
Clinical Decision-Making in the Treatment of Schizophrenia: Focus on Long-Acting Injectable Antipsychotics


Abstract
:
1. Introduction
2. Results
2.1. Participants
2.2. Modalities of Prescription according to the Practice Characteristics of Clinicians
2.3. Modalities of Decision-Making about Treatment of Schizophrenia
3. Discussion
- -
- Clinicians treating the highest proportion of schizophrenic patients prescribed significantly more LAI antipsychotics and fewer oral SGAs.
- -
- Other clinicians’ practice characteristics were not significantly associated with a differential use of LAI antipsychotics.
- -
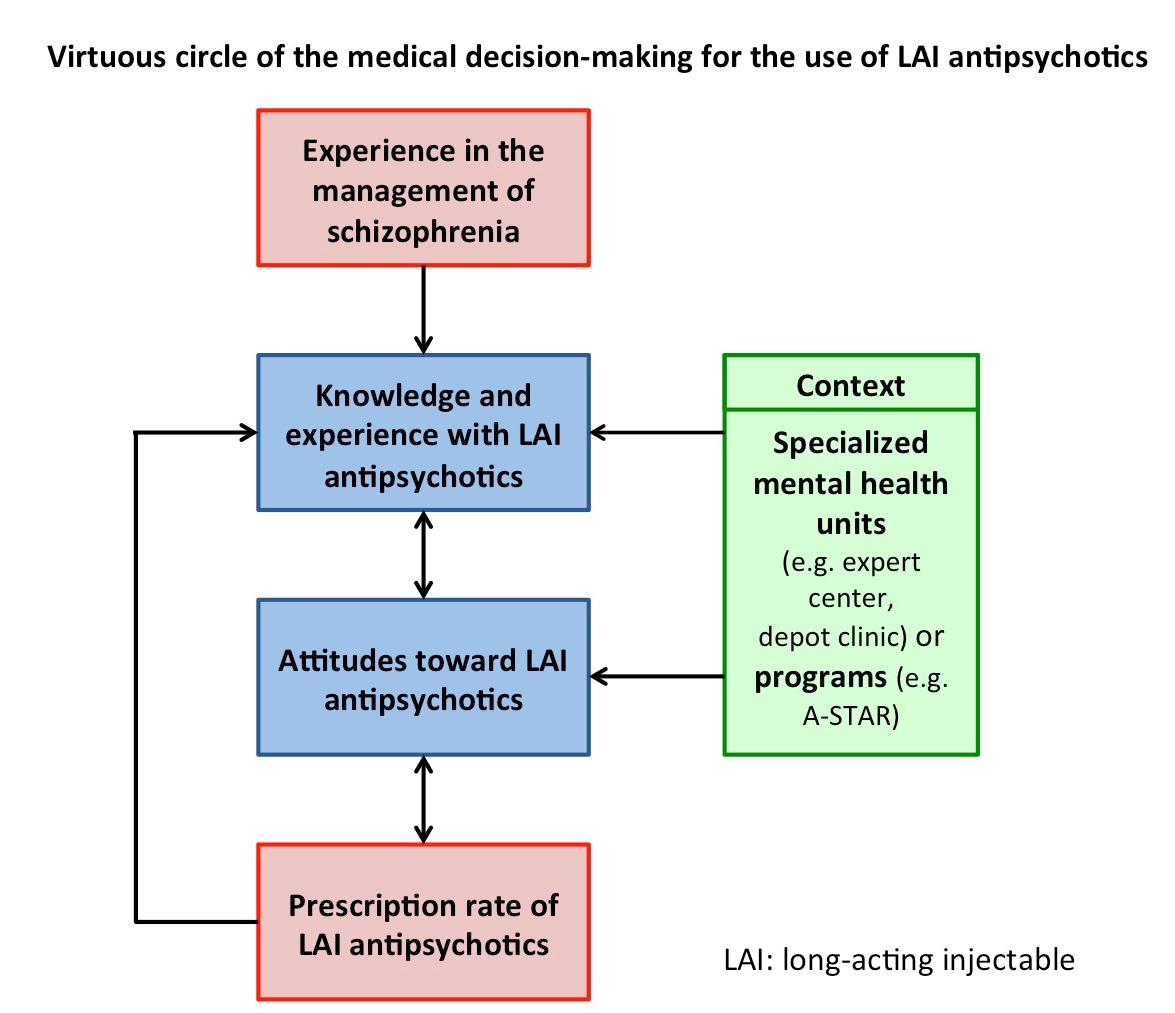
- Personal experience, government regulatory approval, and guidelines for the treatment of schizophrenia were the main factors guiding clinicians’ decision-making regarding the type and formulation of antipsychotic prescribed.
