
Relationship between Non-Alcoholic Fatty Liver Disease and Psoriasis: A Novel Hepato-Dermal Axis?



Abstract
:
1. Introduction
2. Epidemiology, Clinical Manifestations and Pathogenesis of Psoriasis

3. Epidemiological Evidence Linking Nonalcoholic Fatty Liver Disease (NAFLD) to Psoriasis

{kind=link}
{kind=link}
{kind=link}
| Authors, Year (Reference) | Study Characteristics | NAFLD Diagnosis | Main Findings |
|---|---|---|---|
| Gisondi et al. 2009 [19] | Cross-sectional: 130 consecutive Italian patients with chronic plaque psoriasis and 260 healthy controls matched for age, sex and BMI | Ultrasonography | Prevalence of NAFLD was remarkably higher in psoriatic patients than in matched controls (47% vs. 28%; p < 0.001). Patients with psoriasis and NAFLD were more likely to have metabolic syndrome and had higher serum C-reactive protein concentrations and greater severity of psoriasis according to PASI score than those with psoriasis alone. At multivariate linear regression analysis, NAFLD was associated with higher PASI score (standardized β coefficient 0.19, p = 0.03), independent of age, sex, BMI, psoriasis duration and alcohol consumption |
| Miele et al. 2009 [20] | Retrospective, case-control: 142 Italian patients with psoriasis and 125 non-psoriatic patients with biopsy-proven NAFLD comparable for age and BMI | Ultrasonography and biopsy | Prevalence of NAFLD was 59.2% in the cohort of psoriatic patients. In these patients NAFLD was significantly associated with metabolic syndrome and psoriatic arthritis. Compared with the non-psoriatic NAFLD cohort, psoriatic patients with NAFLD were likely to have more severe NAFLD reflected by either non-invasive NAFLD Fibrosis score or AST/ALT ratio >1 |
| Madanagobalane et al. 2012 [21] | Cross-sectional: 333 Indian psoriatic patients and 330 controls matched for age, sex and BMI | Ultrasonography and liver enzymes | Prevalence of NAFLD was higher in psoriatic patients than in matched controls (17.4% vs. 7.9%; p < 0.005). Psoriatic patients with NAFLD had more severe psoriasis than those without NAFLD. In a subset of participants, psoriatic patients had more severe forms of NAFLD than non-psoriatic patients with NAFLD (as estimated by non-invasive fibrosis markers) |
| van der Voort et al. 2014 [22] | Cross-sectional: population-based cohort of 2292 Dutch elderly participants (the Rotterdam Study) | Ultrasonography | Prevalence of psoriasis was 5.1% (by a validated algorithm). Prevalence of NAFLD was higher in psoriatic patients than in participants without psoriasis (46.2% vs. 33.3%, p = 0.005). Psoriasis was associated with NAFLD (OR 1.70, 95% CI 1.1–2.6, p = 0.01), independent of age, sex, alcohol consumption, pack-years and smoking status, metabolic syndrome, and serum ALT levels |
| van der Voort et al. 2015 [23] | Cross-sectional: population-based cohort of 1535 elderly participants (the Rotterdam Study) of whom 74 (4.7%) had psoriasis | Ultrasonography and transient elastography (Fibroscan) | Prevalence of NAFLD was higher in subjects with psoriasis than in those without psoriasis (44.3% vs. 34%, p < 0.05). Moreover, prevalence of advanced liver fibrosis was 8.1% in psoriatic patients compared with 3.6% in the control group (p < 0.05). Multivariate logistic regression analysis revealed that the risk of advanced liver fibrosis remained higher in psoriatic patients after adjustment for age, sex, alcohol consumption, serum ALT levels, presence of metabolic syndrome and hepatic steatosis (OR 2.57, 95% CI 1.0–6.6) |
