A Literature Review of Cost-Benefit Analyses for the Treatment of Alcohol Dependence

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Data Extraction
3. Results
3.1. Psychotherapy Studies
3.2. Pharmacotherapy Studies
4. Conclusions
Acknowledgments
References
- Cunningham, JA; Blomquist, J. Examining treatment use among alcohol-dependent individuals from a population perspective. Alcohol Alcohol 2006, 41, 632–635. [Google Scholar]
- Humphreys, K; Moos, R. Can encouraging substance abuse patients to participate in self-help groups reduce demand for health care? A Quasi-experimental study. Alcohol. Clin. Exp. Res 2001, 25, 711–716. [Google Scholar]
- La Chance, H; Feldstein, ESW; Bryan, AD; Hutchison, KE. What makes group motivational enhancement therapy (MET) work? A randomized controlled trial of college student drinkers in mandated alcohol diversion. Psychol. Addict. Behav 2009, 23, 598–612. [Google Scholar]
- Liddle, HA; Dakof, GA; Turner, RM; Henderson, CE; Greenbaum, PE. Treating adolescent drug abuse: A randomized trial comparing multidimensional family therapy and cognitive behavior therapy. Addiction 2008, 103, 1660–1670. [Google Scholar]
- Olive, MF. Pharmacotherapies for alcoholism: The old and the new. CNS Neurol. Disord. Drug Targets 2010, 9, 2–4. [Google Scholar]
- Williams, SH. Medications for treating alcohol dependence. Am. Fam. Phys 2005, 72, 1775–1780. [Google Scholar]
- Anton, R; O’Malley, S; Ciraulo, D; Cisler, R; Couper, D; Donovan, DM; Gastfriend, DR; Hosking, JD; Johnson, BA; LoCastro, JS; et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence. The COMBINE study: A randomized controlled trial. JAMA 2006, 17, 2003–2017. [Google Scholar]
- Bouza, C; Angeles, M; Munoz, A; Amate, JM. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: A systematic review. Addiction 2004, 99, 811–828. [Google Scholar]
- Kranzler, HR; van Kirk, M. Efficacy of naltrexone and acamprosate for alcoholism treatment: A meta-analysis. Alcohol. Clin. Exp. Res 2001, 25, 1335–1341. [Google Scholar]
- Garbutt, JC; Kranzler, HR; O’Malley, SS; Gastriend, DR; Pettinati, HM. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence. JAMA 2005, 293, 1617–1625. [Google Scholar]
- Mann, K; Lehert, P; Morgan, MY. The efficacy of acamprosate in the maintenance of abstinence in alcohol-dependent individuals: Results of a meta-analysis. Alcohol. Clin. Exp. Res 2004, 28, 51–63. [Google Scholar]
- Johnson, BA; Ait-Daoud, N; Seneviratne, C; Roache, JD; Javors, MA; Wang, XQ; Liu, L; Penberthy, JK; DiClemente, CC; Li, MD. Pharmacogenetic approach at the serotonin transporter gene as a method of reducing the severity of alcohol drinking. Am. J. Psychiatry 2011, 168, 265–275. [Google Scholar]
- Leggio, L; Garbutt, JC; Addolorato, G. Effectiveness and safety of baclofen in the treatment of alcohol dependent patients. CNS Neurol. Disord. Drug Targets 2010, 9, 33–44. [Google Scholar]
- Kranzler, HR; Armeli, S; Tennen, H; Covault, J; Feinn, R; Arias, AJ; Pettinati, H; Oncken, C. A double-blind, randomized trial of sertraline for alcohol dependence: Moderation by age and 5-hydroxytryptamine transporter-linked promoter region genotype. J. Clin. Psychopharmacol 2011, 31, 22–30. [Google Scholar]
- Pettinati, HM; Oslin, DW; Kampman, KM; Dundon, WD; Xie, H; Gallis, TL; Dackis, CA; O’Brien, CP. A double-blind, placebo-controlled trial combining sertraline and naltrexone for treating co-occurring depression and alcohol dependence. Am. J. Psychiatry 2010, 167, 668–675. [Google Scholar]
- Litten, RZ; Fertig, J; Mattson, ME; Egli, M. Development of medications for alcohol use disorders: Recent advances and ongoing challenges. Expert Opin. Emerging Drugs 2005, 10, 323–343. [Google Scholar]
- Kraemer, KL. The cost-effectiveness and cost-benefit of screening and brief intervention for unhealthy alcohol use in medical settings. Subst. Abus 2007, 28, 67–77. [Google Scholar]
- For Windows XP. Version 14. Minitab Inc.: State College, PA, USA, 2007.
