
MicroRNA in United Airway Diseases

Abstract
:
{kind=link}
{kind=link}
1. Introduction
2. MicroRNA Expression in Patients with Coexistence of AR and Asthma
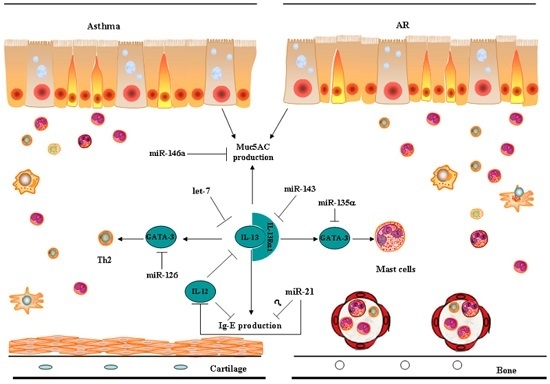
3. MicroRNAs in Common Inflammatory Processes of UAD
4. MicroRNA Profiling in UAD
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Passalacqua, G.; Ciprandi, G.; Canonica, G.W. The nose-lung interaction: United airways disease. Curr. Opin. Allergy Clin. Immunol. 2001, 1, 7–14. [Google Scholar] [PubMed]
- Compalati, E.; Ridolo, E.; Passalacqua, G.; Braido, F.; Villa, E.; Canonica, G.W. The link between allergic rhinitis and asthma: The united airways disease. Expert Rev. Clin. Immunol. 2010, 6, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Simons, F.E. Allergic rhinobronchitis: The asthma-allergic rhinitis link. J. Allergy Clin. Immunol. 1994, 104, 534–540. [Google Scholar] [CrossRef]
- Shi, J.B.; Fu, Q.L.; Zhang, H.; Cheng, L.; Wang, Y.J.; Zhu, D.D.; Lv, W.; Liu, S.X.; Li, P.Z.; Ou, C.Q.; et al. Epidemiology of chronic rhinosinusitis: Results from a cross-sectional survey in seven Chinese cities. Allergy 2015, 70, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.L.; Pattemore, P.K.; Sanderson, G.; Smith, S.; Campbell, M.J.; Josephs, L.K.; Cunningham, A.; Robinson, B.S.; Myint, S.H.; Ward, M.E.; et al. The relationship between upper respiratory infections and hospital admissions for asthma: A time-trend analysis. Am. J. Respir. Crit. Care Med. 1996, 154, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Fuhlbrigge, A.L.; Finkelstein, J.A.; Weiss, S.T. Intranasal steroids and the risk of emergency department visits for asthma. J. Allergy Clin. Immunol. 2002, 109, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Crystal-Peters, J.; Neslusan, C.; Crown, W.H.; Torres, A. Treating allergic rhinitis in patients with comorbid asthma: The risk of asthma-related hospitalizations and emergency department visits. J. Allergy Clin. Immunol. 2002, 109, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.H.; Zuo, K.J.; Guo, Y.B.; Li, Z.P.; Xu, G.; Xu, R.; Shi, J.B. Long-term results of endoscopic sinus surgery-oriented treatment for chronic rhinosinusitis with asthma. Laryngoscope 2014, 124, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, H.H.; Rotirot, G. Allergic rhinitis, chronic rhinosinusitis and asthma, unravelling a complex relationship. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Hutvágner, G.; Zamore, P.D. A microRNA in a multiple-turnover RNAi enzyme complex. Science 2002, 297, 2056–2060. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs, Target recognition and regulatory functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef] [PubMed]
- Kawaji, H.; Hayashizaki, Y. Exploration of small RNAs. PLoS Genet. 2008, 4, e22. [Google Scholar] [CrossRef] [PubMed]
- Bushati, N.; Cohen, S.M. MicroRNA functions. Annu. Rev. Cell Dev. Biol. 2007, 23, 175–205. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.X.; Rothenberg, M.E. Diagnostic, functional, and therapeutic roles of microRNA in allergic diseases. J. Allergy Clin. Immunol. 2013, 132, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Rebane, A.; Akdis, C.A. MicroRNAs in allergy and asthma. Curr. Allergy Asthma Rep. 2014, 14, 424. [Google Scholar] [CrossRef] [PubMed]
- Long, X.B.; Sun, G.B.; Hu, S.; Liang, G.T.; Wang, N.; Zhang, X.H.; Cao, P.P.; Zhen, H.T.; Cui, Y.H.; Liu, Z. Let-7a microRNA functions as a potential tumor suppressor in human laryngeal cancer. Oncol. Rep. 2009, 22, 1189–1195. [Google Scholar] [PubMed]
- Li, T.; Leong, M.H.; Harms, B.; Kennedy, G.; Chen, L. MicroRNA-21 as a potential colon and rectal cancer biomarker. World J. Gastroenterol. 2013, 19, 5615–5621. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.L.; Chen, H.Y.; Chang, G.C.; Chen, C.Y.; Chen, H.W.; Singh, S.; Cheng, C.L.; Yu, C.J.; Lee, Y.C.; Chen, H.S.; et al. MicroRNA signature predicts survival and relapse in lung cancer. Cell 2008, 13, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Panganiban, R.; Wang, Y.; Howrylak, J.; Chinchilli, M.; Craig, T.; August, A.; Ishmael, F. Circulating microRNAs as biomarkers in patients with allergic rhinitis and asthma. J. Allergy Clin. Immunol. 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Ahmad, T.; Sharma, A.; Mabalirajan, U.; Kulshreshtha, A.; Agrawal, A.; Ghosh, B. Let-7 microRNA-mediated regulation of IL-13 and allergic airway inflammation. J. Allergy Clin. Immunol. 2011, 128, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Suojalehto, H.; Lindström, I.; Majuri, M.L.; Mitts, C.; Karjalainen, J.; Wolff, H.; Alenius, H. Altered microRNA expression of nasal mucosa in long-term asthma and allergic rhinitis. Int. Arch. Allergy Immunol. 