
The Ultimaster Biodegradable-Polymer Sirolimus-Eluting Stent: An Updated Review of Clinical Evidence


{kind=link}
{kind=link}
Abstract
:1. Introduction
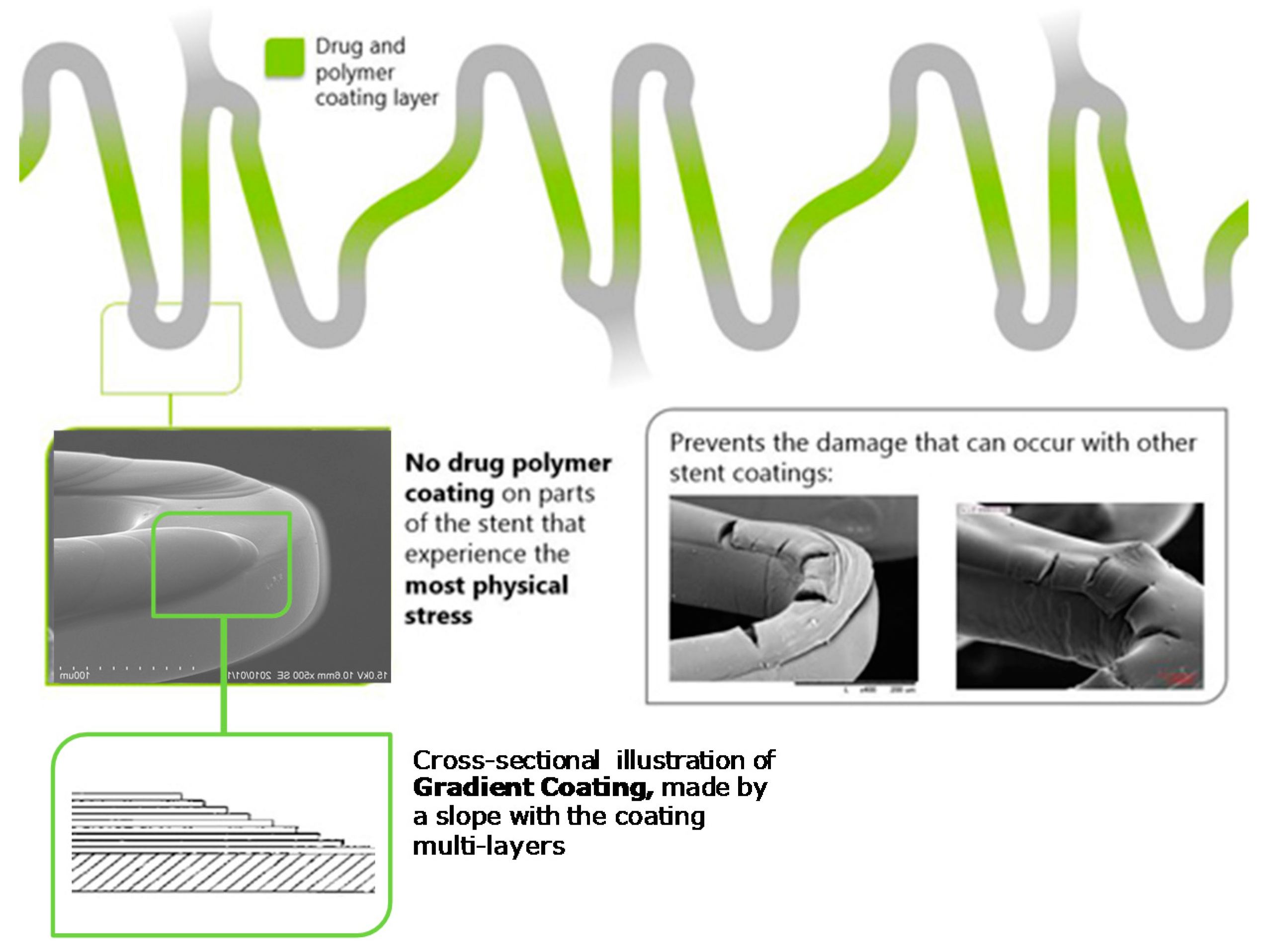
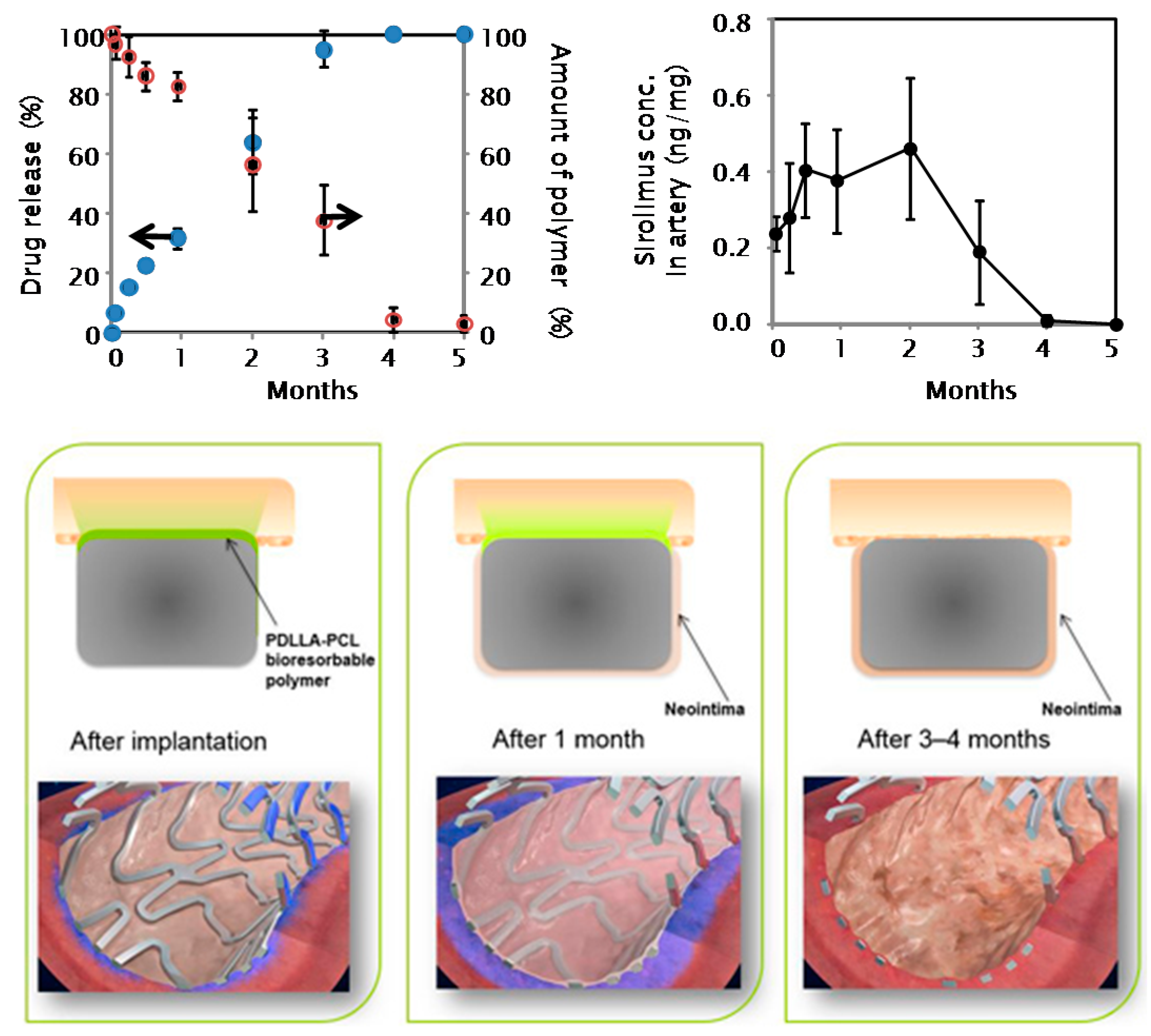
2. Stent Characteristics
3. Clinical Trials
3.1. CENTURY Study
3.2. CENTURY II Trial
4. Subgroup Analyses
4.1. Bifurcation Lesions
4.2. Small Vessel Disease
4.3. Long Lesions
4.4. Acute Coronary Syndromes (ACS)
4.5. OCT Substudy
5. Discussion
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Moses, J.W.; Leon, M.B.; Popma, J.J.; Fitzgerald, P.J.; Holmes, D.R.; O’Shaughnessy, C.; Caputo, R.P.; Kereiakes, D.J.; Williams, D.O.; Teirstein, P.S.; et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N. Engl. J. Med. 2003, 349, 1315–1323. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Lansky, A.J.; Pocock, S.J.; Gersh, B.J.; Dangas, G.; Wong, S.C.; Witzenbichler, B.; Guagliumi, G.; Peruga, J.Z.; Brodie, B.R.; et al. Paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction. N. Engl. J. Med. 2009, 360, 1946–1959. [Google Scholar] [CrossRef] [PubMed]
- Jeremias, A.; Kirtane, A. Balancing efficacy and safety of drug-eluting stents in patients undergoing percutaneous coronary intervention. Ann. Intern. Med. 2008, 148, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Stettler, C.; Wandel, S.; Allemann, S.; Kastrati, A.; Morice, M.C.; Schomig, A.; Pfisterer, M.E.; Stone, G.W.; Leon, M.B.; de Lezo, J.S.; et al. Outcomes associated with drug-eluting and bare-metal stents: A collaborative network meta-analysis. Lancet 2007, 370, 937–948. [Google Scholar] [CrossRef]
- Camenzind, E.; Steg, P.G.; Wijns, W. Stent thrombosis late after implantation of first-generation drug-eluting stents: A cause for concern. Circulation 2007, 115, 1440–1455. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Moses, J.W.; Ellis, S.G.; Schofer, J.; Dawkins, K.D.; Morice, M.C.; Colombo, A.; Schampaert, E.; Grube, E.; Kirtane, A.J.; et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N. Engl. J. Med. 2007, 356, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Lagerqvist, B.; James, S.K.; Stenestrand, U.; Lindback, J.; Nilsson, T.; Wallentin, L.; SCAAR Study Group. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N. Engl. J. Med. 2007, 356, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Van Beusekom, H.M.; Saia, F.; Zindler, J.D.; Lemos, P.A.; Swager-Ten Hoor, S.L.; van Leeuwen, M.A.; de Feijter, P.J.; Serruys, P.W.; van der Giessen, W.J. Drug-eluting stents show delayed healing: Paclitaxel more pronounced than sirolimus. Eur. Heart J. 2007, 28, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Finn, A.V.; Nakazawa, G.; Joner, M.; Kolodgie, F.D.; Mont, E.K.; Gold, H.K.; Virmani, R. Vascular responses to drug eluting stents: Importance of delayed healing. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1500–1510. [Google Scholar] [CrossRef] [PubMed]
- Finn, A.V.; Joner, M.; Nakazawa, G.; Kolodgie, F.; Newell, J.; John, M.C.; Gold, H.K.; Virmani, R. Pathological correlates of late drug-eluting stent thrombosis: Strut coverage as a marker of endothelialization. Circulation 2007, 115, 2435–2441. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Guagliumi, G.; Farb, A.; Musumeci, G.; Grieco, N.; Motta, T.; Mihalcsik, L.; Tespili, M.; Valsecchi, O.; Kolodgie, F.D. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious? Circulation 2004, 109, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Piscione, F.; Piccolo, R.; Cassese, S.; Galasso, G.; Chiariello, M. Clinical impact of sirolimus-eluting stent in ST-segment elevation myocardial infarction: A meta-analysis of randomized clinical trials. Catheter. Cardiovasc. Interv. 2009, 74, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Cassese, S.; Galasso, G.; Niglio, T.; de Rosa, R.; de Biase, C.; Piscione, F. Long-term clinical outcomes following sirolimus-eluting stent implantation in patients with acute myocardial infarction. A meta-analysis of randomized trials. Clin. Res. Cardiol. 2012, 101, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Cassese, S.; Galasso, G.; de Rosa, R.; D’Anna, C.; Piscione, F. Long-term safety and efficacy of drug-eluting stents in patients with acute myocardial infarction: A meta-analysis of randomized trials. Atherosclerosis 2011, 217, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, O.D.; Sakakura, K.; Otsuka, F.; Yahagi, K.; Virmani, R.; Joner, M. Coronary stent evolution: From pathology to clinic. EMJ Int. Cardiol. 2014, 1, 107–116. [Google Scholar]