4. Materials and Methods
4.1. Procedure
4.2. Assessments
- -
- demographic characteristics and characterization of practice (i.e., gender, age, duration of career, type of practice, and proportion of schizophrenic patients follow-up);
- -
- estimation of antipsychotic prescription rates by the psychiatrists (oral FGAs, oral SGAs, LAI FGAs, and LAI SGAs);
- -
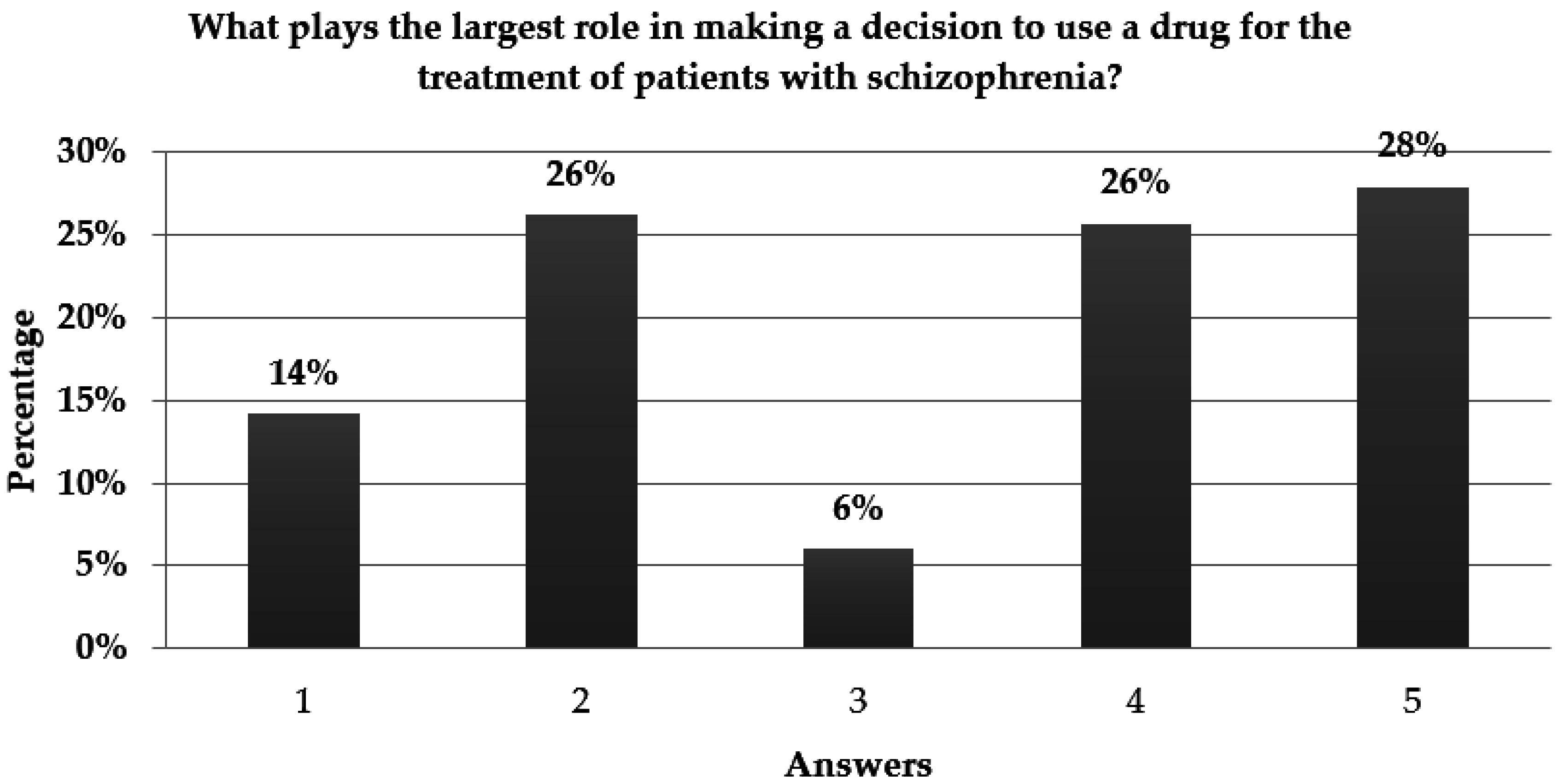
- sources of information influencing the medical decision-making regarding the treatment of schizophrenia—clinicians had to grade the sources of information proposed (i.e., published clinical studies, guidelines for the treatment of schizophrenia, information from congresses or conferences, government regulatory approval, and personal experience) from 1 (first-line source) to 5 (last-line source).
