
Influence of Preoperative Serum Aspartate Aminotransferase (AST) Level on the Prognosis of Patients with Non-Small Cell Lung Cancer

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
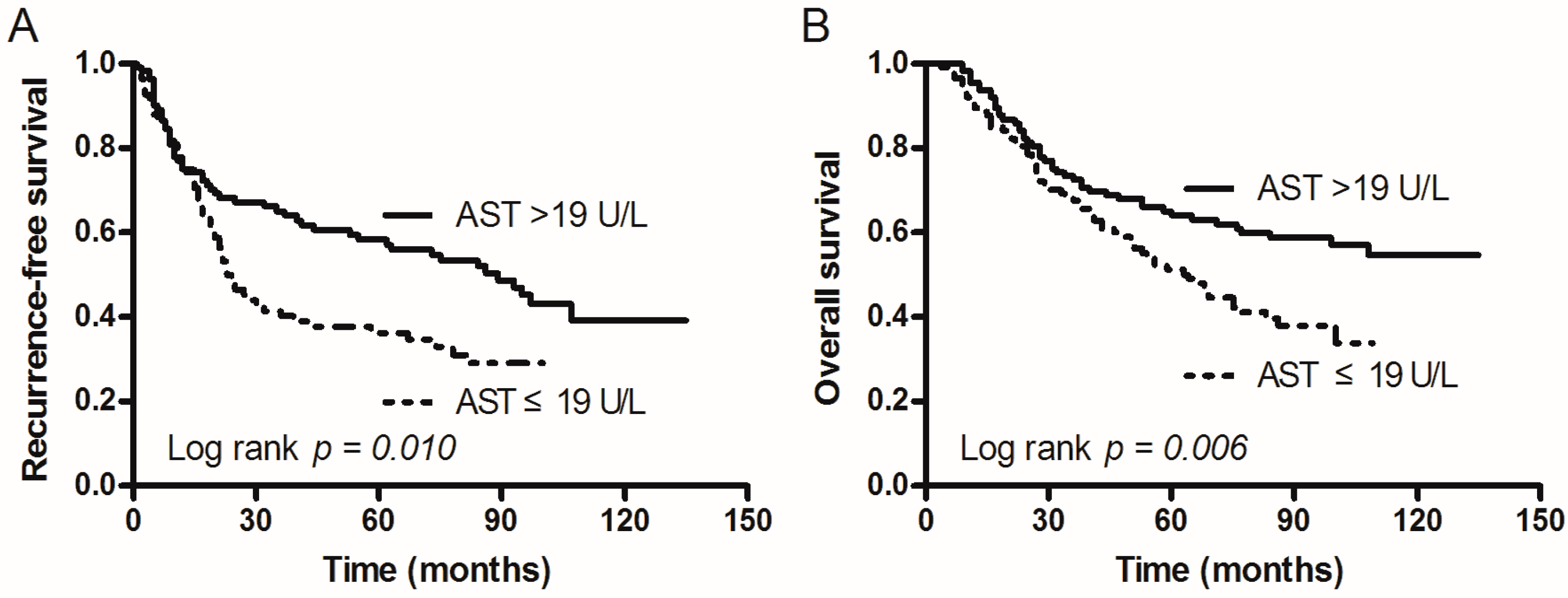
2.2. Relation of Patient Recurrence-Free Survival (RFS) and Overall Survival (OS) to AST Levels
2.3. Univariate and Multivariate Analyses of Prognostic Factors
2.4. The Distribution of Clinical Characteristics in the AST Subgroup
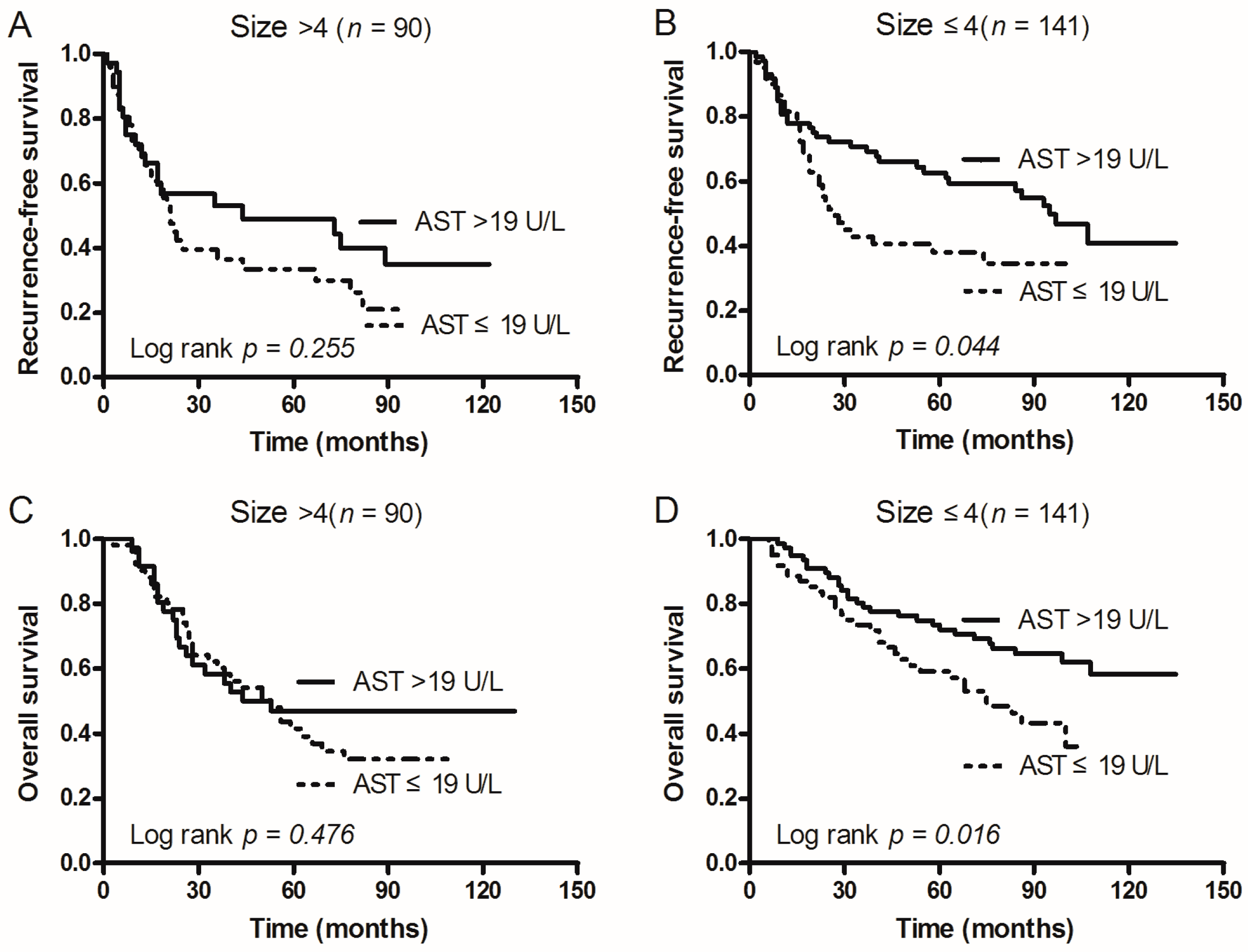
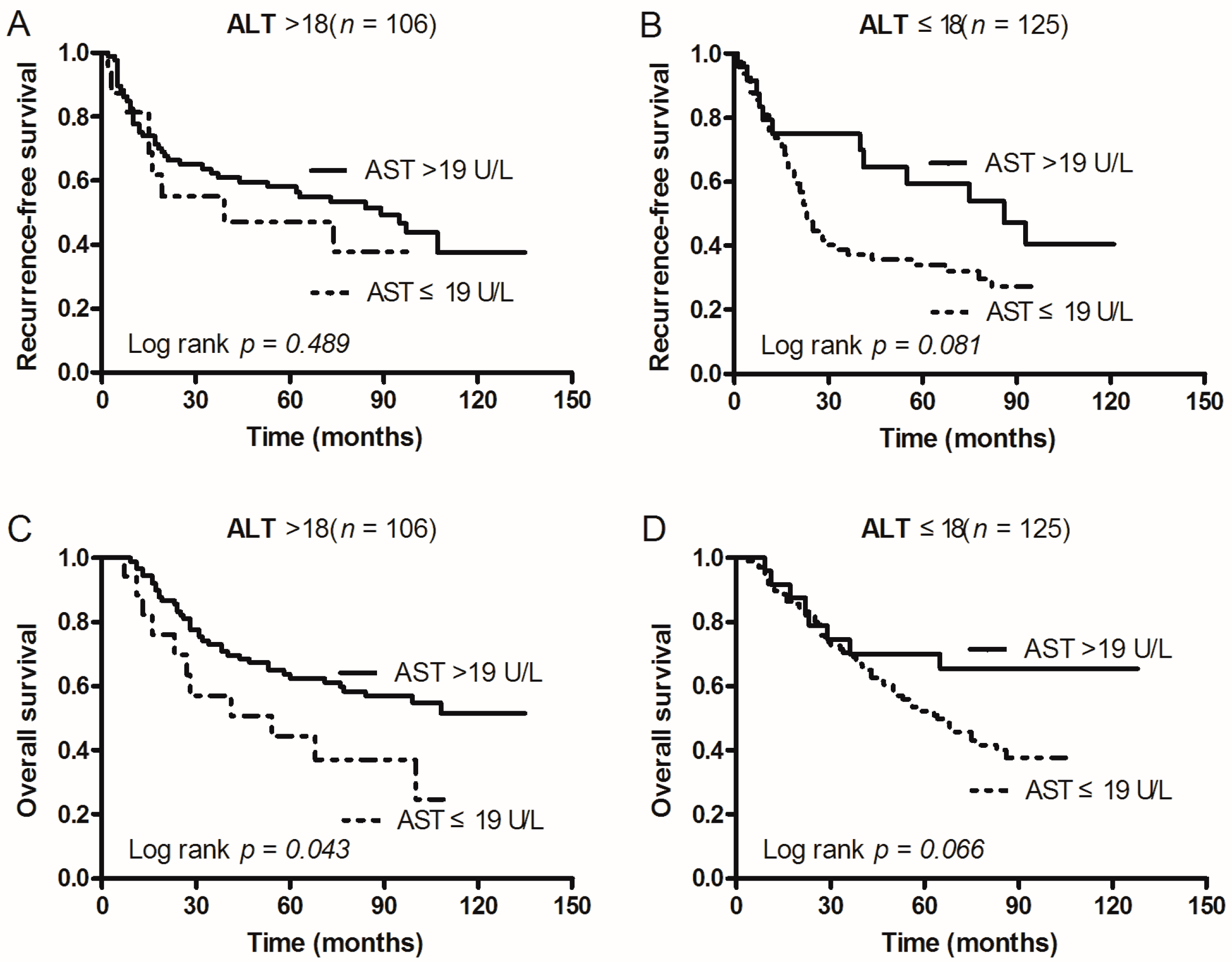
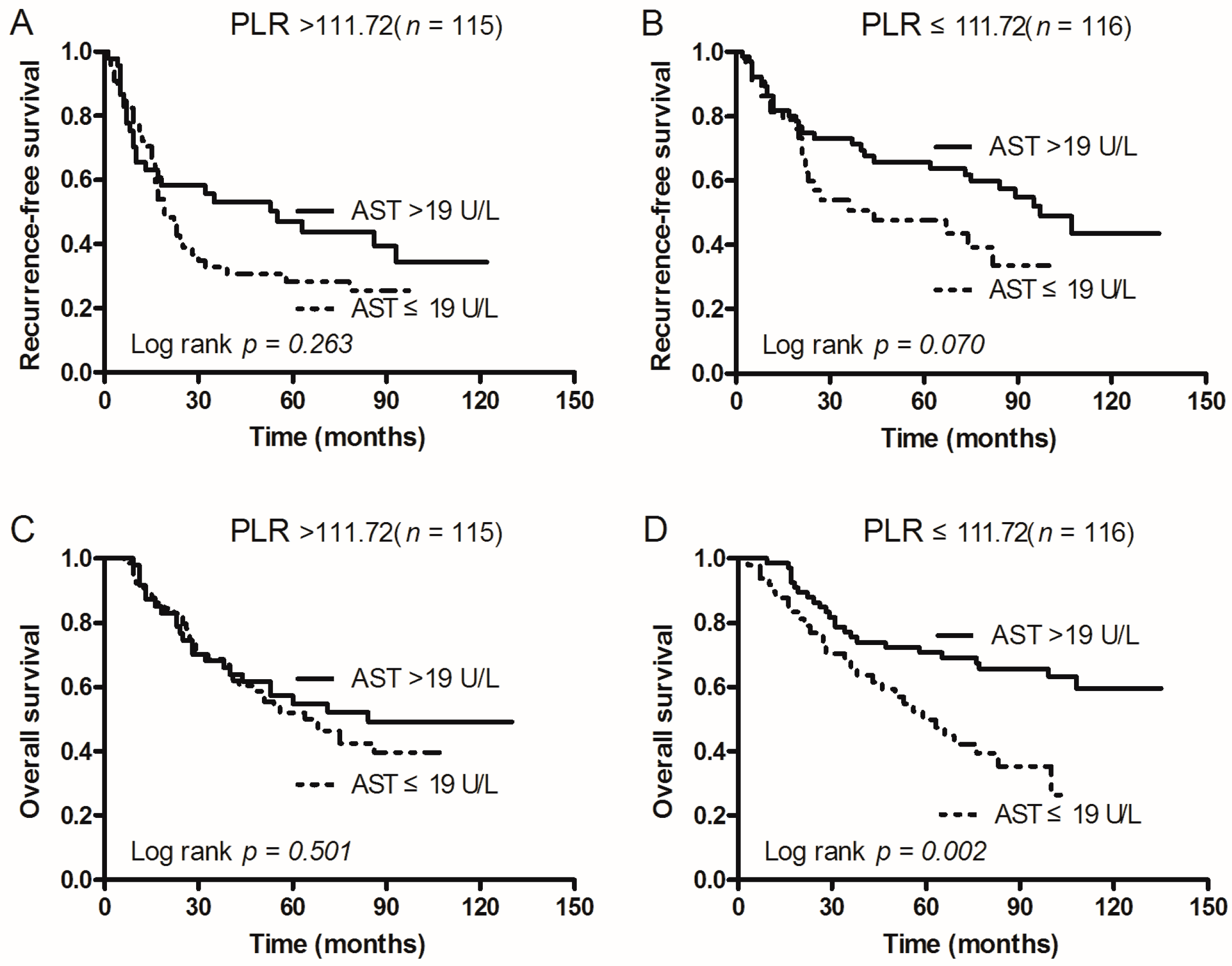
2.5. Subgroup Analysis According to Tumor Size, ALT, and PLR
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Inclusion Criteria
4.3. Exclusion Criteria
4.4. Clinical Outcomes Assessment and Patient Follow-up
4.5. Statistical Analysis Method
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed]
- She, J.; Yang, P.; Hong, Q.; Bai, C. Lung cancer in China: challenges and interventions. CHEST J. 2013, 143, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- D’addario, G.; Früh, M.; Reck, M.; Baumann, P.; Klepetko, W.; Felip, E. Metastatic non-small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21 (Suppl. 5), v116–v119. [Google Scholar] [CrossRef] [PubMed]
- Karmen, A.; Wroblewski, F.; Ladue, J.S. Transaminase activity in human blood. J. Clin. Investig. 1955, 34, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.-L.; Fu, S.-J.; Chen, B.; Kuang, M.; Li, S.-Q.; Hua, Y.-P.; Liang, L.J.; Guo, P.; Hao, Y.; Peng, B.G. Preoperative aspartate aminotransferase to platelet ratio is an independent prognostic factor for hepatitis B-induced hepatocellular carcinoma after hepatic resection. Ann. Surg. Oncol. 2014, 21, 3802–3809. [Google Scholar] [CrossRef] [PubMed]