- Raber, L.; Kelbaek, H.; Ostojic, M.; Baumbach, A.; Heg, D.; Tüller, D.; von Birgelen, C.; Roffi, M.; Moschovitis, A.; Khattab, A.A.; et al. Effect of biolimus-eluting stents with biodegradable polymer vs. bare-metal stents on cardiovascular events among patients with acute myocardial infarction: The comfortable AMI randomized trial. JAMA 2012, 308, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Stefanini, G.G.; Byrne, R.A.; Serruys, P.W.; de Waha, A.; Meier, B.; Massberg, S.; Juni, P.; Schomig, A.; Windecker, S.; Kastrati, A. Biodegradable polymer drug-eluting stents reduce the risk of stent thrombosis at 4 years in patients undergoing percutaneous coronary intervention: A pooled analysis of individual patient data from the ISAR-TEST 3, ISARTEST 4, and LEADERS randomized trials. Eur. Heart J. 2012, 33, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Stefanini, G.G.; Franzone, A.; Spitzer, E.; Blöchlinger, S.; Heg, D.; Jüni, P.; Windecker, S. Safety and efficacy of resolute zotarolimus-eluting stents compared with everolimus-eluting stents: A meta-analysis. Circ. Cardiovasc. Interv. 2015. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Pilgrim, T.; Heg, D.; Franzone, A.; Rat-Wirtzler, J.; Räber, L.; Silber, S.; Serruys, P.W.; Jüni, P.; Windecker, S. Comparative effectiveness and safety of new-generation versus early-generation drug-eluting stents according to complexity of coronary artery Disease: A patient-level pooled analysis of 6081 patients. JACC Cardiovasc. Interv. 2015, 8, 1657–1666. [Google Scholar] [CrossRef] [PubMed]
- Cassese, S.; Piccolo, R.; Galasso, G.; de Rosa, R.; Piscione, F. Twelve-month clinical outcomes of everolimus-eluting stent as compared to paclitaxel- and sirolimus-eluting stent in patients undergoing percutaneous coronary interventions. A meta-analysis of randomized clinical trials. Int. J. Cardiol. 2011, 150, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Giustino, G.; Mehran, R.; Windecker, S. Stable coronary artery disease: Revascularisation and invasive strategies. Lancet 2015, 386, 702–713. [Google Scholar] [CrossRef]
- Kastrati, A.; Mehilli, J.; Dirschinger, J.; Dotzer, F.; Schühlen, H.; Neumann, F.J.; Fleckenstein, M.; Pfafferott, C.; Seyfarth, M.; Schomig, A. Intracoronary stenting and angiographic results: Strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation 2001, 103, 2816–2821. [Google Scholar] [CrossRef] [PubMed]