4.3. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Heres, S.; Lambert, M.; Vauth, R. Treatment of early episode in patients with schizophrenia: The role of long acting antipsychotics. Eur. Psychiatry 2014, 29 (Suppl. 2), 1409–1413. [Google Scholar] [CrossRef]
- Geerts, P.; Martinez, G.; Schreiner, A. Attitudes towards the administration of long-acting antipsychotics: A survey of physicians and nurses. BMC Psychiatry 2013, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Kirson, N.Y.; Weiden, P.J.; Yermakov, S.; Huang, W.; Samuelson, T.; Offord, S.J.; Greenberg, P.E.; Wong, B.J. Efficacy and effectiveness of depot versus oral antipsychotics in schizophrenia: Synthesizing results across different research designs. J. Clin. Psychiatry 2013, 74, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Brissos, S.; Veguilla, M.R.; Taylor, D.; Balanzá-Martinez, V. The role of long-acting injectable antipsychotics in schizophrenia: A critical appraisal. Ther. Adv. Psychopharmacol. 2014, 4, 198–219. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Kempton, M.J.; Rosenheck, R.A. Efficacy and safety of second-generation long-acting injections in schizophrenia: A meta-analysis of randomized-controlled trials. Int. Clin. Psychopharmacol. 2013, 28, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Manchanda, R.; Chue, P.; Malla, A.; Tibbo, P.; Roy, M.A.; Williams, R.; Iyer, S.; Lutgens, D.; Banks, N. Long-acting injectable antipsychotics: Evidence of effectiveness and use. Can. J. Psychiatry 2013, 58 (Suppl. 1), 5S–13S. [Google Scholar] [PubMed]
- Alphs, L.; Schooler, N.; Lauriello, J. How study designs influence comparative effectiveness outcomes: The case of oral versus long-acting injectable antipsychotic treatments for schizophrenia. Schizophr. Res. 2014, 156, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Kane, J.M.; Garcia-Ribera, C. Clinical guideline recommendations for antipsychotic long-acting injections. Br. J. Psychiatry 2009, 52, S63–S67. [Google Scholar] [CrossRef] [PubMed]
- Stip, E.; Abdel-Baki, A.; Bloom, D.; Grignon, S.; Roy, M.A. Long-acting injectable antipsychotics: An expert opinion from the Association des médecins psychiatres du Québec. Can. J. Psychiatry 2011, 56, 367–376. [Google Scholar] [PubMed]
- Malla, A.; Tibbo, P.; Chue, P.; Levy, E.; Manchanda, R.; Teehan, M.; Williams, R.; Iyer, S.; Roy, M.A. Long-acting injectable antipsychotics: Recommendations for clinicians. Can. J. Psychiatry 2013, 58, 30S–35S. [Google Scholar] [PubMed]
- Llorca, P.M.; Abbar, M.; Courtet, P.; Guillaume, S.; Lancrenon, S.; Samalin, L. Guidelines for the use and management of long-acting injectable antipsychotics in serious mental illness. BMC Psychiatry 2013, 13, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, A.; Falkai, P.; Wobrock, T.; Lieberman, J.; Glenthoj, B.; Gattaz, W.F.; Thibaut, F.; Möller, H.J.; WFSBP Task force on Treatment Guidelines for Schizophrenia. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 2: Update 2012 on the long-term treatment of schizophrenia and management of antipsychotic-induced side effects. World J. Biol. Psychiatry 2013, 14, 2–44. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.X.; Haddad, P.M.; Chaudhry, I.B.; McLoughlin, S.; Husain, N.; David, A.S. Psychiatrists’ use, knowledge and attitudes to first- and second-generation antipsychotic long-acting injections: Comparisons over 5 years. J. Psychopharmacol. 2010, 24, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Samalin, L.; Charpeaud, T.; Blanc, O.; Heres, S.; Llorca, P.M. Clinicians’ attitudes toward the use of long-acting injectable antipsychotics. J. Nerv. Mental Dis. 2013, 201, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.M.; Morrissette, D.A.; Citrome, L.; Saklad, S.R.; Cummings, M.A.; Meyer, J.M.; O’Day, J.A.; Dardashti, L.J.; Warburton, K.D. “Meta-guidelines” for the management of patients with schizophrenia. CNS Spectr. 2013, 18, 150–162. [Google Scholar] [CrossRef] [PubMed]