| Gisondi et al. 2015 [24] | Cross-sectional: 124 Italian patients with psoriasis and 79 healthy controls | Ultrasonography | Prevalence of NAFLD was higher in psoriatic patients than in controls (44% vs. 26%, p < 0.001). NAFLD fibrosis score was also higher in psoriatic patients (p < 0.001). Multivariate regression analysis revealed that psoriasis was associated with higher NAFLD fibrosis score, independent of age, sex, BMI, hypertension and pre-existing diabetes |
| Abedini et al. 2015 [25] | Cross-sectional: 123 Iranian patients with psoriasis and 123 healthy controls matched by age, sex and BMI | Ultrasonography | Prevalence of NAFLD was higher in psoriatic patients than in matched controls (65.6% vs. 35%, p < 0.01). Multivariate logistic regression analysis revealed that PASI score, waist circumference, hypertension and serum aminotransferase levels independently predicted the ultrasonographic severity of NAFLD |
| Roberts et al. 2015 [26] | Cross-sectional: 103 United States adult patients with a diagnosis of psoriasis or psoriatic arthritis | Ultrasonography and biopsy (available in a subgroup of 52 patients) | The overall prevalence of NAFLD was 47%. The prevalence of NASH was 22% in those who underwent liver biopsy. Psoriatic patients with NAFLD had higher mean PASI scores than those without NAFLD |
| Candia et al. 2015 [27] | Systematic review and meta-analysis: 7 case-control studies included | Ultrasonography and liver enzymes | Psoriatic patients had an increased risk of prevalent NAFLD compared with control subjects (6 studies, n = 267,761 patients, OR 2.15, 95% CI 1.6–2.9, p < 0.05). The risk of prevalent NAFLD was higher in patients with psoriatic arthritis (3 studies, n = 505 patients, OR 2.25, 95% CI 1.4–3.7, p < 0.05) and in those with moderate-to-severe psoriasis compared with patients with mild psoriasis (2 studies, n = 51,930 patients, OR 2.07, 95% CI 1.6–2.7, p < 0.05) |
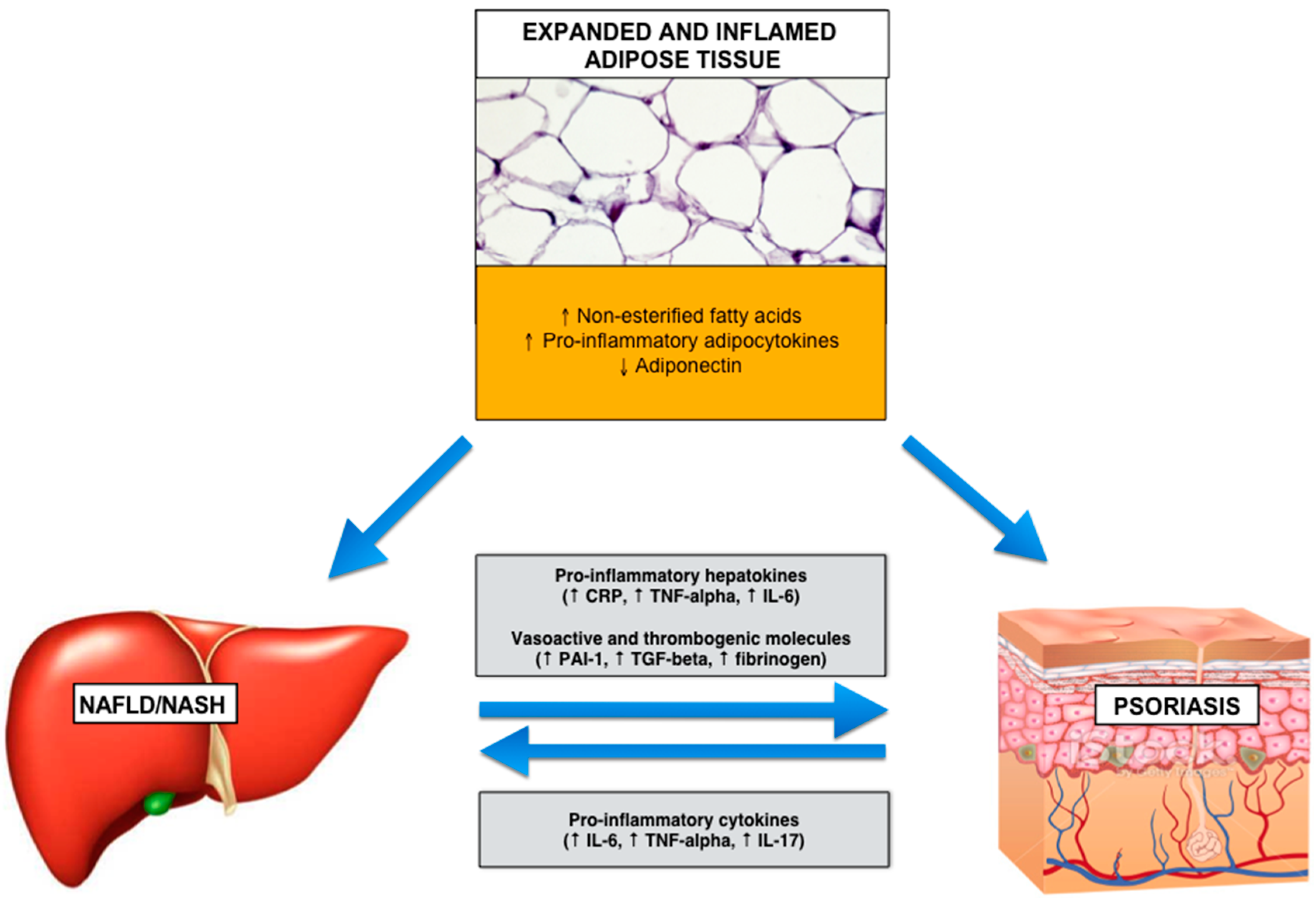
4. Potential Biological Mechanisms Linking Psoriasis and NAFLD

5. Treatment for Psoriasis and Its Potential Implications for NAFLD
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 370, 263–271. [Google Scholar] [CrossRef]
- Gottlieb, A.B.; Chao, C.; Dann, F. Psoriasis comorbidities. J. Dermatol. Treat. 2008, 19, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Non-alcoholic fatty liver disease (NAFLD) Study Group, dedicated to the memory of Prof. Paola Loria; Lonardo, A.; Bellentani, S.; Argo, C.K.; Ballestri, S.; Byrne, C.D.; Caldwell, S.H.; Cortez-Pinto, H.; Grieco, A.; Machado, M.V.; et al. Epidemiological modifiers of non-alcoholic fatty liver disease: Focus on high-risk groups. Dig. Liver Dis. 2015, 47, 997–1006. [Google Scholar]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Ballestri, S.; Marchesini, G.; Angulo, P.; Loria, P. Nonalcoholic fatty liver disease: A precursor of the metabolic syndrome. Dig. Liver Dis. 2015, 47, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, T.; Zhang, C.; Tang, F.; Zhong, N.; Li, H.; Song, X.; Lin, H.; Liu, Y.; Xue, F. Identification of reciprocal causality between non-alcoholic fatty liver disease and metabolic syndrome by a simplified Bayesian network in a Chinese population. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Zona, S.; Targher, G.; Romagnoli, D.; Baldelli, E.; Nascimbeni, F.; Roverato, A.; Guaraldi, G.; Lonardo, A. Nonalcoholic fatty liver disease is associated with an almost two-fold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Lonardo, A.; Bonapace, S.; Byrne, C.D.; Loria, P.; Targher, G. Risk of cardiovascular, cardiac and arrhythmic complications in patients with non-alcoholic fatty liver disease. World J. Gastroenterol. 2014, 20, 1724–1745. [Google Scholar] [CrossRef] [PubMed]
