Antihistamines for Allergic Rhinitis Treatment from the Viewpoint of Nonsedative Properties


Abstract
:1. Introduction
2. Pharmacological Aspects Related to Sedation of Antihistamines
2.1. Histamine and Its Receptors
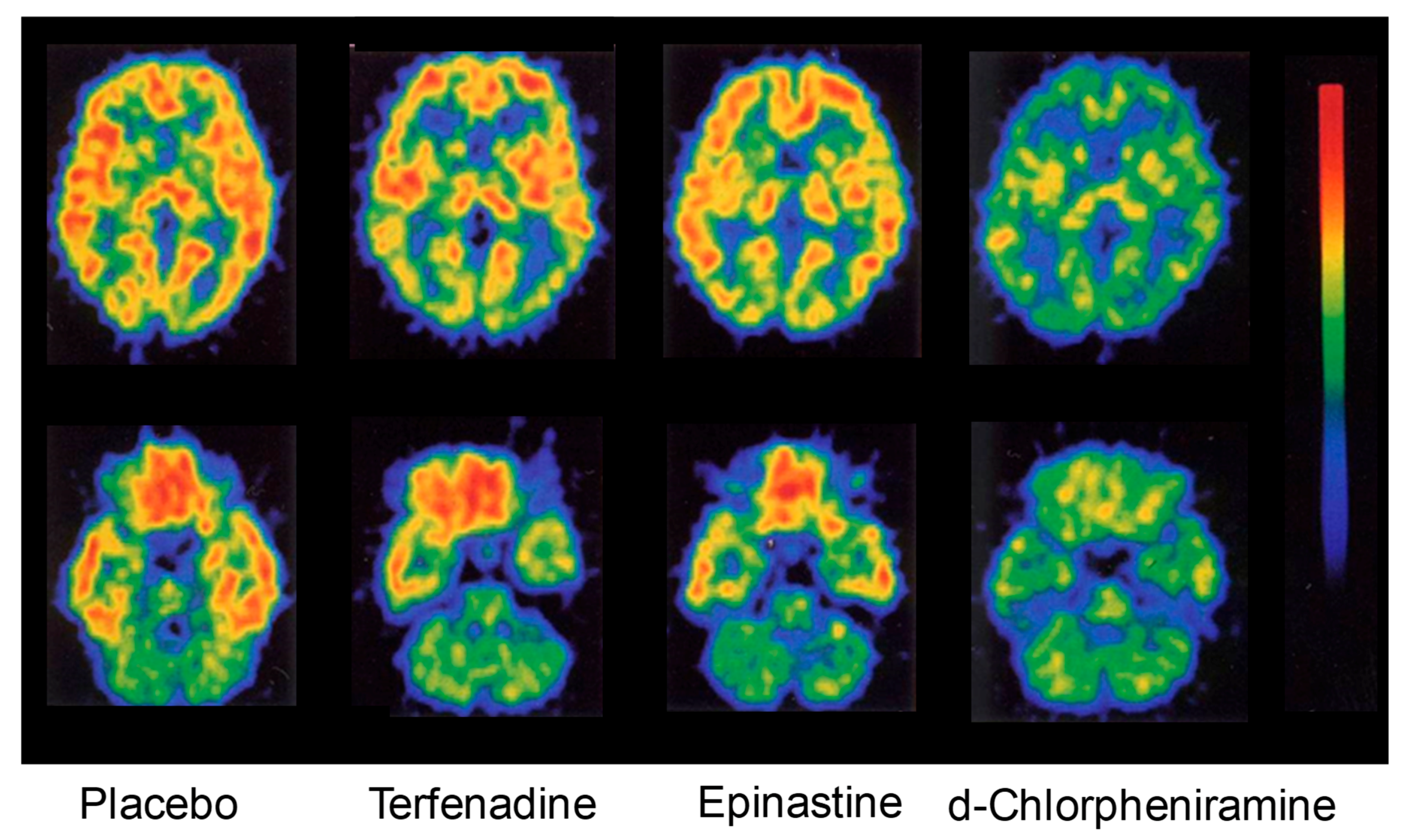
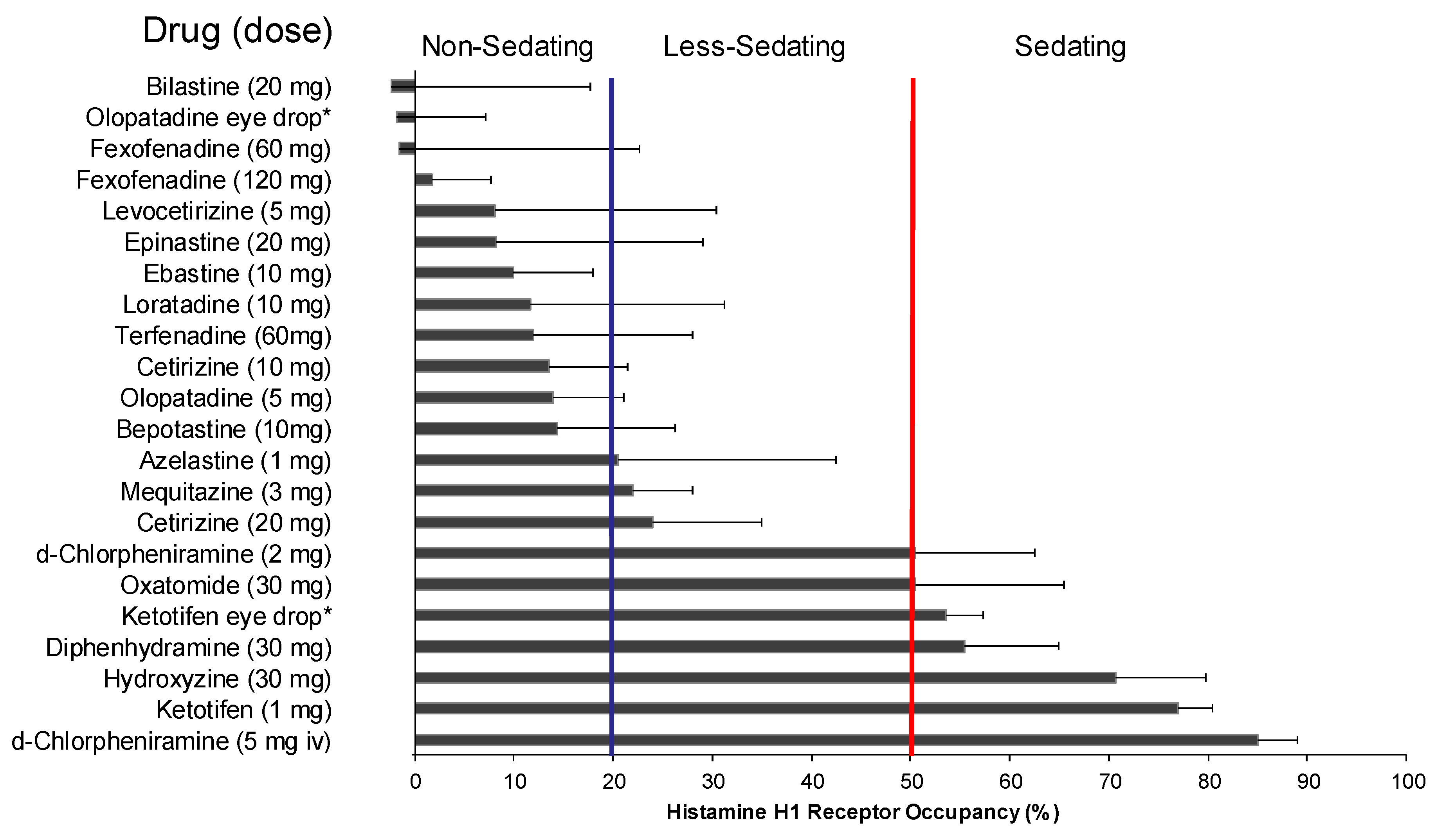
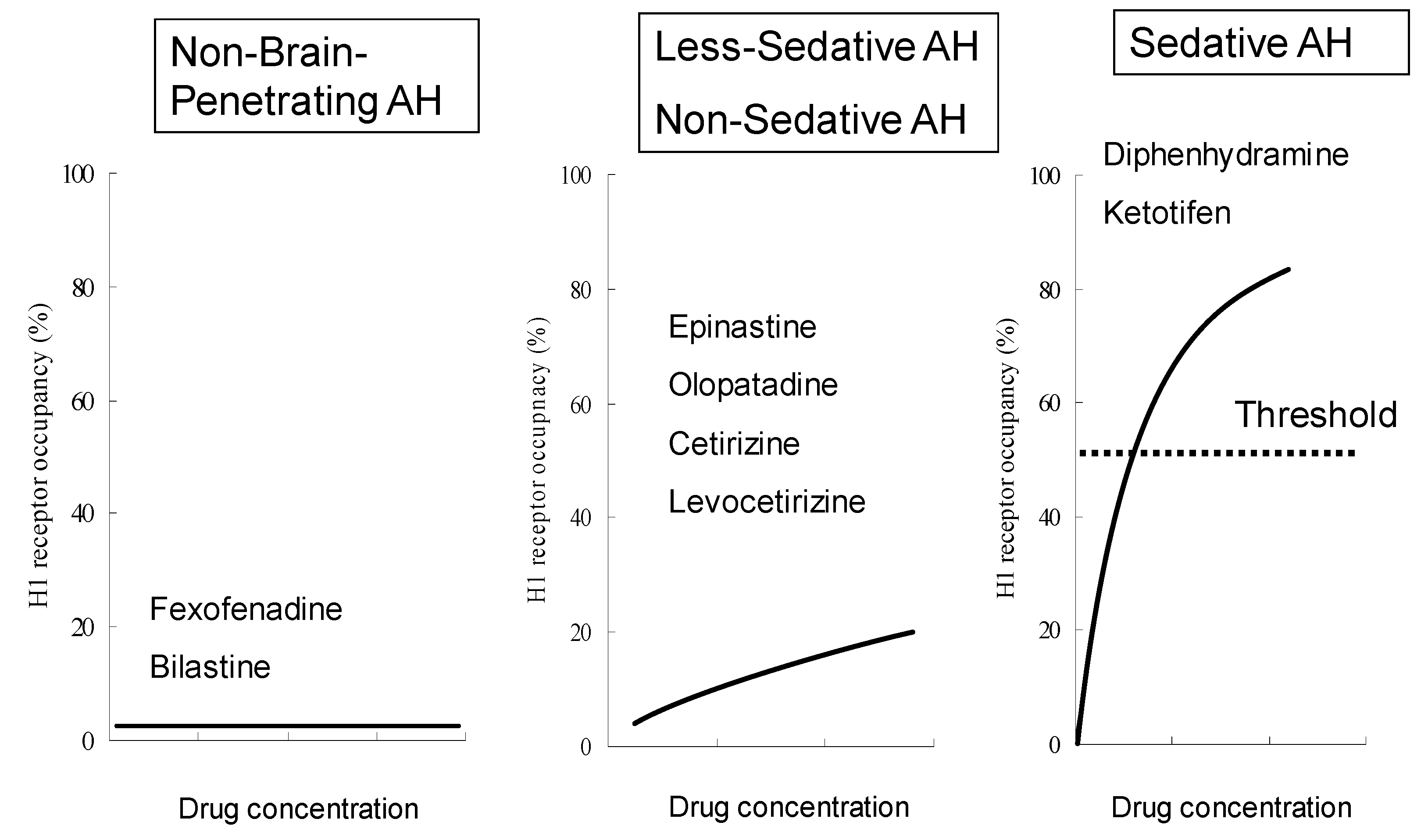
2.2. Sedative Potentials of Antihistamines and Their Classification Based on Brain H1 Receptor Occupancy
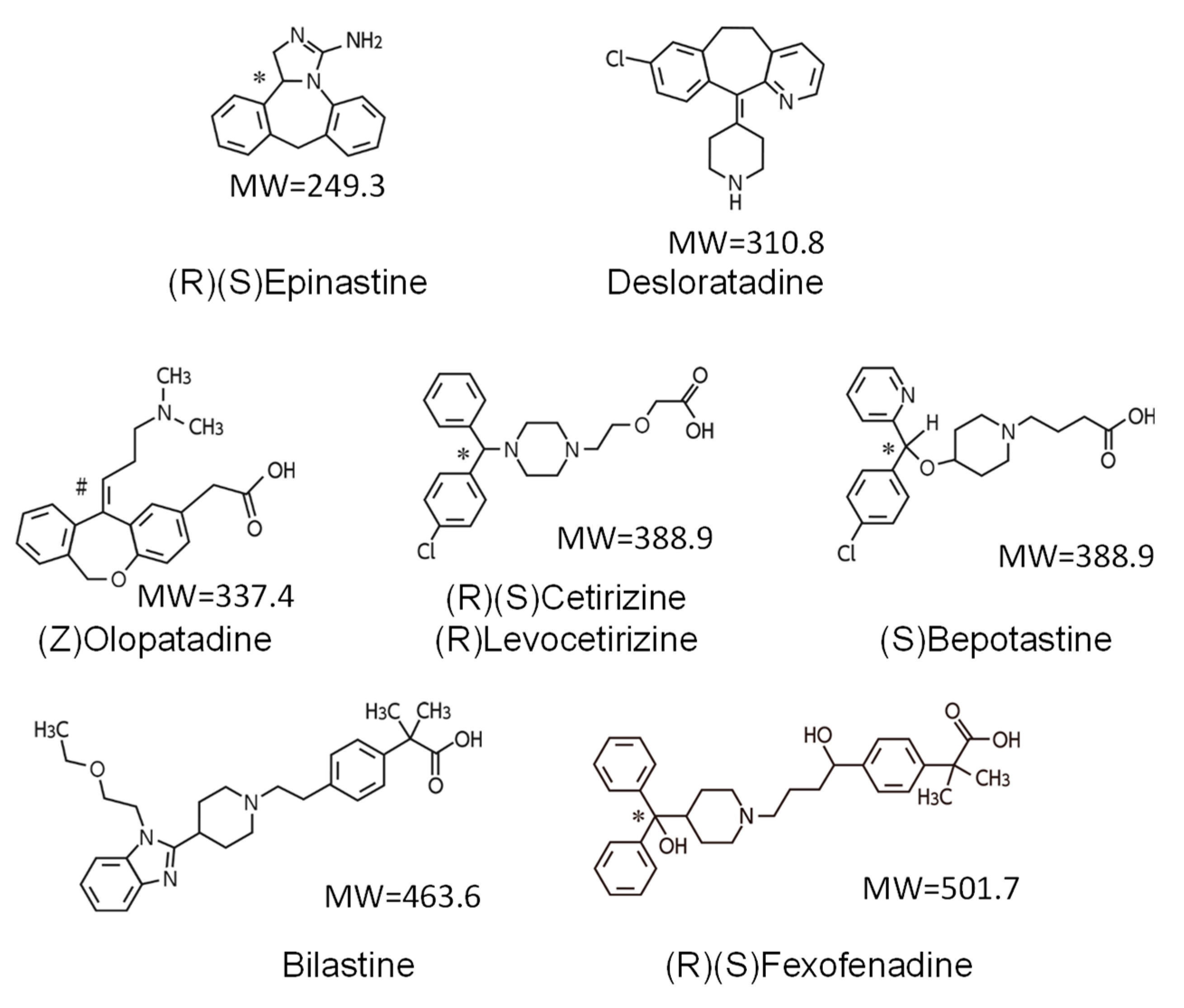
