
Association between Pre-Transplant Serum Malondialdehyde Levels and Survival One Year after Liver Transplantation for Hepatocellular Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Design
4.2. Variables Recorded
4.3. End-Point
4.4. Blood Samples and Serum Malondialdehyde Level Analysis
4.5. Statistical Methods
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| AFP | alpha-fetoprotein |
| AUC | area under curve |
| d-ROM | derivatives of reactive oxygen metabolites |
| HCC | hepatocellular carcinoma |
| LT | liver transplantation |
| MDA | malondialdehyde |
| ROC | receiver operator characteristic |
| ROS | reactive oxygen species |
| RNS | reactive nitrogen species |
| TBARS | thiobarbituric acid-reactive substance |
References
- Bodzin, A.S.; Busuttil, R.W. Hepatocellular carcinoma: Advances in diagnosis, management, and long term outcome. World J. Hepatol. 2015, 7, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Misas, M.; Rodríguez-Perálvarez, M.; de la Mata, M. Strategies to improve outcome of patients with hepatocellular carcinoma receiving a liver transplantation. World J. Hepatol. 2015, 7, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Slotta, J.E.; Kollmar, O.; Ellenrieder, V.; Ghadimi, B.M.; Homayounfar, K. Hepatocellular carcinoma: Surgeon’s view on latest findings and future perspectives. World J. Hepatol. 2015, 7, 1168–1183. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, A.I.; Waked, I. Recent advances in multidisciplinary management of hepatocellular carcinoma. World J. Hepatol. 2015, 7, 673–687. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.; Maximin, S.; Meier, J.; Pokharel, S.; Bhargava, P. Hepatocellular carcinoma: Review of epidemiology, screening, imaging diagnosis, response assessment, and treatment. Curr. Probl. Diagn. Radiol. 2015, 44, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Kumada, T.; Tada, T.; Sone, Y.; Kaneok, Y.; Maeda, A. Tumor markers for hepatocellular carcinoma: Simple and significant predictors of outcome in patients with HCC. Liver Cancer 2015, 4, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Cescon, M.; Bertuzzo, V.R.; Ercolani, G.; Ravaioli, M.; Odaldi, F.; Pinna, A.D. Liver transplantation for hepatocellular carcinoma: Role of inflammatory and immunological state on recurrence and prognosis. World J. Gastroenterol. 2013, 19, 9174–9182. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A.; OLT for HCC Consensus Group. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef]