- Bezan, A.; Mrsic, E.; Krieger, D.; Stojakovic, T.; Pummer, K.; Zigeuner, R.; Hutterer, G.C.; Pichler, M. The Preoperative AST/ALT (De Ritis) Ratio Represents a Poor Prognostic Factor in a Cohort of Patients with Nonmetastatic Renal Cell Carcinoma. J. Urol. 2015, 194, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Lindmark, G.; Gerdin, B.; Påhlman, L.; Bergström, R.; Glimelius, B. Prognostic predictors in colorectal cancer. Dis. Colon Rectum 1994, 37, 1219–1227. [Google Scholar] [CrossRef] [PubMed]
- Stocken, D.; Hassan, A.; Altman, D.; Billingham, L.; Bramhall, S.; Johnson, P.; Freemantle, N. Modelling prognostic factors in advanced pancreatic cancer. Br. J. Cancer 2008, 99, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Thornburg, J.M.; Nelson, K.K.; Clem, B.F.; Lane, A.N.; Arumugam, S.; Simmons, A.; Eaton, J.W.; Telang, S.; Chesney, J. Targeting aspartate aminotransferase in breast cancer. Breast Cancer Res. 2008, 10, R84. [Google Scholar] [CrossRef] [PubMed]
- Poon, R.T.-P.; Fan, S.-T.; Lo, C.-M.; Liu, C.-L.; Ng, I.O.; Wong, J. Long-term prognosis after resection of hepatocellular carcinoma associated with hepatitis B–related cirrhosis. J. Clin. Oncol. 2000, 18, 1094–1101. [Google Scholar] [PubMed]
- O’Reilly, S.M.; Richards, M.A.; Rubens, R.D. Liver metastases from breast cancer: the relationship between clinical, biochemical and pathological features and survival. Eur. J. Cancer Clin. Oncol. 1990, 26, 574–577. [Google Scholar] [CrossRef]
- Lee, H.; Lee, S.E.; Byun, S.S.; Kim, H.H.; Kwak, C.; Hong, S.K. De Ritis ratio (AST/ALT) as a significant prognostic factor after surgical treatment in patients with clear cell localized renal cell carcinoma: A propensity score matched study. BJU Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-L.; Li, J.-P.; Li, L.-F.; Zeng, T.; He, X. Elevated Preoperative Serum Alanine Aminotransferase/Aspartate Aminotransferase (ALT/AST) Ratio Is Associated with Better Prognosis in Patients Undergoing Curative Treatment for Gastric Adenocarcinoma. Int. J. Mol. Sci. 2016, 17, 911. