
Highly Expression of CD11b and CD32 on Peripheral Blood Mononuclear Cells from Patients with Adult-Onset Still’s Disease

Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of the Patients
2.2. Percentage of Surface-Stained Cells Presenting CD11b, CD11c, CD32, CD206, CD209, and Dectin-1 in AOSD Patients, RA Patients, and HC
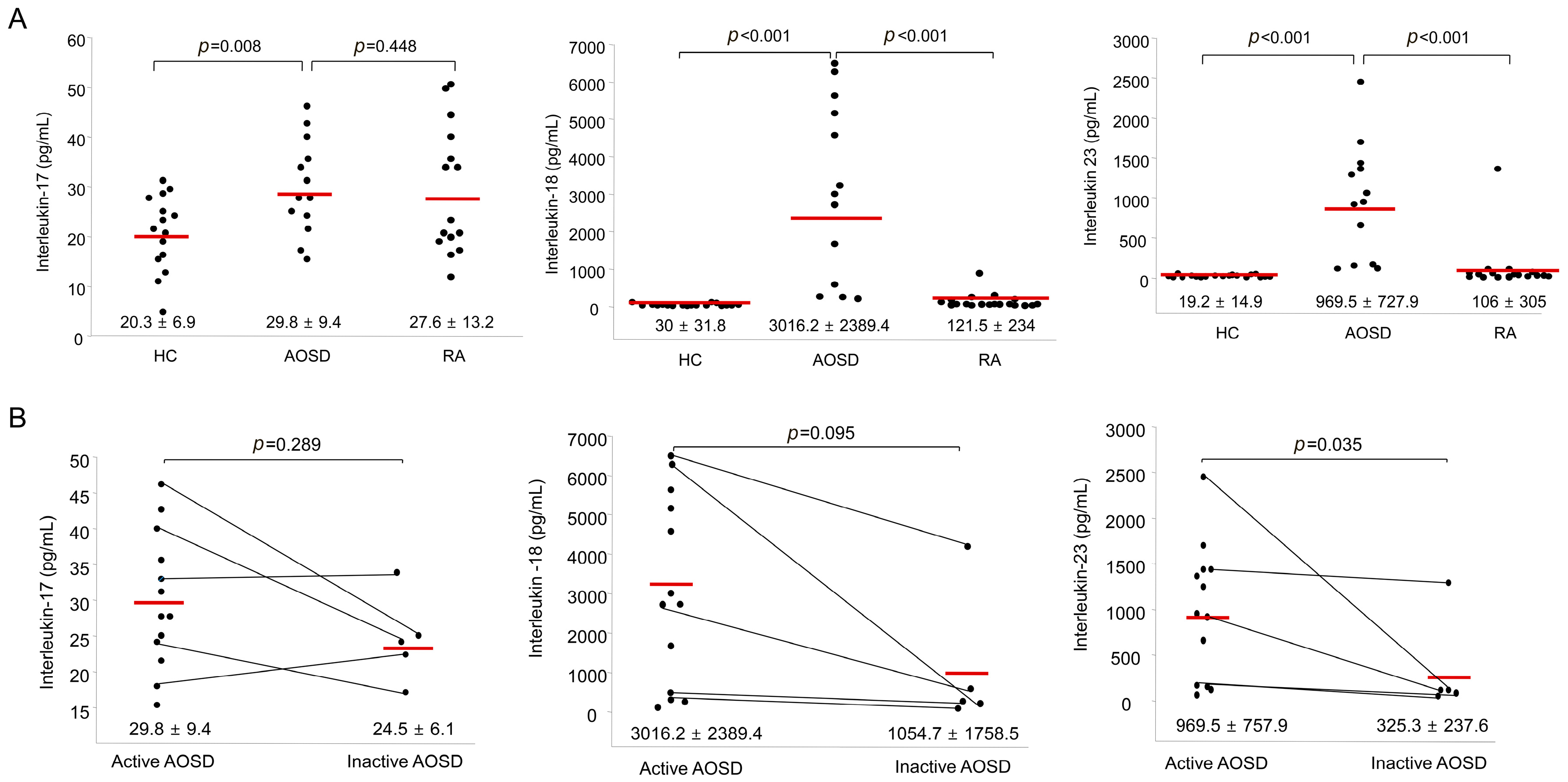
2.3. Serum Levels of IL-17, IL-18, and IL-23 in AOSD Patients, RA Patients, and HC
2.4. Percentages of Surface-Stained Cells Presenting CD11b, CD11c, CD32, CD206, CD209, and Dectin-1, and Serum Levels of IL-17, IL-18, and IL-23 According to Disease Activity in AOSD Patients
2.5. Correlation between the Frequencies of Stained Cells Presenting Several Markers and Disease Activity Markers in AOSD Patients
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Flow Cytometry of Surface-Stained Cells Presenting CD11b, CD11c, CD32, CD206, CD209, and Dectin-1
4.3. Cytokine Assay
4.4. Statistical Analyses
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Fautrel, B. Adult-onset Still disease. Best Pract. Res. Clin. Rheumatol. 2008, 22, 773–792. [Google Scholar] [CrossRef] [PubMed]
- Wouters, J.M.; van der Veen, J.; van de Putte, L.B.; de Rooij, D.J. Adult onset Still’s disease and viral infections. Ann. Rheum. Dis. 1988, 47, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Pouchot, J.; Sampalis, J.S.; Beaudet, F.; Carette, S.; Decary, F.; Salusinsky-Sternbach, M.; Hill, R.O.; Gutkowski, A.; Harth, M.; Myhal, D.; et al. Adult Still’s disease: Manifestations, disease course, and outcome in 62 patients. Medicine (Baltimore) 1991, 70, 118–136. [Google Scholar] [CrossRef] [PubMed]
- Wouters, J.M.; Reekers, P.; van de Putte, L.B. Adult-onset Still’s disease. Disease course and HLA associations. Arthritis Rheum. 1986, 29, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Y.; Chen, Y.M.; Lan, J.L.; Tzang, B.S.; Lin, C.C.; Hsu, T.C. Significant association of past parvovirus B19 infection with cytopenia in both adult-onset Still’s disease and systemic lupus erythematosus patients. Clin. Chim. Acta 2012, 413, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Fujita, M.; Hatachi, S.; Yagita, M. Acute Chlamydia pneumoniae infection in the pathogenesis of autoimmune diseases. Lupus 2009, 18, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Pouchot, J.; Ouakil, H.; Debin, M.L.; Vinceneux, P. Adult Still’s disease associated with acute human parvovirus B19 infection. Lancet 1993, 341, 1280–1281. [Google Scholar] [CrossRef]
- Chen, D.Y.; Lan, J.L.; Lin, F.J.; Hsieh, T.Y. Proinflammatory cytokine profiles in sera and pathological tissues of patients with active untreated adult onset Still’s disease. J. Rheumatol. 2004, 31, 2189–2198. [Google Scholar] [PubMed]