- Verslype, C.; Rosmorduc, O.; Rougier, P.; ESMO Guidelines Working Group. Hepatocellular carcinoma: ESMO-ESDO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23, vii41–vii48. [Google Scholar] [CrossRef] [PubMed]
- Takaki, A.; Yamamoto, K. Control of oxidative stress in hepatocellular carcinoma: Helpful or harmful? World J. Hepatol. 2015, 7, 968–979. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Corder, N.L.; Koduru, B.; Wang, Y. Oxidative stress and hepatic Nox proteins in chronic hepatitis C and hepatocellular carcinoma. Free Radic. Biol. Med. 2014, 72, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.; Sordelli, I.M.; Lombardi, A.; Lamberti, M.; Tarantino, L.; Giudice, A.; Stiuso, P.; Abbruzzese, A.; Sperlongano, R.; Accardo, M.; et al. Molecular targets and oxidative stress biomarkers in hepatocellular carcinoma: An overview. J. Transl. Med. 2011, 9, 171. [Google Scholar] [CrossRef] [PubMed]
- Hoshida, Y. Molecular signatures and prognosis of hepatocellular carcinoma. Minerva Gastroenterol. Dietol. 2011, 57, 311–322. [Google Scholar] [PubMed]
- Draper, H.H.; Hadley, M. Malondialdehyde determination as index of lipid peroxidation. Methods Enzymol. 1990, 186, 421–431. [Google Scholar] [PubMed]
- Dalle-Donne, I.; Rossi, R.; Colombo, R.; Giustarini, D.; Milzani, A. Biomarkers of oxidative damage in human disease. Clin. Chem. 2006, 52, 601–623. [Google Scholar] [CrossRef] [PubMed]
- Yahya, R.S.; Ghanem, O.H.; Foyouh, A.A.; Atwa, M.; Enany, S.A. Role of interleukin-8 and oxidative stress in patients with hepatocellular carcinoma. Clin. Lab. 2013, 59, 969–976. [Google Scholar] [PubMed]
- Zhao, J.; Zhao, Y.; Wang, H.; Gu, X.; Ji, J.; Gao, C. Association between metabolic abnormalities and HBV related hepatocelluar carcinoma in Chinese: A cross-sectional study. Nutr. J. 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.M.; Lin, S.K.; Lee, K.T.; Hsiao, J.K.; Huang, J.C.; Wu, S.H.; Ma, H.; Wu, S.H.; Tsai, L.Y. Evaluation of redox statuses in patients with hepatitis B virus-associated hepatocellular carcinoma. Ann. Clin. Biochem. 2009, 46, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Czeczot, H.; Scibior, D.; Skrzycki, M.; Podsiad, M. Glutathione and GSH-dependent enzymes in patients with liver cirrhosis and hepatocellular carcinoma. Acta Biochim. Pol. 2006, 53, 237–242. [Google Scholar] [PubMed]