2014, 163, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Suojalehto, H.; Toskala, E.; Kilpeläinen, M.; Majuri, M.L.; Mitts, C.; Lindström, I.; Puustinen, A.; Plosila, T.; Sipilä, J.; Wolff, H.; et al. MicroRNA profiles in nasal mucosa of patients with allergic and nonallergic rhinitis and asthma. Int. Forum Allergy Rhinol. 2013, 3, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.H.; Zhang, Y.N.; Liu, Z. MicroRNA in chronic rhinosinusitis and allergic rhinitis. Curr. Allergy Asthma Rep. 2014, 14, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.F.; Huang, H.C.; Ou, C.Y.; Hsu, T.Y.; Chuang, H.; Chang, J.C.; Wang, L.; Kuo, H.C.; Yang, K.D. MicroRNA-21 expression in neonatal blood associated with antenatal immunoglobulin E production and development of allergic rhinitis. Clin. Exp. Allergy 2010, 40, 1482–1490. [Google Scholar] [CrossRef] [PubMed]
- Salib, R.J.; Kumar, S.; Wilson, S.J.; Howarth, P.H. Nasal mucosal immunoexpression of the mast cell chemoattractants TGF-β, eotaxin, and stem cell factor and their receptors in allergic rhinitis. J. Allergy Clin. Immunol. 2004, 114, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.X.; Munitz, A.; Rothenberg, M.E. MicroRNA-21 is up-regulated in allergic airway inflammation and regulates IL-12p35 expression. J. Immunol. 2009, 182, 4994–5002. [Google Scholar] [CrossRef] [PubMed]
- Shaoqing, Y.; Ruxin, Z.; Guojun, L.; Zhiqiang, Y.; Hua, H.; Shudong, Y.; Jie, Z. Microarray analysis of differentially expressed microRNAs in allergic rhinitis. Am. J. Rhinol. Allergy 2011, 25, e242–e246. [Google Scholar] [CrossRef] [PubMed]
- Teng, Y.; Zhang, R.; Liu, C.; Zhou, L.; Wang, H.; Zhuang, W.; Huang, Y.; Hong, Z. miR-143 inhibits interleukin-13-induced inflammatory cytokine and mucus production in nasal epithelial cells from allergic rhinitis patients by targeting IL13Rα1. Biochem. Biophys. Res. Commun. 2015, 457, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Mayoral, R.J.; Deho, L.; Rusca, N.; Bartonicek, N.; Saini, H.K.; Enright, A.J.; Monticelli, S. miR-221 influences effector functions and actin cytoskeleton in mast cells. PLoS ONE 2011, 6, e26133. [Google Scholar] [CrossRef] [PubMed]
- Rusca, N.; Deho, L.; Montagner, S.; Zielinski, C.E.; Sica, A.; Sallusto, F.; Monticelli, S. MiR-146a and NF-κB regulate mast cell survival and T lymphocyte differentiation. Mol. Cell. Biol. 2012, 32, 4432–4444. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.Q.; Yang, Y.Q.; Wang, S.B.; Li, F.; Liu, M.Z.; Hua, Q.Q.; Tao, Z.Z. Intranasal administration of lentiviral miR-135a regulates mast cell and allergen-induced inflammation by targeting GATA-3. PLoS ONE 2015, 10, e0139322. [Google Scholar] [CrossRef] [PubMed]
- Mattes, J.; Collison, A.; Plank, M.; Phipps, S.; Foste, P.S. Antagonism of microRNA-126 suppresses the effector function of TH2 cells and the development of allergic airways disease. Proc. Natl. Acad. Sci. USA 2009, 106, 18704–18709. [Google Scholar] [CrossRef]
- Zhong, T.; Perelman, J.M.; Kolosov, V.P.; Zhou, X.D. miR-146a negatively regulates neutrophil elastase-induced MUC5AC secretion from 16HBE human bronchial epithelial cells. Mol. Cell. Biochem. 2011, 358, 249–255. [Google Scholar] [CrossRef]
- Luo, X.; Hong, H.; Tang, J.; Wu, X.; Lin, Z.; Ma, R.; Fan, Y.; Xu, G.; Liu, D.; Li, H. Increased expression of miR-146a in children with allergic rhinitis after allergen-specific immunotherapy. Allergy Asthma Immunol. Res. 2016, 8, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, C.; Cheng, H.; Tewari, M. MicroRNA profiling: Approaches and considerations. Nat. Rev. Genet. 2012, 13, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Antón, A.; Mullol, J. MicroRNA: Endotyping united airways. Int. Arch. Allergy Immunol. 2014, 164, 10–12. [Google Scholar] [CrossRef] [PubMed]

© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Z.; Zhang, X.-H.; Callejas-Díaz, B.; Mullol, J. MicroRNA in United Airway Diseases. Int. J. Mol. Sci. 2016, 17, 716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17050716
Liu Z, Zhang X-H, Callejas-Díaz B, Mullol J. MicroRNA in United Airway Diseases. International Journal of Molecular Sciences. 2016; 17(5):716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17050716
Chicago/Turabian StyleLiu, Zheng, Xin-Hao Zhang, Borja Callejas-Díaz, and Joaquim Mullol. 2016. "MicroRNA in United Airway Diseases" International Journal of Molecular Sciences 17, no. 5: 716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17050716