
The Value of In Vitro Tests to Diminish Drug Challenges
by
Cristobalina Mayorga
1,2,*, 
Inmaculada Doña
2,
Ezequiel Perez-Inestrosa
3,4,
Tahia D. Fernández
1 and
Maria J. Torres
2,4 1
Research Laboratory-Allergy Unit, Biomedical Institute of Málaga-IBIMA, Regional University Hospital of Malaga-UMA, Málaga 29009, Spain
2
Allergy Service, IBIMA-Regional University Hospital of Malaga-UMA, Málaga 29009, Spain
3
Department of Organic Chemistry, University of Málaga, Biomedical Institute of Málaga-IBIMA, Málaga 29071, Spain
4
Andalusian Center for Nanomedicine and Biotechnology-BIONAND, Málaga 29590, Spain
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2017, 18(6), 1222; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061222
Submission received: 4 May 2017
/
Revised: 31 May 2017
/
Accepted: 2 June 2017
/
Published: 7 June 2017
(This article belongs to the Special Issue Drug Hypersensitivity)
Abstract
:Drug hypersensitivity reactions have multiple implications for patient safety and health system costs, thus it is important to perform an accurate diagnosis. The diagnostic procedure includes a detailed clinical history, often unreliable; followed by skin tests, sometimes with low sensitivity or unavailable; and drug provocation testing, which is not risk-free for the patient, especially in severe reactions. In vitro tests could help to identify correctly the responsible agent, thus improving the diagnosis of these reactions, helping the physician to find safe alternatives, and reducing the need to perform drug provocation testing. However, it is necessary to confirm the sensitivity, specificity, negative and positive predictive values for these in vitro tests to enable their implementation in clinical practice. In this review, we have analyzed these parameters from different studies that have used in vitro test for evaluating drug hypersensitivity reactions and estimated the added value of these tests to the in vivo diagnosis.
Keywords:
drug; hypersensitivity; allergy; diagnosis; in vitro; IgE; T-cells; basophils; cytokines; immunoassays1. Introduction
Drug hypersensitivity reactions (DHR) represent 5–10% of all adverse drug reactions [1]. Longer inpatient stays and higher rates of hospital associated infections have been reported for antibiotic allergic patients [2]. These reactions have multiple implications for patient safety and health system costs, often requiring alternative drugs to be prescribed; these alternative drugs may be less effective, more toxic and more expensive; moreover, in the case of antibiotics, this can augment the development of bacterial resistance [2]. For these reasons, it is important to establish an accurate diagnosis of DHRs, and to avoid labeling tolerant individuals as allergic. However, it is just as important to correctly identify the responsible agent and find safe alternatives to avoid serious problems due to reactions. This is particularly important for severe DHR such as anaphylaxis, Steven–Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN).
Although in theory drugs can induce the four types of reaction proposed in the Coombs and Gell classification [3], types I and IV are the most frequent. Type I or immediate DHR (IDHR) are mediated by drug specific IgE (sIgE) antibodies attached to high-affinity IgE receptors, FcεRI, on mast cells or basophils, inducing release of mediators that lead to the reaction [3]. Type IV or non-immediate DHR (NIDHR), are induced by T-cells through the involvement of different inflammatory mediators [4]. Different reaction types show different clinical manifestations and timings, therefore mechanism should be taken into account during the allergological work-up.
The diagnostic procedure of a suspected DHR includes a detailed clinical history [5], followed by skin tests (STs) [6] and drug provocation testing (DPT) [7]. This procedure can be complex, time-consuming, and expensive. Moreover, it can present some risk to the patient. A detailed clinical history is the most important step towards an accurate diagnosis of DHR. However, it can be unreliable since there may be a lack of accurate information, i.e., the chronology may be imprecise, the clinical manifestations may be heterogeneous and the exact name of drug or corrective treatment may be not recalled precisely by the patient, making drug causality assessment difficult to ascertain [8].
Regarding STs, their diagnostic value is not well established for most drugs. Detailed, validated ST protocols for the diagnosis of DHR are lacking, and test concentrations are unknown or poorly validated. In many cases, STs have low sensitivity and require high drug concentrations; this can result in false-positive reactions due to the irritative properties of the drug. Moreover, many drugs are not available in injectable form and hence intradermal tests are not possible. Although STs are not validated and standardized for all drugs [6,9], experts from both Europe and America suggest that it is possible to recommend specific drug concentrations for β-lactam (BLs) antibiotics, perioperative drugs, heparins, platinum salts, and radio contrast media (RCM) [9].
Since clinical history can be unreliable and the sensitivity of STs may be suboptimal or unknown, the definitive diagnosis of DHR frequently relies upon DPT [10]. DPT must be performed by controlled administration under medical surveillance. It is widely considered to be the gold standard to establish or exclude the diagnosis of hypersensitivity to a certain substance. It not only reproduces allergic symptoms but also any other adverse clinical manifestations, irrespective of the mechanism. Moreover, it can be used to provide alternative drugs [10]. However, DPT is a procedure that consumes time and resources and, due to the possibility of reproducing the allergic reaction, is not risk free, especially when evaluating severe reactions. Therefore, it should be performed after balancing the risk–benefit ratio for each individual case. Patients at risk of more severe reactions should be given DPT in a hospital setting. It should not be performed in patients with co-morbidities such as acute infections or serious underlying diseases, as drug-exposure might provoke reactions that are hard to control. It should not be performed in patients who have experienced severe life-threatening reactions such as anaphylaxis, SJS or TEN [10].
Given the low sensitivity of in vivo procedures, potential unreliability of clinical history, and riskiness of DPT, there is a clear need for the development of validated in vitro tests to aid and improve the diagnosis of DHR. These tests will help us to correctly identify the responsible agent for a reaction and evaluate cross-reactivity with other drugs, helping the physician to find safe alternatives, and reducing the need to perform DPT.
2. In Vitro Tests for the Diagnosis of Drug Hypersensitivity Reactions (DHR)
Nowadays, in vitro methods for evaluating DHR depend on the underlying mechanism, whether IgE or T cell-mediated, and are mainly based on the analysis of drug sIgE or T cell subpopulations as well as the detection of specific markers after stimulation with the culprit drug and/or its metabolites.
As noted above, IDHR are IgE mediated. Therefore, the most widely used in vitro tests are immunoassays and basophil activation test (BAT). For NIDHR, which are cell-mediated, lymphocyte transformation tests (LTT), enzyme-linked immunosorbent spot assay (ELISpot), enzyme-linked immunosorbent assay (ELISA) and flow cytometry are typically used [11,12]. However, there is high variability between published studies regarding their accuracy. This is likely due to small sample sizes, and in some studies the lack of appropriate control subjects. There is no general consensus regarding under which circumstances these tests are most appropriate. Recently, experts from the European Network on Drug Allergy and Drug Allergy Interest Group of the European Academy of Allergy and Clinical Immunology provided recommendations regarding the available in vitro tests for DHR. They identified several unmet needs from which they highlighted the necessity to confirm the sensitivity, specificity, NPV and PPV for these in vitro tests. Such data are crucial to enable the implementation of in vitro testing in clinical practice, in order to reduce the need to perform DPT.
In this review, we have analyzed sensitivity and specificity as well as positive predictive value (PPV) and negative predictive value (NPV). Where possible, we have calculated these values using the data given in the studies. In total, we have obtained values from 60 publications, selecting studies that used in vitro test for evaluating DHR, for at least five patients. We have also estimated the added value of these tests to the in vivo diagnosis, paying special attention to how they can lead to increased ST sensitivity, avoiding the need to perform DPT.
3. IgE-Mediated Reactions
The main goal of in vitro tests for these types of reaction is the determination of drug/drug metabolite sIgE, either soluble in serum, or bound to the basophil surface. However, since sIgE and especially drug sIgE are found at a very low concentration in the blood [13], these in vitro methods must be highly sensitive. Another important issue is the need for different drugs to bind covalently to a carrier protein such as a hapten; this is required for a drug to induce an immune response. It is therefore important that the test includes the correct carrier molecules for appropriate IgE recognition [14,15]. All these factors are critical for in vitro test development.
The most frequent methods to evaluate IDHR are immunoassays (radioimmunoassays and fluorimmunoassays) and tests based on basophil activation (BAT).
3.1. Immunoassays
“Immunoassays” refers to a group of techniques that are based on the quantification of drug-sIgE present in patient sera. For this, the drug is conjugated to a carrier and coupled to a solid phase which is incubated with patient serum. If present, sIgE in the sera recognizes the drug, forming a drug-carrier-antibody complex which is quantified using a secondary anti-human IgE antibody labeled with a radioisotope (RIA) or a fluorescent enzyme (FEIA) [11]. RIA is generally conducted using in house techniques, such as the radioallergosorbent test (RAST); FEIA can be performed using commercial products, such as the ImmunoCAP-FEIA, although such products are only available for few drugs [16,17].
The majority of studies for evaluating the value of immunoassays for diagnosing IDHR have been performed with BLs [13,15,16,18,19,20,21,22] and neuromuscular blocking agents (NMBAs) [23,24,25,26,27,28,29], although a handful of studies have been carried out on other drugs, including chlorhexidine [30], quinolones [31,32] and biological agents [33,34,35,36]. Many of these studies have included large numbers of allergic patients and controls, allowing us to estimate the sensitivity, specificity, PPV and NPV (Table 1). Overall, we have calculated an average sensitivity of 62.9%, specificity of 89.2% and a PPV and NPV of 83.3% and 77.8%, respectively. In our opinion this sensitivity value is sub-optimal for clinical diagnosis, especially for BLs and no-BLs antibiotics. Moreover, NPV, the most useful parameter to decide whether to perform a DPT, is also relatively low [37]. Interestingly, immunoassays show higher results for NMBAs, with sensitivity of 79.3%, specificity of 92.2% and PPV and NPV of 91.3% and 83.3%, respectively. Regarding biological agents, although the global sensitivity is low (48.2%), immunoassays show a high specificity (92.5%) and NPV (83.6%).
3.2. Basophil Activation Test
This test is based on the determination of basophil activation or degranulation markers after drug stimulation using flow cytometry [17,38]. Compared with the determination of sIgE by immunoassays, BAT analysis is used to demonstrate a functional response [37]. BAT has been shown to be useful as an additional test for the diagnosis of DHR, especially for those cases where there are no other diagnostic tool available besides DPT. Basophils can be detected using a single cell marker, such as anti-IgE, CCR3, CRTH2, or CD203c, or a combination of several. Activation is usually assessed by determining the expression of CD63 or CD203c on the basophil surface [37]. It is important to take into account that differences have been found in the upregulation of both markers depending on the drug tested and the clinical entity [39,40]. When evaluating DHR using BAT, the possibility of activating basophils by a non-IgE-mediated mechanism exist, thus the involvement of the FcεRI-mediated pathway should be confirmed by inhibition with PI3Kinase inhibitors such as wortmannin [32,41].
