3D Bioprinted Artificial Trachea with Epithelial Cells and Chondrogenic-Differentiated Bone Marrow-Derived Mesenchymal Stem Cells


Abstract
:1. Introduction
2. Results
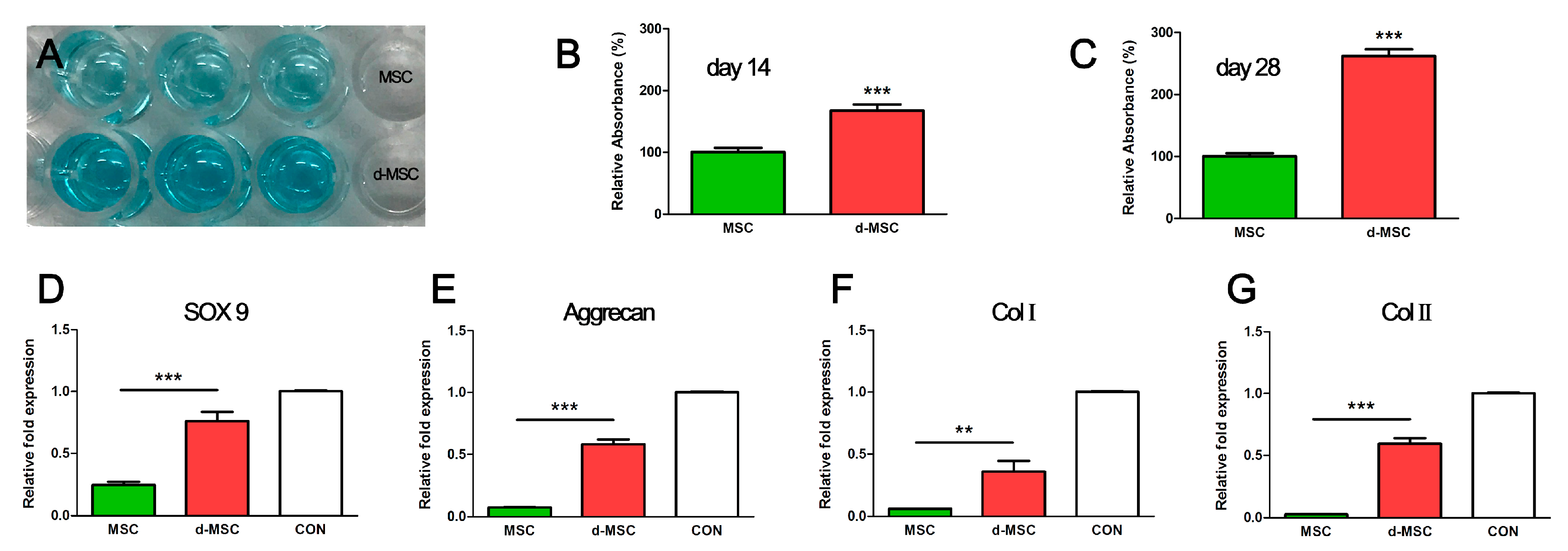
2.1. Relative Quantification of Glycosaminoglycan (GAG) in bMSC and Chondrogenic-Differentiated bMSC
2.2. Chondrogenic Gene Expression
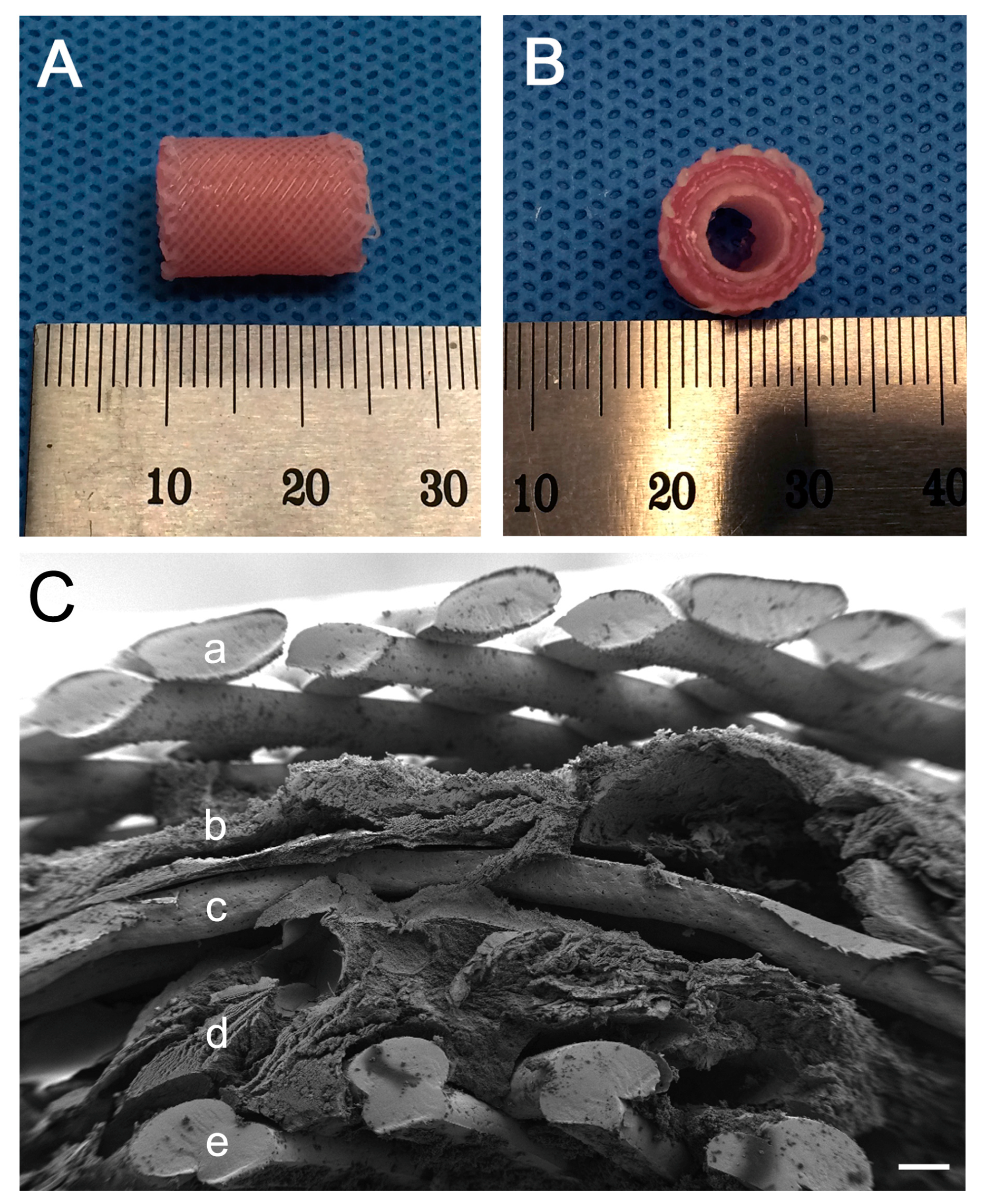
2.3. Structure of the 3D Bioprinted Artificial Trachea
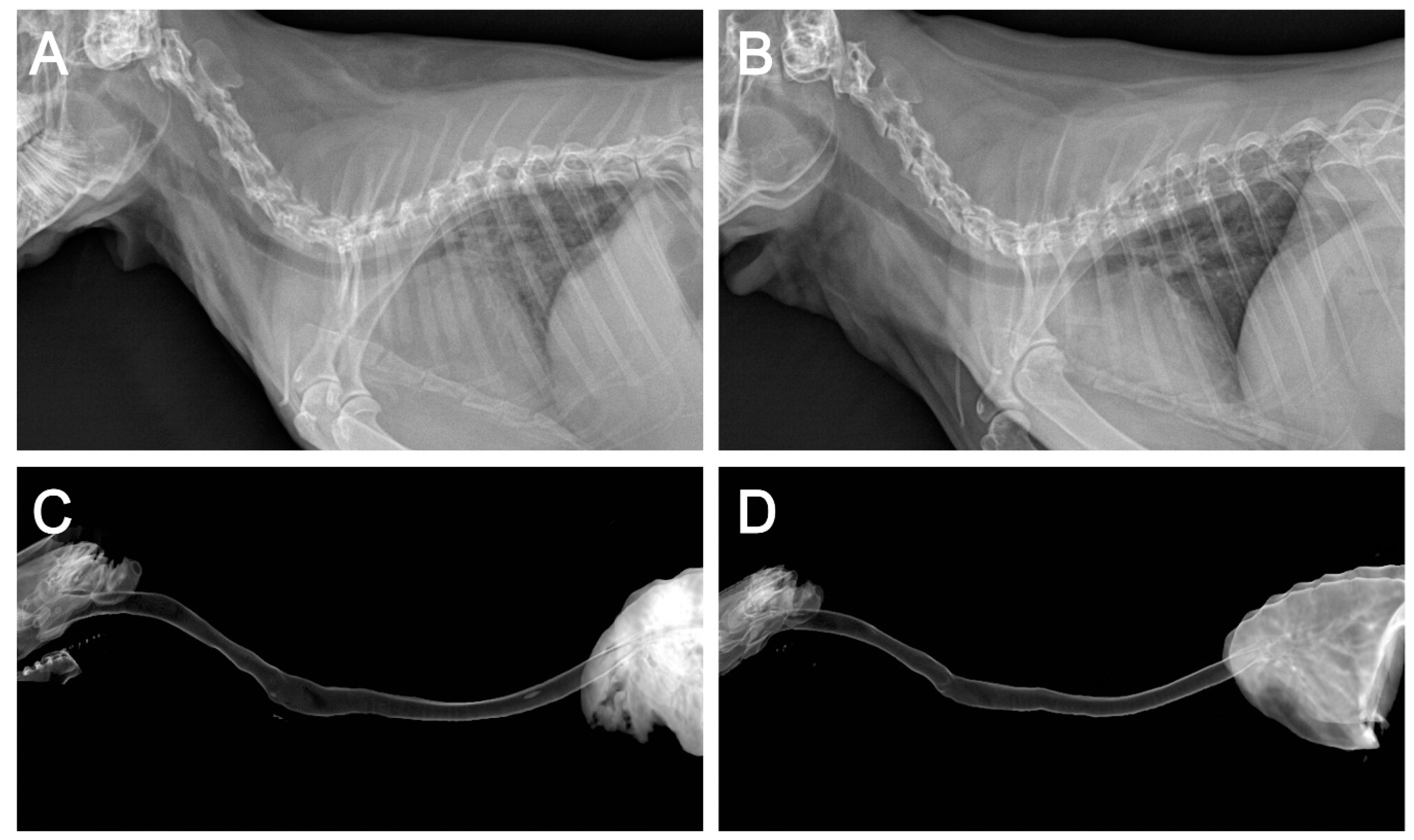
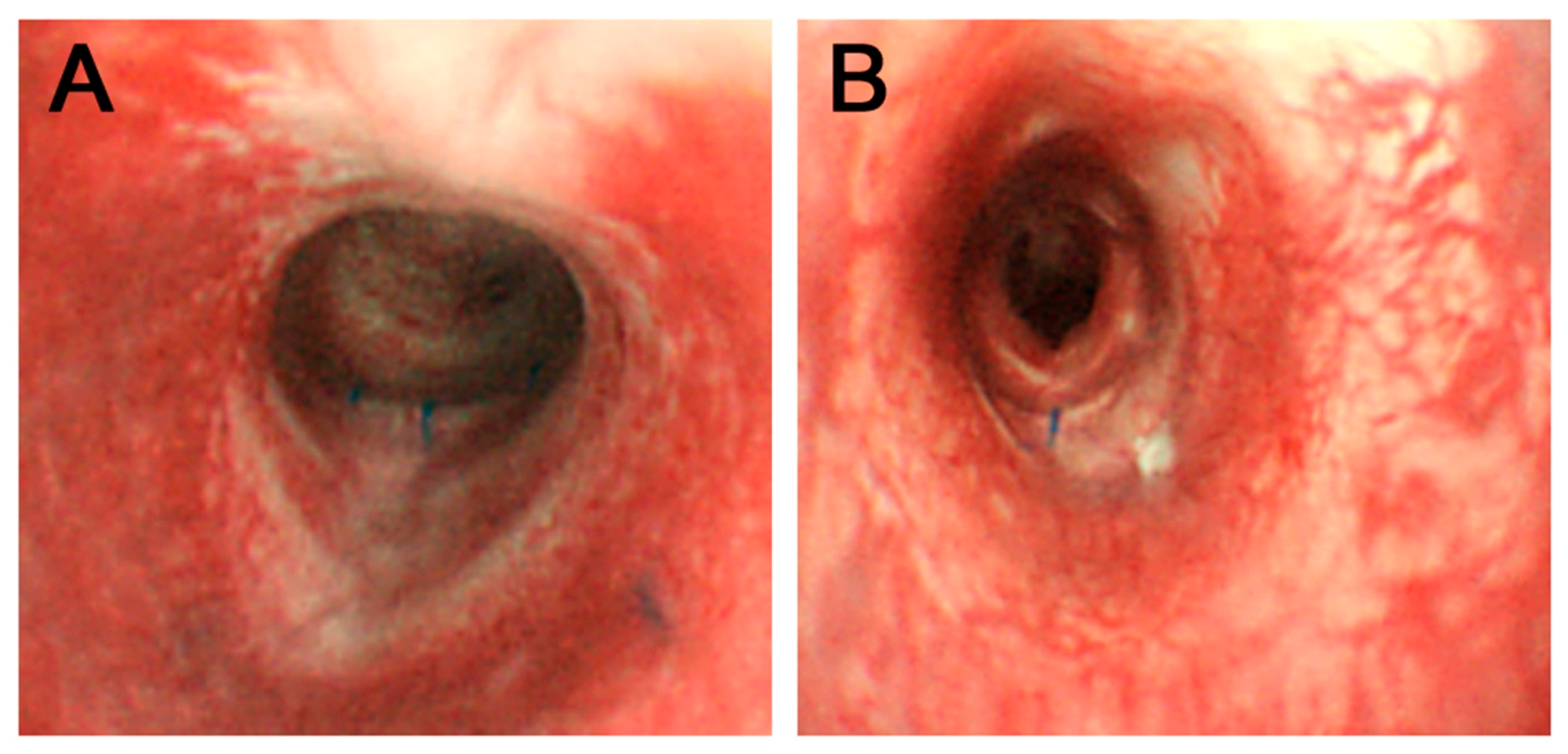
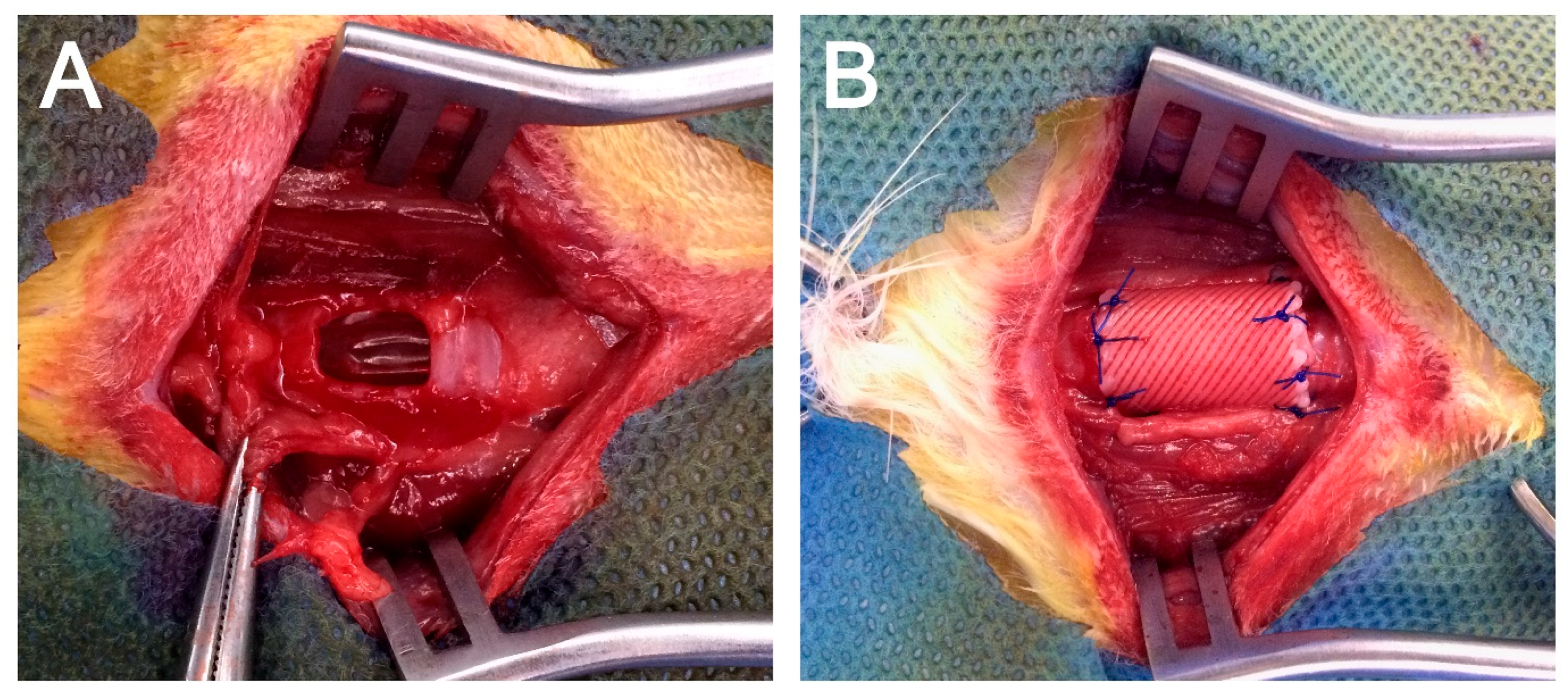
2.4. Application of the 3D Bioprinted Artificial Trachea
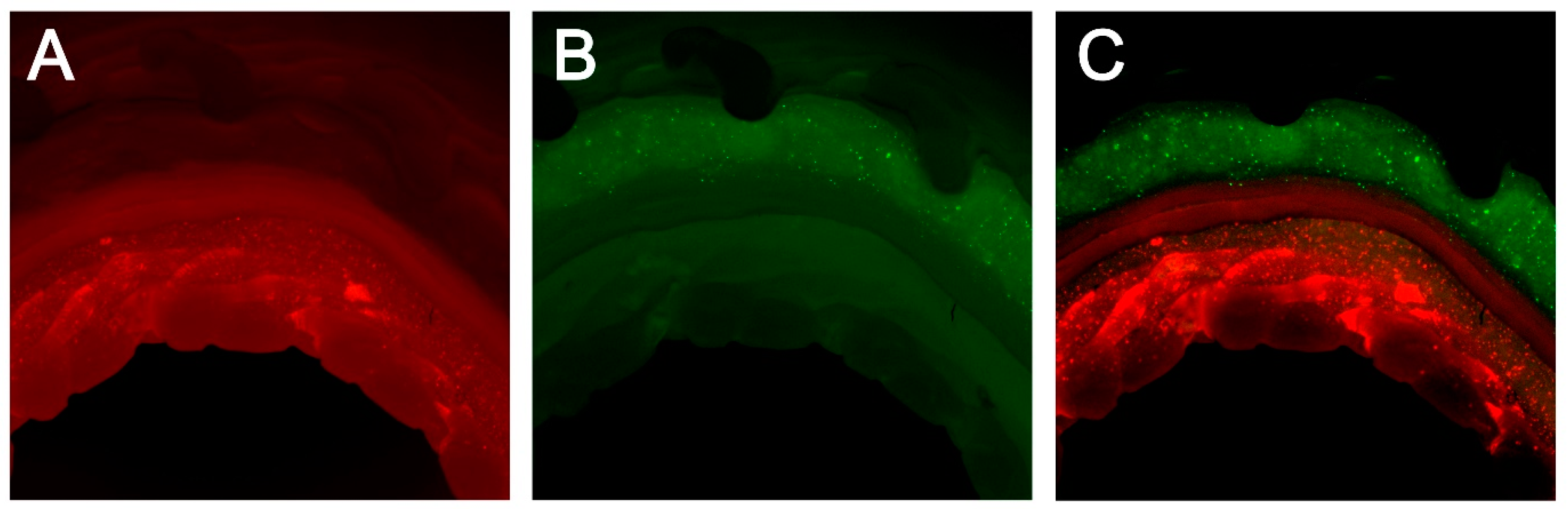
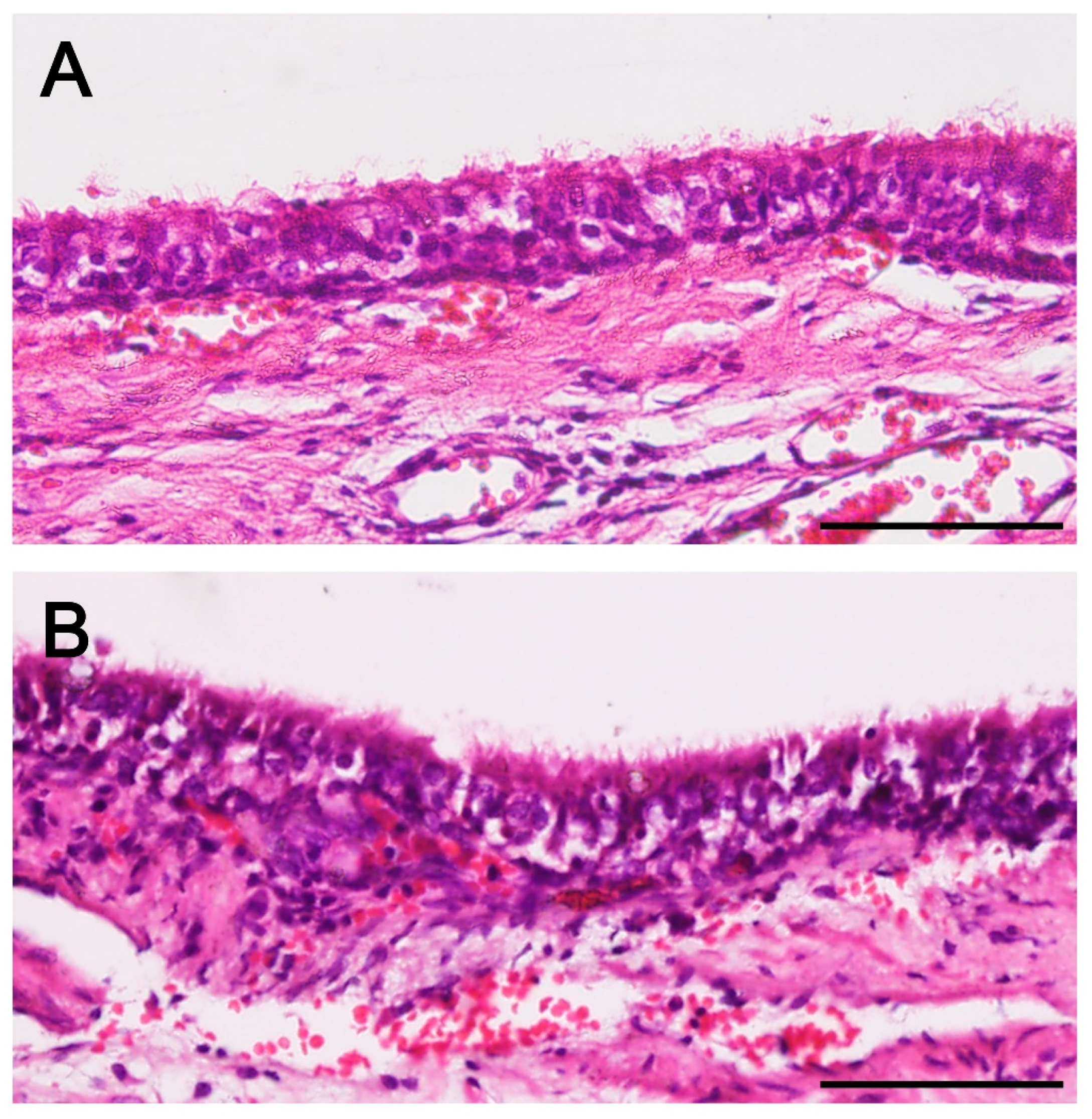
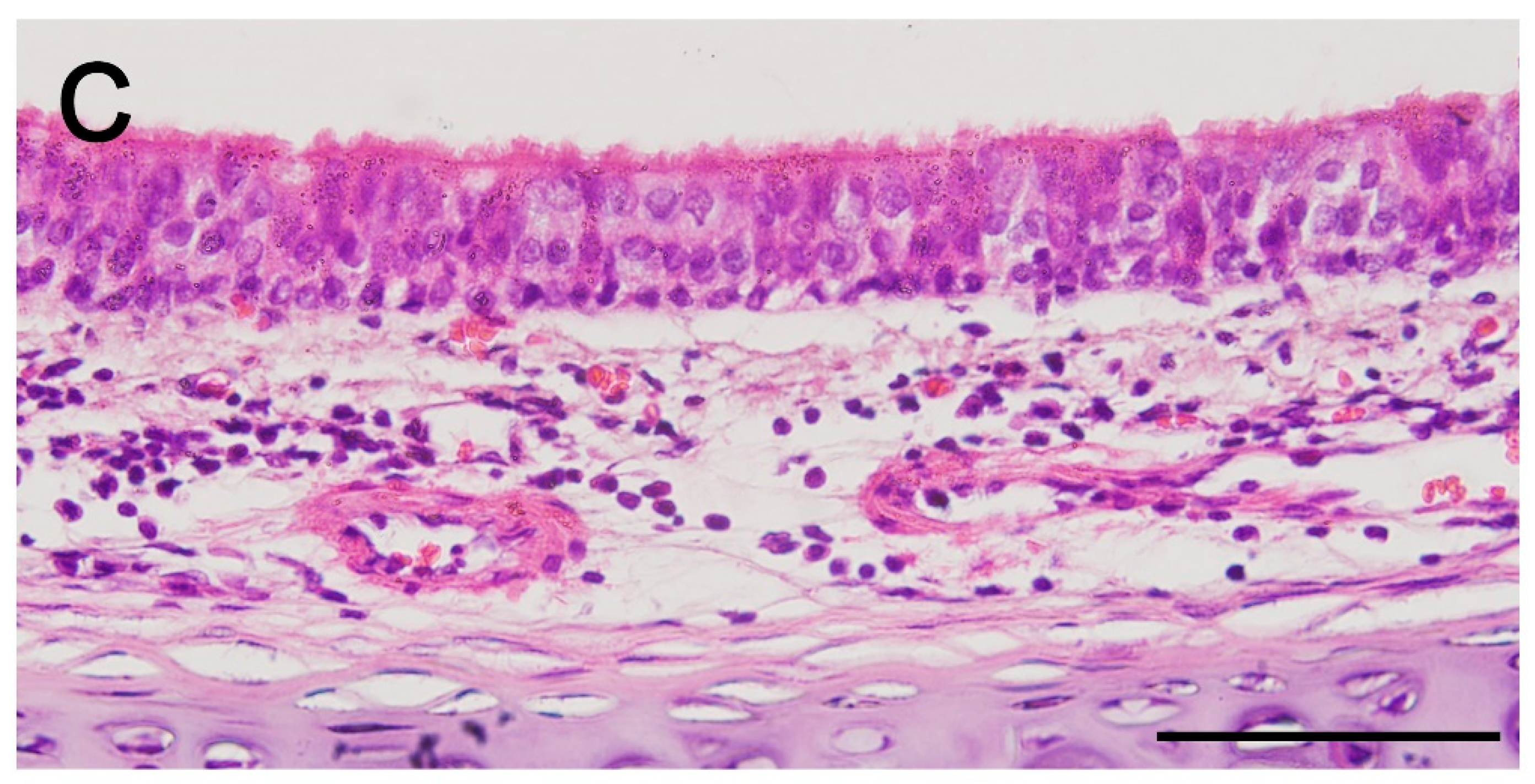
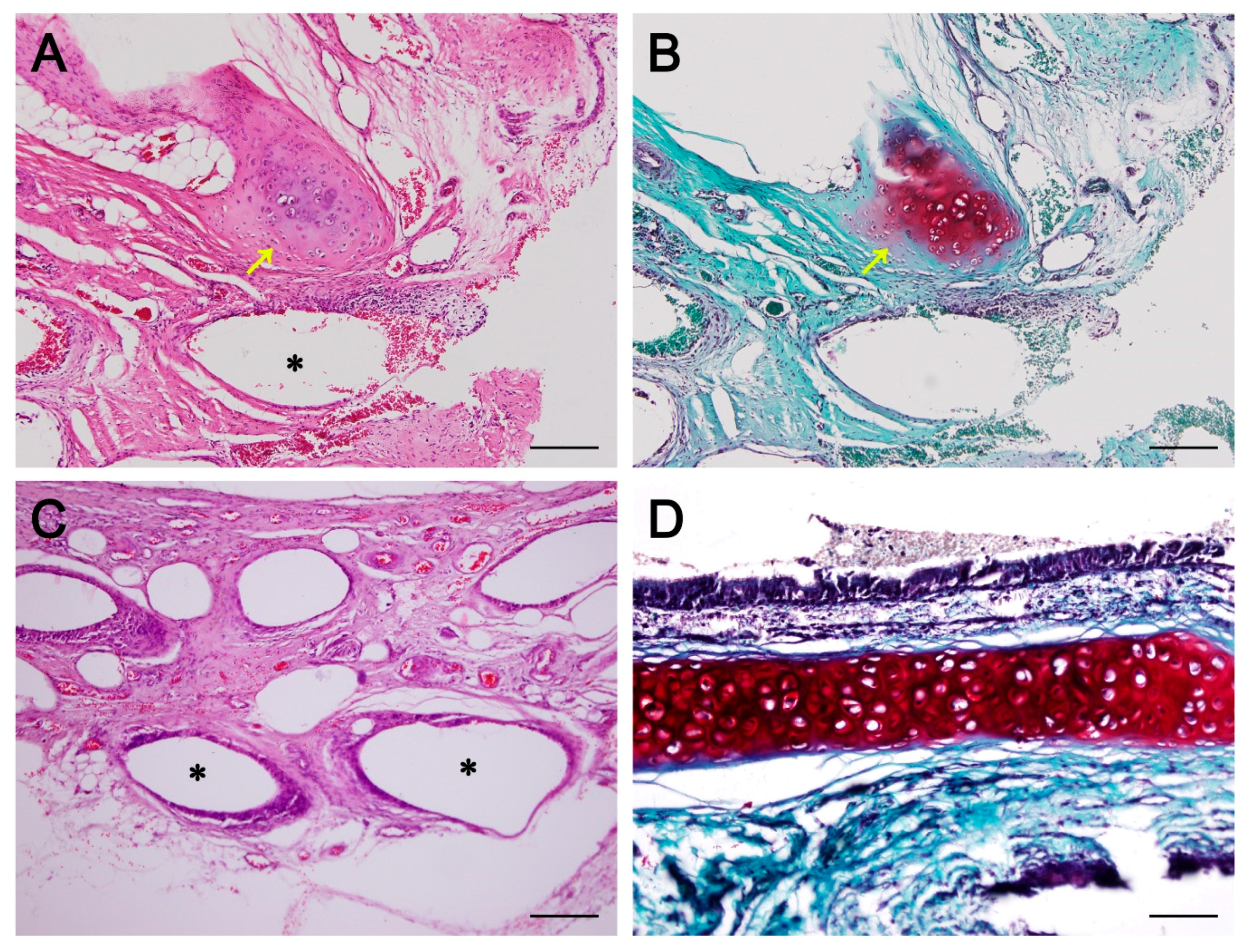
2.5. In Vivo Epithelialization and Neo-Cartilage Formation
3. Discussion
4. Materials and Methods
4.1. Primary Cell Culture
4.1.1. Isolation and Culture of Autologous bMSC
4.1.2. Isolation and Chondrogenic Differentiation of Autologous bMSC (d-MSC)
4.1.3. Isolation and Culture of Autologous Epithelial Cells
4.2. In Vitro Study
4.2.1. Modified Alcian Blue Absorbance Test
4.2.2. RNA Extraction and Quantitative Reverse Transcription Polymerase Chain Reaction (qRT-PCR)
4.3. In Vivo Study
