
Assessment of Dextran Antigenicity of Intravenous Iron Preparations with Enzyme-Linked Immunosorbent Assay (ELISA)

Abstract
:1. Introduction
2. Results
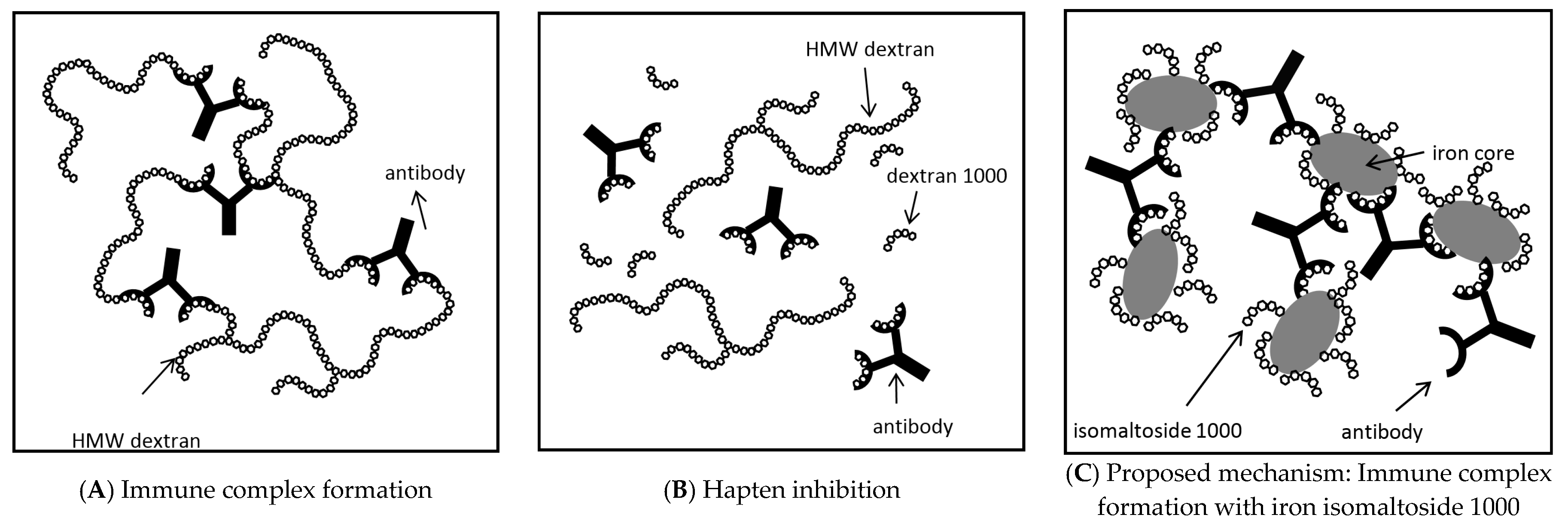
3. Discussion
4. Materials and Methods
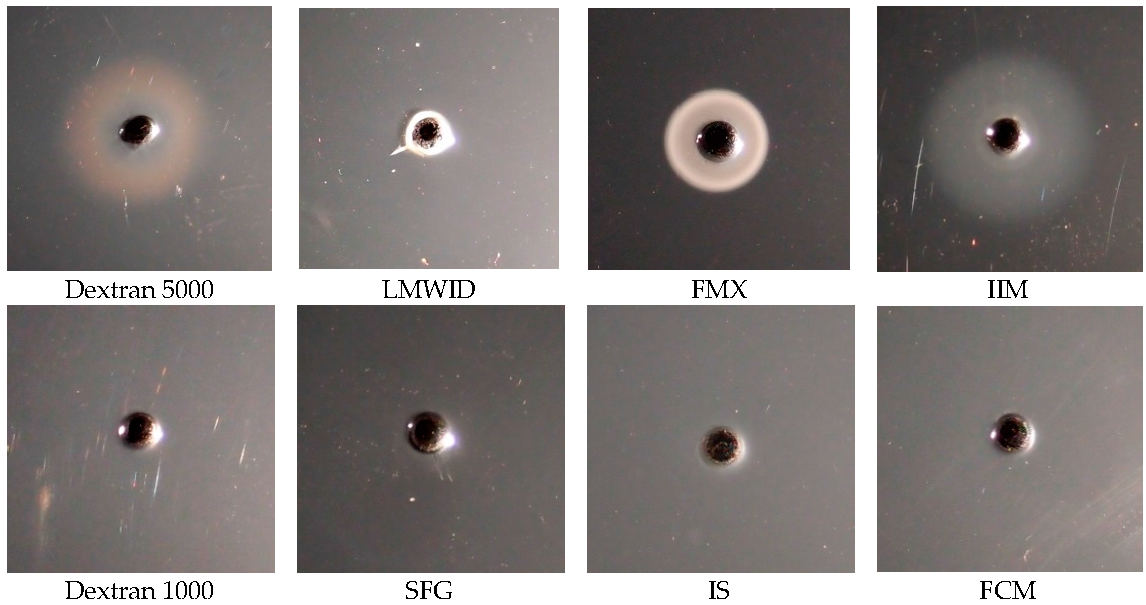
4.1. Reverse Single Radial Immunodiffusion Assay
4.2. Indirect Enzyme-Linked Immunosorbent Assay (ELISA)
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Anderson, G.J.; Wang, F. Essential but toxic: Controlling the flux of iron in the body. Clin. Exp. Pharmacol. Physiol. 2012, 39, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Koskenkorva-Frank, T.S.; Weiss, G.; Koppenol, W.H.; Burckhardt, S. The complex interplay of iron metabolism, reactive oxygen and reactive nitrogen species: Insights into the potential of different iron therapies to induce oxidative and nitrosative stress. Free Radic. Biol. Med. 2013, 65, 1174–1194. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T. Systemic iron homeostasis. Physiol. Rev. 2013, 93, 1721–1741. [Google Scholar] [CrossRef] [PubMed]
- Crichton, R.R.; Danielson, B.G.; Geisser, P. Iron Therapy with Special Emphasis on Intravenous Administration, 4th ed.; UNI-MED: Bremen, Germany, 2008. [Google Scholar]
- Kudasheva, S.; Lai, J.; Ulman, A.; Cowman, M.K. Structure of carbohydrate-bound polynuclear iron oxyhydroxide nanoparticles in parenteral formulations. J. Inorg. Chem. 2004, 98, 1757–1769. [Google Scholar] [CrossRef] [PubMed]
- Mühlebach, S.; Borchard, G.; Yildiz, S. Regulatory challenges and approaches to characterize nanomedicines and their follow-on similars. Nanomedicine 2015, 10, 659–674. [Google Scholar] [CrossRef] [PubMed]
- Breymann, C. Iron Deficiency and Anaemia in Women in the Gynaecological and Obstetrical Practice (with Case Reports), 1st ed.; UNI-MED: Bremen, Germany, 2015. [Google Scholar]
- Jahn, M.R.; Andreasen, H.B.; Fütterer, S.; Nawroth, T.; Schünemann, V.; Kolb, U.; Hofmeister, W.; Muñoz, M.; Bock, K.; Meldal, M.; et al. A comparative study of the physicochemical properties of iron isomaltoside 1000 (Monofer), a new intravenous iron preparation and its clinical implications. Eur. J. Pharm. Biopharm. 