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.; Shiner, R.; Seckl, M.; Stebbing, J.; Sharma, R.; Mauri, F. Prognostic performance of inflammation-based prognostic indices in primary operable non-small cell lung cancer. Br. J. Cancer 2014, 110, 1930–1935. [Google Scholar] [CrossRef] [PubMed]
- Sarraf, K.M.; Belcher, E.; Raevsky, E.; Nicholson, A.G.; Goldstraw, P.; Lim, E. Neutrophil/lymphocyte ratio and its association with survival after complete resection in non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2009, 137, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Thapa, B.; Walia, A. Liver function tests and their interpretation. Indian J. Pediatr. 2007, 74, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Damcott, C.; Shuldiner, S.R.; Chai, S.; Yang, R.; Hu, H.; Gibson, Q.; Ryan, K.A.; Mitchell, B.D.; Gong, D.W. Genome-wide association study identifies genetic variants in GOT1 determining serum aspartate aminotransferase levels. J. Hum. Genet. 2011, 56, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.P.; Sabatini, D.M. Cancer cell metabolism: Warburg and beyond. Cell 2008, 134, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Sudderth, J.; Dang, T.; Bachoo, R.G.; McDonald, J.G.; DeBerardinis, R.J. Glioblastoma cells require glutamate dehydrogenase to survive impairments of glucose metabolism or Akt signaling. Cancer Res. 2009, 69, 7986–7993. [Google Scholar] [CrossRef] [PubMed]
- DeBerardinis, R.J.; Mancuso, A.; Daikhin, E.; Nissim, I.; Yudkoff, M.; Wehrli, S.; Thompson, C.B. Beyond aerobic glycolysis: Transformed cells can engage in glutamine metabolism that exceeds the requirement for protein and nucleotide synthesis. Proc. Natl. Acad. Sci. USA 2007, 104, 19345–19350. [Google Scholar] [CrossRef]