4.3.1. Manufacturing Artificial Trachea Using a 3D Bioprinter
4.3.2. Cell Distribution in the 3D Bioprinted Artificial Trachea
4.3.3. Scanning Electron Microscope (SEM)
4.3.4. Surgical Procedures for Tracheal Replacement Using 3D Bioprinted Artificial Trachea and Post Experimental Observation
4.3.5. Histopathology
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Chang, J.W.; Park, S.A.; Park, J.K.; Choi, J.W.; Kim, Y.S.; Shin, Y.S.; Kim, C.H. Tissue-engineered tracheal reconstruction using three-dimensionally printed artificial tracheal graft: Preliminary report. Artif. Organs 2014, 38, E95–E105. [Google Scholar] [CrossRef] [PubMed]
- Villegas-Álvarez, F.; González-Zamora, J.F.; González-Maciel, A.; Soriano-Rosales, R.; Pérez-Guille, B.; Padilla-Sánchez, L.; Reynoso-Robles, R.; Ramos-Morales, A.; Zenteno-Galindo, E.; Pérez-Torres, A.; et al. Fibrocollagen-covered prosthesis for a noncircumferential segmental tracheal replacement. J. Thorac. Cardiovasc. Surg. 2010, 139, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Doss, A.E.; Dunn, S.S.; Kucera, K.A.; Clemson, L.A.; Zwischenberger, J.B. Tracheal replacements: Part 2. ASAIO J. 2007, 53, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Rose, K.; Sesterhenn, K.; Wustrow, F. Tracheal allotransplantation in man. Lancet 1979, 1, 433. [Google Scholar] [CrossRef]