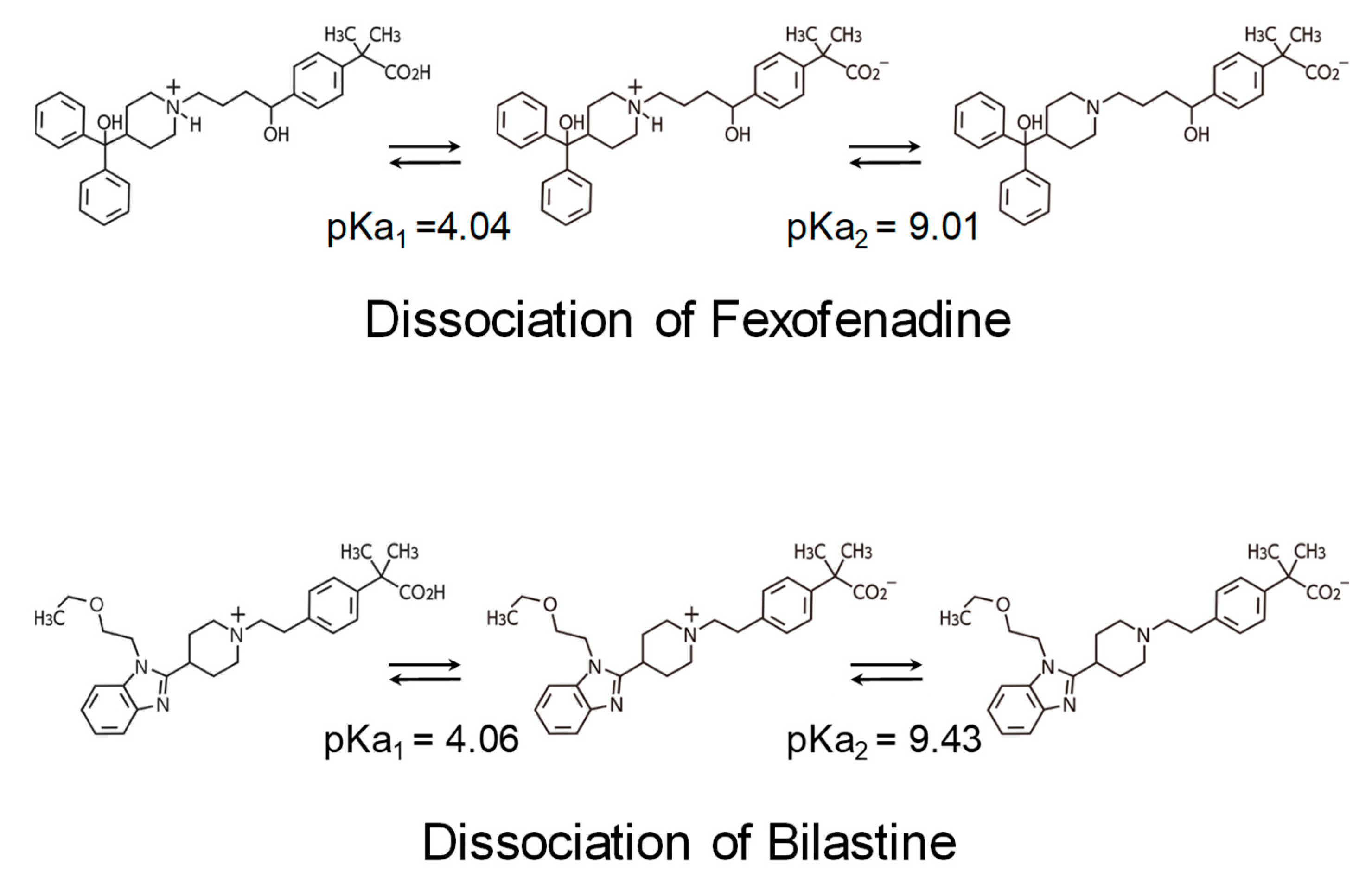
2.3. Non-Brain-Penetrating Antihistamines: Bilastine and Fexofenadine
2.4. Residual Effects by Sedating Antihistamines
3. Clinical Aspects of Non-Sedating Antihistamines
3.1. Clinical Profiles of Representative Second-Generation Antihistamines
3.2. Efficacy for Seasonal Allergic Rhinitis
3.3. Central Nervous System Safety of Bilastine
4. Conclusions
5. Expert Opinion
Article Highlights Box
- In selecting antihistamines for allergic rhinitis, it is particularly important for safety that the selected drug does not have central depressant/sedative properties and anticholinergic effects.
- Differences in sedative effects and anticholinergic effects were observed among the second-generation antihistamines.
- Based on the brain H1 receptor occupancy, which is an index of sedative properties, fexofenadine and bilastine belonging to the non-sedating group can be distinguished as “non-brain-penetrating antihistamines”.
- No major differences in efficacy are observed among recent, representative, non-sedating antihistamines for allergic rhinitis.
- Central nervous system safety of antihistamines needs to be evaluated not only by subjective indices, such as drowsiness, but also by the results of objective performance tests.
- Non-brain-penetrating antihistamines have been confirmed not to show sedative properties even at twice the usual dose and thus are considered to be the first-line antihistamines for allergic rhinitis.