- Elf, S.E.; Chen, J. Targeting glucose metabolism in patients with cancer. Cancer 2014, 120, 774–780. [Google Scholar] [CrossRef] [PubMed]
- Cairns, R.A.; Harris, I.S.; Mak, T.W. Regulation of cancer cell metabolism. Nat. Rev. Cancer 2011, 11, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Mizuguchi, S.; Nishiyama, N.; Iwata, T.; Nishida, T.; Izumi, N.; Tsukioka, T.; Izumi, N.; Tsukioka, T.; Inoue, K.; Uenishi, T.; et al. Serum Sialyl LewisX and cytokeratin 19 fragment as predictive factors for recurrence in patients with stage I non-small cell lung cancer. Lung Cancer 2007, 58, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ventosa, E.Y.; Blanco-Prieto, S.; González-Piñeiro, A.L.; Rodríguez-Berrocal, F.J.; Piñeiro-Corrales, G.; de la Cadena, M.P. Pretreatment levels of the serum biomarkers CEA, CYFRA 21-1, SCC and the soluble EGFR and its ligands EGF, TGF-alpha, HB-EGF in the prediction of outcome in erlotinib treated non-small-cell lung cancer patients. Springerplus 2015, 4, 171. [Google Scholar] [CrossRef] [PubMed]
- Molina, R.; Filella, X.; Auge, J.; Fuentes, R.; Bover, I.; Rifa, J.; Moreno, V.; Canals, E.; Viñolas, N.; Marquez, A.; et al. Tumor markers (CEA, CA 125, CYFRA 21-1, SCC and NSE) in patients with non-small cell lung cancer as an aid in histological diagnosis and prognosis. Tumor Biol. 2003, 24, 209–218. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Age (years) | |
| >55 | 115 (49.78) |
| ≤55 | 116 (50.22) |
| Sex | |
| Male | 160 (69.26) |
| Female | 71 (30.74) |
| Smoking behavior | |
| Yes | 132 (57.14) |
| No | 99 (42.86) |
| Family history of cancer | |
| Yes | 34 (14.72) |
| No | 197 (85.28) |
| BMI (kg/m2) | |
| ≥25 | 42 (18.18) |
| <25 | 189 (81.82) |
| Histology type | |
| AC | 118 (51.08) |
| SCC | 88 (38.10) |
| OTH | 25 (10.82) |
| pTNM stage | |
| I | 99 (42.86) |
| II | 47 (20.35) |