2011, 78, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Neiser, S.; Rentsch, D.; Dippon, U.; Kappler, A.; Weidler, P.G.; Gottlicher, J.; Steininger, R.; Wilhelm, M.; Braitsch, M.; Funk, F.; et al. Physico-chemical properties of the new generation IV iron preparations ferumoxytol, iron isomaltoside 1000 and ferric carboxymaltose. Biometals 2015, 28, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Neiser, S.; Wilhelm, M.; Schwarz, K.; Funk, F.; Geisser, P.; Burckhardt, S. Assessment of dextran antigenicity of intravenous iron products by an immunodiffusion assay. Port J. Nephrol. Hypertens. 2011, 25, 219–224. [Google Scholar]
- Ring, J.; Valenta, R. Letter to the Editor on the article “Assessment of dextran antigenicity of intravenous iron products by an immunodiffusion assay”. Port. J. Nephrol. Hypertens. 2012, 26, 308–312. [Google Scholar]
- Neiser, S.; Schwarz, K.; Wilhelm, M.; Funk, F.; Geisser, P.; Burckhardt, S. Reply to the letter to the editor by Johannes Ring and Rudi Valenta on the article “Assessment of dextran antigenicity of intravenous iron products by an immunodiffusion assay”. Port. J. Nephrol. Hypertens. 2012, 26, 308–312. [Google Scholar]
- Szebeni, J.; Fishbane, S.; Hedenus, M.; Howaldt, S.; Locatelli, F.; Patni, S.; Rampton, D.; Weiss, G.; Folkersen, J. Hypersensitivity to intravenous iron: Classification, terminology, mechanisms and management. Br. J. Pharmacol. 2015, 172, 5025–5036. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Mason, P.D.; Vaage-Nilsen, O.; Ahlmen, J. Update on adverse drug events associated with parenteral iron. Nephrol. Dial. Transplant. 2006, 21, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Graham, D.J.; Kane, R.C.; Xie, D.; Wernecke, M.; Levenson, M.; MaCurdy, T.E.; Houstoun, M.; Ryan, Q.; Wong, S.; et al. Comparative Risk of Anaphylactic Reactions Associated With Intravenous Iron Products. JAMA 2015, 314, 2062–2068. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, M.; Macdougall, I.C. Safety of intravenous iron formulations: facts and folklore. Blood Transfus. 2014, 12, 296–300. [Google Scholar] [PubMed]
- Rodgers, G.M.; Auerbach, M.; Cella, D.; Chertow, G.M.; Coyne, D.W.; Glaspy, J.A.; Henry, D.H. High-molecular weight iron dextran: a wolf in sheep’s clothing? J. Am. Soc. Nephrol. 2008, 19, 833–834. [Google Scholar] [CrossRef] [PubMed]
- Demoly, P.; Lebel, B.; Messaad, D.; Sahla, H.; Rongier, M.; Daures, J.P.; Godard, P.; Bousquet, J. Predictive capacity of histamine release for the diagnosis of drug allergy. Allergy 1999, 54, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Fleming, L.W.; Stewart, W.K.; Parratt, D. Dextran antibodies, complement conversion and circulating immune complexes after intravenous iron dextran therapy in dialysed patients. Nephrol. Dial. Transplant. 1992, 7, 35–39. [Google Scholar] [PubMed]