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| H1RO | Brain H1 receptor occupancy |
| GPCR | G-protein-coupled receptors |
| PIR | proportional impairment ratio |
| CONGA | Consensus Group of New Generation of Antihistamines |
| BBB | blood–brain barrier |
| pKa | Acid–Base Dissociation Constant |
| Tmax | time to maximum plasma concentration |
| t½ | elimination half-life |
| ARIA | Allergic Rhinitis and its Impact on Asthma |
| SAR | seasonal allergic rhinitis |
| TSS | total symptom score |
| NSS | nasal symptom score |
| NNSS | non-nasal symptom score |
| PAR | perennial allergic rhinitis |
| FMT | Fine Motoric Test |
| CFF | Critical Flicker-Fusion Frequency Test |
| D2T | “d2” Cancellation Test |
| SRT | Simple Reaction Time |
| SDLP | standard deviations of lateral position |
References
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; van Weel, C.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008. Allergy 2008, 63 (Suppl. 86), 8–160. [Google Scholar]
- Okubo, K.; Kurono, Y.; Ichimura, K.; Enomoto, T.; Okamoto, Y.; Kawauchi, H.; Suzaki, H.; Fujieda, S.; Masuyama, K. Japanese guidelines for allergic rhinitis 2017. Allergol. Int. 2017, 66, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Kay, A.B. Allergy and allergic diseases. First of two parts. N. Engl. J. Med. 2001, 344, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Clement, P.; Smitz, J.; De Waele, M.; Derde, M.P. Correlations between complaints, inflammatory cells and mediator concentrations in nasalsecretions after nasal allergen challenge and during natural allergen exposure. Int. Arch. Allergy Immunol. 1995, 106, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Mandhane, S.N.; Shah, J.H.; Thennati, R. Allergic rhinitis: An update on disease, present treatments and future prospects. Int. Immunopharmacol. 2011, 11, 1646–1662. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.Y.; Ghoshal, A.G.; Bin Abdul Muttalif, A.R.; Lin, H.C.; Thanaviratananich, S.; Bagga, S.; Faruqi, R.; Sajjan, S.; Brnabic, A.J.; Dehle, F.C.; et al. Quality of life and economic burden of respiratory disease in Asia-Pacific—Asia-Pacific Burden of Respiratory Diseases Study. Value Health Reg. Issues 2016, 9, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Lim-Jurado, M.; Prepageran, N.; Tantilipikorn, P.; Wang de, Y. Treatment of allergic rhinitis and urticaria: A review of the newest antihistamine drug bilastine. Ther. Clin. Risk Manag. 2016, 12, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Yanai, K.; Yoshikawa, T.; Yanai, A.; Nakamura, T.; Iida, T.; Leurs, R.; Tashiro, M. The clinical pharmacology of non-sedating antihistamines. Pharmacol. Ther. 2017, 178, 148–156. [Google Scholar] [CrossRef]
- Yanai, K.; Zhang, D.; Tashiro, M.; Yoshikawa, T.; Naganuma, F.; Harada, R.; Nakamura, T.; Shibuya, K.; Okamura, N. Positron emission tomography evaluation of sedative properties of antihistamines. Expert Opin. Drug Saf. 2011, 10, 613–622. [Google Scholar] [CrossRef]
- Panula, P.; Chazot, P.L.; Cowart, M.; Gutzmer, R.; Leurs, R.; Liu, W.L.; Stark, H.; Thurmond, R.L.; Haas, H.L. International Union of Basic and Clinical Pharmacology. XCVIII. Histamine receptors. Pharmacol. Rev. 2015, 67, 601–655. [Google Scholar] [CrossRef]
- Leurs, R.; Church, M.K.; Taglialatela, M. H1-antihistamines: Inverse agonism, anti-inflammatory actions and cardiac effects. Clin. Exp. Allergy 2002, 32, 489–498. [Google Scholar] [CrossRef]
- Church, D.S.; Church, M.K. Pharmacology of antihistamines. World Allergy Organ. J. 2011, 4 (Suppl. 3), S22–S27. [Google Scholar] [CrossRef]
- Shimamura, T.; Shiroishi, M.; Weyand, S.; Tsujimoto, H.; Winter, G.; Katritch, V.; Abagyan, R.; Cherezov, V.; Liu, W.; Han, G.W.; et al. Structure of the human histamine H1 receptor complex with doxepin. Nature 2011, 475, 65–70. [Google Scholar] [CrossRef]
- Haas, H.; Panula, P. The role of histamine and the tuberomamillary nucleus in the nervous system. Nat. Rev. Neurosci. 2003, 4, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Haas, H.; Sergeeva, O.A.; Selbach, O. Histamine in the nervous system. Physiol. Rev. 2008, 88, 1183–1241. [Google Scholar] [CrossRef] [PubMed]
- Shan, L.; Dauvilliers, Y.; Siegel, J.M. Interactions of the histamine and hypocretin systems in CNS disorders. Nat. Rev. Neurol. 2015, 11, 401–413. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Yanai, K. Studies on functional roles of the histaminergic neuron system by using pharmacological agents, knockout mice and positron emission tomography. Tohoku J. Exp. Med. 2001, 195, 197–217. [Google Scholar] [CrossRef]
- Yanai, K.; Ryu, J.H.; Watanabe, T.; Iwata, R.; Ido, T.; Sawai, Y.; Ito, K.; Itoh, M. Histamine H1 receptor occupancy in human brains after single oral doses of histamine H1 antagonists measured by positron emission tomography. Br. J. Pharmacol. 1995, 116, 1649–1655. [Google Scholar] [CrossRef]
- Okamura, N.; Yanai, K.; Higuchi, M.; Sakai, J.; Iwata, R.; Ido, T.; Sasaki, H.; Watanabe, T.; Itoh, M. Functional neuroimaging of cognition impaired by a classical antihistamine, d-chlorpheniramine. Br. J. Pharmacol. 2000, 129, 115–123. [Google Scholar] [CrossRef]