- O’Farrell, TJ; Choquette, KA; Cutter, HSG; Floyd, FJ; Bayog, R; Brown, ED; Lowe, J; Chan, A; Deneault, P. Cost-benefit and cost-effectiveness analyses of behavioral marital therapy as an addition to outpatient alcoholism treatment. J. Subst. Abus 1996, 8, 145–166. [Google Scholar]
- O’Farrell, TJ; Choquette, KA; Cutter, HSG; Brown, E; Bayog, R; McCourt, W; Lowe, J; Chan, A; Deneault, P. Cost-benefit and cost-effectiveness analyses of behavioral marital therapy with or without relapse prevention sessions for alcoholics and their spouses. Behav. Ther 1996, 27, 7–24. [Google Scholar]
- Fleming, MF; Mundt, MP; French, MT; Manwell, LB; Stauffacher, EA; Barry, KL. Benefit-cost analysis of brief physician advice with problem drinkers in primary care settings. Med. Care 2000, 38, 7–18. [Google Scholar]
- Fleming, MF; Mundt, MP; French, MT; Manwell, LB; Stauffacher, EA; Barry, KL. Brief Physician advice for problem drinkers: Long term efficacy and benefit-cost analysis. Alcohol. Clin. Exp. Res 2002, 26, 36–43. [Google Scholar]
- Mundt, MP; French, MT; Roebuck, MC; Manwell, LB; Barry, KL. Brief physician advice for problem drinking among older adults: An economic analysis of cost and benefits. J. Stud. Alcohol 2005, 66, 389–394. [Google Scholar]
- Mundt, MP. Analyzing the costs and benefits of brief intervention. Alcohol. Res. Health 2006, 29, 34–36. [Google Scholar]
- Gentilello, LM; Ebel, BE; Wickizer, TM; Salkever, DS; Rivara, FP. Alcohol interventions for trauma patients treated in emergency departments and hospitals. Ann. Surg 2005, 241, 541–550. [Google Scholar]
- Annemans, L; Vanoverbeke, N; Tecco, J; D’Hooghe, D. Economic evaluation of campral (acamprosate) compared to placebo in maintaining abstinence in alcohol-dependent patients. Eur. Addict. Res 2000, 6, 71–78. [Google Scholar]
- Portella, E; Ridao, M; Carrillo, E; Ribas, E; Ribó, C; Salvat, M. Alcohol y su abuso: Impacto Socio Económico; Editorial Medica Panamericana, S.A.: Madrid, Spain, 1998. [Google Scholar]
- Poldrugo, F; Haeger, DA; Comte, S; Walburg, J; Palmer, A. A critical review of pharmacoeconomic studies of acamprosate. Alcohol Alcohol 2005, 40, 422–430. [Google Scholar]
- Holder, HD. Cost benefits of substance abuse treatment: An overview of results from alcohol and drug abuse. J. Ment. Health Policy Econ 1998, 1, 23–29. [Google Scholar]
- Kane, R; Wall, M; Potthoff, S; Stromberg, K; Dai, Y; Meyer, Z. The effect of alcoholism treatment on medical care use. Med. Care 2004, 42, 395–402. [Google Scholar]
- Swift, RM. The pharmacotherapy of alcohol dependence: Clinical and economic aspects. Econ. Neurosci 2001, 3, 62–66. [Google Scholar]
- Kranzler, HR. Pharmacotherapy of alcoholism: Gaps in knowledge and opportunities for research. Alcohol Alcohol 2002, 35, 537–547. [Google Scholar]
- Graham, R; Wodak, AD; Whelan, G. New pharmacotherapies for alcohol dependence. Med. J. Aust 2002, 177, 103–107. [Google Scholar]
- Carroll, KM; Kosten, TR; Rounsaville, BJ. Choosing a behavioral therapy platform for pharmacotherapy of substance users. Drug Alcohol Depend 2004, 75, 123–134. [Google Scholar]



{kind=link}
{kind=link}
| Reference | Country | Population & Sample Size | Type of Intervention | Type of Cost |
|---|---|---|---|---|
| PSYCHOTHERAPY | ||||
| [19] | USA | 36 newly abstinent married male alcoholics | Average costs: | |
| 1. IC | IC $450; | |||
| 2. IC + BMT | IC + BMT $857 | |||
| 3. IC + ICT & 24 month follow-up | IC + ICT $895 | |||
| [20] | USA | 59 couples with a newly abstinent alcoholic husband | Average costs: | |
| 1. BMT | BMT $864, | |||
| 2. BMT + RP | BMT + RP $1,640 | |||