- Ogdie, A.; Gelfand, J.M. Clinical risk factors for the development of psoriatic arthritis among patients with psoriasis: A review of available evidence. Curr. Rheumatol. Rep. 2015, 17. [Google Scholar] [CrossRef] [PubMed]
- Sommer, D.M.; Jenisch, S.; Suchan, M.; Christophers, E.; Weichenthal, M. Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis. Arch. Dermatol. Res. 2006, 298, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Tessari, G.; Conti, A.; Piaserico, S.; Schianchi, S.; Peserico, A.; Giannetti, A.; Girolomoni, G. Prevalence of metabolic syndrome in patients with psoriasis: A hospital-based case-control study. Br. J. Dermatol. 2007, 157, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Ray, A.; Senapati, S.; Chatterjee, R. Genetic and epigenetic basis of psoriasis pathogenesis. Mol. Immunol. 2015, 64, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Lowes, M.A.; Suarez-Farinas, M.; Krueger, J.G. Immunology of psoriasis. Annu. Rev. Immunol. 2014, 32, 227–255. [Google Scholar] [CrossRef] [PubMed]
- Durham, L.E.; Kirkham, B.W.; Taams, L.S. Contribution of the IL-17 pathway to psoriasis and psoriatic arthritis. Curr. Rheumatol. Rep. 2015, 17. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Loria, P.; Carulli, N. Concurrent non-alcoholic steatohepatitis and psoriasis. Report of three cases from the POLI.ST.E.N.A. Study. Dig. Liver Dis. 2001, 33, 86–87. [Google Scholar] [CrossRef]
- Matsumoto, T.; Suziki, N.; Watanabe, H.; Irie, M.; Iwata, K.; Anan, A.; Nakane, H.; Yoshikane, M.; Nishizawa, S.; Sohda, T.; et al. Nonalcoholic steatohepatitis associated with psoriasis vulgaris. J. Gastroenterol. 2004, 39, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Targher, G.; Zoppini, G.; Girolomoni, G. Non-alcoholic fatty liver disease in patients with chronic plaque psoriasis. J. Hepatol. 2009, 51, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Miele, L.; Vallone, S.; Cefalo, C.; la Torre, G.; di Stasi, C.; Vecchio, F.M.; D’Agostino, M.; Gabrieli, M.L.; Vero, V.; Biolato, M.; et al. Prevalence, characteristics and severity of non-alcoholic fatty liver disease in patients with chronic plaque psoriasis. J. Hepatol. 2009, 51, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Madanagobalane, S.; Anandan, S. The increased prevalence of non-alcoholic fatty liver disease in psoriatic patients: A study from South India. Australas. J. Dermatol. 2012, 53, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Van der Voort, E.A.; Koehler, E.M.; Dowlatshahi, E.A.; Hofman, A.; Stricker, B.H.; Janssen, H.L.; Schouten, J.N.; Nijsten, T. Psoriasis is independently associated with nonalcoholic fatty liver disease in patients 55 years old or older: Results from a population-based study. J. Am. Acad. Dermatol. 2014, 70, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Van der Voort, E.A.; Koehler, E.M.; Nijsten, T.; Stricker, B.H.; Hofman, A.; Janssen, H.L.; Schouten, J.N.; Wakkee, M. Increased prevalence of advanced liver fibrosis in patients with psoriasis: A cross-sectional analysis from the Rotterdam study. Acta Derm. Venereol. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gisondi, P.; Barba, E.; Girolomoni, G. Non-alcoholic fatty liver disease fibrosis score in patients with psoriasis. J. Eur. Acad. Dermatol. Venereol. 2015, 30, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Abedini, R.; Salehi, M.; Lajevardi, V.; Beygi, S. Patients with psoriasis are at a higher risk of developing nonalcoholic fatty liver disease. Clin. Exp. Dermatol. 2015, 40, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.K.; Cochet, A.E.; Lamb, P.B.; Brown, P.J.; Battafarano, D.F.; Brunt, E.M.; Harrison, S.A. The prevalence of NAFLD and NASH among patients with psoriasis in a tertiary care dermatology and rheumatology clinic. Aliment. Pharmacol. Ther. 2015, 41, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Candia, R.; Ruiz, A.; Torres-Robles, R.; Chávez-Tapia, N.; Méndez-Sánchez, N.; Arrese, M. Risk of non-alcoholic fatty liver disease in patients with psoriasis: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Birkenfeld, A.L.; Shulman, G.I. Nonalcoholic fatty liver disease, hepatic insulin resistance, and type 2 diabetes. Hepatology 2014, 59, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Shoelson, S.E.; Lee, J.; Goldfine, A.B. Inflammation and insulin resistance. J. Clin. Investig. 2006, 116, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Ucak, S.; Ekmekci, T.; Basat, O. Comparison of various insulin sensitivity indices in psoriatic patients and their relationship with types of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. Ectopic fat, insulin resistance, and nonalcoholic fatty liver disease: Implications for cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Loria, P.; Carulli, L.; Bertolotti, M.; Lonardo, A. Endocrine and liver interaction: The role of endocrine pathways in NASH. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Shulmann, G.I. Ectopic fat in insulin resistance, dyslipidemia, and cardiometabolic disease. N. Engl. J. Med. 2014, 371, 1131–1141. [Google Scholar] [CrossRef] [PubMed]
- Hunter, C.A.; Jones, S.A. IL-6 as a keystone cytokine in health and disease. Nat. Immunol. 2015, 16, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Häring, H.U. The role of hepatokines in metabolism. Nat. Rev. Endocrinol. 2013, 9, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Day, C.P.; Bonora, E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar]
- Kulkarni, N.M.; Jaji, M.S.; Shetty, P.; Kurhe, Y.V.; Chaudhary, S.; Vijaykant, G.; Raghul, J.; Vishwakarma, S.L.; Rajesh, B.N.; Mookkan, J.; et al. A novel animal model of metabolic syndrome with non-alcoholic fatty liver disease and skin inflammation. Pharm. Biol. 2015, 53, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Gisondi, P.; Ormerod, A.D.; Saiag, P.; Smith, C.; Spuls, P.I.; Arenberger, P.; Bachelez, H.; Barker, J.; Dauden, E.; et al. European S3-Guidelines on the systemic treatment of psoriasis vulgaris—Update 2015—Short version—EDF in cooperation with EADV and IPC. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2277–2294. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Galvan, A.; Idolazzi, L.; Girolomoni, G. Management of moderate to severe psoriasis in patients with metabolic comorbidities. Front. Med. 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Kalb, R.E.; Strober, B.; Weinstein, G.; Lebwohl, M. Methotrexate and psoriasis: 2009 National psoriasis foundation consensus conference. J. Am. Acad. Dermatol. 2009, 60, 824–837. [Google Scholar] [CrossRef] [PubMed]