- Novey, H.S.; Pahl, M.; Haydik, I.; Vaziri, N.D. Immunologic studies of anaphylaxis to iron dextran in patients on renal dialysis. Ann. Allergy 1994, 72, 224–228. [Google Scholar] [PubMed]
- Getzen, J.H.; Speiggle, W. Anaphylactic reaction to dextran. A case report. Arch. Intern. Med. 1963, 112, 168–170. [Google Scholar] [CrossRef] [PubMed]
- Kraft, D.; Hedin, H.; Richter, W.; Scheiner, O.; Rumpold, H.; Devey, M.E. Immunoglobulin class and subclass distribution of dextran-reactive antibodies in human reactors and non reactors to clinical dextran. Allergy 1982, 37, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.W.; Hedin, H.I. Dextran hypersensitivity. Immunol. Today 1982, 3, 132–138. [Google Scholar] [CrossRef]
- Funk, F.; Ryle, P.; Canclini, C.; Neiser, S.; Geisser, P. The new generation of intravenous iron: Chemistry, pharmacology, and toxicology of ferric carboxymaltose. Arzneimittel-Forschung 2010, 60, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Provenzano, R.; Schiller, B.; Rao, M.; Coyne, D.; Brenner, L.; Pereira, B.J. Ferumoxytol as an intravenous iron replacement therapy in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Cohen, M.H.; Rieves, D.; Pazdur, R. FDA report: Ferumoxytol for intravenous iron therapy in adult patients with chronic kidney disease. Am. J. Hematol. 2010, 85, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Nordfjeld, K.; Andreasen, H.; Thomsen, L.L. Pharmacokinetics of iron isomaltoside 1000 in patients with inflammatory bowel disease. Drug Des. Dev. Ther. 2012, 6, 43–51. [Google Scholar]
- Wikström, B.; Bhandari, S.; Barany, P.; Kalra, P.A.; Ladefoged, S.; Wilske, J.; Thomsen, L.L. Iron isomaltoside 1000: A new intravenous iron for treating iron deficiency in chronic kidney disease. J. Nephrol. 2011, 24, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, P.R.; Bruun, N.E.; Nielsen, O.W.; Pantev, E.; Shiva, F.; Videbaek, L.; Wikström, G.; Thomsen, L.L. Effects of administration of iron isomaltoside 1000 in patients with chronic heart failure. A pilot study. Transfus. Altern. Transfus. Med. 2010, 11, 131–137. [Google Scholar] [CrossRef]