- Choi, J.H.; Suh, C.H.; Lee, Y.M.; Suh, Y.J.; Lee, S.K.; Kim, S.S.; Nahm, D.H.; Park, H.S. Serum cytokine profiles in patients with adult onset Still’s disease. J. Rheumatol. 2003, 30, 2422–2427. [Google Scholar] [PubMed]
- Priori, R.; Barone, F.; Alessandri, C.; Colafrancesco, S.; McInnes, I.B.; Pitzalis, C.; Valesini, G.; Bombardieri, M. Markedly increased IL-18 liver expression in adult-onset Still’s disease-related hepatitis. Rheumatology 2011, 50, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Bryant, C.E.; Orr, S.; Ferguson, B.; Symmons, M.F.; Boyle, J.P.; Monie, T.P. International Union of Basic and Clinical Pharmacology. XCVI. Pattern recognition receptors in health and disease. Pharmacol. Rev. 2015, 67, 462–504. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Akira, S. The role of pattern-recognition receptors in innate immunity: Update on Toll-like receptors. Nat. Immunol. 2010, 11, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Frosch, M.; Ahlmann, M.; Vogl, T.; Wittkowski, H.; Wulffraat, N.; Foell, D.; Roth, J. The myeloid-related proteins 8 and 14 complex, a novel ligand of toll-like receptor 4, and interleukin-1β form a positive feedback mechanism in systemic-onset juvenile idiopathic arthritis. Arthritis Rheum. 2009, 60, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.A.; An, J.M.; Nam, J.Y.; Jeon, J.Y.; Suh, C.H. Serum S100A8/A9, but not follistatin-like protein 1 and interleukin 18, may be a useful biomarker of disease activity in adult-onset Still’s disease. J. Rheumatol. 2012, 39, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Panda, A.K.; Parida, J.R.; Tripathy, R.; Pattanaik, S.S.; Ravindran, B.; Das, B.K. Mannose binding lectin: A biomarker of systemic lupus erythematosus disease activity. Arthritis Res. Ther. 2012, 14, R218. [Google Scholar] [CrossRef] [PubMed]
- Wei-yuan, M.; Wen-ting, L.; Chen, Z.; Qing, S. Significance of DC-LAMP and DC-SIGN expression in psoriasis vulgaris lesions. Exp. Mol. Pathol. 2011, 91, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Aldrete, C.; Galan-Diez, M.; Fernandez-Ruiz, E.; Nino-Moreno, P.; Estrada-Capetillo, L.; Abud-Mendoza, C.; Layseca-Espinosa, E.; Baranda, L.; Gonzalez-Amaro, R. Expression and function of dectin-1 is defective in monocytes from patients with systemic lupus erythematosus and rheumatoid arthritis. J. Clin. Immunol. 2013, 33, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.M.; Zhou, H.; Zhang, F.; Wilson, B.C.; Kam, W.; Hong, J.S. HMGB1 acts on microglia Mac1 to mediate chronic neuroinflammation that drives progressive neurodegeneration. J. Neurosci. 2011, 31, 1081–1092. [Google Scholar] [CrossRef] [PubMed]