- Tagawa, M.; Kano, M.; Okamura, N.; Higuchi, M.; Matsuda, M.; Mizuki, Y.; Arai, H.; Iwata, R.; Fujii, T.; Komemushi, S.; et al. Neuroimaging of histamine H1-receptor occupancy in human brain by positron emission tomography (PET): A comparative study of ebastine, a second-generation antihistamine and (+)-chlorpheniramine, a classical antihistamine. Br. J. Clin. Pharmacol. 2001, 52, 501–509. [Google Scholar] [CrossRef]
- Tashiro, M.; Sakurada, Y.; Iwabuchi, K.; Mochizuki, H.; Kato, M.; Aoki, M.; Funaki, Y.; Itoh, M.; Iwata, R.; Wong, D.F.; et al. Central effects of fexofenadine and cetirizine: Measurement of psychomotor performance, subjective sleepiness, and brain histamine H1-receptor occupancy using 11C-doxepin positron emission tomography. J. Clin. Pharmacol. 2004, 44, 890–900. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, K.; Tashiro, M.; Grobosch, T.; Maurer, M.; Oda, K.; Toyohara, J.; Ishii, K.; Ishiwata, K.; Yanai, K. Brain histamine H1 receptor occupancy measured by PET after oral administration of levocetirizine, a non-sedating antihistamine. Expert Opin. Drug Saf. 2015, 14, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Yanai, K.; Watanabe, T.; Yokoyama, H.; Hatazawa, J.; Iwata, R.; Ishiwata, K.; Meguro, K.; Itoh, M.; Takahashi, T.; Ido, T.; et al. Mapping of histamine H1 receptors in the human brain using [11C]pyrilamine and positron emission tomography. J. Neurochem. 1992, 59, 128–136. [Google Scholar] [CrossRef]
- Yanai, K.; Watanabe, T.; Yokoyama, H.; Meguro, K.; Hatazawa, J.; Itoh, M.; Iwata, R.; Ishiwata, K.; Takahashi, T.; Ido, T. Histamine H1 receptors in human brain visualized in vivo by [11C]doxepin and positron emission tomography. Neurosci. Lett. 1992, 137, 145–148. [Google Scholar] [CrossRef]
- Yanai, K.; Watanabe, T.; Meguro, K.; Yokoyama, H.; Sato, I.; Sasano, H.; Itoh, M.; Iwata, R.; Takahashi, T.; Ido, T. Age-dependent decrease in histamine H1 receptor in human brains revealed by PET. Neuroreport 1992, 3, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, M.; Horikawa, E.; Mochizuki, H.; Sakurada, Y.; Kato, M.; Inokuchi, T.; Ridout, F.; Hindmarch, I.; Yanai, K. Effects of fexofenadine and hydroxyzine on brake reaction time during car-driving with cellular phone use. Hum. Psychopharmacol. 2005, 20, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Shamsi, Z.; Hindmarch, I. Sedation and antihistamines: A review of inter-drug differences using proportional impairment ratios. Hum. Psychopharmacol. 2000, 15, S3–S30. [Google Scholar] [CrossRef]
- McDonald, K.; Trick, L.; Boyle, J. Sedation and antihistamines: An update. Review of inter-drug differences using proportional impairment ratios. Hum. Psychopharmacol. 2008, 23, 555–570. [Google Scholar] [CrossRef] [PubMed]
- Yanai, K.; Tashiro, M. The physiological and pathophysiological roles of neuronal histamine: An insight from human positron emission tomography studies. Pharmacol. Ther. 2007, 113, 1–15. [Google Scholar] [CrossRef]
- Holgate, S.T.; Canonica, G.W.; Simons, F.E.; Taglialatela, M.; Tharp, M.; Timmerman, H.; Yanai, K. Consensus Group on New-Generation Antihistamines (CONGA): Present status and recommendations. Clin. Exp. Allergy 2003, 33, 1305–1324. [Google Scholar] [CrossRef]
- Farré, M.; Pérez-Mañá, C.; Papaseit, E.; Menoyo, E.; Pérez, M.; Martin, S.; Bullich, S.; Rojas, S.; Herance, J.R.; Trampal, C.; et al. Bilastine vs. hydroxyzine: Occupation of brain histamine H1 -receptors evaluated by positron emission tomography in healthy volunteers. Br. J. Clin. Pharmacol. 2014, 78, 970–980. [Google Scholar] [CrossRef] [PubMed]
- Yanai, K.; Hiraoka, K.; Kárpáti, A.; Naganuma, F.; Okamura, N.; Tashiro, M.; Nakamura, T.; Yoshikawa, T. Histamine H1 receptor occupancy in human brain. In Histamine Receptors: Preclinical and Clinical Aspects. The Receptors; Blandina, P., Passani, B.M., Eds.; Humana Press: Cham, Switzerland, 2016; Volume 28, pp. 311–326. [Google Scholar]
- Obradovic, T.; Dobson, G.G.; Shingaki, T.; Kungu, T.; Hidalgo, I.J. Assessment of the first and second generation antihistamines brain penetration and role of P-glycoprotein. Pharm. Res. 2007, 24, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Lucero, M.L.; Gonzalo, A.; Ganza, A.; Leal, N.; Soengas, I.; Ioja, E.; Gedey, S.; Jahic, M.; Bednarczyk, D. Interactions of bilastine, a new oral H1 antihistamine, with human transporter systems. Drug Chem. Toxicol. 2012, 35 (Suppl. 1), 8–17. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Funahashi, J.; Mori, K.; Hayashi, K.; Yano, H. The noncompetitive antagonism of histamine H1 receptors expressed in Chinese hamster ovary cells by olopatadine hydrochloride: Its potency and molecular mechanism. Pharmacology 2008, 81, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Corcóstegui, R.; Labeaga, L.; Innerárity, A.; Berisa, A.; Orjales, A. Preclinical pharmacology of bilastine, a new selective histamine H1 receptor antagonist: Receptor selectivity and in vitro antihistaminic activity. Drugs R D 2005, 6, 371–384. [Google Scholar] [CrossRef]