| III | 77 (33.33) |
| IV | 8 (3.46) |
| Maximum tumor diameter (cm) | |
| >4 | 90 (38.96) |
| ≤4 | 141 (61.04) |
| Lymph node status | |
| NEG | 128 (55.41) |
| POS | 103 (44.59) |
| ALB (g/L) | |
| >35 | 225 (97.40) |
| ≤35 | 6 (2.60) |
| ALT (U/L) | |
| >18 | 106 (45.89) |
| ≤18 | 125 (54.11) |
| AST (U/L) | |
| >19 | 113 (48.92) |
| ≤19 | 118 (51.08) |
| PLR | |
| >111.72 | 115 (49.78) |
| ≤111.72 | 116 (50.22) |
| NLR | |
| >2.14 | 114 (49.35) |
| ≤2.14 | 117 (50.65) |
| Patient Characteristics | OS (Months) Mean (95% CI) | p | RFS (Months) Mean (95% CI) | p |
|---|---|---|---|---|
| Age (years) | ||||
| >55 | 76.665 (67.565–85.766) | 0.359 | 63.009 (53.369–72.650) | 0.329 |
| ≤55 | 86.066 (76.251–95.882) | 63.447 (52.182–74.712) | ||
| Sex | ||||
| Male | 80.981 (72.625–89.337) | 0.367 | 66.107 (56.491–75.724) | 0.973 |
| Female | 85.290 (73.692–96.888) | 62.291 (49.820–74.762) | ||
| Smoking behavior | ||||
| Yes | 76.098 (67.424–84.772) | 0.154 | 64.175 (54.373–73.978) | 0.493 |
| No | 87.945 (77.661–98.228) | 62.324 (50.469–74.179) | ||
| Family history of cancer | ||||
| Yes | 90.878 (73.913–107.842) | 0.370 | 73.886 (53.745–94.027) | 0.390 |
| No | 79.310 (72.120–86.500) | 60.293 (52.583–68.004) | ||
| BMI (kg/m2) | ||||
| ≥25 | 80.675 (64.345–97.006) | 0.820 | 76.185 (56.974–95.397) | 0.222 |
| <25 | 81.451 (74.199–88.703) | 58.999 (51.380–66.618) | ||
| Histology type | ||||
| AC | 85.729 (76.289–95.168) | 0.405 | 63.068 (52.399–73.738) | 0.896 |
| SCC | 77.553 (67.136–87.971) | 63.293 (51.408–75.178) | ||
| OTH | 66.185 (48.611–83.760) | 66.965 (44.968–88.962) | ||
| pTNM stage | ||||
| I | 102.736 (93.568–111.905) | 0.000 | 84.840 (73.536–96.144) | 0.000 |
| II | 67.075 (53.697–80.453) | 54.221 (37.712–70.729) | ||
| III | 63.093 (51.851–74.335) | 45.489 (33.275–57.704) | ||
| IV | 47.425 (10.633–26.583) | 14.625 (3.929–25.321) | ||
