
Transcranial Magnetic Stimulation of the Supplementary Motor Area in the Treatment of Obsessive-Compulsive Disorder: A Multi-Site Study

Abstract
:1. Introduction
2. Results
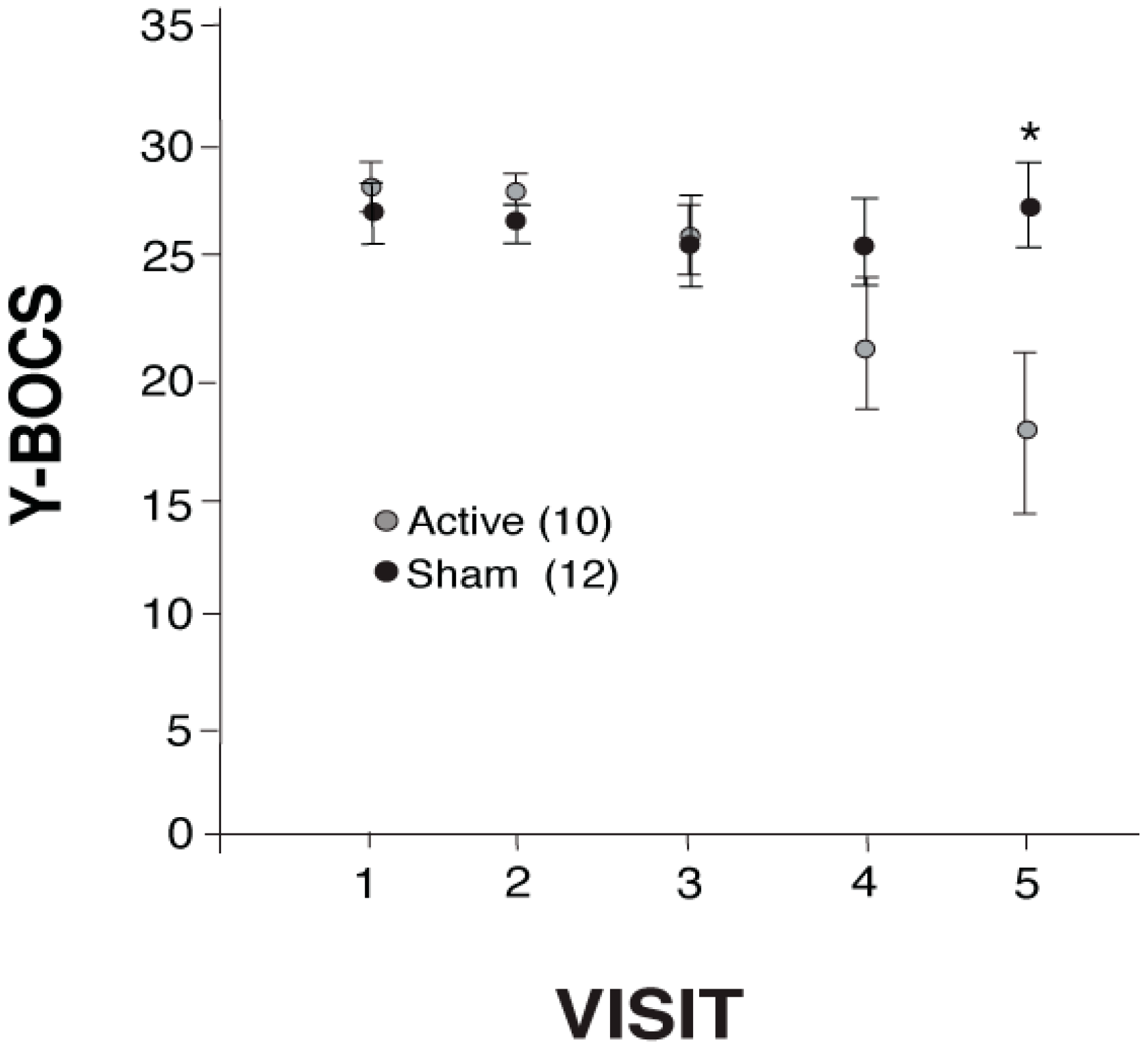
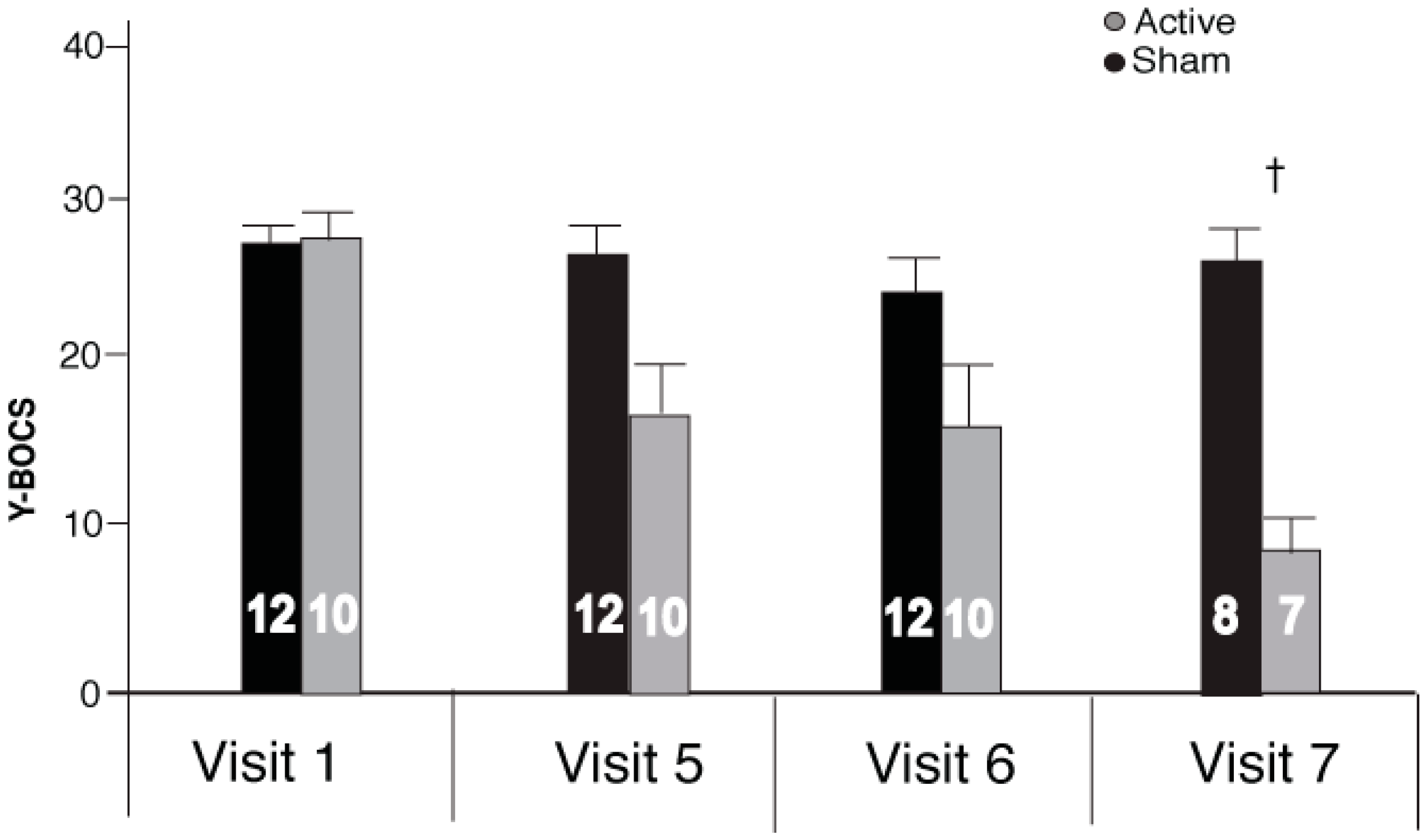
2.1. Repetitive Transcranial Stimulation (rTMS) Effects on Yale-Brown Obsessive Compulsive Scale (Y-BOCS)
2.2. rTMS Effects on the Hamilton Depression Rating Scale 21 (HDRS-21) and Clinical Global Impression Scale (CGI)
3. Discussion
4. Methods
4.1. Patients
4.2. Stimulation Parameters
4.3. Outcome Measures
4.4. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Torres, A.R.; Prince, M.J.; Bebbington, P.E.; Bhugra, D.; Brugha, T.S.; Farrell, M.; Jenkins, R.; Lewis, G.; Meltzer, H.; Singleton, N. Obsessive-compulsive disorder: Prevalence, comorbidity, impact, and help-seeking in the British National Psychiatric Morbidity Survey of 2000. Am. J. Psychiatry 2006, 163, 1978–1985. [Google Scholar] [CrossRef] [PubMed]
- Horwath, E.; Weissman, M.M. The epidemiology and cross-national presentation of obessesive-compulsive disorder. Psychiatr. Clin. N. Am. 2000, 23, 493–507. [Google Scholar] [CrossRef]
- Stein, D.J. Obsessive-compulsive disorder. Lancet 2002, 360, 397–405. [Google Scholar] [CrossRef]
- Heyman, I.; Mataix-Cols, D.; Fineberg, N.A. Obsessive-compulsive disorder. BMJ 2006, 333, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, J.S.; Taylor, S.; McKay, D. Obsessive-compulsive disorder. Lancet 2009, 374, 491–499. [Google Scholar] [CrossRef]
- Eisen, J.L.; Sibrava, N.J.; Boisseau, C.L.; Mancebo, M.C.; Stout, R.L.; Pinto, A.; Rasmussen, S.A. Five-year course of obsessive-compulsive disorder: Predictors of remission and relapse. J. Clin. Psychiatry 2013, 74, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Pallanti, S.; Quercioli, L. Treatment-refractory obsessive-compulsive disorder: Methodological issues, operational definitions and therapeutic lines. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2006, 30, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Rosa-Alcazar, A.I.; Sanchez-Meca, J.; Gomez-Conesa, A.; Marin-Martinez, F. Psychological treatment of obsessive-compulsive disorder: A meta-analysis. Clin. Psychol. Rev. 2008, 28, 1310–1325. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, N.A.; Gale, T.M. Evidence-based pharmacotherapy of obsessive-compulsive disorder. Int. Clin. Psychopharmacol. 2005, 22, 2313–322. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Consoli, G. Treatment strategies for obsessive-compulsive disorder. Exp. Opin. Pharmacother. 2010, 11, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, N.A.; Brown, A.; Reghunandanan, S.; Pampaloni, I. Evidence-based pharmacotherapy of obsessive-complusive disorder. Int. J. Neuropsychopharmacol. 2012, 15, 1173–1191. [Google Scholar] [CrossRef] [PubMed]