| [21] | USA | 482 M & 292 W, age 18–65 | BI by physicians & 12 month follow-up; Review of the prevalence of problem drinking, PT specific alcohol effects, worksheet on drinking cues, drinking agreement as a prescription & drinking diary cards | $205 per PT (clinic cost $165.65, PT cost $38.97) |
| [22] | USA | 482 M & 292 W, age 18–65 | BI by physicians & 48 month follow-up; Review of normative drinking, PT specific alcohol effects, worksheet on drinking cues, drinking diary cards, drinking agreement as a prescription | $205 per PT (clinic cost $166, PT cost $39) |
| [23] | USA | 105 M & 53 W, age 65+ | Brief intervention by physicians & 24-month follow-up assessment, feedback, contracting & goal-setting | $236 per PT (clinic cost $197, PT cost $39) |
| [24] | USA | Primary care clinics | BI by physicians: 12- & 48-month follow-up | $205 per PT (Screening & assessment $88, training cost $23, intervention cost $55, PT cost $39) |
| [25] | USA | Injured PT treated in an emergency department or admitted to a hospital (6% of 20,507,601 adult PTs treated for injuries) | Screening + BI | Direct injury-related medical costs (screening + BI) $600 per PT |
| PHARMACOTHERAPY | ||||
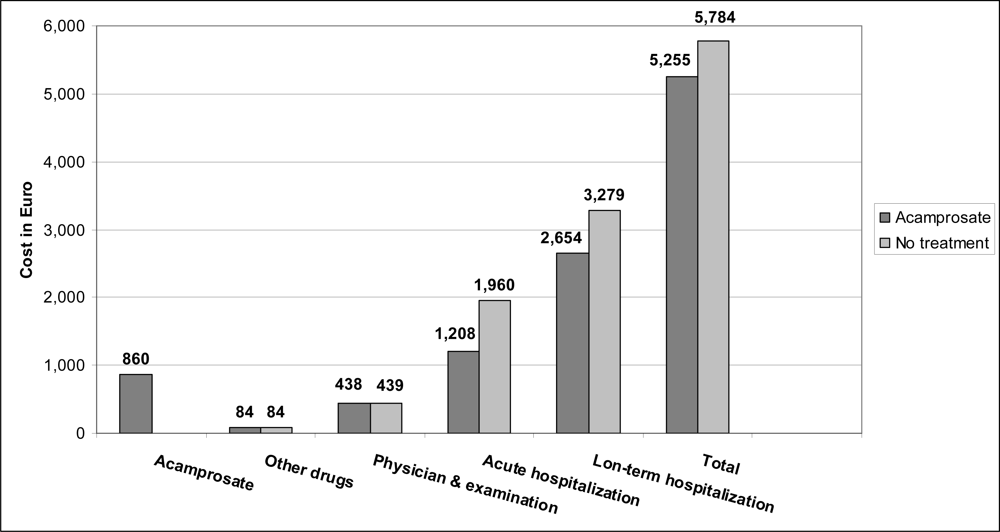
| [26] | Belgium | 448 alcoholic PT | 12-month treatment with acamprosate & 12-month follow-up | Per-PT cost: No treatment 5,783 €; Acamprosate 5,255 € |
| [27] | Spain | Total alcohol-dependent PT population in Spain (approximately 627,400) | Treatment with acamprosate for 1 year, time horizon for benefit was 11–16 years | Spain Pta 42,430 million per year if 50% of affected PT received treatment (Pta 33,944 million if 40% received treatment & Pta 50,917 million if 60% received treatment) |
| Reference | Country | Net Benefits | Benefit-cost Ratio |
|---|---|---|---|
| PSYCHOTHERAPY | |||
| [19] | USA | Average benefits: IC, $7,581; IC + BMT, $6,681; IC + ICT, (−)$2,248 | IC, 20.77 IC + BMT, 8.64 IC + ICT, (−)$2.82 |
| [20] | USA | Average benefits: BMT, $5,053; BMT + RP, $3,365 | BMT, 5.97, BMT + RP, 1.89 |
| [21] | USA | $1,151 per PT Savings: Medical $523, Legal cost & MVE $629 | 3.2 Medical, 5.6 Societal |
| [22] | USA | $7,985 per PT Savings: Medical $712, Legal cost $102, MVE $7,171 | 4.3 Medical, 39.0 Societal |
| [23] | USA | $5,241 per PT Savings: Medical $3,260, MVE $1,613, Life-years lost $368, Other social consequences $1,981 | NA |
| [24] | USA | $7,985 per PT Savings: Medical $712, Legal cost $102, MVE $7,171 | 4.3 Medical, 39.0 Societal |
| [25] | USA | $89 for each PT screened; $330 for each PT offered BI | 3.81 Medical |
| PHARMACOTHERAPY | |||
| [26] | Belgium | Per PT acamprosate-attributable net cost-savings: € 528 over 2 years | NA |
| [27] | Spain | Lifetime benefit for each PT, Pta 3,914,680; avoidance of indirect costs & nonspecific direct costs, Pta 3,409,349; avoidance of direct health-related benefits, Pta 505,331 | NA |
© 2011 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Popova, S.; Mohapatra, S.; Patra, J.; Duhig, A.; Rehm, J. A Literature Review of Cost-Benefit Analyses for the Treatment of Alcohol Dependence. Int. J. Environ. Res. Public Health 2011, 8, 3351-3364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph8083351
Popova S, Mohapatra S, Patra J, Duhig A, Rehm J. A Literature Review of Cost-Benefit Analyses for the Treatment of Alcohol Dependence. International Journal of Environmental Research and Public Health. 2011; 8(8):3351-3364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph8083351
Chicago/Turabian StylePopova, Svetlana, Satya Mohapatra, Jayadeep Patra, Amy Duhig, and Jürgen Rehm. 2011. "A Literature Review of Cost-Benefit Analyses for the Treatment of Alcohol Dependence" International Journal of Environmental Research and Public Health 8, no. 8: 3351-3364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph8083351