- Verdoux, H.; Pambrun, E.; Tournier, M.; Bezin, J.; Pariente, A. Antipsychotic long-acting injections: A community-based study from 2007 to 2014 of prescribing trends and characteristics associated with initiation. Schizophr. Res. 2016, in press. [Google Scholar] [CrossRef] [PubMed]
- Bret, P.; Heil, M.; Queuille, E.; Bret, M.C. Evaluation of prescription practices of long acting injectable risperidone in French hospitals. Encephale 2011, 37, S58–S65. [Google Scholar] [CrossRef] [PubMed]
- Barnes, T.R.; Shingleton-Smith, A.; Paton, C. Antipsychotic long-acting injections: Prescribing practice in the UK. Br. J. Psychiatry 2009, 52, S37–S42. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.T.; Weng, Y.Z.; Leung, C.M.; Tang, W.K.; Ungvari, G.S. Clinical and social correlates with the use of depot antipsychotic drugs in outpatients with schizophrenia in China. Int. J. Clin. Pharmacol. Ther. 2008, 46, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.X.; Nikolaou, V.; David, A.S. Psychiatrists’ attitudes to maintenance medication for patients with schizophrenia. Psychol. Med. 2003, 33, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Lee, Y.H.; Jang, J.E.; Yoo, T.; Kim, J.M.; Shin, I.S.; Yoon, J.S. Comparison of attitudes toward long-acting injectable antipsychotics among psychiatrists and patients. Int. Clin. Psychopharmacol. 2013, 28, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.; Banks, N.; Roy, M.A.; Tibbo, P.; Williams, R.; Manchanda, R.; Chue, P.; Malla, A. A qualitative study of experiences with and perceptions regarding long-acting injectable antipsychotics: Part II—Physician perspectives. Can. J. Psychiatry 2013, 58, 23S–29S. [Google Scholar] [PubMed]
- Heres, S.; Hamann, J.; Kissling, W.; Leucht, S. Attitudes of psychiatrists toward antipsychotic depot medication. J. Clin. Psychiatry 2006, 67, 1948–1953. [Google Scholar] [CrossRef] [PubMed]
- Samalin, L.; Guillaume, S.; Auclair, C.; Llorca, P.M. Adherence to guidelines by French psychiatrists in their real world of clinical practice. J. Nerv. Mental Dis. 2011, 199, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Samalin, L.; Abbar, M.; Courtet, P.; Guillaume, S.; Lancrenon, S.; Llorca, P.M. French Society for Biological Psychiatry and Neuropsychopharmacology task force: Formal Consensus for the prescription of depot antipsychotics. Encephale 2013, 39, 189–203. [Google Scholar] [CrossRef]
- Flodgren, G.; Hall, A.M.; Goulding, L.; Eccles, M.P.; Grimshaw, J.M.; Leng, G.C.; Shepperd, S. Tools developed and disseminated by guideline producers to promote the uptake of their guidelines. Cochrane Database Syst. Rev. 2016, 22, CD010669. [Google Scholar] [CrossRef]
- Velligan, D.I.; Medellin, E.; Draper, M.; Maples, N.; Dassori, A.; Moore, T.A.; Lopez, L. Barriers to, and strategies for, starting a long acting injection clinic in a community mental health center. Community Mental Health J. 2011, 47, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Schürhoff, F.; Fond, G.; Berna, F.; Bulzacka, E.; Vilain, J.; Capdevielle, D.; Misdrahi, D.; Leboyer, M.; Llorca, P.M.; FondaMental Academic Centers of Expertise for Schizophrenia (FACE-SZ) Collaborators. A National network of schizophrenia expert centres: An innovative tool to bridge the research-practice gap. Eur. Psychiatry 2015, 30, 728–735. [Google Scholar]
- Conseil National de l’Ordre des Médecins. Atlas de la Démographie Médicale en France: Situation Au 1er Janvier 2014. Available online: https://www.conseil-national.medecin.fr/sites/default/files/atlas_2014.pdf (accessed on 12 September 2016).