As for immunoassays, multiple studies with BAT using reasonable numbers of patients have been performed for BLs [18,19,39,42,43,44,45] and NMBAs [24,25,46,47,48,49,50,51]. Additional studies have been performed for fluoroquinolones (FQs) [31,40,52,53], pyrazolones [54,55,56] and RCM [57,58] (Table 2). The analyses of these studies, taken together, show an average sensitivity of 59.4%, specificity of 94.6% and PPV and NPV of 93.4% and 66.3%, respectively. Sensitivity and specificity are relatively similar for the different drugs, ranging from 51.7% to 66.9% and 89.2% to 97.8%, respectively. The lowest values of sensitivity and NPV have been found for BLs, being 51.7% and 49.9%, respectively. On the contrary, the highest sensitivity and NPV values were found for IDHR to FQs, 64.4% and 68.1%, respectively, and NMBAs, 66.9% and 72.1% respectively.
3.3. Combining In Vitro Tests for Evaluating Immediate Drug Hypersensitivity Reactions (IDHR)
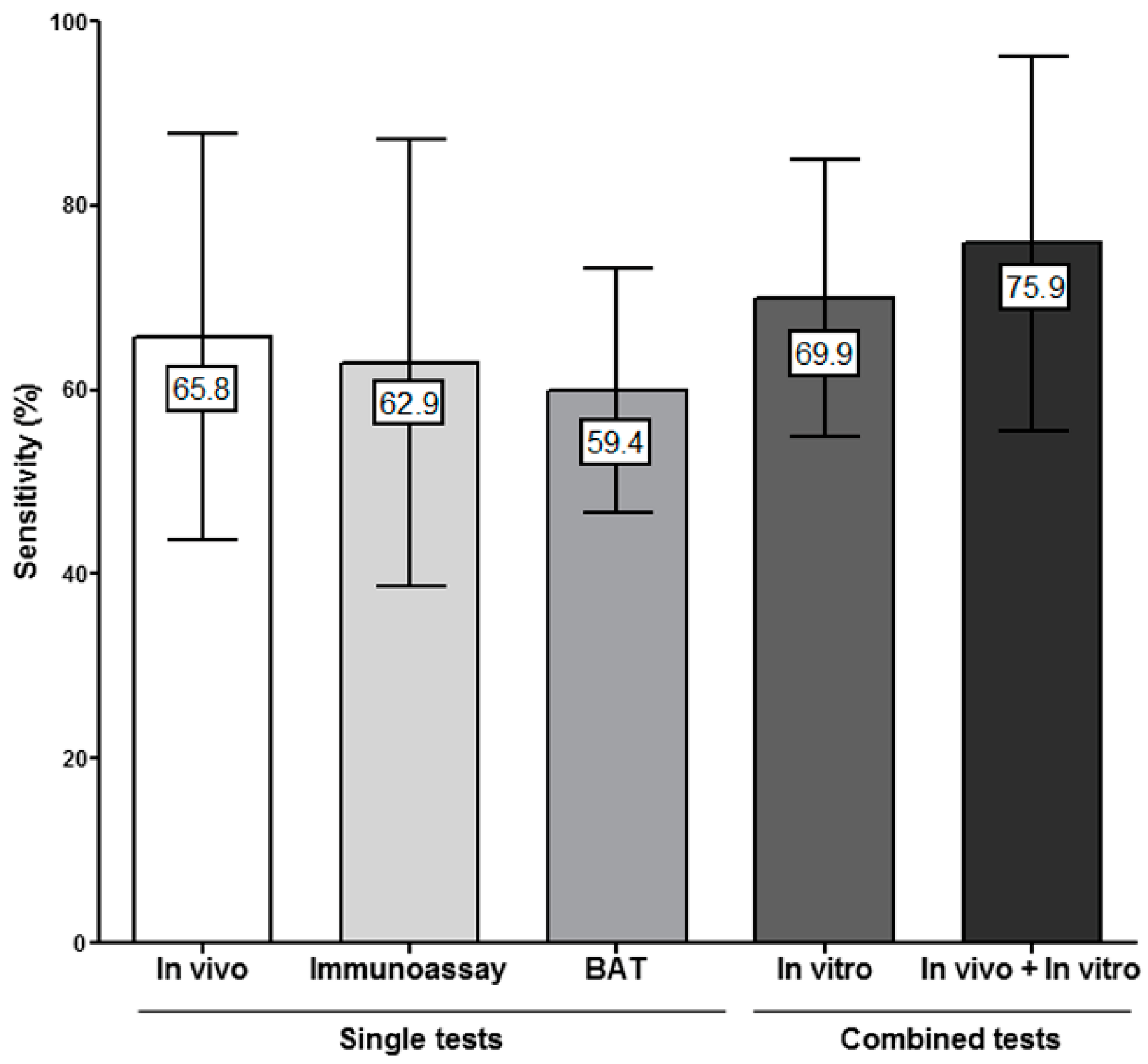
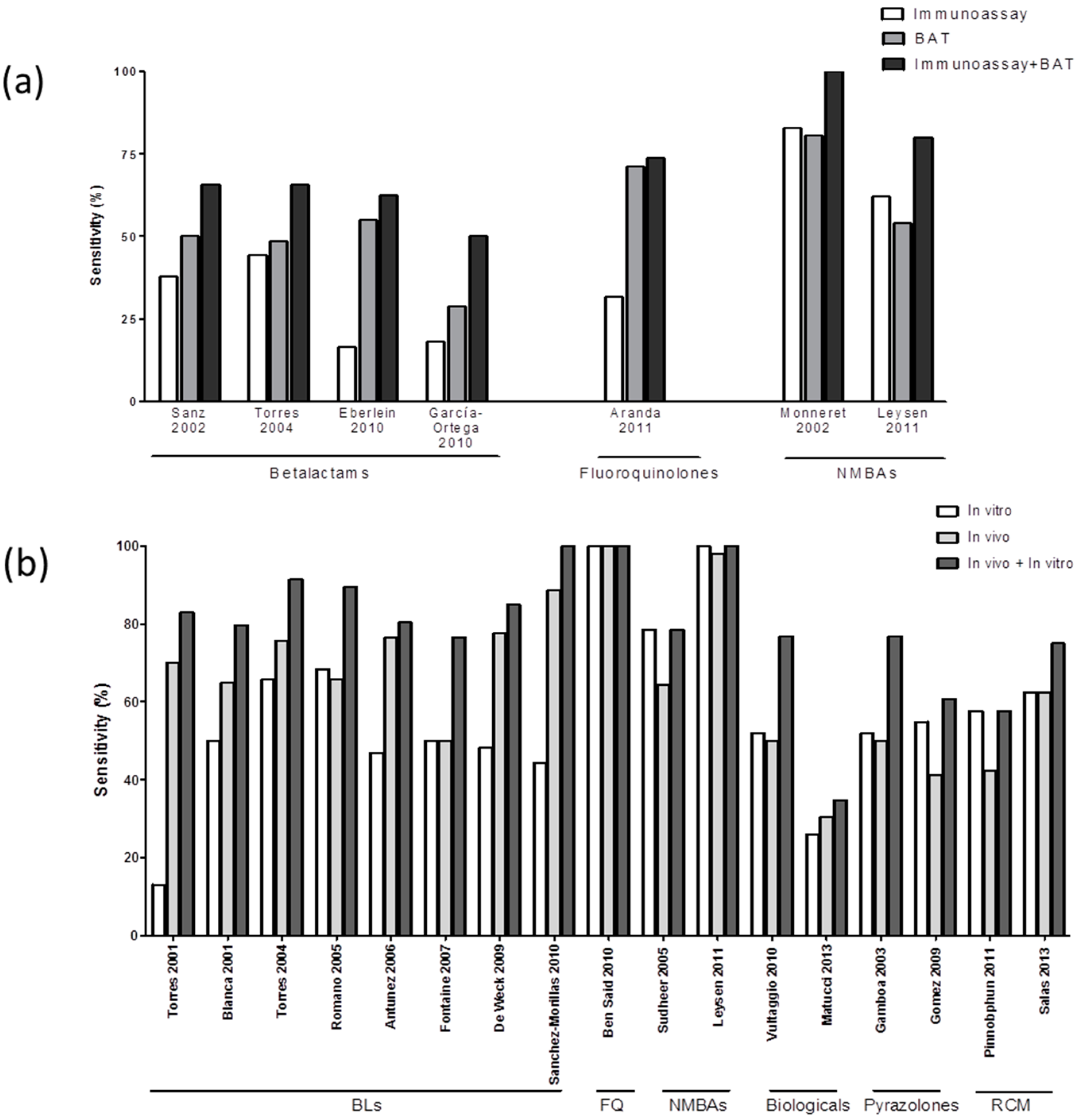
Several studies have performed both tests, immunoassays and BAT, for BLs [18,42,44,59], FQs [31] and NMBAs [24,25]. We have used the data from these studies to estimate the diagnostic value obtained by combining the results of both tests. We found an overall mean in vitro sensitivity of 69.9% (Figure 1). Combining immunoassay + BAT results according to the culprit drug showed an increase in sensitivity of around 20%, for both BLs and NMBAs, compared to using only one test. In the only study performed in FQs, the inclusion of RIA had little effect compared to the results obtained with BAT alone (Figure 2a). The specificity of the combined in vitro tests was 90.9% which is in the range of the mean specificity of individual tests (89.2–94.6%).
3.4. Combining In Vitro and In Vivo Tests for Evaluating IDHR
We evaluated the sensitivity obtained when combining the results of both in vivo and in vitro tests, using studies that included ST data. We observed an increase from 65.7% when only in vivo tests are considered, to 75.9% when including both in vitro and in vivo tests (Figure 1). Combining in vivo and in vitro testing lead to an average increase of around 15% in sensitivity over in vivo testing alone for eight studies performed in BLs allergic patients [16,19,20,42,45,60,61,62] as well as for other drugs such as NMBAs [24,48], biological agents [34,36], pyrazolones [55,56] or RCM [57,58] (Figure 1 and Figure 2b). Regarding specificity, it was 91.8%.
It is interesting to note that in vitro tests, such as BAT, can produce positive results in IDHR patients who give negative STs; in fact 40% of ST negative patients with IDHR to BLs give positive BAT results [19,42]; this figure is around 12% for FQs [53] and 30% for pyrazolones [55,56]. These results clearly indicate that the inclusion of in vitro tests complement the results of in vivo testing in the evaluation of IDHR, increasing the diagnostic sensitivity [24]. However, we must take into account that in this test we can found 1–10% false positive results.
4. T Cell-Mediated Reactions
The evaluation of cell-mediated DHR or NIDHR is more complex than for IDHR, mainly due to the heterogeneity of clinical symptoms. These differences in symptoms imply that although in most reactions T cells are involved, many other cell subpopulations are likely to play a critical role [41,63]. It is therefore important to study and characterize effector cells and their corresponding inflammatory mediators.