- Bosma, R.; van den Bor, J.; Vischer, H.F.; Labeaga, L.; Leurs, R. The long duration of action of the second generation antihistamine bilastine coincides with its long residence time at the histamine H1 receptor. Eur. J. Pharmacol. 2018, 838, 107–111. [Google Scholar] [CrossRef]
- Church, M.K.; Maurer, M.; Simons, F.E.; Bindslev-Jensen, C.; van Cauwenberge, P.; Bousquet, J.; Holgate, S.T.; Zuberbier, T. Risk of first-generation H1-antihistamines: A GA2LEN position paper. Allergy 2010, 65, 459–466. [Google Scholar] [CrossRef]
- Yanai, K.; Rogala, B.; Chugh, K.; Paraskakis, E.; Pampura, A.N.; Boev, R. Safety considerations in the management of allergic diseases: Focus on antihistamines. Curr. Med. Res. Opin. 2012, 28, 623–642. [Google Scholar] [CrossRef]
- Dresser, G.K.; Bailey, D.G.; Leake, B.F.; Schwarz, U.I.; Dawson, P.A.; Freeman, D.J.; Kim, R.B. Fruit juices inhibit organic anion transporting polypeptide-mediated drug uptake to decrease the oral availability of fexofenadine. Clin. Pharmacol. Ther. 2002, 71, 11–20. [Google Scholar] [CrossRef]
- Kuna, P.; Bachert, C.; Nowacki, Z.; van Cauwenberge, P.; Agache, I.; Fouquert, L.; Roger, A.; Sologuren, A.; Valiente, R. Efficacy and safety of bilastine 20 mg compared with cetirizine 10 mg and placebo for the symptomatic treatment of seasonal allergic rhinitis: A randomized, double-blind, parallel-group study. Clin. Exp. Allergy 2009, 39, 1338–1347. [Google Scholar] [CrossRef]
- Bachert, C.; Kuna, P.; Sanquer, F.; Ivan, P.; Dimitrov, V.; Gorina, M.M.; van de Heyning, P.; Loureiro, A. Comparison of the efficacy and safety of bilastine 20 mg vs desloratadine 5 mg in seasonal allergic rhinitis patients. Allergy 2009, 6, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.; Zieglmayer, P.; Zieglmayer, R.; Lemell, P. The effects of bilastine compared with cetirizine, fexofenadine, and placebo on allergen-induced nasal and ocular symptoms in patients exposed to aeroallergen in the Vienna Challenge Chamber. Inflamm. Res. 2010, 59, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Hashiguchi, K.; Wakabayashi, K.I.; Togawa, M.; Saito, A.; Okubo, K. Therapeutic effect of bilastine in Japanese cedar pollinosis using an artificial exposure chamber (OHIO Chamber). Allergol. Int. 2017, 66, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sastre, J.; Mullol, J.; Valero, A.; Valiente, R. Efficacy and safety of bilastine 20 mg compared with cetirizine 10 mg and placebo in the treatment of perennial allergic rhinitis. Curr. Med. Res. Opin. 2012, 28, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Okubo, K.; Gotoh, M.; Asako, M.; Nomura, Y.; Togawa, M.; Saito, A.; Honda, T.; Ohashi, Y. Efficacy and safety of bilastine in Japanese patients with perennial allergic rhinitis: A multicenter, randomized, double-blind, placebo-controlled, parallel-group phase III study. Allergol. Int. 2017, 66, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Gea, C.; Martínez-Colomer, J.; Antonijoan, R.M.; Valiente, R.; Barbanoj, M.J. Comparison of peripheral and central effects of single and repeated oral dose administrations of bilastine, a new H1 antihistamine: A dose-range study in healthy volunteers with hydroxyzine and placebo as control treatments. J. Clin. Psychopharmacol. 2008, 28, 675–685. [Google Scholar] [CrossRef]
- Conen, S.; Theunissen, E.L.; Van Oers, A.C.; Valiente, R.; Ramaekers, J.G. Acute and subchronic effects of bilastine (20 and 40 mg) and hydroxyzine (50 mg) on actual driving performance in healthy volunteers. J. Psychopharmacol. 2011, 25, 1517–1523. [Google Scholar] [CrossRef]
- Jáuregui, I.; Ramaekers, J.G.; Yanai, K.; Farré, M.; Redondo, E.; Valiente, R.; Labeaga, L. Bilastine: A new antihistamine with an optimal benefit-to-risk ratio for safety during driving. Expert Opin. Drug Saf. 2016, 15, 89–98. [Google Scholar] [CrossRef]
- García-Gea, C.; Martínez, J.; Ballester, M.R.; Gich, I.; Valiente, R.; Antonijoan, R.M. Psychomotor and subjective effects of bilastine, hydroxyzine, and cetirizine, in combination with alcohol: A randomized, double-blind, crossover, and positive-controlled and placebo-controlled Phase I clinical trials. Hum. Psychopharmacol. 2014, 29, 120–132. [Google Scholar] [CrossRef]
- Brozek, J.L.; Bousquet, J.; Baena-Cagnani, C.E.; Bonini, S.; Canonica, G.W.; Casale, T.B.; van Wijk, R.G.; Ohta, K.; Zuberbier, T.; Schünemann, H.J. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J. Allergy Clin. Immunol. 2010, 126, 466–476. [Google Scholar] [CrossRef]