| Maximum tumor diameter (cm) | ||||
| >4 | 68.968 (58.271–79.664) | 0.004 | 51.870 (40.398–63.342) | 0.017 |
| ≤4 | 90.734 (82.198–99.270) | 72.029 (61.938–82.119) | ||
| Lymph node status | ||||
| NEG | 97.137 (88.423–105.850) | 0.000 | 80.866 (70.495–91.237) | 0.000 |
| POS | 62.962 (53.589–72.336) | 42.230 (32.059–52.402) | ||
| ALB (g/L) | ||||
| >35 | 83.133 (76.131–90.136) | 0.732 | 65.655 (57.586–73.723) | 0.844 |
| ≤35 | 57.167 (32.407–81.926) | 55.000 (19.572–90.428) | ||
| ALT (U/L) | ||||
| >18 | 86.252 (76.245–96.258) | 0.332 | 73.243 (61.645–84.840) | 0.081 |
| ≤18 | 77.381 (68.506–86.256) | 54.699 (45.117–64.282) | ||
| AST (U/L) | ||||
| >19 | 91.878 (82.276–101.480) | 0.006 | 76.137 (65.207–87.067) | 0.010 |
| ≤19 | 64.624 (57.282–71.967) | 45.437 (37.405–53.469) | ||
| PLR | ||||
| >117.2 | 77.121 (67.702–86.540) | 0.236 | 51.428 (41.478–61.378) | 0.003 |
| ≤117.2 | 86.983 (77.387–96.580) | 76.815 (65.777–87.853) | ||
| NLR | ||||
| >2.14 | 75.314 (66.031–84.598) | 0.168 | 55.143 (45.256–65.030) | 0.076 |
| ≤2.14 | 87.570 (78.010–97.129) | 73.198 (61.769–84.626) | ||
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (years) | ||||||
| >55/≤55 | 0.837 | 0.583–1.201 | 0.333 | - | - | - |
| Sex | ||||||
| male/female | 1.007 | 0.683–1.484 | 0.974 | - | - | - |
| Smoking behavior | ||||||
| yes/no | 0.882 | 0.615–1.266 | 0.497 | - | - | - |
| Family history of cancer | ||||||
| yes/no | 0.800 | 0.478–1.338 | 0.395 | - | - | - |
| BMI (kg/m2) | ||||||
| ≥25/<25 | 0.734 | 0.444–1.212 | 0.227 | - | - | - |
| Histology type | ||||||
| AC/SCC/OTH | 1.001 | 0.754–1.330 | 0.993 | - | - | - |
| pTNM stage | ||||||
| I/II/III/IV | 1.626 | 1.346–1.964 | 0.000 | 1.351 | 1.006–1.814 | 0.450 |
| Maximum tumor diameter (cm) | ||||||
| >4/≤4 | 1.549 | 1.075–2.232 | 0.019 | 1.358 | 0.939–1.965 | 0.104 |
| Lymph node status | ||||||