Most of the in vitro tests used for evaluating NIDHR have as their main goal the assessment of the drug involved in the reaction. The idea is to reproduce the effector reaction in vitro by activating T cells and inducing the appropriate inflammatory and cytotoxic mediator release that will be determined by LTT, ELISpot or ELISA. Most currently available studies for evaluating these types of reactions include small numbers of patients and have included a heterogeneous mix of patients and culprit drugs, generally including BLs, anticonvulsants, local anesthetic and NSAIDs. Another important limitation of these studies is that in most publications, the diagnosis has been confirmed by clinical history and/or STs and did not include DPT. Therefore, we cannot know if a patient would react to the drug. This limitation is compounded by the low sensitivity of STs in this type of reaction [64].
4.1. Lymphocyte Transformation Test (LTT)
This test is based on the determination of the lymphocyte proliferative response after stimulation with the specific drug [12]. This proliferation has classically been measured via the incorporation of tritiated thymidine (3H) into the genome of proliferating cells and assessed by measuring the increase in radioactivity in a liquid scintillation counter system [38]. With advances in flow cytometry, the possibility of assessing proliferation by the serial dilution of a fluorescent molecule (carboxyfluorescein diacetate succinimidyl ester (CFSE)) into the cells has appeared, introducing the possibility of identifying the effector cells involved in the reaction [11]. However, there is a lack of studies comparing these two methods in terms of sensitivity and clinical value [17].
We have analyzed the results of 13 studies [65,66,67,68,69,70,71,72,73,74,75,76,77] of LTT containing at least five patients. We calculated a mean sensitivity of 56.1% and a specificity of 93.9%, while PPV and NPV were 92.3% and 63.2% respectively (Table 3). Higher values were found when evaluating studies including mild and moderate reactions [65,66,67,68,69,70,71,72], showing sensitivity and specificity values of 65.1% and 96.5% with PPV and NPV of 94.4% and 67.2%, respectively. However, these figures decreased when we only included severe reactions [73,74,75,76,77], showing a sensitivity of 39.9%, specificity of 89.8% and PPV and NPV of 87.8% and 52.4%, respectively. These data suggest that LTT is better suited to evaluating moderate NIDHR compared to severe reactions, such as TEN and organ specific reactions [11,12,75].
4.2. Enzyme-Linked Immunosorbent Spot (ELISpot)
ELISpot determines the number of cells producing an inflammatory marker, such as relevant cytokines and cytotoxic markers, after their activation by the specific drug [80]. This method provides both qualitative and quantitative information and has demonstrated to be highly sensitive, enabling the detection of less than 25 secreting cells per 106 peripheral blood mononuclear cells [17,38]. It has been increasingly used for the evaluation of effector cells in NIDHR over the last decades [67,74,77,81,82,83,84]. The six studies using ELISpot that have been included in this review are focused on BLs and/or anticonvulsants and measure the number of cells producing IFN-γ, IL-4, IL-5 or Granzyme B [67,76,77,85,86,87]. Data showed a mean sensitivity of 61.2%, a specificity of 98.6, a PPV of 96.2% and a NPV of 59.1% (Table 3).
4.3. Flow Cytometry and Enzyme-Linked Immunosorbent Assay (ELISA)
Another approach for evaluating NIDHR after stimulation with the specific drug is by the determination of the cell activation and/or cytokines or cytotoxic production by either flow cytometry analysis of cells in culture or ELISA using the culture supernatants [72,79,88,89,90,91,92]. These methodologies have been used for determining IL-2, IL-5, IL-10 and IFN-γ [74,93]. We have included four studies that contained over five patients [74,93,94,95], which found the mean sensitivity of these tests to be 66.6% and the specificity 87.5%, with PPV and NPV being 88.5% and 69.5%, respectively (Table 3).
4.4. Combining In Vitro Tests for Evaluating Non-Immediate Drug Hypersensitivity Reactions (NIDHR)
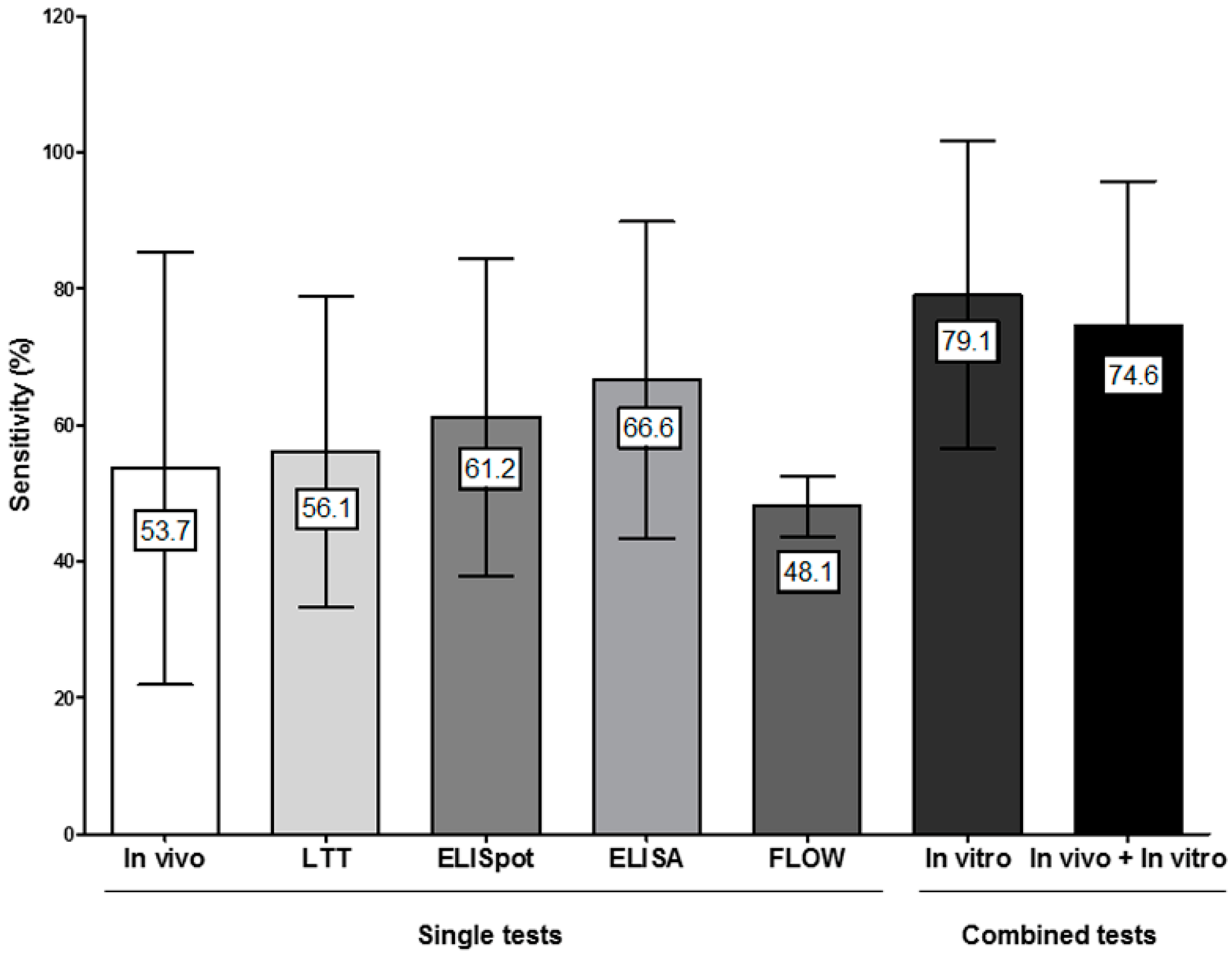
Although the sensitivity of the above-mentioned tests for evaluating NIDHR showed a similar values ranging from 56.1 to 66.6% (Table 3), it has been proposed that the combination of results from different assays could be useful [76,77,93]. Different combinations have been reported, including LTT and a panel of cytokines/cytotoxic molecules determined by ELISpot, flow cytometry and/or ELISA (using IFN-γ, IL-2, IL-4, IL-5, granzyme B and granulysin) [67,74,76,77,85,93]. Here, we have calculated the sensitivity of the combination of the results from different tests including data from those studies that performed at least two different in vitro methods. Results show an increase in sensitivity, up to 79.1% when evaluating patients with both moderate and severe NIDHR to betalactams and anticonvulsants (Figure 3 and Figure 4). The specificity of the combined in vitro tests was 97.5% which is in the range of the specificity of individual tests (87.7–98.6%) (Table 3).
These data indicate that the combination of different in vitro tests could help better identify the culprit drug in these types of reactions.
4.5. Combining In Vitro and In Vivo Tests for Evaluating NIDHR
We further analyzed the sensitivity of the allergological evaluation of NIDHR when the results of in vitro tests were combined with those obtained in in vivo (STs) tests and observed that it increases from 53.7% to 74.6% (Figure 3 and Figure 4). This is very important if we take into account that many of these reactions show severe symptoms and that in many cases in vivo testing cannot be performed.
Interestingly, the mean sensitivity of in vitro tests (79.1%) is higher than those we have obtained when combining in vivo and in vitro results (74.6%), this is because different studies have been included in each case. Most studies that included in vivo sensitivity data used LTT as the in vitro test, which is relatively less sensitive. Thus, more studies including either ELISpot or ELISA/Flow cytometry in combination with skin testing should be performed in order to obtain a more accurate estimate of sensitivity for the in vivo/in vitro evaluation of NIDHR. Regarding specificity, it was 97.8%.
5. Conclusions
DHR diagnosis is a complex and unresolved issue due to the low sensitivity of the different approaches and the possible risks associated with performing DPT, especially for severe reactions, both for IDHR and NIDHR. The data presented in this review indicate that current in vitro methods, although not sufficient by themselves, can be helpful in assessing IDHR and NIDHR, and have been shown to increase the overall sensitivity of the diagnostic procedure when combined with in vivo testing.
They show, in general, a low sensitivity that depends on the drug involved and for those evaluating NIDHR also on the clinical manifestation. The low sensitivity could be related to other factors such as the use of non-appropriate drug metabolite(s) or drug-carrier conjugates that hide the relevant epitopes.
Cellular test has shown similar values of PPV and NPV independently of the type of reaction, IDHR or NIDHR. Additionally, it is important to note that, although NPVs are not optimal, in vitro tests have shown a good specificity, which correlates with a high PPV indicating that they could reduce the number of false positive results and help to decrease the administration of alternative drugs that, as mentioned before, could be less effective and induce undesired side effects. On the other hand, the low sensitivity could have serious effects when falsely labeling a patient as non-allergic, especially for severe reactions.
There is certainly room for improvement in in vitro testing. Areas requiring attention include: characterizing the drug metabolites involved in the reactions and that are recognized by the immunological system; characterizing the effector immunological mechanism involved in order to determine specific biomarkers; and combining results from multiple in vitro and in vivo tests.
Further studies are needed that include a large number of patients and controls and that take into account the combination of in vivo and in vitro tests in order to evaluate the real added value of the latter and therefore the possibility of avoiding the performance of drug provocation tests.