- Wurtz, A.; Hysi, I.; Kipnis, E.; Zawadzki, C.; Hubert, T.; Jashari, R.; Copin, M.C.; Jude, B. Tracheal reconstruction with a composite graft: Fascial flap-wrapped allogenic aorta with external cartilage-ring support. Interact. Cardiovasc. Thorac. Surg. 2013, 16, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Jungebluth, P.; Moll, G.; Baiguera, S.; Macchiarini, P. Tissue-engineered airway: A regenerative solution. Clin. Pharmacol. Ther. 2012, 91, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, N.; Bullock, A.J.; Macneil, S.; Janes, S.M.; Birchall, M. Tissue engineering airway mucosa: A systematic review. Laryngoscope 2014, 124, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Vacanti, C.A.; Paige, K.T.; Kim, W.S.; Sakata, J.; Upton, J.; Vacanti, J.P. Experimental tracheal replacement using tissue-engineered cartilage. J. Pediatr. Surg. 1994, 29, 201–205. [Google Scholar] [CrossRef]
- Sakata, J.; Vacanti, C.; Schloo, B.; Healy, G.; Langer, R.; Vacanti, J. Tracheal composites tissue engineered from chondrocytes, tracheal epithelial cells and synthetic degradable scaffolding. Transplant. Proc. 1994, 26, 3309–3310. [Google Scholar] [PubMed]