| NEG/POS | 2.406 | 1.670–3.467 | 0.000 | 1.610 | 0.923–2.807 | 0.093 |
| ALB (g/L) | ||||||
| >35/≤35 | 1.149 | 0.284–4.654 | 0.846 | - | - | - |
| ALT (U/L) | ||||||
| >18/≤18 | 0.726 | 0.504–1.045 | 0.085 | - | - | - |
| AST (U/L) | ||||||
| >19/≤19 | 0.623 | 0.432–0.899 | 0.012 | 0.685 | 0.473–0.994 | 0.046 |
| PLR | ||||||
| >111.72/≤111.72 | 1.728 | 1.200–2.487 | 0.003 | 1.714 | 1.187–2.476 | 0.004 |
| NLR | ||||||
| >2.14/≤2.14 | 1.383 | 0.963–1.986 | 0.079 | - | - | - |
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age (years) | ||||||
| >55/≤55 | 1.189 | 0820–1.724 | 0.362 | - | - | - |
| Sex | ||||||
| male/female | 1.206 | 0.800–1.818 | 0.370 | - | - | - |
| Smoking behavior | ||||||
| yes/no | 1.267 | 0.867–1.852 | 0.221 | - | - | - |
| Family history of cancer | ||||||
| yes/no | 0.781 | 0.453–1.346 | 0.373 | - | - | - |
| BMI (kg/m2) | ||||||
| ≥25/<25 | 1.055 | 0.661–1.684 | 0.821 | - | - | - |
| Histology type | ||||||
| AC/SCC/OTH | 1.106 | 0.828–1.476 | 0.495 | - | - | - |
| pTNM stage | ||||||
| I/II/III/IV | 1.572 | 1.297–1.905 | 0.000 | 1.219 | 0.897–1.656 | 0.207 |
| Maximum tumor diameter (cm) | ||||||
| >4/≤4 | 1.711 | 1.179–2.484 | 0.005 | 1.451 | 0.987–2.131 | 0.058 |
| Lymph node status | ||||||
| NEG/POS | 2.373 | 1.627–3.461 | 0.000 | 1.741 | 0.968–3.130 | 0.064 |
| ALB (g/L) | ||||||
| >35/≤35 | 0.819 | 0.260–2.584 | 0.733 | - | - | - |
| ALT (U/L) | ||||||
| >18/≤18 | 0.832 | 0.573–1.209 | 0.335 | - | - | - |
| AST (U/L) | ||||||
| >19/≤19 | 0.594 | 0.407–0.869 | 0.007 | 0.646 | 0.438–0.954 | 0.028 |
| PLR | ||||||
| >111.72/≤111.72 | 1.250 | 0.862–1.813 | 0.239 | - | - | - |
| NLR | ||||||
| >2.14/≤2.14 | 1.297 | 0.894–1.881 | 0.171 | - | - | - |
| Characteristics | Subcategories | AST | AST | p |
|---|---|---|---|---|
| >19 | ≤19 | |||
| Age (years) | >55 | 58 | 57 | 0.694 |