Acknowledgments
We thank James R. Perkins for his help with the final English language version of this manuscript. The present study has been supported by Institute of Health “Carlos III” of the Ministry of Economy and Competitiveness (grants cofunded by European Regional Development Fund (ERDF): PI12/02529, PI15/01206, RETICs RIRAAF (RD12/0013/0001 and RD12/0013/0003) and ARADyAL (RD16/0006/0001 and RD16/0006/0012); the Ministry of Economy and Competitiveness (grants cofunded by European Regional Development Fund (ERDF): CTQ2016-75870-P) and by Andalusian Regional Ministry of Economy and Knowledge (grants cofunded by European Regional Development Fund (ERDF): CTS-06603); Andalusian Regional Ministry Health (grants: PI-0179-2014, PI-0241-2015 and PI-0250-2016). TD Fernandez holds a “Ramon y Cajal” research contract by Ministry of Economy and Competitiveness (RYC-2013-13138). C Mayorga holds a “Nicolas Monardes” research contract by Andalusian Regional Ministry Health: C-0044-2012 SAS 2013. I Doña holds a “Joan Rodes” research contract (JR15/00036) supported by Institute of Health “Carlos III” of the Ministry of Economy and Competitiveness (grants cofunded by European Social Fund (ESF)).
Author Contributions
All authors have made substantial intellectual contributions to the preparation of the manuscript and approved it for publication.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| DHR | Drug Hypersensitivity Reactions |
| SJS | Steven–Johnson Syndrome |
| TEN | Toxic Epidermal Necrolysis |
| IDHR | Immediate DH |
| sIgE | Specific IgE |
| NIDHR | Non-Immediate DHR |
| STs | Skin Tests |
| DPT | Drug Provocation Tests |
| BLs | β-Lactam |
| RCM | Radio Contrast Media |
| BAT | Basophil Activation Test |
| LTT | Lymphocyte Transformation Tests |
| ELISpot | Enzyme-Linked Immunosorbent Spot Assay |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| PPV | Positive Predictive Value |
| NPV | Negative Predictive Value |
| RAST | Radioallergosorbent Test |
| NMBAs | Neuromuscular Blocking Agents |
| FQs | Fluoroquinolones |
| NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
| CFSE | Carboxyfluorescein Diacetate Succinimidyl Ester |
References
- Dona, I.; Blanca-Lopez, N.; Torres, M.J.; Garcia-Campos, J.; Garcia-Nunez, I.; Gomez, F.; Salas, M.; Rondon, C.; Canto, M.G.; Blanca, M. Drug hypersensitivity reactions: Response patterns, drug involved, and temporal variations in a large series of patients. J. Investig. Allergol. Clin. Immunol. 2012, 22, 363–371. [Google Scholar] [PubMed]
- Macy, E.; Contreras, R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: A cohort study. J. Allergy Clin. Immunol. 2014, 133, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Coombs, R.R.A. Classification of allergic reactions responsible for clinical hypersensitivity and disease. In Clinical Aspects of Immunology; Gell, P.G.H., Ed.; Oxford University Press: Oxford, UK, 1968; pp. 575–596. [Google Scholar]
- Pichler, W.J. Delayed drug hypersensitivity reactions. Ann. Int. Med. 2003, 139, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Demoly, P.; Kropf, R.; Bircher, A.; Pichler, W.J. Drug hypersensitivity: Questionnaire. EAACI interest group on drug hypersensitivity. Allergy 1999, 54, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Brockow, K.; Romano, A.; Blanca, M.; Ring, J.; Pichler, W.; Demoly, P. General considerations for skin test procedures in the diagnosis of drug hypersensitivity. Allergy 2002, 57, 45–51. [Google Scholar] [PubMed]
- Demoly, P.; Bousquet, J. Drug allergy diagnosis work up. Allergy 2002, 57 (Suppl. S72), 37–40. [Google Scholar] [CrossRef] [PubMed]
- Benahmed, S.; Picot, M.C.; Dumas, F.; Demoly, P. Accuracy of a pharmacovigilance algorithm in diagnosing drug hypersensitivity reactions. Arch. Int. Med. 2005, 165, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.J.; Romano, A.; Celik, G.; Demoly, P.; Khan, D.A.; Macy, E.; Park, M.; Blumenthal, K.; Aberer, W.; Castells, M.; et al. Approach to the diagnosis of drug hypersensitivity reactions: Similarities and differences between Europe and North America. Clin. Transl. Allergy 2017, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Aberer, W.; Bircher, A.; Romano, A.; Blanca, M.; Campi, P.; Fernandez, J.; Brockow, K.; Pichler, W.J.; Demoly, P.; European Network for Drug Allergy. Drug provocation testing in the diagnosis of drug hypersensitivity reactions: General considerations. Allergy 2003, 58, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Mayorga, C.; Celik, G.; Rouzaire, P.; Whitaker, P.; Bonadonna, P.; Cernadas, J.R.; Vultaggio, A.; Brockow, K.; Caubet, J.C.; Makowska, J.; et al. In vitro tests for drug hypersensitivity reactions: An ENDA/EAACI drug allergy interest group position paper. Allergy 2016, 71, 1103–1134. [Google Scholar] [CrossRef] [PubMed]
- Ebo, D.G.; Leysen, J.; Mayorga, C.; Rozieres, A.; Knol, E.F.; Terreehorst, I. The in vitro diagnosis of drug allergy: Status and perspectives. Allergy 2011, 66, 1275–1286. [Google Scholar] [CrossRef] [PubMed]
- Vultaggio, A.; Matucci, A.; Virgili, G.; Rossi, O.; Fili, L.; Parronchi, P.; Romagnani, S.; Maggi, E. Influence of total serum IgE levels on the in vitro detection of β-lactams-specific IgE antibodies. Clin. Exp. Allergy 2009, 39, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Ariza, A.; Mayorga, C.; Salas, M.; Dona, I.; Martin-Serrano, A.; Perez-Inestrosa, E.; Perez-Sala, D.; Guzman, A.E.; Montanez, M.I.; Torres, M.J. The influence of the carrier molecule on amoxicillin recognition by specific IgE in patients with immediate hypersensitivity reactions to betalactams. Sci. Rep. 2016, 6, 35113. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.J.; Blanca, M.; Moreno, F.; Vega, J.M.; Mayorga, C.; Fernandez, J.; Juarez, C.; Romano, A.; de Ramon, E. Determination of IgE antibodies to the benzylpenicilloyl determinant: A comparison of the sensitivity and specificity of three radio allergo sorbent test methods. J. Clin. Lab. Anal. 1997, 11, 251–257. [Google Scholar] [CrossRef]
- Blanca, M.; Mayorga, C.; Torres, M.J.; Reche, M.; Moya, M.C.; Rodriguez, J.L.; Romano, A.; Juarez, C. Clinical evaluation of Pharmacia CAP System™ RAST FEIA amoxicilloyl and benzylpenicilloyl in patients with penicillin allergy. Allergy 2001, 56, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Doña, I.; Torres, M.J.; Montañez, M.I.; Fernandez, T.D. In vitro diagnostic testing for antibiotic allergy. Allergy Asthma Immunol. Res. 2017, 9, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.L.; Gamboa, P.M.; Antepara, I.; Uasuf, C.; Vila, L.; Garcia-Aviles, C.; Chazot, M.; de Weck, A.L. Flow cytometric basophil activation test by detection of CD63 expression in patients with immediate-type reactions to betalactam antibiotics. Clin. Exp. Allergy 2002, 32, 277–286. [Google Scholar] [CrossRef] [PubMed]
- De Weck, A.L.; Sanz, M.L.; Gamboa, P.M.; Aberer, W.; Sturm, G.; Bilo, M.B.; Montroni, M.; Blanca, M.; Torres, M.J.; Mayorga, L.; et al. Diagnosis of immediate-type β-lactam allergy in vitro by flow-cytometric basophil activation test and sulfidoleukotriene production: A multicenter study. J. Investig. Allergol. Clin. Immunol. 2009, 19, 91–109. [Google Scholar]
- Fontaine, C.; Mayorga, C.; Bousquet, P.J.; Arnoux, B.; Torres, M.J.; Blanca, M.; Demoly, P. Relevance of the determination of serum-specific IgE antibodies in the diagnosis of immediate β-lactam allergy. Allergy 2007, 62, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Aviles, C.; Sanz, M.L.; Gamboa, P.M.; Urrutia, I.; Antepara, I.; Jauregui, I.; de Weck, A.L. Antigen specific quantification of sulfidoleukotrienes in patients allergic to betalactam antibiotics. J. Investig. Allergol. Clin. Immunol. 2005, 15, 37–45. [Google Scholar] [PubMed]
- Vultaggio, A.; Virgili, G.; Gaeta, F.; Romano, A.; Maggi, E.; Matucci, A. High serum β-lactams specific/total IgE ratio is associated with immediate reactions to β-lactams antibiotics. PLoS ONE 2015, 10, e0121857. [Google Scholar] [CrossRef] [PubMed]
- Ebo, D.G.; Venemalm, L.; Bridts, C.H.; Degerbeck, F.; Hagberg, H.; de Clerck, L.S.; Stevens, W.J. Immunoglobulin E antibodies to rocuronium: A new diagnostic tool. Anesthesiology 2007, 107, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Leysen, J.; Bridts, C.H.; de Clerck, L.S.; Vercauteren, M.; Lambert, J.; Weyler, J.J.; Stevens, W.J.; Ebo, D.G. Allergy to rocuronium: From clinical suspicion to correct diagnosis. Allergy 2011, 66, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Monneret, G.; Benoit, Y.; Debard, A.L.; Gutowski, M.C.; Topenot, I.; Bienvenu, J. Monitoring of basophil activation using CD63 and CCR3 in allergy to muscle relaxant drugs. Clin. Immunol. 2002, 102, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Guilloux, L.; Ricard-Blum, S.; Ville, G.; Motin, J. A new radioimmunoassay using a commercially available solid support for the detection of IgE antibodies against muscle relaxants. J. Allergy Clin. Immunol. 1992, 90, 153–159. [Google Scholar] [CrossRef]