- Berlim, M.T.; Neufeld, N.H.; van den Eynde, F. Repetitive transcranial magnetic stimulation (rTMS) for obsessive-compulsive disorder (OCD): An exploratory meta-analysis of randomized and sham-controlled trails. J. Psychiatr. Res. 2013, 47, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Figee, M.; Luigjes, J.; Smolders, R.; Valencia-Alfonso, C.E.; van Wingen, G.; de Kwaasteniet, B.; Mantione, M.; Ooms, P.; de Koning, P.; Vulink, N.; et al. Deep brain stimulation restores frontostriatal network activity in obsessive-compulsive disorder. Nat. Neurosci. 2013, 16, 386–387. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Simpson, H.B.; Fallon, B.A.; Rossi, S.; Lisanby, S.H. Randomized sham-controlled trial of repetitive transcranial magnetic stimulation in treatment-resistant obsessive-compulsive disorder. Int. J. Neuropsychopharmacol. 2010, 13, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Gomes, P.V.O.; Brasil-Neto, J.P.; Allam, N.; Rodrigues de Souza, E. A randomized, double-blind trial of repetitive transcrainial magnetic stimulation in obsessive-compulsive disorder with three-month follow-up. J. Neuropsychiatry Clin. Neurosci. 2010, 24, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Figee, M.; Vink, M.; de Geus, F.; Vulink, N.; Veltman, D.J.; Westenberg, H.; Denys, D. Dysfunctional reward circuitry in obsessive-compulsive disorder. Biol. Psychiatry 2011, 69, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Harrison, B.J.; Pujol, J.; Cardoner, N.; Dues, J.; Alonso, P.; López-Solà, M.; Contreras-Rodríguez Real, E.; Segalàs, C.; Blanco-Hinojo, L.; Menchon, J.M.; et al. Brain corticostriatal systems and the major clinical symptom dimensions of obsessive-compulsive disorder. Biol. Psychiatry 2013, 73, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.H.; Kim, J.H.; Jung, W.H.; Choi, J.S.; Jung, M.H.; Lee, J.M.; Choi, C.H.; Kang, D.H.; Kwon, J.S. Functional connectivity in fronto-subcortical circuitry during the resting state in obsessive-compulsive disorder. Neurosci. Lett. 2010, 474, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Min, B.K.; Kim, S.J.; Park, J.Y.; Park, H.J. Prestimulus top-down reflection of obsessive-compulsive disorder in EEG frontal theta and occipital α oscillations. Neurosci. Lett. 2011, 496, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Lee, J.; Park, H.J.; Kim, J.J.; Namkoong, K.; Kim, S.J. α Amplitude and phase locking in obsessive-compulsive disorder during working memory. Int. J. Psychophysiol. 2012, 83, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Stern, E.R.; Fitzgerald, K.D.; Welsh, R.C.; Abelson, J.L.; Taylor, S.F. Resting-state functional connectivity between fronto-parietal and default mode networks in obsessive-compulsive disorder. PLoS ONE 2012, 7, e36356. [Google Scholar] [CrossRef] [PubMed]