- Singh, A.; Patel, T.; Hertel, J.; Bernardo, M.; Kausz, A.; Brenner, L. Safety of ferumoxytol in patients with anemia and CKD. Am. J. Kidney Dis. 2008, 52, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Spinowitz, B.S.; Kausz, A.T.; Baptista, J.; Noble, S.D.; Sothinathan, R.; Bernardo, M.V.; Brenner, L.; Pereira, B.J. Ferumoxytol for treating iron deficiency anemia in CKD. J. Am. Soc. Nephrol. 2008, 19, 1599–1605. [Google Scholar] [CrossRef] [PubMed]
- Pai, A.B.; Garba, A.O. Ferumoxytol: A silver lining in the treatment of anemia of chronic kidney disease or another dark cloud? J. Blood Med. 2012, 3, 77–85. [Google Scholar] [PubMed]
- Kabat, E.A. The upper limit for the size of the human antidextran combining site. J. Immunol. 1960, 84, 82–85. [Google Scholar] [PubMed]
- Dorner, M.M.; Kabat, E.A. Immunochemical studies on dextrans—VI. Reactivity with antidextran of low molecular weight dextran and its iron-dextran complex (“Imferon”). Immunochemistry 1968, 5, 485–495. [Google Scholar] [CrossRef]
- Bachmann, M.F.; Rohrer, U.H.; Kundig, T.M.; Burki, K.; Hengartner, H.; Zinkernagel, R.M. The influence of antigen organization on B cell responsiveness. Science 1993, 262, 1448–1451. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, M.F.; Zinkernagel, R.M. The influence of virus structure on antibody responses and virus serotype formation. Immunol. Today 1996, 17, 553–558. [Google Scholar] [CrossRef]
- Andreasen, H.B.; Christensen, L. Iron-Dextran Compound for the Use as Component in a Therapeutical Composition for Prophylaxis or Treatment of Iron-Deficiency. U.S. Patent 6,291,440, 18 September 2001. [Google Scholar]
- Medical Products Agency Sweden. Public Assessment Report, Scientific discussion, MonoFer(R) 100 mg/mL Solution for Injection/Infusion (iron(III)isomaltoside 1000). Report No.: SE/H/734/01/DC. 2009. Available online: https://docetp.mpa.se/LMF/Monofer%20solution%20for%20injection%20or%20infusion%20ENG%20PAR.pdf (accessed on 19 July 2016).
- Ljungström, K.G. Safety of dextran in relation to other colloids—Ten years experience with hapten inhibition. Infusionsther. Transfusionsmed. 1993, 20, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Richter, W.; Hedin, H.; Ring, J.; Kraft, D.; Messmer, K. Anaphylaktoide Reaktionen nach Dextran. Allergologie 1980, 3, 51–58. [Google Scholar]
- European Medicines Agency. CHMP Assessment Report Rienso®. Report No.: EMA/CHMP/221776/2012. 2012. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002215/WC500129751.pdf (accessed on 19 July 2016).