- Rouzaire, P.; Proton, G.; Bienvenu, F.; Guilloux, L.; Benoit, Y.; Piriou, V.; Bienvenu, J.; Mertes, P. IgE antibody detection in the diagnosis of hypersensitivity to neuromuscular blocking agents. Acta Anaesthesiol. Scand. 2012, 56, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Mata, E.; Gueant, J.L.; Moneret-Vautrin, D.A.; Bermejo, N.; Gerard, P.; Nicolas, J.P.; Laxenaire, M.C. Clinical evaluation of in vitro leukocyte histamine release in allergy to muscle relaxant drugs. Allergy 1992, 47, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Laroche, D.; Chollet-Martin, S.; Leturgie, P.; Malzac, L.; Vergnaud, M.C.; Neukirch, C.; Venemalm, L.; Gueant, J.L.; Nicaise Roland, P. Evaluation of a new routine diagnostic test for immunoglobulin E sensitization to neuromuscular blocking agents. Anesthesiology 2011, 114, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Garvey, L.H.; Kroigaard, M.; Poulsen, L.K.; Skov, P.S.; Mosbech, H.; Venemalm, L.; Degerbeck, F.; Husum, B. IgE-mediated allergy to chlorhexidine. J. Allergy Clin. Immunol. 2007, 120, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Aranda, A.; Mayorga, C.; Ariza, A.; Dona, I.; Rosado, A.; Blanca-Lopez, N.; Andreu, I.; Torres, M.J. In vitro evaluation of IgE-mediated hypersensitivity reactions to quinolones. Allergy 2011, 66, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; Severino, M.; Testi, S.; Macchia, D.; Ermini, G.; Pichler, W.J.; Campi, P. Detection of specific IgE to quinolones. J. Allergy Clin. Immunol. 2004, 113, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Mirakhur, B.; Chan, E.; Le, Q.T.; Berlin, J.; Morse, M.; Murphy, B.A.; Satinover, S.M.; Hosen, J.; Mauro, D.; et al. Cetuximab-induced anaphylaxis and IgE specific for galactose-α-1,3-galactose. N. Engl. J. Med. 2008, 358, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Vultaggio, A.; Matucci, A.; Nencini, F.; Pratesi, S.; Parronchi, P.; Rossi, O.; Romagnani, S.; Maggi, E. Anti-infliximab IgE and non-IgE antibodies and induction of infusion-related severe anaphylactic reactions. Allergy 2010, 65, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Mariotte, D.; Dupont, B.; Gervais, R.; Galais, M.-P.; Laroche, D.; Tranchant, A.; Comby, E.; Bouhier-Leporrier, K.; Reimund, J.-M.; Le Mauff, B. Anti-cetuximab IgE ELISA for identification of patients at a high risk of cetuximab-induced anaphylaxis. mAbs 2011, 3, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Matucci, A.; Pratesi, S.; Petroni, G.; Nencini, F.; Virgili, G.; Milla, M.; Maggi, E.; Vultaggio, A. Allergological in vitro and in vivo evaluation of patients with hypersensitivity reactions to infliximab. Clin. Exp. Allergy 2013, 43, 659–664. [Google Scholar] [PubMed]
- Hoffmann, H.J.; Santos, A.F.; Mayorga, C.; Nopp, A.; Eberlein, B.; Ferrer, M.; Rouzaire, P.; Ebo, D.G.; Sabato, V.; Sanz, M.L.; et al. The clinical utility of basophil activation testing in diagnosis and monitoring of allergic disease. Allergy 2015, 70, 1393–1405. [Google Scholar] [CrossRef] [PubMed]
- Ariza, A.; Montanez, M.I.; Fernandez, T.D.; Perkins, J.R.; Mayorga, C. Cellular tests for the evaluation of drug hypersensitivity. Curr. Pharm. Des. 2016, 22, 6773–6783. [Google Scholar] [CrossRef] [PubMed]
- Abuaf, N.; Rostane, H.; Rajoely, B.; Gaouar, H.; Autegarden, J.E.; Leynadier, F.; Girot, R. Comparison of two basophil activation markers CD63 and CD203c in the diagnosis of amoxicillin allergy. Clin. Exp. Allergy 2008, 38, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, T.D.; Ariza, A.; Palomares, F.; Montanez, M.I.; Salas, M.; Martin-Serrano, A.; Fernandez, R.; Ruiz, A.; Blanca, M.; Mayorga, C.; et al. Hypersensitivity to fluoroquinolones: The expression of basophil activation markers depends on the clinical entity and the culprit fluoroquinolone. Medicine 2016, 95, e3679. [Google Scholar] [CrossRef] [PubMed]
- Perkins, J.R.; Ariza, A.; Blanca, M.; Fernandez, T.D. Tests for evaluating non-immediate allergic drug reactions. Expert Rev. Clin. Immunol. 2014, 10, 1475–1486. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.J.; Padial, A.; Mayorga, C.; Fernandez, T.; Sanchez-Sabate, E.; Cornejo-Garcia, J.A.; Antunez, C.; Blanca, M. The diagnostic interpretation of basophil activation test in immediate allergic reactions to betalactams. Clin. Exp. Allergy 2004, 34, 1768–1775. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.J.; Ariza, A.; Mayorga, C.; Dona, I.; Blanca-Lopez, N.; Rondon, C.; Blanca, M. Clavulanic acid can be the component in amoxicillin-clavulanic acid responsible for immediate hypersensitivity reactions. J. Allergy Clin. Immunol. 2010, 125, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, B.; Leon Suarez, I.; Darsow, U.; Rueff, F.; Behrendt, H.; Ring, J. A new basophil activation test using CD63 and CCR3 in allergy to antibiotics. Clin. Exp. Allergy 2010, 40, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Morillas, L.; Perez-Ezquerra, P.R.; Reano-Martos, M.; Laguna-Martinez, J.J.; Sanz, M.L.; Martinez, L.M. Selective allergic reactions to clavulanic acid: A report of 9 cases. J. Allergy Clin. Immunol. 2010, 126, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Ebo, D.G.; Bridts, C.H.; Hagendorens, M.M.; Mertens, C.H.; de Clerck, L.S.; Stevens, W.J. Flow-assisted diagnostic management of anaphylaxis from rocuronium bromide. Allergy 2006, 61, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Kvedariene, V.; Kamey, S.; Ryckwaert, Y.; Rongier, M.; Bousquet, J.; Demoly, P.; Arnoux, B. Diagnosis of neuromuscular blocking agent hypersensitivity reactions using cytofluorimetric analysis of basophils. Allergy 2006, 61, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Sudheer, P.S.; Hall, J.E.; Read, G.F.; Rowbottom, A.W.; Williams, P.E. Flow cytometric investigation of peri-anaesthetic anaphylaxis using CD63 and CD203c. Anaesthesia 2005, 60, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Hagau, N.; Gherman-Ionica, N.; Sfichi, M.; Petrisor, C. Threshold for basophil activation test positivity in neuromuscular blocking agents hypersensitivity reactions. Allergy Asthma Clin. Immunol. 2013, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Uyttebroek, A.P.; Sabato, V.; Leysen, J.; Bridts, C.H.; de Clerck, L.S.; Ebo, D.G. Flowcytometric diagnosis of atracurium-induced anaphylaxis. Allergy 2014, 69, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Abuaf, N.; Rajoely, B.; Ghazouani, E.; Levy, D.A.; Pecquet, C.; Chabane, H.; Leynadier, F. Validation of a flow cytometric assay detecting in vitro basophil activation for the diagnosis of muscle relaxant allergy. J. Allergy Clin. Immunol. 1999, 104, 411–418. [Google Scholar] [CrossRef]
- Mayorga, C.; Andreu, I.; Aranda, A.; Dona, I.; Montanez, M.I.; Blanca-Lopez, N.; Ariza, A.; Nuin, E.; Blanca, M.; Miranda, M.A.; et al. Fluoroquinolone photodegradation influences specific basophil activation. Int. Arch. Allergy Immunol. 2013, 160, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Rouzaire, P.; Nosbaum, A.; Denis, L.; Bienvenu, F.; Berard, F.; Cozon, G.; Bienvenu, J. Negativity of the basophil activation test in quinolone hypersensitivity: A breakthrough for provocation test decision-making. Int. Arch. Allergy Immunol. 2012, 157, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Hagau, N.; Longrois, D.; Petrisor, C. Threshold for positivity and optimal dipyrone concentration in flow cytometry-assisted basophil activation test. Allergy Asthma Immunol. Res. 2013, 5, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, P.M.; Sanz, M.L.; Caballero, M.R.; Antepara, I.; Urrutia, I.; Jauregui, I.; Gonzalez, G.; Dieguez, I.; de Weck, A.L. Use of CD63 expression as a marker of in vitro basophil activation and leukotriene determination in metamizol allergic patients. Allergy 2003, 58, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Gomez, E.; Blanca-Lopez, N.; Torres, M.J.; Requena, G.; Rondon, C.; Canto, G.; Blanca, M.; Mayorga, C. Immunoglobulin E-mediated immediate allergic reactions to dipyrone: Value of basophil activation test in the identification of patients. Clin. Exp. Allergy 2009, 39, 1217–1224. [Google Scholar] [CrossRef] [PubMed]
- Pinnobphun, P.; Buranapraditkun, S.; Kampitak, T.; Hirankarn, N.; Klaewsongkram, J. The diagnostic value of basophil activation test in patients with an immediate hypersensitivity reaction to radiocontrast media. Ann. Allergy Asthma Immunol. 2011, 106, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Salas, M.; Gomez, F.; Fernandez, T.D.; Dona, I.; Aranda, A.; Ariza, A.; Blanca-Lopez, N.; Mayorga, C.; Blanca, M.; Torres, M.J. Diagnosis of immediate hypersensitivity reactions to radiocontrast media. Allergy 2013, 68, 1203–1206. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Ortega, P.; Marin, A. Usefulness of the basophil activation test (BAT) in the diagnosis of life-threatening drug anaphylaxis. Allergy 2010, 65, 1204. [Google Scholar] [CrossRef] [PubMed]
- Antunez, C.; Blanca-Lopez, N.; Torres, M.J.; Mayorga, C.; Perez-Inestrosa, E.; Montanez, M.I.; Fernandez, T.; Blanca, M. Immediate allergic reactions to cephalosporins: Evaluation of cross-reactivity with a panel of penicillins and cephalosporins. J. Allergy Clin. Immunol. 2006, 117, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Gueant-Rodriguez, R.M.; Viola, M.; Amoghly, F.; Gaeta, F.; Nicolas, J.P.; Gueant, J.L. Diagnosing immediate reactions to cephalosporins. Clin. Exp. Allergy 2005, 35, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.J.; Romano, A.; Mayorga, C.; Moya, M.C.; Guzman, A.E.; Reche, M.; Juarez, C.; Blanca, M. Diagnostic evaluation of a large group of patients with immediate allergy to penicillins: The role of skin testing. Allergy 2001, 56, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Mayorga, C.; Pena, R.R.; Blanca-Lopez, N.; Lopez, S.; Martin, E.; Torres, M.J. Monitoring the acute phase response in non-immediate allergic drug reactions. Curr. Opin. Allergy Clin. Immunol. 2006, 6, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Barbaud, A. Skin testing and patch testing in non-IgE-mediated drug allergy. Curr. Allergy Asthma Rep. 2014, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, P.; Meng, X.; Lavergne, S.N.; El-Ghaiesh, S.; Monshi, M.; Earnshaw, C.; Peckham, D.; Gooi, J.; Conway, S.; Pirmohamed, M.; et al. Mass spectrometric characterization of circulating and functional antigens derived from piperacillin in patients with cystic fibrosis. J. Immunol. 2011, 187, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Schnyder, B.; Pichler, W.J. Skin and laboratory tests in amoxicillin- and penicillin-induced morbilliform skin eruption. Clin. Exp. Allergy 2000, 30, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Rozieres, A.; Hennino, A.; Rodet, K.; Gutowski, M.C.; Gunera-Saad, N.; Berard, F.; Cozon, G.; Bienvenu, J.; Nicolas, J.F. Detection and quantification of drug-specific T cells in penicillin allergy. Allergy 2009, 64, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Pena, R.; Lopez, S.; Mayorga, C.; Antunez, C.; Fernandez, T.D.; Torres, M.J.; Blanca, M. Potential involvement of dendritic cells in delayed-type hypersensitivity reactions to β-lactams. J. Allergy Clin. Immunol. 2006, 118, 949–956. [Google Scholar] [CrossRef] [PubMed]