- Buzsaki, G.; Draguhn, A. Neuronal oscillations in cortical networks. Science 2004, 304, 1926–1929. [Google Scholar] [CrossRef] [PubMed]
- Basar, E.; Basar-Eroglu, C.; Karakas, S.; Schurmann, M. γ, α, δ, and θ oscillations govern cognitive processes. Int. J. Psychophysiol. 2001, 39, 241–248. [Google Scholar] [CrossRef]
- Engel, A.K.; Fries, P.; Singer, W. Dynamic predictions: Oscillations and synchrony in top-down processing. Nat. Rev. Neurosci. 2001, 2, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Fuggetta, G.; Noh, N.A. A neurophysiological insight into the potential link between transcranial magnetic stimulation, thalamocortical dysrhythmia and neuropsychiatric disorders. Exp. Neurol. 2013, 245, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Van den Heuvel, O.A.; Veltman, D.J.; Groenewegen, H.J.; Cath, D.C.; van Balkom, A.J.L.M.; van Hartskamp, J.; Barkhof, F.; van Dyck, R. Frontal-striatal dysfunction during planning in obsessive-compulsive disorder. Arch. Gen. Psychiatry 2005, 62, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, S.R.; Blackwell, A.D.; Fineberg, N.A.; Robbins, T.W.; Sahakian, B.J. The neuropsychology of obsessive compulsive disorder: The importance of failures in cognitive and behavioural inhibition as candidate endophenotypic markers. Neurosci. Biobehav. Rev. 2005, 29, 399–419. [Google Scholar] [CrossRef] [PubMed]
- De Wit, S.J.; de Vries, F.E.; van der Werf, Y.D.; Cath, D.C.; Heslenfeld, D.J.; Veltman, E.M.; van Balkom, A.J.L.M.; Veltman, D.J.; van den Heuvel, O.A. Presupplementary motor area hyperactivity during response inhibition: A candidate endophenotype of obsessive compulsive disorder. Am. J. Psychiatry 2012, 169, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Modirrousta, M.; Shams, E.; Mansouri, B.; Moussavi, Z.; Sareen, J.; Enns, M. The efficacy of deep repetitive transcranial magnetic stimulation over the medial prefrontal cortex in obsessive compulsive disorder: Results from an open-label study. Depress Anxiety 2015, 32, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, B.D.; Ziemann, U.; Harmon, A.; Murphy, D.L.; Wassermann, E.M. Decreased neuronal inhibition in cerebral cortex in obsessive-compulsive disorder on transcranial magnetic stimulation. Lancet 1998, 352, 881–882. [Google Scholar] [CrossRef]