- Kolandaivelu, K.; Swaminathan, R.; Gibson, W.J.; Kolachalama, V.B.; Nguyen-Ehrenreich, K.L.; Giddings, V.L.; Coleman, L.; Wong, G.K.; Edelman, E.R. Stent thrombogenicity early in high-risk interventional settings is driven by stent design and deployment and protected by polymer-drug coatings. Circulation 2011, 123, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Barbato, E.; Salinger-Martinovic, S.; Sagic, D.; Beleslin, B.; Vrolix, M.; Neskovic, A.N.; Jagic, N.; Verheye, S.; Mehmedbegovic, Z.; Wijns, W. A first-in-man clinical evaluation of Ultimaster, a new drug-eluting coronary stent system: CENTURY study. EuroIntervention 2015, 11, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Valdes-Chavarri, M.; Richardt, G.; Moreno, R.; Iniguez Romo, A.; Barbato, E.; Carrie, D.; Ando, K.; Merkely, B.; Kornowski, R.; et al. A randomized, prospective, intercontinental evaluation of a bioresorbable polymer sirolimus-eluting coronary stent system: The CENTURY II (Clinical Evaluation of New Terumo Drug-Eluting Coronary Stent System in the Treatment of Patients with Coronary Artery Disease) trial. Eur. Heart J. 2014, 35, 2021–2031. [Google Scholar] [PubMed]
- Orvin, K.; Carrie, D.; Richardt, G.; Desmet, W.; Assali, A.; Werner, G.; Ikari, Y.; Fujii, K.; Goicolea, J.; Dangoisse, V.; et al. Comparison of sirolimus eluting stent with bioresorbable polymer to everolimus eluting stent with permanent polymer in bifurcation lesions: Results from CENTURY II trial. Catheter. Cardiovasc. Interv. 2016, 87, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Wöhrle, J.; Markovic, S.; Rottbauer, W.; Muramatsu, T.; Kadota, K.; Vázquez-González, N.; Odenstedt, J.; Serra, A.; Antoniucci, D.; Varenne, O.; et al. Bioresorbable polymer sirolimus-eluting coronary stent compared with permanent polymer everolimus-eluting coronary stent implantation for treatment of small vessel coronary artery disease: CENTURY II trial. EuroIntervention 2016, 12, e167–e174. [Google Scholar] [CrossRef] [PubMed]
- Lesiak, M.; Araszkiewicz, A.; Grajek, S.; Colombo, A.; Lalmand, J.; Carstensen, S.; Namiki, A.; Tobaru, T.; Merkely, B.; Moreno, R.; et al. Long coronary lesions treated with thin strut bioresorbable polymer drug eluting stent: Experience from multicentre randomized CENTURY II study. J. Interv. Cardiol. 2016, 29, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, V.A.; Iñiguez, A.; Baz, J.A.; Valdés, M.; Ortiz, A.; Vuilliomenet, A.; Mainar, V.; Dudek, D.; Banai, S.; Tüller, D.; et al. A randomized comparison of novel bioresorbable polymer sirolimus-eluting stent and durable polymer everolimus-eluting stent in patients with acute coronary syndromes: The CENTURY II high risk ACS substudy. Cardiovasc. Revasc. Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Kuramitsu, S.; Kazuno, Y.; Sonoda, S.; Domei, T.; Jinnouchi, H.; Yamaji, K.; Soga, Y.; Shirai, S.; Ando, K.; Saito, S. Vascular response to bioresorbable polymer sirolimus-eluting stent vs. permanent polymer everolimus-eluting stent at 9-month follow-up: An optical coherence tomography sub-study from the CENTURY II trial. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Attizzani, G.F.; Capodanno, D.; Ohno, Y.; Tamburino, C. Mechanisms, pathophysiology, and clinical aspects of incomplete stent apposition. J. Am. Coll. Cardiol. 2014, 63, 1355–1367. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Ladich, E.; Nakazawa, G.; Eshtehardi, P.; Neidhart, M.; Vogel, R.; Togni, M.; Wenaweser, P.; Billinger, M.; Seiler, C.; et al. Correlation of intravascular ultrasound findings with histopathological analysis of thrombus aspirates in patients with very late drug eluting stent thrombosis. Circulation 2009, 120, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Wenaweser, P.; Daemen, J.; Zwahlen, M.; van Domburg, R.; Jeuni, P.; Vaina, S.; Hellige, G.; Tsuchida, K.; Morger, C.; Boersma, E.; et al. Incidence and correlates of drug-eluting stent thrombosis in routine clinical practice: 4-Year results from a large 2-institutional cohort study. J. Am. Coll. Cardiol. 2008, 52, 1134–1440. [Google Scholar] [CrossRef] [PubMed]
- Joner, M.; Finn, A.V.; Farb, A.; Mont, E.K.; Kolodgie, F.D.; Ladich, E.; Kutys, R.; Skorija, K.; Gold, H.K.; Virmani, R. Pathology of drug eluting stents in humans: Delayed healing and late thrombotic risk. J. Am. Coll. Cardiol. 2006, 48, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, G.; Finn, A.V.; Joner, M.; Ladich, E.; Kutys, R.; Mont, E.K.; Gold, H.K.; Burke, A.P.; Kolodgie, F.D.; Virmani, R. Delayed arterial healing and increased late stent thrombosis at culprit sites after drug-eluting stent placement for acute myocardial infarction patients: An autopsy study. Circulation 2008, 118, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Park, K.W.; Kang, D.Y.; Lim, W.H.; Park, K.T.; Han, J.K.; Kang, H.J.; Koo, B.K.; Oh, B.H.; Park, Y.B.; et al. Biodegradable polymer drug-eluting stents