- Orasch, C.E.; Helbling, A.; Zanni, M.P.; Yawalkar, N.; Hari, Y.; Pichler, W.J. T-cell reaction to local anaesthetics: Relationship to angioedema and urticaria after subcutaneous application—Patch testing and LTT in patients with adverse reaction to local anaesthetics. Clin. Exp. Allergy 1999, 29, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Nyfeler, B.; Pichler, W.J. The lymphocyte transformation test for the diagnosis of drug allergy: Sensitivity and specificity. Clin. Exp. Allergy 1997, 27, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Luque, I.; Leyva, L.; Jose Torres, M.; Rosal, M.; Mayorga, C.; Segura, J.M.; Blanca, M.; Juarez, C. In vitro T-cell responses to β-lactam drugs in immediate and nonimmediate allergic reactions. Allergy 2001, 56, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Hari, Y.; Frutig-Schnyder, K.; Hurni, M.; Yawalkar, N.; Zanni, M.P.; Schnyder, B.; Kappeler, A.; von Greyerz, S.; Braathen, L.R.; Pichler, W.J. T cell involvement in cutaneous drug eruptions. Clin. Exp. Allergy 2001, 31, 1398–1408. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Miwa, S.; Shirai, M.; Ohba, H.; Murakami, M.; Fujita, K.; Suda, T.; Nakamura, H.; Hayakawa, H.; Chida, K. Drug lymphocyte stimulation test in the diagnosis of adverse reactions to antituberculosis drugs. Chest 2008, 134, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Sachs, B.; Erdmann, S.; Malte Baron, J.; Neis, M.; Al Masaoudi, T.; Merk, H.F. Determination of interleukin-5 secretion from drug-specific activated ex vivo peripheral blood mononuclear cells as a test system for the in vitro detection of drug sensitization. Clin. Exp. Allergy 2002, 32, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Roujeau, J.C.; Albengres, E.; Moritz, S.; Piacentino, A.; Cuny, M.; Revuz, J.; Touraine, R. Lymphocyte transformation test in drug-induced toxic epidermal necrolysis. Int. Arch. Allergy Appl. Immunol. 1985, 78, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Porebski, G.; Pecaric-Petkovic, T.; Groux-Keller, M.; Bosak, M.; Kawabata, T.T.; Pichler, W.J. In vitro drug causality assessment in Stevens-Johnson syndrome-alternatives for lymphocyte transformation test. Clin. Exp. Allergy 2013, 43, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Polak, M.E.; Belgi, G.; McGuire, C.; Pickard, C.; Healy, E.; Friedmann, P.S.; Ardern-Jones, M.R. In vitro diagnostic assays are effective during the acute phase of delayed-type drug hypersensitivity reactions. Br. J. Dermatol. 2013, 168, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Antunez, C.; Barbaud, A.; Gomez, E.; Audonnet, S.; Lopez, S.; Gueant-Rodriguez, R.M.; Aimone-Gastin, I.; Gomez, F.; Blanca, M.; Gueant, J.L. Recognition of iodixanol by dendritic cells increases the cellular response in delayed allergic reactions to contrast media. Clin. Exp. Allergy 2011, 41, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Quintero, M.J.; Torres, M.J.; Blazquez, A.B.; Gomez, E.; Fernandez, T.D.; Dona, I.; Ariza, A.; Andreu, I.; Melendez, L.; Blanca, M.; et al. Synergistic effect between amoxicillin and TLR ligands on dendritic cells from amoxicillin-delayed allergic patients. PLoS ONE 2013, 8, e74198. [Google Scholar] [CrossRef] [PubMed]
- Czerkinsky, C.; Moldoveanu, Z.; Mestecky, J.; Nilsson, L.A.; Ouchterlony, O. A novel two colour ELISPOT assay: I. Simultaneous detection of distinct types of antibody-secreting cells. J. Immunol. Methods 1988, 115, 31–37. [Google Scholar] [CrossRef]
- Lochmatter, P.; Beeler, A.; Kawabata, T.T.; Gerber, B.O.; Pichler, W.J. Drug-specific in vitro release of IL-2, IL-5, IL-13 and IFN-γ in patients with delayed-type drug hypersensitivity. Allergy 2009, 64, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Naisbitt, D.J.; Farrell, J.; Wong, G.; Depta, J.P.; Dodd, C.C.; Hopkins, J.E.; Gibney, C.A.; Chadwick, D.W.; Pichler, W.J.; Pirmohamed, M.; et al. Characterization of drug-specific T cells in lamotrigine hypersensitivity. J. Allergy Clin. Immunol. 2003, 111, 1393–1403. [Google Scholar] [CrossRef] [PubMed]
- Zawodniak, A.; Lochmatter, P.; Yerly, D.; Kawabata, T.; Lerch, M.; Yawalkar, N.; Pichler, W.J. In vitro detection of cytotoxic T and NK cells in peripheral blood of patients with various drug-induced skin diseases. Allergy 2010, 65, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Rozieres, A.; Vocanson, M.; Said, B.B.; Nosbaum, A.; Nicolas, J.F. Role of T cells in nonimmediate allergic drug reactions. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Tanvarasethee, B.; Buranapraditkun, S.; Klaewsongkram, J. The potential of using enzyme-linked immunospot to diagnose cephalosporin-induced maculopapular exanthems. Acta Derm. Venereol. 2013, 93, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Klaewsongkram, J.; Thantiworasit, P.; Suthumchai, N.; Rerknimitr, P.; Sukasem, C.; Tuchinda, P.; Chularojanamontri, L.; Srinoulprasert, Y.; Rerkpattanapipat, T.; Chanprapaph, K.; et al. In vitro test to confirm diagnosis of allopurinol-induced severe cutaneous adverse reactions. Br. J. Dermatol. 2016, 175, 994–1002. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Kawase, A.; Azukizawa, H.; Hanafusa, T.; Nakagawa, Y.; Murota, H.; Sakaguchi, S.; Asada, H.; Katayama, I. Novel interferon-γ enzyme-linked immunoSpot assay using activated cells for identifying hypersensitivity-inducing drug culprits. J. Dermatol. Sci. 2017, 86, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Mauri-Hellweg, D.; Bettens, F.; Mauri, D.; Brander, C.; Hunziker, T.; Pichler, W.J. Activation of drug-specific CD4+ and CD8+ T cells in individuals allergic to sulfonamides, phenytoin, and carbamazepine. J. Immunol. 1995, 155, 462–472. [Google Scholar] [PubMed]
- Yawalkar, N.; Shrikhande, M.; Hari, Y.; Nievergelt, H.; Braathen, L.R.; Pichler, W.J. Evidence for a role for IL-5 and eotaxin in activating and recruiting eosinophils in drug-induced cutaneous eruptions. J. Allergy Clin. Immunol. 2000, 106, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Beeler, A.; Zaccaria, L.; Kawabata, T.; Gerber, B.O.; Pichler, W.J. CD69 upregulation on T cells as an in vitro marker for delayed-type drug hypersensitivity. Allergy 2008, 63, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Cornejo-Garcia, J.A.; Fernandez, T.D.; Torres, M.J.; Carballo, M.; Hernan, I.; Antunez, C.; Blanca, M.; Mayorga, C. Differential cytokine and transcription factor expression in patients with allergic reactions to drugs. Allergy 2007, 62, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, T.D.; Mayorga, C.; Torres, M.J.; Cornejo-Garcia, J.A.; Lopez, S.; Chaves, P.; Rondon, C.; Blanca, M. Cytokine and chemokine expression in the skin from patients with maculopapular exanthema to drugs. Allergy 2008, 63, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Wurpts, G.; Ott, H.; Baron, J.M.; Erdmann, S.; Merk, H.F.; Sachs, B. In vitro detection and characterization of drug hypersensitivity using flow cytometry. Allergy 2010, 65, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Khalil, G.; El-Sabban, M.; Al-Ghadban, S.; Azzi, S.; Shamra, S.; Khalife, S.; Maroun, R. Cytokine expression profile of sensitized human T lymphocytes following in vitro stimulation with amoxicillin. Eur. Cytokine Netw. 2008, 19, 131–141. [Google Scholar] [PubMed]
- Halevy, S.; Grossman, N. Multiple drug allergy in patients with cutaneous adverse drug reactions diagnosed by in vitro drug-induced interferon-γ release. Isr. Med. Assoc. J. 2008, 10, 865–868. [Google Scholar] [PubMed]
Figure 1.
Bars represent the global sensitivity (mean plus standard deviation) for in vivo and in vitro tests alone or in combination for the evaluation of immediate drug hypersensitivity reactions (IDHR). BAT: Basophil activation test.
Figure 1.
Bars represent the global sensitivity (mean plus standard deviation) for in vivo and in vitro tests alone or in combination for the evaluation of immediate drug hypersensitivity reactions (IDHR). BAT: Basophil activation test.

Figure 2.
(a) Bars represent the sensitivity of immunoassays (white bars), basophil activation test (BAT) (light grey bars) and immunoassay + BAT (dark grey bars) in individual studies performed with patients with IDHR to BLs, FQs or NMBAs; and (b) Bars represent the sensitivity of in vitro tests (including immunoassay and BAT) (white bars), in vivo tests (light grey bars) and combination of the results of both in vitro and in vivo tests (dark grey bars) in individual studies performed with patients with IDHR to different drug groups. BLs: β-lactams; FQ: Fluoroquinolones; NMBAs: Neuromuscular blocking agents; and RCM: Radio contrast media.
Figure 2.
(a) Bars represent the sensitivity of immunoassays (white bars), basophil activation test (BAT) (light grey bars) and immunoassay + BAT (dark grey bars) in individual studies performed with patients with IDHR to BLs, FQs or NMBAs; and (b) Bars represent the sensitivity of in vitro tests (including immunoassay and BAT) (white bars), in vivo tests (light grey bars) and combination of the results of both in vitro and in vivo tests (dark grey bars) in individual studies performed with patients with IDHR to different drug groups. BLs: β-lactams; FQ: Fluoroquinolones; NMBAs: Neuromuscular blocking agents; and RCM: Radio contrast media.

Figure 3.
Bars represent the global sensitivity of different in vivo and in vitro tests (mean plus standard deviation), either alone or in combination, for the evaluation of non-immediate drug hypersensitivity reactions (NIDHR).
Figure 3.
Bars represent the global sensitivity of different in vivo and in vitro tests (mean plus standard deviation), either alone or in combination, for the evaluation of non-immediate drug hypersensitivity reactions (NIDHR).

Figure 4.
Bars represent the sensitivity of in vitro tests (white bars), in vivo tests (light grey bars) and combination of the results of both in vitro and in vivo tests (dark grey bars) in individual studies performed with NIDHR patients.
Figure 4.