- Greenberg, B.D.; Ziemann, U.; Cora-Locatelli, G.; Harmon, A.; Murphy, D.L.; Keel, J.C.; Wassermann, E.M. Altered cortical excitability in obsessive-compulsive disorder. Neurology 2000, 54, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Lisanby, S.H.; Pieraccini, F.; Ulivelli, M.; Castrogiovanni, P.; Rossi, S. Repetitive transcranial magnetic stimulation (rTMS) in the treatment of obsessive-compulsive disorder (OCD) and Tourette’s syndrome (TS). Int. J. Neuropsychopharmacol. 2006, 9, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Naro, A.; Mastroeni, C.; Morgante, C.; Terranova, M.R.; Muscatello, R.; Zoccali, R.; Calabro, R.S.; Quartarone, A. Obsessive-compulsive disorder: A “sensory-motor” problem? Int. J. Psychophysiol. 2014, 92, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Rossi, S.; Bassi, B.D.; Simpson, H.B.; Fallon, B.A.; Lisanby, S.H. Modulation of motor cortex excitability in obsessive-compulsive disorder: An exploratory study on the relations of neurophysiology measures with clinical outcome. Psychiatry Res. 2013, 210, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Simpson, H.B.; Huppert, J.D.; Petkova, E.; Foa, E.B.; Liebowitz, M.R. Response versus remission in obsessive-compulsive disorder. J. Clin. Psychiatry 2006, 67, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Menzies, L.; Chamberlain, S.R.; Laird, A.R.; Thelan, S.M.; Sahakian, B.J.; Bullmore, E.T. Integrating evidence from neuroimaging and neuropsychological studies of obsessive-compulsive disorder: The orbitofronto-striatal model revisited. Neurosci. Biobehav. Rev. 2008, 32, 525–549. [Google Scholar] [CrossRef] [PubMed]
- Dold, M.; Aigner, M.; Lanzenberger, R.; Kasper, S. Antipsychotic augmentation of serotonin reuptake inhibitors in treatment-resistent obsessive-compulsive disorder: A meta-analysis of double-blind, randomized, placebo-controlled trials. Int. J. Neuropsychopharmacol. 2013, 16, 557–574. [Google Scholar] [CrossRef] [PubMed]
- Overbeek, T.; Schruers, K.; Vermetten, E.; Griez, E. Comorbidity of obsessive-compulsive disorder and depression: Prevalence, symptom severity, and treatment effect. J. Clin. Psychiatry 2002, 63, 1106–1112. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhou, C.; Wu, B.; Want, Y.; Li, Q.; Wei, Y.; Yang, D.; Mu, J.; Zhu, D.; Zou, D.; et al. Left versus right repetitive transcranial magnetic stimulation in treating major depression: A meta-analysis of randomized controlled trials. Psychiatry Res. 2013, 210, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Drevets, W.C.; Price, J.L.; Furey, M.L. Brain structural functional abnormalities in mood disorders: Implications for neurocircuitry models of depression. Brain Struct. Funct. 2008, 213, 93–118. [Google Scholar] [CrossRef] [PubMed]