- Trevisani, F.; Caraceni, P.; Simoncini, M.; Micati, M.; Domenicali, M.; Dazzani, F.; Zambruni, A.; Stefanelli, C.; Grazi, G.; Nardo, B.; et al. Evidence of oxidative imbalance in long-term liver transplant patients. Dig. Liver Dis. 2002, 34, 279–284. [Google Scholar] [CrossRef]
- Thorat, V.N.; Suryakar, A.N.; Naik, P.; Tiwale, B.M. Total antioxidant capacity and lipid peroxidation in liver transplantation. Indian J. Clin. Biochem. 2009, 24, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Váli, L.; Hahn, O.; Kupcsulik, P.; Drahos, A.; Sárváry, E.; Szentmihályi, K.; Pallai, Z.; Kurucz, T.; Sípos, P.; Blázovics, A. Oxidative stress with altered element content and decreased ATP level of erythrocytes in hepatocellular carcinoma and colorectal liver metastases. Eur. J. Gastroenterol. Hepatol. 2008, 20, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Teng, F.; Wang, G.H.; Tao, Y.F.; Guo, W.Y.; Wang, Z.X.; Ding, G.S.; Shi, X.M.; Fu, Z.R. Criteria-specific long-term survival prediction model for hepatocellular carcinoma patients after liver transplantation. World J. Gastroenterol. 2014, 20, 10900–10907. [Google Scholar] [CrossRef] [PubMed]
- Dumitra, S.; Salleh, I.; Alabbad, S.I.; Barkun, J.S.; Dumitra, T.C.; Coutsinos, D.; Metrakos, P.P.; Hassanain, M.; Paraskevas, S.; Chaudhury, P.; et al. Hepatitis C infection and hepatocellular carcinoma in liver transplantation: A 20-year experience. HPB 2013, 15, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Martínez Ares, D.; Suárez López, F.J.; Souto Ruzo, J.; Otero Ferreiro, A.; Gómez Gutiérrez, M.; González Conde, B.; Fernández Sellés, C.; Gala López, B.; Arnal Monreal, F.; Vázquez Iglesias, J.L. Liver transplantation in patients with hepatocellular carcinoma: Factors implicated in tumor relapse. Rev. Esp. Enferm. Dig. 2004, 96, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, M.; Shirabe, K.; Facciuto, M.E.; Schwartz, M.E.; Florman, S.S.; Yoshizumi, T.; Harimoto, N.; Ikegami, T.; Uchiyama, H.; Maehara, Y. Comparative study of living and deceased donor liver transplantation as a treatment for hepatocellular carcinoma. J. Am. Coll. Surg. 2015, 220, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Imai, K.; Takai, K.; Hanai, T.; Hayashi, H.; Naiki, T.; Nishigaki, Y.; Tomita, E.; Shimizu, M.; Moriwaki, H. Hepatocellular carcinoma patients with increased oxidative stress levels are prone to recurrence after curative treatment: A prospective case series study using the d-ROM test. J. Cancer Res. Clin. Oncol. 