- Senda, M.; Kubo, N.; Adachi, K.; Ikari, Y.; Matsumoto, K.; Shimizu, K.; Tominaga, H. Cerebral histamine H1 receptor binding potential measured with PET under a test dose of olopatadine, an antihistamine, is reduced after repeated administration of olopatadine. J. Nucl. Med. 2009, 50, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Novák, Z.; Yáñez, A.; Kiss, I.; Kuna, P.; Tortajada-Girbés, M.; Valiente, R. Safety and tolerability of bilastine 10 mg administered for 12 weeks in children with allergic diseases. Pediatr. Allergy Immunol. 2016, 27, 493–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuberbier, T.; Aberer, W.; Asero, R.; Bindslev-Jensen, C.; Brzoza, Z.; Canonica, G.W.; Church, M.K.; Ensina, L.F.; Giménez-Arnau, A.; Godse, K.; et al. The EAACI/GA2 LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: The 2013 revision and update. Allergy 2014, 69, 868–887. [Google Scholar] [CrossRef] [PubMed]
- Krause, K.; Spohr, A.; Zuberbier, T.; Church, M.K.; Maurer, M. Up-dosing with bilastine results in improved effectiveness in cold contact urticaria. Allergy 2013, 68, 921–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Church, M.K. Safety and efficacy of bilastine: A new H1-antihistamine for the treatment of allergic rhinoconjunctivitis and urticaria. Expert Opin. Drug Saf. 2011, 10, 779–793. [Google Scholar] [CrossRef] [PubMed]
- Antonijoan, R.; Coimbra, J.; García-Gea, C.; Puntes, M.; Gich, I.; Campo, C.; Valiente, R.; Labeaga, L. Comparative efficacy of bilastine, desloratadine and rupatadine in the suppression of wheal and flare response induced by intradermal histamine in healthy volunteers. Curr. Med. Res. Opin. 2017, 33, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Jutel, M.; Watanabe, T.; Klunker, S.; Akdis, M.; Thomet, O.A.; Malolepszy, J.; Zak-Nejmark, T.; Koga, R.; Kobayashi, T.; Blaser, K.; et al. Histamine regulates T-cell and antibody responses by differential expression of H1 and H2 receptors. Nature 2001, 413, 420–425. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Bilastine | Fexofenadine | Cetirizine | Levocetirizine | Loratadine | Desloratadine | Ebastine |
|---|---|---|---|---|---|---|---|
| H1 receptor selectivity | +++ | + | + | ++ | + | ++ | ++ |
| Affinity for H2/3 receptors | ± | ± | ± | ± | ± | ± | + |
| Metabolism | Not metabolized | ± | ± | ++ | +++ | +++ | +++ |
| tmax (h) | 1.3 | 1–3 | 1.0 | 0.9 | 1.0–1.5 | 3.0 | 2.6–4.0 (carebastine metabolite) |
| t1/2 (h) | 14.5 | 11–15 | 10.0 | 7.9 | 8.4 | 27.0 | 15–19 (carebastine metabolite) |
| Indicated for allergic rhinoconjunctivitis? | Yes | No | Yes/No (some but not all formulations) | No | No | No | No |
| Indicated for allergic rhinitis? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Indicated for urticaria? | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Pediatric indication? | No (ongoing studies) | children > 3 years | children 6–12 years | children > 2 years | children > 2 years | children > 1 year | children > 2 years |
| Dosage adjustment in renal impairment? † | No | No | Yes (in moderate to severe) | Yes (in moderate-to-severe) | Yes | Caution (severe impairment) | Caution |
| Dosage adjustment in hepatic impairment? | No | No | Yes (if concomitant renal dysfunction) | Yes (if concomitant renal dysfunction) | Yes (severe disease) | Not mentioned | Caution (in mild to moderate) |
| Dosage adjustment in elderly? | No | No | No (if renal function OK) | Yes (for concomitant moderate-to-severe renal impairment) | No | Not mentioned | No |
| Interaction with food? | Yes (give on empty stomach) | Not mentioned | No | No | No | No | No |
| Use in pregnancy and lactation? | Caution (very limited data) | No | Caution | Caution | No | No | No |
| Clinically relevant drug interactions? | No | Yes (antacids) | No | Unlikely (no available data) | Potential (with inhibitors of CYP3A4 and CYP2D6) | No | Caution |
| Interaction with alcohol? | No | Not mentioned | Caution | Caution | No | No | No |
| Can patients drive and operate machinery (i.e., lack of sedative potential)? | Yes (caution: drowsiness) | Yes (impairment unlikely) | Yes (check drug response when intending to drive) | Yes (check drug response when intending to drive) | Yes (caution: drowsiness) | Yes (caution: drowsiness) | Yes (caution: somnolence) |
| Contraindications | None | None | Severe renal impairment | Severe renal impairment | None | None | Severe hepatic impairment |
| Number of ARIA recommended antihistamine properties ‡ | 10 | 9.5 | 6 | 6.5 | 6.5 | 6.5 | 6.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawauchi, H.; Yanai, K.; Wang, D.-Y.; Itahashi, K.; Okubo, K. Antihistamines for Allergic Rhinitis Treatment from the Viewpoint of Nonsedative Properties. Int. J. Mol. Sci. 2019, 20, 213. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20010213
Kawauchi H, Yanai K, Wang D-Y, Itahashi K, Okubo K. Antihistamines for Allergic Rhinitis Treatment from the Viewpoint of Nonsedative Properties. International Journal of Molecular Sciences. 2019; 20(1):213. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20010213
Chicago/Turabian StyleKawauchi, Hideyuki, Kazuhiko Yanai, De-Yun Wang, Koju Itahashi, and Kimihiro Okubo. 2019. "Antihistamines for Allergic Rhinitis Treatment from the Viewpoint of Nonsedative Properties" International Journal of Molecular Sciences 20, no. 1: 213. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20010213