{kind=link}
{kind=link}
| Characteristics of Psychiatrists | N (%) |
|---|---|
| Gender (males) | 97 (48.0) |
| Mean ± SD | |
| Age (years) | 42.8 ± 11.4 |
| Duration of career (years) | 13.0 ± 10.7 |
| Type of practice (%) | |
| Outpatient | 55.4 ± 29.1 |
| Inpatient | 60.2 ± 27.2 |
| Proportion of schizophrenic patients followed (%) | 46.3 ± 24.3 |
| Prescription of antipsychotics (% of schizophrenic patients) | |
| Oral FGAs | 16.2 ± 13.2 |
| Oral SGAs | 54.9 ± 21.7 |
| LAI FGAs | 13.6 ± 12.2 |
| LAI SGAs | 30.4 ± 19.3 |
| Antipsychotics | Career Duration (Years) | % of Inpatients | % of Schizophrenic Patients | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Oral FGAs | 0.10 | 0.23 | 0.04 | 0.60 | 0.06 | 0.41 |
| Oral SGAs | 0.04 | 0.65 | −0.07 | 0.33 | −0.25 | <0.01 |
| LAI FGAs | 0.11 | 0.16 | 0.01 | 0.94 | 0.35 | <0.01 |
| LAI SGAs | 0.04 | 0.62 | 0.05 | 0.51 | 0.27 | <0.01 |
| Factors Affecting Decision-Making | Career Duration, Mean (Year) (SD) | % of Inpatients, % (SD) | % of Schizophrenic Patients, % (SD) | ||||
|---|---|---|---|---|---|---|---|
| p-Value | p-Value | p-Value | |||||
| Published clinical study literature | Yes | 11.1 (10.2) | 0.47 | 41.2 (35.6) | 0.64 | 38.0 (25.7) | 0.09 |
| No | 12.7 (10.6) | 50.3 (32.6) | 47.2 (23.9) | ||||
| Guidelines for the treatment of schizophrenia | Yes | 10.2 (9.6) | 0.11 | 46.7 (30.4) | 0.64 | 52.0 (23.0) | 0.05 |
| No | 13 (10.8) | 49.8 (33.9) | 43.5 (23.5) | ||||
| Information from congresses or conferences | Yes | 16.1 (13.0) | NA * | 51.0 (38.7) | 0.86 | 28.9 (24.2) | NA * |
| No | 12.3 (10.4) | 49.1 (32.7) | 47.1 (24.0) | ||||
| Government regular approval | Yes | 11.4 (9.0) | 0.68 | 48.3 (35.7) | 0.89 | 49.4 (25.4) | 0.36 |
| No | 12.9 (11.1) | 49.4 (31.9) | 45.0 (23.9) | ||||
| Personal experience | Yes | 15.4 (11.8) | 0.03 | 55.1 (30.4) | 0.13 | 44.1 (22.0) | 0.61 |
| No | 11.3 (9.8) | 46.5 (33.7) | 46.5 (25.3) | ||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samalin, L.; Garnier, M.; Auclair, C.; Llorca, P.-M. Clinical Decision-Making in the Treatment of Schizophrenia: Focus on Long-Acting Injectable Antipsychotics. Int. J. Mol. Sci. 2016, 17, 1935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17111935
Samalin L, Garnier M, Auclair C, Llorca P-M. Clinical Decision-Making in the Treatment of Schizophrenia: Focus on Long-Acting Injectable Antipsychotics. International Journal of Molecular Sciences. 2016; 17(11):1935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17111935
Chicago/Turabian StyleSamalin, Ludovic, Marion Garnier, Candy Auclair, and Pierre-Michel Llorca. 2016. "Clinical Decision-Making in the Treatment of Schizophrenia: Focus on Long-Acting Injectable Antipsychotics" International Journal of Molecular Sciences 17, no. 11: 1935. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17111935