2013, 139, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhou, X.S.; Geng, Q.M. Evaluation oxygen free radicals related index before liver transplantation to forejudge prognosis. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2003, 15, 560–562. [Google Scholar] [PubMed]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Lorenzo, J.M.; Molina, I.; Jiménez, A. Association between serum malondialdehyde levels and mortality in patients with severe brain trauma injury. J. Neurotrauma 2015, 32, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Riaño-Ruiz, M.; Jiménez, A. Serum malondialdehyde levels in patients with malignant middle cerebral artery infarction are associated with mortality. PLoS ONE 2015, 10, e0125893. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Domínguez-Rodríguez, A.; Labarta, L.; Díaz, C.; Solé-Violán, J.; Ferreres, J.; Borreguero-León, J.M.; Jiménez, A.; et al. Prognostic value of malondialdehyde serum levels in severe sepsis: A multicenter study. PLoS ONE 2013, 8, e53741. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Domínguez-Rodriguez, A.; Labarta, L.; Díaz, C.; Solé-Violán, J.; Ferreres, J.; Cabrera, J.; Igeño, J.C.; et al. Sustained high serum malondialdehyde levels are associated with severity and mortality in septic patients. Crit. Care 2013, 17. [Google Scholar] [CrossRef] [PubMed]
- Varona, M.A.; Del Pino, J.M.; Barrera, M.; Arranz, J.; Hernández, B.M.; Perez, H.F.; Padilla, J.; Fuentes, J.S.; Aguirre, A.; Mendez, S.; et al. Hepatocellular carcinoma and liver transplantation: A 12-year experience. Transpl. Proc. 2009, 41, 1005–1008. [Google Scholar] [CrossRef] [PubMed]
- Varona, M.A.; Soriano, A.; Aguirre-Jaime, A.; Garrido, S.; Oton, E.; Diaz, D.; Portero, J.; Bravo, P.; Barrera, M.A.; Perera, A. Risk factors of hepatocellular carcinoma recurrence after liver transplantation: Accuracy of the α-fetoprotein model in a single-center experience. Transpl. Proc. 2015, 47, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Sener, G.; Toklu, H.; Kapucu, C.; Ercan, F.; Erkanli, G.; Kaçmaz, A.; Tilki, M.; Yeğen, B.C. Melatonin protects against oxidative organ injury in a rat model of sepsis. Surg. Today 2005, 35, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Vico, A.; Lardone, P.J.; Naji, L.; Fernández-Santos, J.M.; Martín-Lacave, I.; Guerrero, J.M.; Calvo, J.R. Beneficial pleiotropic actions of melatonin in an experimental model of septic shock in mice: Regulation of pro-/anti-inflammatory cytokine network, protection against oxidative damage and anti-apoptotic effects. J. Pineal Res. 2005, 39, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Lowes, D.A.; Webster, N.R.; Murphy, M.P.; Galley, H.F. Antioxidants that protect mitochondria reduce interleukin-6 and oxidative stress, improve mitochondrial function, and reduce biochemical markers of organ dysfunction in a rat model of acute sepsis. Br. J. Anaesth. 2013, 110, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Paskaloğlu, K.; Sener, G.; Kapucu, C.; Ayanoğlu-Dülger, G. Melatonin treatment protects against sepsis-induced functional and biochemical changes in rat ileum and urinary bladder. Life Sci. 2004, 74, 1093–1104. [Google Scholar] [CrossRef] [PubMed]
- Kerman, M.; Cirak, B.; Ozguner, M.F.; Dagtekin, A.; Sutcu, R.; Altuntas, I.; Delibas, N. Does melatonin protect or treat brain damage from traumatic oxidative stress? Exp. Brain Res. 2005, 163, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Horakova, L.; Onrejickova, O.; Barchrrata, K.; Vajdova, M. Preventive effect of several antioxidants after oxidative stress on rat brain homogenates. Gen. Physiol. Biophys. 2000, 19, 195–205. [Google Scholar] [PubMed]
- Ozsüer, H.; Görgülü, A.; Kiriş, T.; Cobanoğlu, S. The effects of memantine on lipid peroxidation following closed-head trauma in rats. Neurosurg. Rev. 2005, 28, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Fulia, F.; Gitto, E.; Cuzzocrea, S.; Reiter, R.J.; Dugo, L.; Gitto, P.; Barberi, S.; Cordaro, S.; Barberi, I. Increased levels of malondialdehyde and nitrite/nitrate in the blood of asphyxiated newborns: Reduction by melatonin. J. Pineal Res. 2001, 31, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Gitto, E.; Karbownik, M.; Reiter, R.J.; Tan, D.X.; Cuzzocrea, S.; Chiurazzi, P.; Cordaro, S.; Corona, G.; Trimarchi, G.; Barberi, I. Effects of melatonin treatment in septic newborns. Pediatr. Res. 2001, 50, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Sahib, A.S.; Al-Jawad, F.H.; Alkaisy, A.A. Effect of antioxidants on the incidence of wound infection in burn patients. Ann. Burns Fire Dis. 2010, 23, 199–205. [Google Scholar]