- Zein, I.; Hutmacher, W.; Tan, K.; Teoh, S. Fused Deposition Modeling of Novel Scaffold Architectures for Tissue Engineering Applications. Biomaterials 2002, 23, 1169–1185. [Google Scholar] [CrossRef]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Ciuffreda, M.C.; Malpasso, G.; Musarò, P.; Turco, V.; Gnecchi, M. Protocols for in vitro differentiation of human mesenchymal stem cells into osteogenic, chondrogenic and adipogenic lineages. Mesenchymal Stem Cells: Methods and Protoc. 2016, 1416, 149–158. [Google Scholar] [CrossRef]
- Tanthaisong, P.; Imsoonthornruksa, S.; Ngernsoungnern, A.; Ngernsoungnern, P.; Ketudat-Cairns, M.; Parnpai, R. Enhanced chondrogenic differentiation of human umbilical cord wharton’s jelly derived mesenchymal stem cells by GSK-3 Inhibitors. PLoS ONE 2017, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, V.; Behringer, R.R.; De Crombrugghe, B. L-Sox5, Sox6 and SOx9 control essential steps of the chondrocyte differentiation pathway. Osteoarthr. Cartil. 2001, 9, 69–75. [Google Scholar] [CrossRef]
- Wei, B.; Jin, C.; Xu, Y.; Du, X.; Yan, C.; Tang, C.; Ansari, M.; Wang, L. Chondrogenic Differentiation of Marrow Clots after Microfracture with BMSC-Derived ECM Scaffold in Vitro. Tissue Eng. Part A 2014, 20, 2646–2655. [Google Scholar] [CrossRef] [PubMed]