- Benimetskaya, L.; Loike, J.D.; Khaled, Z.; Loike, G.; Silverstein, S.C.; Cao, L.; el Khoury, J.; Cai, T.Q.; Stein, C.A. Mac-1 (CD11b/CD18) is an oligodeoxynucleotide-binding protein. Nat. Med. 1997, 3, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Vetvicka, V.; Xia, Y.; Coxon, A.; Carroll, M.C.; Mayadas, T.N.; Ross, G.D. Beta-glucan, a “specific” biologic response modifier that uses antibodies to target tumors for cytotoxic recognition by leukocyte complement receptor type 3 (CD11b/CD18). J. Immunol. 1999, 163, 3045–3052. [Google Scholar] [PubMed]
- Rosetti, F.; Mayadas, T.N. The many faces of Mac-1 in autoimmune disease. Immunol. Rev. 2016, 269, 175–193. [Google Scholar] [CrossRef] [PubMed]
- Jamsa, J.; Huotari, V.; Savolainen, E.R.; Syrjala, H.; Ala-Kokko, T. Kinetics of leukocyte CD11b and CD64 expression in severe sepsis and non-infectious critical care patients. Acta Anaesthesiol. Scand. 2015, 59, 881–891. [Google Scholar] [CrossRef] [PubMed]
- Fagerholm, S.C.; MacPherson, M.; James, M.J.; Sevier-Guy, C.; Lau, C.S. The CD11b-integrin (ITGAM) and systemic lupus erythematosus. Lupus 2013, 22, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Warmerdam, P.A.; van de Winkel, J.G.; Gosselin, E.J.; Capel, P.J. Molecular basis for a polymorphism of human Fc gamma receptor II (CD32). J. Exp. Med. 1990, 172, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Stewart-Akers, A.M.; Cunningham, A.; Wasko, M.C.; Morel, P.A. Fc gamma R expression on NK cells influences disease severity in rheumatoid arthritis. Genes Immun. 2004, 5, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Van de Winkel, J.G.; Capel, P.J. Human IgG Fc receptor heterogeneity: Molecular aspects and clinical implications. Immunol. Today 1993, 14, 215–221. [Google Scholar] [CrossRef]
- Hepburn, A.L.; Mason, J.C.; Davies, K.A. Expression of Fcgamma and complement receptors on peripheral blood monocytes in systemic lupus erythematosus and rheumatoid arthritis. Rheumatology 2004, 43, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, S.; Hirohata, S.; Inoue, T.; Ito, K. Phenotypic analysis of peripheral blood monocytes isolated from patients with rheumatoid arthritis. J. Rheumatol. 1992, 19, 211–215. [Google Scholar] [PubMed]
- Torsteinsdottir, I.; Arvidson, N.G.; Hallgren, R.; Hakansson, L. Monocyte activation in rheumatoid arthritis (RA): Increased integrin, Fc gamma and complement receptor expression and the effect of glucocorticoids. Clin. Exp. Immunol. 1999, 115, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Wallace, C.A.; Ruperto, N.; Giannini, E.; Childhood, A.; Childhood Arthritis and Rheumatology Research Alliance; Pediatric Rheumatology International Trials Organization; Pediatric Rheumatology Collaborative Study Group. Preliminary criteria for clinical remission for select categories of juvenile idiopathic arthritis. J. Rheumatol. 2004, 31, 2290–2294. [Google Scholar] [PubMed]