- Ullegaddi, R.; Powers, H.J.; Gariballa, S.E. B-group vitamin supplementation mitigates oxidative damage after acute ischaemic stroke. Clin. Sci. 2004, 107, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Ullegaddi, R.; Powers, H.J.; Gariballa, S.E. Antioxidant supplementation enhances antioxidant capacity and mitigates oxidative damage following acute ischaemic stroke. Eur. J. Clin. Nutr. 2005, 59, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Ullegaddi, R.; Powers, H.J.; Gariballa, S.E. Antioxidant supplementation with or without B-group vitamins after acute ischemic stroke: A randomized controlled trial. J. Parent. Enter. Nutr. 2006, 30, 108–114. [Google Scholar] [CrossRef]
- Saniova, B.; Drobny, M.; Lehotsky, J.; Sulaj, M.; Schudichova, J. Biochemical and clinical improvement of cytotoxic state by amantadine sulphate. Cell. Mol. Neurobiol. 2006, 26, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Kikugawa, K.; Kojima, T.; Yamaki, S.; Kosugi, H. Interpretation of the thiobarbituric acid reactivity of rat liver and brain homogenates in the presence of ferric ion and ethylediaminotetraacetic acid. Anal. Biochem. 1992, 202, 249–255. [Google Scholar] [CrossRef]
- Youden, W.J. An index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Healthy Controls (n = 80) | HCC Patients (n = 127) | p-Value |
|---|---|---|---|
| Female gender—n (%) | 18 (22.5) | 20 (15.7) | 0.27 |
| Age—median years (P25–P75) | 56 (46–68) | 58 (52–62) | 0.71 |
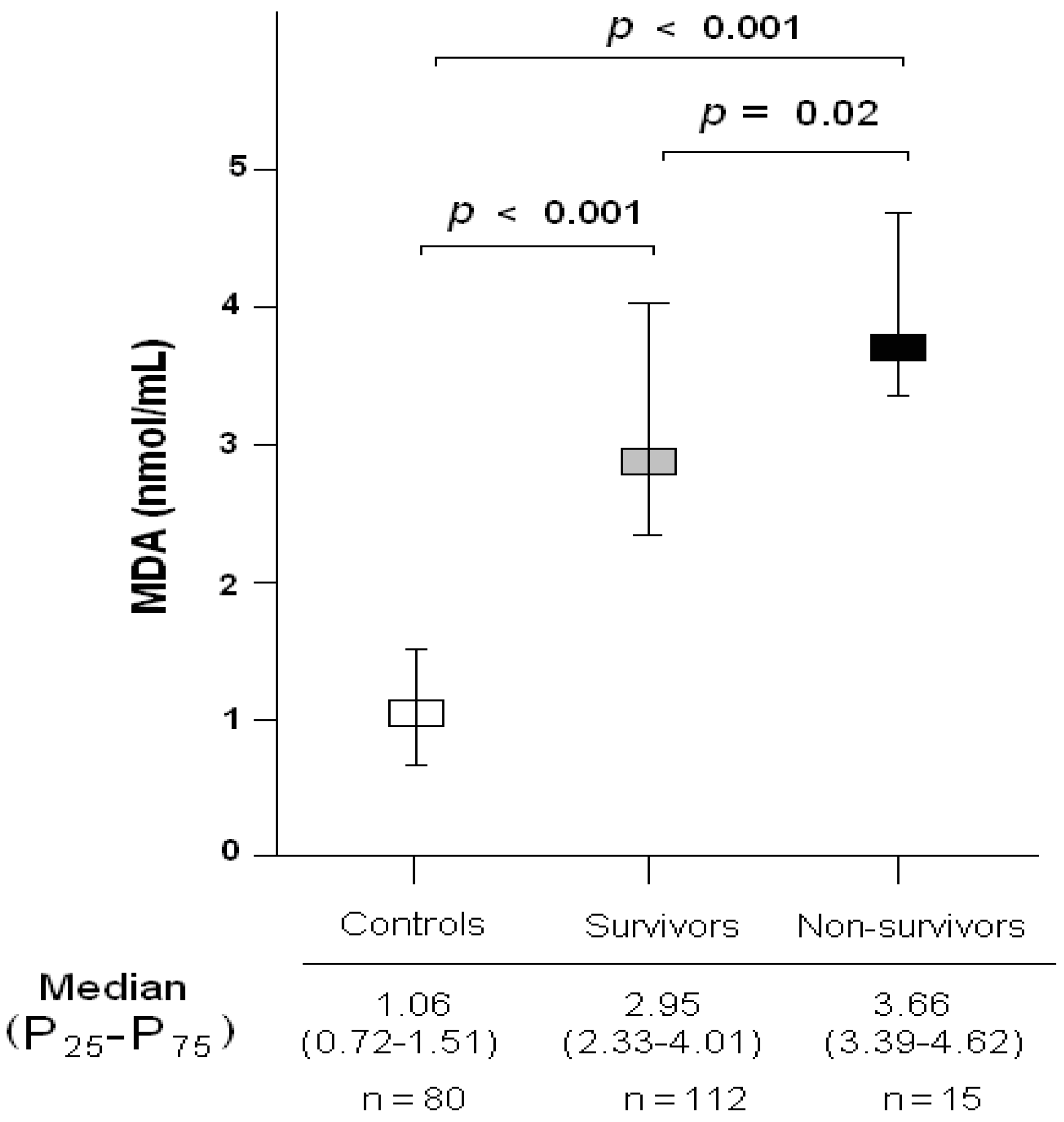
| Serum malondialdehyde levels (nmol/mL)—median (P25–P75) | 1.06 (0.72–1.51) | 3.11 (2.39–4.17) | <0.001 |
| Demographic and Clinical Characteristics | Survivors at 1 Year (n = 112) | Non-Survivors at 1 Year (n = 15) | p-Value |
|---|---|---|---|
| Female gender—n (%) | 20 (17.9) | 0 | 0.13 |
| Age (years)—median (P25–P75) | 58 (52–62) | 56 (53–62) | 0.84 |
| Age of liver donor (years)—median (P25–P75) | 52 (36–63) | 62 (49–72) | 0.02 |
| ABO blood type—n (%) | |||
| A | 53 (47.3) | 6 (40.0) | 0.87 |
| B | 9 (8.0) | 2 (13.3) | |
| O | 45 (40.2) | 6 (40.0) | |
| AB | 5 (4.5) | 1 (6.7) | |
| Child-Pugh score—n (%) | |||
| A | 54 (48.2) | 10 (66.7) | 0.41 |
| B | 35 (31.3) | 3 (20.0) | |
| C | 23 (20.5) | 2 (13.3) | |
| MELD score—median (P25–P75) | 15 (11–18) | 15 (15–18) | 0.44 |
| Inside Milan criteria previously to LT—n (%) | 107 (95.5) | 14 (93.3) | 0.54 |
| Inside Milan criteria after LT—n (%) | 94 (83.9) | 11 (73.3) | 0.16 |