- Santosh, S.; Podaralla, P.; Miller, B. Anaphylaxis with elevated serum tryptase after administration of intravenous ferumoxytol. Nephrol. Dial. Transplant. Plus 2010, 3, 341–342. [Google Scholar] [CrossRef] [PubMed]
- Richter, W. Effect of substitution on reactivity of B 512 dextran fractions with anti-B 512 dextran in heterologous passive cutaneous anaphylaxis. Int. Arch. Allergy Appl. Immunol. 1975, 48, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Groman, E.V.; Paul, K.G.; Frigo, T.B.; Bengele, H.; Lewis, J.M. Heat Stable Colloidal Iron Oxides Coated with Reduced Carbohydrates and Carbohydrate Derivatives. U.S. Patent 6,599,498, 29 July 2003. [Google Scholar]
- Simon, G.H.; von Vopelius-Feldt, J.; Fu, Y.; Schlegel, J.; Pinotek, G.; Wendland, M.F.; Chen, M.H.; Daldrup-Link, H.E. Ultrasmall supraparamagnetic iron oxide-enhanced magnetic resonance imaging of antigen-induced arthritis: A comparative study between SHU 555 C, ferumoxtran-10, and ferumoxytol. Investig. Radiol. 2006, 41, 45–51. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Antibody Dilution | 1:1000 b | 1:3000 | 1:9000 | 1:27,000 | 1:81,000 |
|---|---|---|---|---|---|
| LMWID | 17.3 | 15.8 | 14.0 | 11.7 | 8.0 c |
| FMX | 12.7 | 8.7 | 4.4 | 2.2 c | 1.5 |
| IIM | 3.9 | 2.4 c | 1.6 | 1.1 | 1.3 |
| FCM | 1.2 | 1.1 | 1.4 | 1.9 | 1.1 |
| IS | 0.8 | 1.2 | 1.1 | 1.6 | 0.8 |
| SFG | 0.7 | 0.8 | 2.0 | 1.3 | 1.3 |
| Dextran 50,000 | 35.0 | 32.3 | 27.9 | 17.5 | 6.4 c |
| Dextran 5000 | 5.5 | 3.0 | 2.7 c | 1.6 | 1.2 |
| Dextran 1000 | 1.3 | 0.9 | 0.9 | 1.3 | 1.7 |
| Antibody Dilution | 1:1000 b | 1:2000 | 1:4000 | 1:8000 | 1:16,000 | 1:32,000 | 1:64,000 |
|---|---|---|---|---|---|---|---|
| IIM | 8.6 | 5.1 | 3.5 | 2.2 c | 1.4 | 1.2 | 1.1 |
| IM1000 | 0.9 | 0.9 | 0.8 | 0.7 | 0.7 | 0.9 | 0.8 |
| Dextran 5000 | 5.2 | 3.9 | 2.9 c | 1.9 | 1.4 | 1.7 | 1.2 |
| Assay | Immunodiffusion | ELISA | ||
|---|---|---|---|---|
| Lot No. | Reaction | Lot No. | Reaction | |
| Dextran 5000 | F201 | + | 00309 | + |
| Dextran 1000 | BCBD4347V | − | BCBD4347V | − |
| FMX | 10061002 | + | 09060402 | + |
| IIM | 042838-3 | + | 949171-1 | + |
| IM1000 | n.c. | n.c. | 949171-1 | − |
| LMWID | 1009019-4 | + | 1009019-4 | + |
| FCM | 144001 | − | 10667273 | − |
| IS | 133001 | − | 10674663 | − |
| SFG | D7A743A | − | D7A743A | − |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neiser, S.; Koskenkorva, T.S.; Schwarz, K.; Wilhelm, M.; Burckhardt, S. Assessment of Dextran Antigenicity of Intravenous Iron Preparations with Enzyme-Linked Immunosorbent Assay (ELISA). Int. J. Mol. Sci. 2016, 17, 1185. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071185
Neiser S, Koskenkorva TS, Schwarz K, Wilhelm M, Burckhardt S. Assessment of Dextran Antigenicity of Intravenous Iron Preparations with Enzyme-Linked Immunosorbent Assay (ELISA). International Journal of Molecular Sciences. 2016; 17(7):1185. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071185
Chicago/Turabian StyleNeiser, Susann, Taija S. Koskenkorva, Katrin Schwarz, Maria Wilhelm, and Susanna Burckhardt. 2016. "Assessment of Dextran Antigenicity of Intravenous Iron Preparations with Enzyme-Linked Immunosorbent Assay (ELISA)" International Journal of Molecular Sciences 17, no. 7: 1185. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17071185