- Barry, F.; Boynton, R.E.; Liu, B.; Murphy, J.M. Chondrogenic differentiation of mesenchymal stem cells from bone marrow: Differentiation-dependent gene expression of matrix components. Exp. Cell Res. 2001, 268, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Kojima, K.; Ignotz, R.A.; Kushibiki, T.; Tinsley, K.W.; Tabata, Y.; Vacanti, C.A. Tissue-engineered trachea from sheep marrow stromal cells with transforming growth factor β2 released from biodegradable microspheres in a nude rat recipient. J. Thorac. Cardiovasc. Surg. 2004, 128, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Behrend, M.; Kluge, E. The fate of homograft tracheal transplants in sheep. World J. Surg. 2008, 32, 1669–1675. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Pyun, J.H.; Choi, J.W.; Kim, J.H.; Lee, J.S.; Shin, H.A.; Kim, H.J.; Lee, H.N.; Min, B.H.; Cha, H.E.; et al. Tissue-engineered allograft tracheal cartilage using fibrin/hyaluronan composite gel and its in vivo implantation. Laryngoscope 2010, 120, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Ott, L.M.; Weatherly, R.A.; Detamore, M.S. Overview of tracheal tissue engineering: Clinical need drives the laboratory approach. Ann. Biomed. Eng. 2011, 39, 2091–2113. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Lan, N.; Pang, C.; Tong, X. Bone marrow-derived mesenchymal stem cells enhance cryopreserved trachea allograft epithelium regeneration and vascular endothelial growth factor expression. Transplantation 2011, 92, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Patrício, T.; Domingos, M.; Gloria, A.; D’Amora, U.; Coelho, J.F.; Bártolo, P.J. Fabrication and characterisation of PCL and PCL/PLA scaffolds for tissue engineering. Rapid Prototyp. J. 2014, 20, 145–156. [Google Scholar] [CrossRef]
- Domingos, M.; Gloria, A.; Coelho, J.; Bartolo, P.; Ciurana, J. Three-dimensional printed bone scaffolds: The role of nano/micro-hydroxyapatite particles on the adhesion and differentiation of human mesenchymal stem cells. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Zopf, D.; Hollister, S.; Nelson, M.; Ohye, R.; Green, G. Bioresorbable airway splint created with a three-dimensional printer. N. Engl. J. Med. 2013, 368, 2043–2045. [Google Scholar] [CrossRef] [PubMed]
- Son, S.R.; Linh, N.T.B.; Yang, H.M.; Lee, B.T. In vitro and in vivo evaluation of electrospun PCL/PMMA fibrous scaffolds for bone regeneration. Sci. Technol. Adv. Mater. 2013, 14. [Google Scholar] [CrossRef] [PubMed]