| Serum AFP (ng/dL)—median (P25–P75) | 8.0 (4.0–32.0) | 12.0 (4.8–164.9) | 0.42 |
| Portal hypertension—n (%) | 78 (69.6) | 11 (73.3) | 0.99 |
| Multinodular tumor—n (%) | 34 (30.4) | 5 (33.3) | 0.77 |
| Nodule size (cm)—median (P25–P75) | 3.0 (2.0–3.5) | 3.2 (1.7–4.6) | 0.83 |
| Degree of tumor differentiation—n (%) | |||
| Well | 84 (75.0) | 12 (80.0) | 0.55 |
| Moderate | 25 (22.3) | 2 (13.3) | |
| Poor | 3 (2.7) | 1 (6.7) | |
| Infiltration—n (%) | 36 (32.1) | 4 (26.7) | 0.77 |
| Microvascular invasion—n (%) | 24 (21.4) | 3 (20.0) | 0.99 |
| Macrovascular invasion—n (%) | 6 (5.4) | 0 | 0.99 |
| Treatment prior to LT—n (%) | 61 (54.1) | 10 (66.7) | 0.42 |
| Transplantation technique—n (%) | |||
| By-pass | 43 (38.4) | 6 (40.0) | 0.99 |
| Piggy back | 69 (61.6) | 9 (60.0) | |
| Serum MDA (nmol/mL)—median (P25–P75) | 2.95 (2.33–4.01) | 3.66 (3.39–4.62) | 0.02 |
| Predictors | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
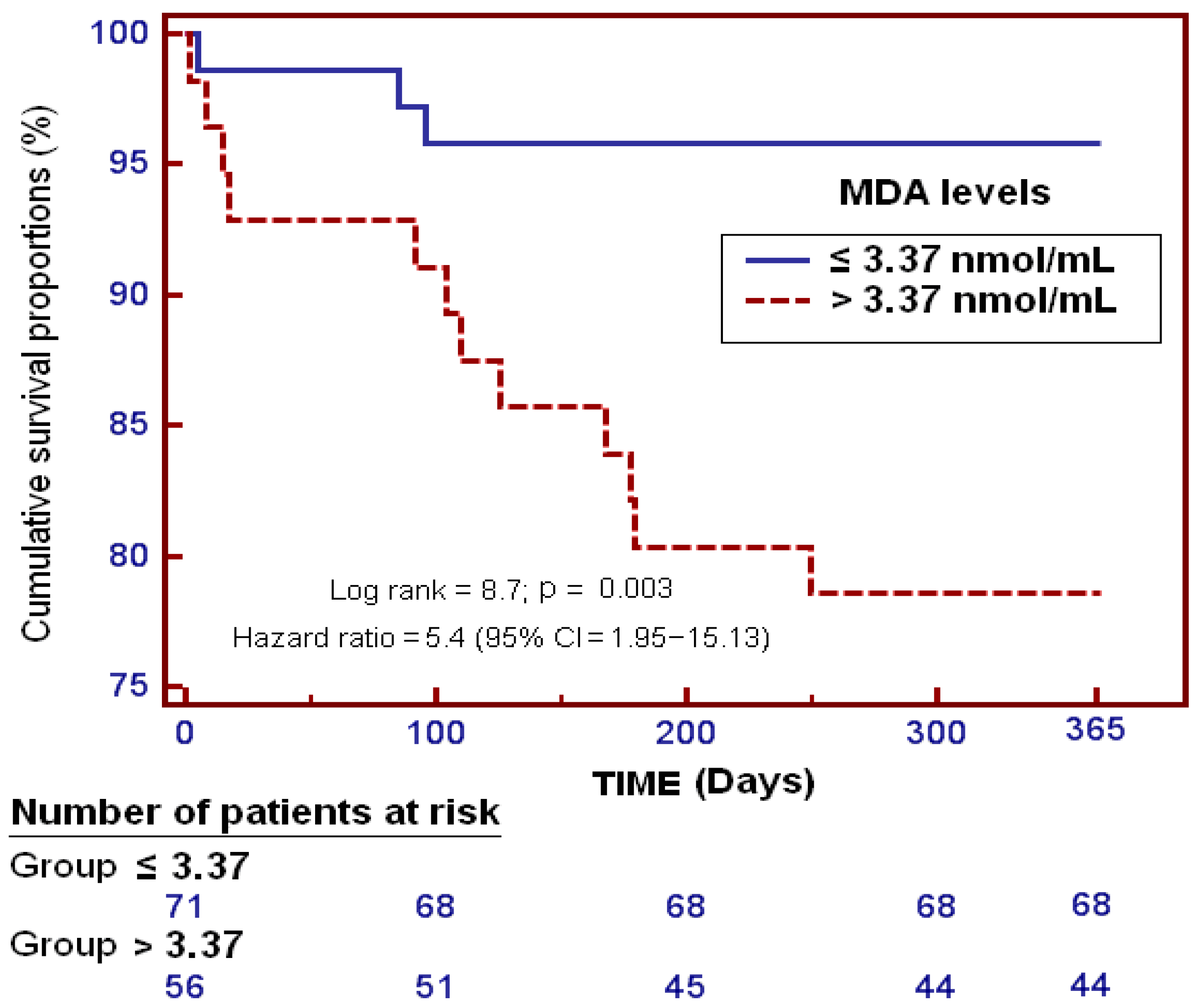
| Serum MDA levels > 3.37 nmol/mL | 5.38 | 1.580–infinite | 0.007 |
| Age of liver donor (age) | 1.04 | 1.003–infinite | 0.04 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorente, L.; Rodriguez, S.T.; Sanz, P.; Abreu-González, P.; Díaz, D.; Moreno, A.M.; Borja, E.; Martín, M.M.; Jiménez, A.; Barrera, M.A. Association between Pre-Transplant Serum Malondialdehyde Levels and Survival One Year after Liver Transplantation for Hepatocellular Carcinoma. Int. J. Mol. Sci. 2016, 17, 500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17040500
Lorente L, Rodriguez ST, Sanz P, Abreu-González P, Díaz D, Moreno AM, Borja E, Martín MM, Jiménez A, Barrera MA. Association between Pre-Transplant Serum Malondialdehyde Levels and Survival One Year after Liver Transplantation for Hepatocellular Carcinoma. International Journal of Molecular Sciences. 2016; 17(4):500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17040500
Chicago/Turabian StyleLorente, Leonardo, Sergio T. Rodriguez, Pablo Sanz, Pedro Abreu-González, Dácil Díaz, Antonia M. Moreno, Elisa Borja, María M. Martín, Alejandro Jiménez, and Manuel A. Barrera. 2016. "Association between Pre-Transplant Serum Malondialdehyde Levels and Survival One Year after Liver Transplantation for Hepatocellular Carcinoma" International Journal of Molecular Sciences 17, no. 4: 500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17040500