vs. bare metal stents vs. durable-polymer drug eluting stents: A systematic review and Bayesian approach network meta-analysis. Eur. Heart J. 2014, 35, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, R.; Nicolino, A.; Danzi, G.B. The Nobori biolimus-eluting stent: Update of available evidence. Expert Rev. Med. Devices 2014, 11, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Danzi, G.B.; Piccolo, R.; Galasso, G.; Piscione, F. Nobori biolimus-eluting stent versus permanent polymer drug-eluting stents in patients undergoing percutaneous coronary intervention: A meta-analysis of randomized clinical trials. Circ. J. 2014, 78, 1858–1866. [Google Scholar] [CrossRef] [PubMed]
- Longo, G.; La Manna, A.; Capodanno, D.; Tamburino, C. The Ultimaster coronary stent system: State of the art. Minerva Cardioangiol. 2015, 63, 193–203. [Google Scholar] [PubMed]
- Serruys, P.W.; Farooq, V.; Kalesan, B.; de Vries, T.; Buszman, P.; Linke, A.; Ischinger, T.; Klauss, V.; Eberli, F.; Wijns, W.; et al. Improved safety and reduction in stent thrombosis associated with biodegradable polymer based biolimus-eluting stents versus durable polymer-based sirolimus-eluting stents in patients with coronary artery disease: Final 5-year report of the LEADERS (Limus Eluted From A Durable Versus ERodable Stent Coating) randomized, non-inferiority trial. JACC Cardiovasc. Interv. 2013, 6, 777–789. [Google Scholar] [PubMed]


© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chisari, A.; Pistritto, A.M.; Piccolo, R.; La Manna, A.; Danzi, G.B. The Ultimaster Biodegradable-Polymer Sirolimus-Eluting Stent: An Updated Review of Clinical Evidence. Int. J. Mol. Sci. 2016, 17, 1490. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17091490
Chisari A, Pistritto AM, Piccolo R, La Manna A, Danzi GB. The Ultimaster Biodegradable-Polymer Sirolimus-Eluting Stent: An Updated Review of Clinical Evidence. International Journal of Molecular Sciences. 2016; 17(9):1490. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17091490
Chicago/Turabian StyleChisari, Alberto, Anna Maria Pistritto, Raffaele Piccolo, Alessio La Manna, and Gian Battista Danzi. 2016. "The Ultimaster Biodegradable-Polymer Sirolimus-Eluting Stent: An Updated Review of Clinical Evidence" International Journal of Molecular Sciences 17, no. 9: 1490. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17091490