; Dietrich, E.S.; Venetz, W.P. Trends and Stabilization up to 2022 in Overweight and Obesity in Switzerland, Comparison to France, UK, US and Australia. Int. J. Environ. Res. Public Health 2010, 7, 460-472. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph7020460
Schneider H, Dietrich ES, Venetz WP. Trends and Stabilization up to 2022 in Overweight and Obesity in Switzerland, Comparison to France, UK, US and Australia. International Journal of Environmental Research and Public Health. 2010; 7(2):460-472. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph7020460
Chicago/Turabian StyleSchneider, Heinz, Eva S. Dietrich, and Werner P. Venetz. 2010. "Trends and Stabilization up to 2022 in Overweight and Obesity in Switzerland, Comparison to France, UK, US and Australia" International Journal of Environmental Research and Public Health 7, no. 2: 460-472. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph7020460