- Ishikawa, S.; Shimizu, M.; Ueno, K.; Sugimoto, N.; Yachie, A. Soluble ST2 as a marker of disease activity in systemic juvenile idiopathic arthritis. Cytokine 2013, 62, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Frick, C.; Odermatt, A.; Zen, K.; Mandell, K.J.; Edens, H.; Portmann, R.; Mazzucchelli, L.; Jaye, D.L.; Parkos, C.A. Interaction of ICAM-1 with β 2-integrin CD11c/CD18: Characterization of a peptide ligand that mimics a putative binding site on domain D4 of ICAM-1. Eur. J. Immunol. 2005, 35, 3610–3621. [Google Scholar] [CrossRef] [PubMed]
- Ross, G.D.; Reed, W.; Dalzell, J.G.; Becker, S.E.; Hogg, N. Macrophage cytoskeleton association with CR3 and CR4 regulates receptor mobility and phagocytosis of iC3b-opsonized erythrocytes. J. Leukoc. Biol. 1992, 51, 109–117. [Google Scholar] [PubMed]
- Lewis, S.M.; Treacher, D.F.; Edgeworth, J.; Mahalingam, G.; Brown, C.S.; Mare, T.A.; Stacey, M.; Beale, R.; Brown, K.A. Expression of CD11c and EMR2 on neutrophils: Potential diagnostic biomarkers for sepsis and systemic inflammation. Clin. Exp. Immunol. 2015, 182, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Zamze, S.; Martinez-Pomares, L.; Jones, H.; Taylor, P.R.; Stillion, R.J.; Gordon, S.; Wong, S.Y. Recognition of bacterial capsular polysaccharides and lipopolysaccharides by the macrophage mannose receptor. J. Biol. Chem. 2002, 277, 41613–41623. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Evers, S.; Roeder, D.; Parlow, A.F.; Risteli, J.; Risteli, L.; Lee, Y.C.; Feizi, T.; Langen, H.; Nussenzweig, M.C. Mannose receptor-mediated regulation of serum glycoprotein homeostasis. Science 2002, 295, 1898–1901. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.O.; Gordon, S. The M1 and M2 paradigm of macrophage activation: Time for reassessment. F1000Prime Rep. 2014, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- Monrad, S.U.; Rea, K.; Thacker, S.; Kaplan, M.J. Myeloid dendritic cells display downregulation of C-type lectin receptors and aberrant lectin uptake in systemic lupus erythematosus. Arthritis Res. Ther. 2008, 10, R114. [Google Scholar] [CrossRef] [PubMed]
- Kaku, Y.; Imaoka, H.; Morimatsu, Y.; Komohara, Y.; Ohnishi, K.; Oda, H.; Takenaka, S.; Matsuoka, M.; Kawayama, T.; Takeya, M.; Hoshino, T. Overexpression of CD163, CD204 and CD206 on alveolar macrophages in the lungs of patients with severe chronic obstructive pulmonary disease. PLoS ONE 2014, 9, e87400. [Google Scholar] [CrossRef] [PubMed]
- Cuartero, M.I.; Ballesteros, I.; Moraga, A.; Nombela, F.; Vivancos, J.; Hamilton, J.A.; Corbi, A.L.; Lizasoain, I.; Moro, M.A. N2 neutrophils, novel players in brain inflammation after stroke: Modulation by the PPARgamma agonist rosiglitazone. Stroke 2013, 44, 3498–3508. [Google Scholar] [CrossRef] [PubMed]