- Hardwick, R.N.; Clarke, J.D.; Lake, A.D.; Canet, M.J.; Anumol, T.; Street, S.M.; Merrell, M.D.; Goedken, M.J.; Snyder, S.A.; Cherrington, N.J. Increased susceptibility to methotrexate-induced toxicity in nonalcoholic steatohepatitis. Toxicol. Sci. 2014, 142, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.; Urwitz, H.; Johannesson, A.; Ros, A.M.; Lindholm, J.; Kinnman, N.; Hultcrantz, R. Psoriasis patients with diabetes type 2 are at high risk of developing liver fibrosis during methotrexate treatment. J. Hepatol. 2007, 46, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Cazzaniga, S.; Chimenti, S.; Giannetti, A.; Maccarone, M.; Picardo, M.; Girolomoni, G.; Naldi, L. Psocare Study Group. Metabolic abnormalities associated with initiation of systemic treatment for psoriasis: Evidence from the Italian Psocare Registry. J. Eur. Acad. Dermatol. Venereol. 2013, 27, e30–e41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuvonen, P.J.; Niemi, M.; Backman, J.T. Drug interactions with lipid-lowering drugs: Mechanisms and clinical relevance. Clin. Pharmacol. Ther. 2006, 80, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Dunn, L.K.; Gaar, L.R.; Yentzer, B.A.; O’Neill, J.L.; Feldman, S.R. Acitretin in dermatology: A review. J. Drugs Dermatol. 2011, 10, 772–782. [Google Scholar] [PubMed]
- Martinez Abundis, E.; Reynoso-von, D.C.; Hernandez-Salazar, E.; Gonzalez-Ortiz, M. Effect of etanercept on insulin secretion and insulin sensitivity in a randomized trial with psoriatic patients at risk for developing type 2 diabetes mellitus. Arch. Dermatol. Res. 2007, 299, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Stanley, T.L.; Zanni, M.V.; Johnsen, S.; Rasheed, S.; Makimura, H.; Lee, H.; Khor, V.K.; Ahima, R.S.; Grinspoon, S.K. TNF-α antagonism with etanercept decreases glucose and increases the proportion of high molecular weight adiponectin in obese subjects with features of the metabolic syndrome. J. Clin. Endocrinol. Metab. 2011, 96, E146–E150. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.H.; Massarotti, E.; Garg, R.; Liu, J.; Canning, C.; Schneeweiss, S. Association between disease-modifying anti-rheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis. JAMA 2011, 305, 2525–2531. [Google Scholar] [CrossRef] [PubMed]
- Lestre, S.; Diamantino, F.; Veloso, L.; Fidalgo, A.; Ferreira, A. Effects of etanercept treatment on lipid profile in patients with moderate-to-severe chronic plaque psoriasis: A retrospective cohort study. Eur. J. Dermatol. 2011, 21, 916–920. [Google Scholar] [PubMed]
- Gisondi, P.; Conti, A.; Galdo, G.; Piaserico, S.; de Simone, C.; Girolomoni, G. Ustekinumab does not increase body mass index in patients with chronic plaque psoriasis: A prospective cohort study. Br. J. Dermatol. 2013, 168, 1124–1127. [Google Scholar] [CrossRef] [PubMed]
- Tobon, G.J.; Cañas, C.; Jaller, J.J.; Restrepo, J.C.; Anaya, J.M. Serious liver disease induced by infliximab. Clin. Rheumatol. 2007, 26, 578–581. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.W.; Griffiths, C.E. Novel systemic therapies for the treatment of psoriasis. Expert. Opin. Pharmacother. 2016, 17, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Ganzetti, G.; di Sario, A.; Damiani, A.; Sandroni, L.; Rosa, L.; Benedetti, A.; Offidani, A. The effect of etanercept on hepatic fibrosis risk in patients with non-alcoholic fatty liver disease, metabolic syndrome, and psoriasis. J. Gastroenterol. 