Bars represent the sensitivity of in vitro tests (white bars), in vivo tests (light grey bars) and combination of the results of both in vitro and in vivo tests (dark grey bars) in individual studies performed with NIDHR patients.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Immunoassays in immediate reactions to different drugs.
| Paper | Patients | Drugs | Diag | Method | Sens (%) | Spec (%) | NPV (%) | PPV (%) |
|---|---|---|---|---|---|---|---|---|
| Betalactams | ||||||||
| Garcia 1997 [15] | 30 Pat 30 Cont | PG | ST | RAST | 86.66 | 90 | 87.09 | 89.65 |
| Blanca 2001 [16] | 74 Pat 55 Cont | AX, PG | ST, DPT | CAP | 50 | 96 | 58.8 | 94.4 |
| Sanz 2002 [18] | 58 Pat 30 Cont | PG, AX, AMP, CEFU, CEFAZ | ST | CAP | 37.9 | 86.7 | 41.9 | 84.6 |
| Garcia-Aviles 2005 [21] | 67 Pat 30 Cont | AX, PG CEFU, CEPHA | ST, DPT | CAP | 37.8 | 83.3 | 37.5 | 83.5 |
| Fontaine 2007 [20] | 30 Pat 15 Cont | AX, PG, AMP, CEFOT, CEFT, CEPH, CEFAC | ST, DPT | RAST | 50 | 73.3 | 42.3 | 78.9 |
| CAP | 16.6 | 93.3 | 35.9 | 83.2 | ||||
| De Weck 2009 [19] | 178 Pat 81 Cont | BP, AX, AMP, CEFs | ST, DPT | CAP | 28.3 | 86.5 | 35.4 | 82.1 |
| Vultaggio 2009 [13] | 61 Pat 115 Cont | PG, PV, AX, AMP | ST | CAP | 85 | 54 | 87.2 | 49.5 |
| Vultaggio 2015 [22] | 171 Pat 122 Cont | PG, PV, AX, AMP | ST | CAP | 66 | 52 | 52.2 | 65.8 |
| CAP | 43 | 95 | 54.3 | 92.3 | ||||
| Mean Values | 50.1 | 81.01 | 53.3 | 80.4 | ||||
| SD | 23.0 | 16.2 | 19.6 | 13.5 | ||||
| Quinolones | ||||||||
| Manfredi 2004 [32] | 55 Pat 32 Cont | CIPRO, LOME, NORFL, OFLO, PIP, RUFL, PEFL, NALI | CH | SEPH | 54.5 | 100 | 56.1 | 100 |
| Aranda 2011 [31] | 38 Pat 25 Cont | CIPRO, MOXI, LEVO | CH, DPT | SEPH | 31.6 | 100 | 49.0 | 100 |
| Mean Values | 43.1 | 100 | 52.6 | 100 | ||||
| SD | 16.19 | 0 | 5.0 | 0 | ||||
| NMBAs | ||||||||
| Guilloux 1992 [26] | 31 Pat 34 Cont | MOR, SUC, ALCU, TMA, TEA | ST | RIA | 96.7 | 97.2 | 96.9 | 96.9 |
| Mata 1992 [28] | 40 Pat 44 Cont | SUX, VECU, PANCU, ALCU, ATRAC, GALLA | CH, ST | SEPH | 82.5 | 100 | 86.2 | 100 |
| Monneret 2002 [25] | 39 Pat 17 Cont | ROC, SUX, ATRAC | CH, ST | RIA | 62 | 100 | 53.4 | 100 |
| Ebo 2007 [23] | 25 Pat 30 Cont | ROC, SUX, MOR, PHO | ST | CAP | ROC: 92 | ROC: 93 | ROC: 93.3 | ROC: 92 |
| SUX: 72 | SUX: 100 | SUX: 81.1 | SUX: 100 | |||||
| MOR: 88 | MOR: 100 | MOR: 90.9 | MOR: 100 | |||||
| PHO: 86 | PHO: 100 | PHO: 89.5 | PHO: 100 | |||||
| Leysen 2011 [24] | 41 Pat 25 Cont | ROC | CH, ST | CAP | 82.9 | 72.0 | 72.1 | 82.9 |
| Laroche 2011 [29] | 57 Pat 54 Cont | MOR | CH, ST | CAP | 84.2 | 90.7 | 84.2 | 90.7 |
| Rouzaire 2012 [27] | 11 Pat 20 Cont | ROC, SUX, MOR | CH, ST | CAP | SUX: 44 | SUX: 100 | SUX: 76.4 | SUX: 100 |
| ROC: 83 | ROC: 68 | ROC: 87.9 | ROC: 59 | |||||
| MOR: 78 | MOR: 85 | MOR: 87.5 | MOR: 74 | |||||
| Mean Values | 79.3 | 92.2 | 83.3 | 91.3 | ||||
| SD | 14.3 | 11.4 | 11.7 | 13.1 | ||||
| Clorhexidine | ||||||||
| Garvey 2007 [30] | 12 Pat 10 Cont | CHLOR | ST | CAP | 91.6 | 100 | 90.8 | 100 |
| Biological Agents | ||||||||
| Chung 2008 [33] | 26 Pat 512 Cont | CETUX | CH, DPT | CAP | 68.0 | 98.0 | 98.4 | 63.3 |
| Vultaggio 2010 [34] | 11 Pat 20 Cont | INFLIX | CH | CAP | 27.2 | 100 | 71.4 | 100 |
| Mariotte 2011 [35] | 14 Pat 195 Cont | CETUX | CH | ELISA | 71.4 | 82.1 | 97.6 | 22.3 |
| Matucci 2013 [36] | 30 Pat 50 Cont | INFLIX | CH, ST | CAP | 26.0 | 90.0 | 66.9 | 60.9 |
| Mean Values | 48.2 | 92.5 | 83.6 | 61.6 | ||||
| SD | 24.9 | 8.2 | 16.8 | 31.7 | ||||
Pat: Patients; Cont: Controls; PG: Penicillin G; AX: Amoxicillin; AMP: Ampicillin; CEFU: Cefuroxime; CEFAZ: Cefazolin; CEFs: Cephalosporins; CEFOT: Cefotaxime; CEFT: Ceftriaxone; CEFAC: Cefaclor; PV: Penicillin V; CIPRO: Ciprofloxacin; LOME: Lomefloxacin; NORFLO: Norfloxacin; OFLO: Ofloxacin; PIP: pipemidic acid; RUFL: rufloxacin; PEFL: pefloxacin; NALI: nalidixic acid; MOXI: Moxifloxacin; LEVO: Levofloxacin; MOR: Morphine; SUC: succinylcholine; ALCU: Alcuronium; TMA: trimethylamine; TEA: triethylamine; SUX: sulfamethoxazole; VECU: vecuronium; PANCU: pancuronium; ATRAC: Atracurium; GALLA: gallamine; ROC: Rocuronium; PHO: pholcodine; CHLOR: Clorhexidine; CETUX: Cetuximab; INFLIX: Infliximab; Diag: Diagnostic method; ST: Skin test; DPT: Drug provocation test; CH: Clinical History; RAST: Radioallergosorbent test; CAP: ImmunoCAP-FEIA; SEPH: Sepharose; RIA: Radioimmunoassay; ELISA: Enzyme-linked immunosorbent assay; Sens: sensitivity; Spec: specificity; NPV: negative predictive value; PPV: positive predictive value; and SD: standard deviation.
Table 2.
Basophil activation tests in immediate reactions to different drugs.
| Paper | Patients | Drugs | Diag | Method | Sens (%) | Spec (%) | NPV (%) | PPV (%) |
|---|---|---|---|---|---|---|---|---|
| Betalactam | ||||||||
| Sanz 2002 [18] | 58 Pat 30 Cont | PG, AX, AMP, CEFU, CEFAZ | ST | BAT | 50 | 93.3 | 49.1 | 93.5 |
| Torres 2004 [42] | 70 Pat 40 Cont | PG, AX, AMP, CEFU, CEFAZ, CEFAC | ST, DPT | BAT | 48.6 | 93 | 50.8 | 92.4 |
| Abuaf 2008 [39] | 27 Pat 14 Cont | AX, AMP, CEFU | ST | BAT | 63 | 79 | 52.5 | 85.2 |
| De Weck 2009 [19] | 178 Pat 81 Cont | BP, AX, AMP, CEFs | ST, DPT | BAT | 48.3 | 88.9 | 43.8 | 90.5 |
| Torres 2010 [43] | 55 Pat 30 Cont | PG, AX, AX-CLV, CLV | ST | BAT | 52.7 | 90 | 50.9 | 90.6 |
| Eberlein 2010 [44] | 24 Pat 15 Cont | PG, PV, AMP, AX, CEFU | ST | BAT | 55 | 80 | 52.6 | 81.5 |
| Sanchez-Morillas 2010 [45] | 9 Pat 5 Cont | CLV | ST, DPT | BAT | 44.4 | 100 | 49.9 | 100 |
| Mean Values | 51.7 | 89.2 | 50.0 | 90.5 | ||||
| SD | 6.0 | 7.5 | 3.0 | 5.9 | ||||
| Fluoroquinolones | ||||||||
| Aranda 2011 [31] | 38 Pat 25 Cont | CIPRO, MOXI, LEVO | CH, DPT | BAT | 71.1 | 88 | 66.7 | 90.1 |
| Rouzaire 2012 [53] | 17 Pat 15 Cont | CIPRO, MOXI, LEVO, OFLOX, LOME, FLUME, NORFLO, PIPEMI | ST, DPT | BAT | 76.5 | 100 | 78.9 | 100 |
| Mayorga 2013 [52] | 28 Pat 20 Cont | CIPRO, MOXI | CH, DPT | BAT | 57.1 | 90 | 59.9 | 88.9 |
| Fernandez 2016 [40] | 17 Pat 18 Cont | CIPRO, MOXI | CH, DPT | BAT | 52.9 | 88.9 | 66.7 | 81.8 |
| Mean Values | 64.4 | 91.7 | 68.1 | 90.2 | ||||
| SD | 11.2 | 5.6 | 7.9 | 7.5 | ||||
| NMBAs | ||||||||
| Abuaf 1999 [51] | 21 Pat 29 Cont | SUX, GALLA, VECU, PAN | CH, ST | BAT | 64.0 | 93.0 | 78.1 | 86.9 |
| Monneret 2002 [25] | 39 Pat 17 Cont | ROC, SUX, ATRAC | CH, ST | BAT | 54.0 | 100 | 48.6 | 100 |
| Sudheer 2005 [48] | 14 Pat 10 Cont | ROC, ATRAC, SUX, VECU | CH, ST | BAT | 78.6 | 100 | 76.9 | 100 |
| Ebo 2006 [46] | 14 Pat 8 Cont | ROC | ST | BAT | 91.7 | 100 | 87.3 | 100 |
| Kvedariene 2006 [47] | 47 Pat 45 Cont | ROC, VECU, ATRA, PAN, SUX | ST, DPT | BAT | 36.1 | 93.3 | 58.3 | 84.9 |
| Leysen 2011 [24] | 41 Pat 25 Cont | ROC | CH, ST | BAT | 80.5 | 96.0 | 74.5 | 97.0 |
| Hagau 2013 [49] | 22 Pat 34 Cont | ATRAC, ROC, SUX, PAN | ST | BAT | 68.2 | 100 | 82.9 | 100 |
| Uyttebroek 2014 [50] | 8 Pat 7 Cont | ATRA | ST | BAT | 62.5 | 100 | 70.0 | 100 |
| Mean Values | 66.9 | 97.8 | 72.1 | 96.1 | ||||
| SD | 17.2 | 3.2 | 12.9 | 6.4 | ||||
| Pyrazolones | ||||||||
| Gamboa 2003 [55] | 26 Pat 30 Cont | META | ST, DPT | BAT | 42.3 | 100 | 66.7 | 100 |
| Gomez 2009 [56] | 51 Pat 56 Cont | META | CH, ST, DPT | BAT | 54.9 | 85.7 | 65.1 | 79.6 |
| Hagau 2013 [54] | 20 Pat 10 Cont | DIP | ST | BAT | 65.0 | 100 | 58.8 | 100 |
| Mean Values | 54.1 | 95.2 | 63.5 | 93.2 | ||||
| SD | 11.4 | 8.3 | 4.2 | 11.8 | ||||
| Radio Contrast Media | ||||||||
| Pinnobphun 2011 [57] | 26 Pat 43 Cont | IOXIT, IOPR, IOPA, IOH, IOB | CH, ST | BAT | 57.7 | 97.7 | 79.3 | 93.8 |
| Salas 2013 [58] | 8 Pat 20 Cont | IOD, IOH, IOM, IOB | ST, DPT | BAT | 62.5 | 100 | 86.9 | 100 |
| Mean Values | 60.1 | 98.9 | 83.1 | 96.9 | ||||
| SD | 3.4 | 1.6 | 5.4 | 4.4 | ||||
Pat: Patients; Cont: Controls; PG: Penicillin G; AX: Amoxicillin; AMP: Ampicillin; CEFU: Cefuroxime; CEFAZ: Cefazolin; CEFAC: Cefaclor; CEFs: Cephalosporins; CLV: Clavulanic acid; CIPRO: Ciprofloxacin; MOXI: Moxifloxacin; LEVO: Levofloxacin; OFLO: Ofloxacin; LOME: Lomefloxacin; FLUME: Flumequin; NORFLO: Norfloxacin; PIPEMI: Pipedimic acid; SUX: Suxamethonium; GALLA: gallamine; VECU: Vecuronium; PAN: Pancuronium; ROC: Rocuronium; ATRAC: Atracurium; META: Metamizole; DIP: Dipirone; IOXIT: Ioxithalamate; IOPR: Iopromide; IOPA: Iopamidol; IOH: Iohexol; IOB: Iobbitrol; IOD: Iodixanol; IOM: Iomeprol; Diag: Diagnostic method; CH: Clinical History; ST: Skin test; DPT: Drug provocation test; BAT: Basophil activation test; Sens: sensitivity; Spec: specificity; NPV: negative predictive value; PPV: positive predictive value; and SD: standard deviation.