- Costantini, M.; Idaszek, J.; Szöke, K.; Jaroszewicz, J.; Dentini, M.; Barbetta, A.; Brinchmann, J.E.; Święszkowski, W. 3D bioprinting of BM-MSCs-loaded ECM biomimetic hydrogels for in vitro neocartilage formation. Biofabrication 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Go, T.; Jungebluth, P.; Baiguero, S.; Asnaghi, A.; Martorell, J.; Ostertag, H.; Mantero, S.; Birchall, M.; Bader, A.; Macchiarini, P. Both epithelial cells and mesenchymal stem cell-derived chondrocytes contribute to the survival of tissue-engineered airway transplants in pigs. J. Thorac. Cardiovasc. Surg. 2010, 139, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhang, X.; Gao, G.; Yonezawa, T.; Cui, X. 3D bioprinting and the current applications in tissue engineering. Biotechnol. J. 2017. [Google Scholar] [CrossRef] [PubMed]
- Fishman, J.M.; Lowdell, M.; Birchall, M.A. Stem cell-based organ replacements-Airway and lung tissue engineering. Semin. Pediatr. Surg. 2014, 23, 119–126. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Primer Nucleotide Sequence |
|---|---|
| ACAN | Forward: 5-TCGAGGACAGCGAGGCC-3 Reverse: 3-AGAGATGTGCGATGTGGGAGCT-5 |
| Col1α1 | Forward: 5-GCGGTGGTTACGACTTTGGTT-3 Reverse: 3-AGTGAGGAGGGTCTCAATCTG-5 |
| Col2α1 | Forward : 5-GGCAATAGCAGGTTCACGTACA-3 Reverse: 3-TTCACCCCGTTCTGACAATAGC-5 |