| ≤55 | 55 | 61 | ||
| Sex | male | 82 | 78 | 0.320 |
| female | 31 | 40 | ||
| Smoking behavior | yes | 68 | 64 | 0.425 |
| no | 45 | 54 | ||
| Family history of cancer | yes | 15 | 19 | 0.581 |
| no | 98 | 99 | ||
| BMI (kg/m2) | ≥25 | 26 | 16 | 0.087 |
| <25 | 87 | 102 | ||
| Histology type | AC | 60 | 58 | 0.829 |
| SCC | 41 | 47 | ||
| OTH | 12 | 13 | ||
| pTNM stage | I–II | 75 | 71 | 0.343 |
| III–IV | 38 | 47 | ||
| Maximum tumor diameter (cm) | >4 | 36 | 54 | 0.032 |
| ≤4 | 77 | 64 | ||
| Lymph node status | NEG | 65 | 63 | 0.597 |
| POS | 48 | 55 | ||
| ALB (g/L) | >35 | 108 | 117 | 0.113 |
| ≤35 | 5 | 1 | ||
| ALT (U/L) | >18 | 89 | 17 | 0.000 |
| ≤18 | 24 | 101 | ||
| PLR | >111.72 | 47 | 68 | 0.018 |
| ≤111.72 | 66 | 50 | ||
| NLR | >2.14 | 50 | 64 | 0.148 |
| ≤2.14 | 63 | 54 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.-L.; Xue, N.; Wu, M.-T.; Chen, H.; He, X.; Li, J.-P.; Liu, W.-L.; Dai, S.-Q. Influence of Preoperative Serum Aspartate Aminotransferase (AST) Level on the Prognosis of Patients with Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2016, 17, 1474. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17091474
Chen S-L, Xue N, Wu M-T, Chen H, He X, Li J-P, Liu W-L, Dai S-Q. Influence of Preoperative Serum Aspartate Aminotransferase (AST) Level on the Prognosis of Patients with Non-Small Cell Lung Cancer. International Journal of Molecular Sciences. 2016; 17(9):1474. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17091474
Chicago/Turabian StyleChen, Shu-Lin, Ning Xue, Mian-Tao Wu, Hao Chen, Xia He, Jian-Pei Li, Wan-Li Liu, and Shu-Qin Dai. 2016. "Influence of Preoperative Serum Aspartate Aminotransferase (AST) Level on the Prognosis of Patients with Non-Small Cell Lung Cancer" International Journal of Molecular Sciences 17, no. 9: 1474. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17091474