Table 3.
In vitro tests in non-immediate reactions to different drugs.
| Paper | Patients | Clinical Entity | Drugs | Diag | Method | Sens (%) | Spec (%) | NPV (%) | PPV (%) |
|---|---|---|---|---|---|---|---|---|---|
| LTT | |||||||||
| Roujeau 1985 [75] | 12 Pats 8 Cont | TEN | Ant-Con, NSAID | CH | Thymidine | 44.0 | 63.0 | 42.9 | 64.1 |
| Nyfeler 1997 [70] | 100 Pat 102 Cont | ND | BLs | CH, ST | Thymidine | 74.4 | 85.0 | 77.2 | 82.9 |
| Orasch 1999 [69] | 10 Pat 6 Cont | URT/ANG, EXANT | LA | CH, ST | Thymidine | 60.0 | 100 | 60.0 | 100 |
| Schnyder 2000 [66] | 12 Pat 6 Cont | EXANT | BLs | CH | Thymidine | 83.3 | 100 | 74.9 | 100 |
| Luque 2001 [71] | 19 Pat 28 Cont | URT, EXANT | BLs | ST, DPT | Thymidine | 57.9 | 92.8 | 76.5 | 84.5 |
| Hari 2001 [72] | 21 Pat 16 Cont | MPE, BULL-EXANT, URT | Ant-Con, Ant-hyp, others | CH | Thymidine | 66.6 | 93.8 | 68.2 | 93.4 |
| Sachs 2002 [74] | 10 Pat 10 Cont | MPE, AGEP, TEN | BLs, Ant-Con | CH, ST | Thymidine | 75.0 | 100 | 80.0 | 100 |
| Rodriguez-Pena 2006 [68] | 9 Pat 8 Cont | MPE | BLs | CH, ST | Thymidine | 22.2 | 100 | 53.3 | 100 |
| + DC | 88.8 | 100 | 88.8 | 100 | |||||
| Suzuki 2008 [73] | 69 Pat 50 Cont | BULL- EXANT, DILI | Ant-tub | CH, DPT | Thymidine | 28.9 | 90.7 | 48.03 | 81.1 |
| Rozieres 2009 [67] | 22 Pat 11 Cont | MPE | BLs | ST | Thymidine | 68.2 | 100 | 61.1 | 100 |
| Whitaker 2011 [65] | 28 Pat | URT/ANG, MPE, others | BLs | CH | Thymidine | 64.3 | ND | ND | ND |
| Polak 2013 [77] | 43 Pat 14 Cont | MPE, DRESS, TEN, FDE, ECZ | Various | CH | Thymidine | 25.0 | 95.1 | 29.2 | 94.0 |
| Porebski 2013 [76] | 15 Pat 18 Cont | SJS/TEN | Ant-Con | CH | Thymidine | 26.6 | 100 | 62.0 | 100 |
| Mean Values | 56.1 | 93.9 | 63.2 | 92.3 | |||||
| SD | 22.7 | 10.4 | 16.8 | 11.1 | |||||
| ELISpot | |||||||||
| Rozieres 2009 [67] | 22 Pat 11 Cont | MPE | BLs | ST | IFN-γ | 90.9 | 100 | 84.6 | 100 |
| Polak 2013 [77] | 43 Pat 14 Cont | MPE, DRESS, TEN, FDE, ECZ | Various | CH | IFN-γ, IL-4 | IFNγ: 50.0 IL-4: 50.0 | IFNγ: 82.9 IL-4: 92.0 | IFNγ: 35.1 IL-4: 37.5 | IFNγ:90.0 IL-4: 95.0 |
| Porebski 2013 [76] | 15 Pat 18 Cont | SJS/TEN | Ant-Con | CH | GranzymeB | 33.3 | 98.0 | 63.8 | 93.3 |
| Tanvarasethee 2013 [85] | 25 Pat 20 Cont | MPE | BLs | CH | IFN-γ, IL-5 | 40.0 | 100 | 57.1 | 100 |
| Klaewsongkram 2016 [86] | 24 Pat 21 Cont | DRESS, SJS/TEN | Allop | CH | IFN-γ | 79.2 | 95.2 | 80.0 | 95.0 |
| Kato 2017 [87] | 16 Pat 3 Cont | EXANT, DRESS, TEN, SJS | Ant-Con | CH | IFN-γ | 85.0 | 100 | 55.5 | 100 |
| Mean Values | 61.2 | 98.6 | 59.1 | 96.2 | |||||
| SD | 23.3 | 6.3 | 19.0 | 3.9 | |||||
| ELISA+Flow Cytomety | |||||||||
| Sachs 2002 [74] | 10 Pat 10 Cont | MPE, AGEP, TEN | BLs, Ant-Con | CH, ST | IL-5, IFN-γ, IL-10 | IL5: 91.6 IFNγ: 36.4 IL10: 50.0 | IL5: 100 IFNγ: 60.0 IL10: 100 | IL5: 92.3 IFNγ: 48.5 IL10: 66.7 | IL5: 100 IFNγ: 47.6 IL10: 100 |
| Khalil 2008 [94] | 15 Pat 12 Cont | URT/ANG, MPE | BLs | ST | IL-2, IL-5, IFN-γ | IL-2: 86.7 IL-5: 100 IFNγ: 78.5 | IL-2: 100 IL-5: 62.5 IFNγ: 90.0 | IL-2: 85.7 IL-5: 100 IFNγ: 77.1 | IL-2: 100 IL-5: 76.9 IFNγ: 90.8 |
| Halevy 2008 [95] | 12 Pat 11 Cont | VASC, URT, MPE, TEN, FDE, Others | Various | CH | IFN-γ | 80.0 | 62.0 | 74.0 | 70.0 |
| Martin 2010 [93] | 19 Pat 10 Cont | URT, MPE, TEN, others | BLs, Ant-Con, RCM, others | CH | IL-2, IL-5, IFN-γ | IL2: 43.0 IL5: 43.0 IFNγ: 57.0 | 100 | IL2: 48.0 IL5: 48.0 IFNγ: 55.0 | 100 |
| Mean Values | 66.6 | 87.5 | 69.5 | 88.5 | |||||
| SD | 23.2 | 18.2 | 19.4 | 18.1 | |||||
Pat: Patients; Cont: Controls; TEN: Toxic epidermal necrolysis; ND: Not determined; URT: Urticaria; ANG: Angioedema; EXANT: Exanthema; MPE: Maculopapular exanthema; BULL-EXANT: Bullous Exanthema; AGEP: Acute generalized exanthematic pustulosis; DILI: Drug induced liver injury; DRESS: Drug rash with eosinophilia and systemic symptoms; SJS: Stevens–Jonhson Syndrome; FDE: Fixed drug eruption; ECZ: Eczema; VASC: Vasculitis; Ant-Con: Anti-convulsant; NSAID: non-steroidal anti-inflammatory drugs; BLs: Betalactams; LA: Local Anesthetics; Ant-hyp: Anti-hyperthensive; Ant-tub: Anti-tuberculosis; Allop: Allopurinol; Diag: diagnostic method; CH: Clinical History; ST: Skin test; DPT: Drug provocation test; DC: Dendritic cells; Sens: Sensitivity; Spec: Specificity; NPV: Negative predictive value; PPV: Positive predictive value.
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mayorga, C.; Doña, I.; Perez-Inestrosa, E.; Fernández, T.D.; Torres, M.J. The Value of In Vitro Tests to Diminish Drug Challenges. Int. J. Mol. Sci. 2017, 18, 1222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061222
AMA Style
Mayorga C, Doña I, Perez-Inestrosa E, Fernández TD, Torres MJ. The Value of In Vitro Tests to Diminish Drug Challenges. International Journal of Molecular Sciences. 2017; 18(6):1222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061222
Chicago/Turabian StyleMayorga, Cristobalina, Inmaculada Doña, Ezequiel Perez-Inestrosa, Tahia D. Fernández, and Maria J. Torres. 2017. "The Value of In Vitro Tests to Diminish Drug Challenges" International Journal of Molecular Sciences 18, no. 6: 1222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms18061222
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.