- Khoo, U.S.; Chan, K.Y.; Chan, V.S.; Lin, C.L. DC-SIGN and L-SIGN: The SIGNs for infection. J. Mol. Med. 2008, 86, 861–874. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Zhou, T.; Wang, X.; Shang, M.; Zhang, Y.; Luo, M.; Xu, C.; Yuan, W. DC-SIGN expression on podocytes and its role in inflammatory immune response of lupus nephritis. Clin. Exp. Immunol. 2016, 183, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Higashino-Kameda, M.; Yabe-Wada, T.; Matsuba, S.; Takeda, K.; Anzawa, K.; Mochizuki, T.; Makimura, K.; Saijo, S.; Iwakura, Y.; Toga, H.; Nakamura, A. A critical role of Dectin-1 in hypersensitivity pneumonitis. Inflamm. Res. 2016, 65, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Rosas, M.; Liddiard, K.; Kimberg, M.; Faro-Trindade, I.; McDonald, J.U.; Williams, D.L.; Brown, G.D.; Taylor, P.R. The induction of inflammation by dectin-1 in vivo is dependent on myeloid cell programming and the progression of phagocytosis. J. Immunol. 2008, 181, 3549–3557. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Ohta, A.; Tsunematsu, T.; Kasukawa, R.; Mizushima, Y.; Kashiwagi, H.; Kashiwazaki, S.; Tanimoto, K.; Matsumoto, Y.; Ota, T.; et al. Preliminary criteria for classification of adult Still’s disease. J. Rheumatol. 1992, 19, 424–430. [Google Scholar] [PubMed]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Features and Laboratory Results | AOSD Patients (n = 13) | RA Patients (n = 19) | HC (n = 19) |
|---|---|---|---|
| Age (years) | 51.1 ± 20.5 | 48.2 ± 11.6 | 39.3 ± 14.7 |
| Gender (F/M) | 11/2 | 16/3 | 14/5 |
| Fever | 12 (92.3) | ||
| Sore throat | 9 (69.2) | ||
| Skin rash | 9 (69.2) | ||
| Lymphadenopathy | 4 (30.8) | ||
| Splenomegaly | 2 (15.4) | ||
| Hepatomegaly | 2 (15.4) | ||
| Pericarditis | 0 (0) | ||
| Arthritis | 11 (84.6) | ||
| Hemoglobin, g/dL | 11.3 ± 2.1 | 12.7 ± 1.5 | |
| Leukocytes, μL | 12,607 ± 4943 | 6084 ± 1908 | |
| Platelets, ×103/μL | 311.2 ± 96.4 | 227.5 ± 56.4 | |
| Ferritin, ng/mL | 5282.5 ± 9707.7 | ||
| LDH, U/L | 395.1 ± 231.6 | ||
| ESR, mm/h | 61 ± 23.4 | 12.5 ± 10.9 | |
| CRP, mg/dL | 11.17 ± 6.99 | 0.29 ± 0.61 | |
| AST/ALT, mg/dL | 69 ± 57.4 | 26.1 ± 8.4 | |
| AST, mg/dL | 72.2 ± 87.6 | 24.5 ± 19.8 | |
| Bilirubin, mg/dL | 0.84 ± 0.55 | 0.75 ±0.21 | |
| Albumin, g/dL | 4.15 ± 0.54 | 4.4 ± 0.18 | |
| ANA positivity | 3 (23.1) | 4 (21.1) | |
| RF positivity | 1 (7.7) | 14 (73.7) | |
| Systemic score | 4.92 ± 1.85 | ||
| DAS-28 | 2.8 ± 1.25 |
| Disease Activity Marker | Correlation Coefficient, r (p-Value) | ||||||
|---|---|---|---|---|---|---|---|
| CD11b Whole Cells | CD11c Lymphocytes | CD32 Monocytes | CD209 Whole Cells | CD209 Granulocytes | CD209 Monocytes | Dectin-1 Lymphocytes | |
| Systemic score | 0.487 (0.041) | 0.442 (0.066) | −0.559 (0.016) | 0.486 (0.041) | 0.484 (0.021) | 0.424 (0.04) | 0.363 (0.137) |
| Leukocytes | 0.074 (0.769) | 0.127 (0.616) | −0.393 (0.107) | 0.283 (0.255) | 0.212 (0.2) | 0.413 (0.044) | 0.089 (0.4) |
| Hemoglobin | −0.178 (0.481) | −0.376 (0.124) | 0.309 (0.212) | −0.172 (0.496) | −0.274 (0.136) | −0.259 (0.15) | −0.178 (0.301) |