| SOX9 | Forward: 5-CACACAGCTCACTCGACCTTG-3 Reverse: 3-GCTCTACTAGGATTTTATTGGCTT-5 |
| GAPDH | Forward: 5-ATGGGGAAGGTGAAGGTCG-3 Reverse: 3-CCAGTGGTCCCGACGAAAAT-5 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, S.-W.; Lee, K.-W.; Park, J.-H.; Lee, J.; Jung, C.-R.; Yu, J.; Kim, H.-Y.; Kim, D.-H. 3D Bioprinted Artificial Trachea with Epithelial Cells and Chondrogenic-Differentiated Bone Marrow-Derived Mesenchymal Stem Cells. Int. J. Mol. Sci. 2018, 19, 1624. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19061624
Bae S-W, Lee K-W, Park J-H, Lee J, Jung C-R, Yu J, Kim H-Y, Kim D-H. 3D Bioprinted Artificial Trachea with Epithelial Cells and Chondrogenic-Differentiated Bone Marrow-Derived Mesenchymal Stem Cells. International Journal of Molecular Sciences. 2018; 19(6):1624. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19061624
Chicago/Turabian StyleBae, Sang-Woo, Kang-Woog Lee, Jae-Hyun Park, JunHee Lee, Cho-Rok Jung, JunJie Yu, Hwi-Yool Kim, and Dae-Hyun Kim. 2018. "3D Bioprinted Artificial Trachea with Epithelial Cells and Chondrogenic-Differentiated Bone Marrow-Derived Mesenchymal Stem Cells" International Journal of Molecular Sciences 19, no. 6: 1624. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19061624