- Remijnse, P.L.; van den Heuvel, O.; Nielen, M.M.A.; Vriend, C.; Hendriks, G.J.; Hoogendijk, W.J.G.; Uylings, H.B.M.; Veltman, D.J. Cognitive inflexibility in obsessive-compulisve disorder and major depression is associated with distinct neural correlates. PLoS ONE 2013, 8, e59600. [Google Scholar] [CrossRef] [PubMed]
- Nauczyciel, C.; Le Jeune, F.; Naudet, F.; Douabin, S.; Esquevin, A.; Verin, M.; Dondaine, T.; Robert, G.; Drapier, D.; Millet, B. Repetitive transcranial magnetic stimulation over the orbitofrontal cortex for obsessive compulsive disorder: A double-blind, crossover study. Transl. Psychiatry 2014, 4, e436. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Samples | Bulgaria | Turkey | ANOVA |
|---|---|---|---|
| Male (age ± SD) | 7 (28 ± 12) | 4 (28 ± 7) | p = 0.154 (for age, sex collapsed) |
| Female (age ± SD) | 8 (38 ± 11) | 3 (43 ± 16) | – |
| Duration of OCD (y ± SD) | 7 ± 7 | 18 ± 12 | p = 0.037 |
| Baseline (Visit 1) HDRS-17 | 13 ± 1 | 12 ± 4 | p = 0.104 |
| Baseline (Visit 1) Y-BOCS | 28 ± 5 | 28 ± 4 | p = 0.847 |
| Samples | Active (Mean ± SD) | Sham (Mean ± SD) | t-Test |
|---|---|---|---|
| HDRS-21 | |||
| Baseline (Visit 1) | 14 ± 3 | 15 ± 2 | p = 0.437 |
| Treatment end (Visit 5) | 8 ± 8 | 17 ± 6 | p = 0.012 |
| Two-week follow-up (Visit 6) | 9 ± 10 | 16 ± 6 | p = 0.084 |
| CGI | |||
| Baseline (Visit 1) | 5 ± 1 | 5 ± 1 | p = 1.000 |
| Treatment end (Visit 5) | 4 ± 2 | 5 ± 2 | p = 0.084 |
| Two-week follow-up (Visit 6) | 4 ± 2 | 5 ± 2 | p = 0.084 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawken, E.R.; Dilkov, D.; Kaludiev, E.; Simek, S.; Zhang, F.; Milev, R. Transcranial Magnetic Stimulation of the Supplementary Motor Area in the Treatment of Obsessive-Compulsive Disorder: A Multi-Site Study. Int. J. Mol. Sci. 2016, 17, 420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17030420
Hawken ER, Dilkov D, Kaludiev E, Simek S, Zhang F, Milev R. Transcranial Magnetic Stimulation of the Supplementary Motor Area in the Treatment of Obsessive-Compulsive Disorder: A Multi-Site Study. International Journal of Molecular Sciences. 2016; 17(3):420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17030420
Chicago/Turabian StyleHawken, Emily R., Dancho Dilkov, Emil Kaludiev, Selcuk Simek, Felicia Zhang, and Roumen Milev. 2016. "Transcranial Magnetic Stimulation of the Supplementary Motor Area in the Treatment of Obsessive-Compulsive Disorder: A Multi-Site Study" International Journal of Molecular Sciences 17, no. 3: 420. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17030420