| Platelets | −0.022 (0.932) | 0.122 (0.63) | −0.034 (0.893) | 0.024 (0.925) | 0.038 (0.44) | 0.424 (0.04) | −0.182 (0.296) |
| ESR | 0.285 (0.251) | 0.541 (0.02) | −0.363 (0.139) | 0.417 (0.085) | 0.452 (0.03) | 0.433 (0.036) | 0.142 (0.339) |
| CRP | 0.287 (0.248) | 0.409 (0.092) | −0.468 (0.05) | 0.395 (0.105) | 0.428 (0.038) | 0.298 (0.115) | 0.319 (0.17) |
| Ferritin | 0.286 (0.25) | 0.672 (0.002) | −0.583 (0.011) | 0.688 (0.002) | 0.705 (0.001) | 0.749 (<0.001) | 0.829 (0.001) |
| LDH | 0.58 (0.012) | 0.539 (0.021) | −0.412 (0.089) | 0.449 (0.061) | 0.535 (0.011) | 0.55 (0.009) | 0.694 (0.009) |
| Bilirubin | 0.028 (0.911) | −0.01 (0.967) | 0.493 (0.038) | 0.061 (0.809) | 0.045 (0.43) | −0.017 (0.473) | 0.199 (0.279) |
| AST | 0.635 (0.005) | 0.25 (0.317) | −0.276 (0.268) | 0.247 (0.324) | 0.331 (0.09) | 0.394 (0.053) | 0.438 (0.089) |
| ALT | 0.335 (0.174) | −0.045 (0.858) | 0.127 (0.616) | −0.119 (0.639) | −0.072 (0.388) | 0.052 (0.42) | 0.046 (0.447) |
| IL-17 | 0.106 (0.674) | 0.229 (0.227) | −0.189 (0.452) | 0.326 (0.187) | 0.359 (0.072) | 0.321 (0.097) | 0.491 (0.063) |
| IL-18 | 0.564 (0.015) | 0.452 (0.06) | −0.358 (0.145) | 0.441 (0.067) | 0.411 (0.045) | 0.159 (0.265) | 0.525 (0.049) |
| IL-23 | 0.529 (0.024) | 0.367 (0.135) | −0.476 (0.046) | 0.386 (0.113) | 0.458 (0.028) | 0.199 (0.214) | 0.255 (0.224) |
| Correlation Coefficient, r (p-Value) | |||||
|---|---|---|---|---|---|
| CD11c | CD32 | CD206 | CD209 | Dectin-1 | |
| CD11b | 0.243 (0.166) | 0.853 (<0.001) | 0.108 (0.334) | 0.006 (0.49) | 0.147 (0.324) |
| CD11c | 0.263 (0.146) | 0.765 (<0.001) | 0.317 (0.1) | 0.811 (0.001) | |
| CD32 | 0.108 (0.334) | −0.231 (0.178) | 0.035 (0.457) | ||
| CD206 | 0.624 (0.003) | 0.846 (<0.001) | |||
| CD209 | 0.615 (0.017) | ||||
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-A.; Choi, B.; Suh, C.-H.; Han, M.H.; Jung, J.-Y.; Sayeed, H.M.; Kim, Y.W.; Sohn, S. Highly Expression of CD11b and CD32 on Peripheral Blood Mononuclear Cells from Patients with Adult-Onset Still’s Disease. Int. J. Mol. Sci. 2017, 18, 202. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18010202
Kim H-A, Choi B, Suh C-H, Han MH, Jung J-Y, Sayeed HM, Kim YW, Sohn S. Highly Expression of CD11b and CD32 on Peripheral Blood Mononuclear Cells from Patients with Adult-Onset Still’s Disease. International Journal of Molecular Sciences. 2017; 18(1):202. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18010202
Chicago/Turabian StyleKim, Hyoun-Ah, Bunsoon Choi, Chang-Hee Suh, Mi Hwa Han, Ju-Yang Jung, Hasan M. Sayeed, Ye Won Kim, and Seonghyang Sohn. 2017. "Highly Expression of CD11b and CD32 on Peripheral Blood Mononuclear Cells from Patients with Adult-Onset Still’s Disease" International Journal of Molecular Sciences 18, no. 1: 202. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18010202