2013, 48, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Feagins, L.A.; Flores, A.; Arriens, C.; Park, C.; Crook, T.; Reimold, A.; Brown, G. Nonalcoholic fatty liver disease: A potential consequence of tumor necrosis factor-inhibitor therapy. Eur. J. Gastroenterol. Hepatol. 2015, 27, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Del Giglio, M.; Gisondi, P.; Tessari, G.; Girolomoni, G. Weight reduction alone may not be sufficient to maintain disease remission in obese patients with psoriasis: A randomized, investigator-blinded study. Dermatology 2012, 224, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.; Zachariae, C.; Christensen, R.; Geiker, N.R.; Schaadt, B.K.; Stender, S.; Hansen, P.R.; Astrup, A.; Skov, L. Effect of weight loss on the severity of psoriasis: A randomized clinical study. JAMA Dermatol. 2013, 149, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; del Giglio, M.; di Francesco, V.; Zamboni, M.; Girolomoni, G. Weight loss improves the response of obese patients with moderate-to-severe chronic plaque psoriasis to low-dose cyclosporine therapy: A randomized, controlled, investigator-blinded clinical trial. Am. J. Clin. Nutr. 2008, 88, 1242–1247. [Google Scholar] [PubMed]
- Al-Mutairi, N.; Nour, T. The effect of weight reduction on treatment outcomes in obese patients with psoriasis on biologic therapy: A randomized controlled prospective trial. Expert Opin. Biol. Ther. 2014, 14, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Shafiq, N.; Rajagopalan, S.; Dogra, S.; Malhotra, S. Thiazolidinediones for plaque psoriasis: A systematic review and meta-analysis. Evid. Based Med. 2012, 17, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, F.; Pais, R.; Bellentani, S.; Day, C.P.; Ratziu, V.; Loria, P.; Lonardo, A. From NAFLD in clinical practice to answers from guidelines. J. Hepatol. 2013, 59, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Castera, L.; Vilgrain, V.; Angulo, P. Noninvasive evaluation of NAFLD. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Romagnoli, D.; Nascimbeni, F.; Francica, G.; Lonardo, A. Role of ultrasound in the diagnosis and treatment of nonalcoholic fatty liver disease and its complications. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 603–627. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Ballestri, S.; Targher, G.; Loria, P. Diagnosis and management of cardiovascular risk in nonalcoholic fatty liver disease. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 629–650. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, A.; Gisondi, P.; Lonardo, A.; Targher, G. Relationship between Non-Alcoholic Fatty Liver Disease and Psoriasis: A Novel Hepato-Dermal Axis? Int. J. Mol. Sci. 2016, 17, 217. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17020217
Mantovani A, Gisondi P, Lonardo A, Targher G. Relationship between Non-Alcoholic Fatty Liver Disease and Psoriasis: A Novel Hepato-Dermal Axis? International Journal of Molecular Sciences. 2016; 17(2):217. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17020217
Chicago/Turabian StyleMantovani, Alessandro, Paolo Gisondi, Amedeo Lonardo, and Giovanni Targher. 2016. "Relationship between Non-Alcoholic Fatty Liver Disease and Psoriasis: A Novel Hepato-Dermal Axis?" International Journal of Molecular Sciences 17, no. 2: 217. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17020217