Quercetin, a Promising Clinical Candidate for The Prevention of Contrast-Induced Nephropathy

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Basal Renal Function
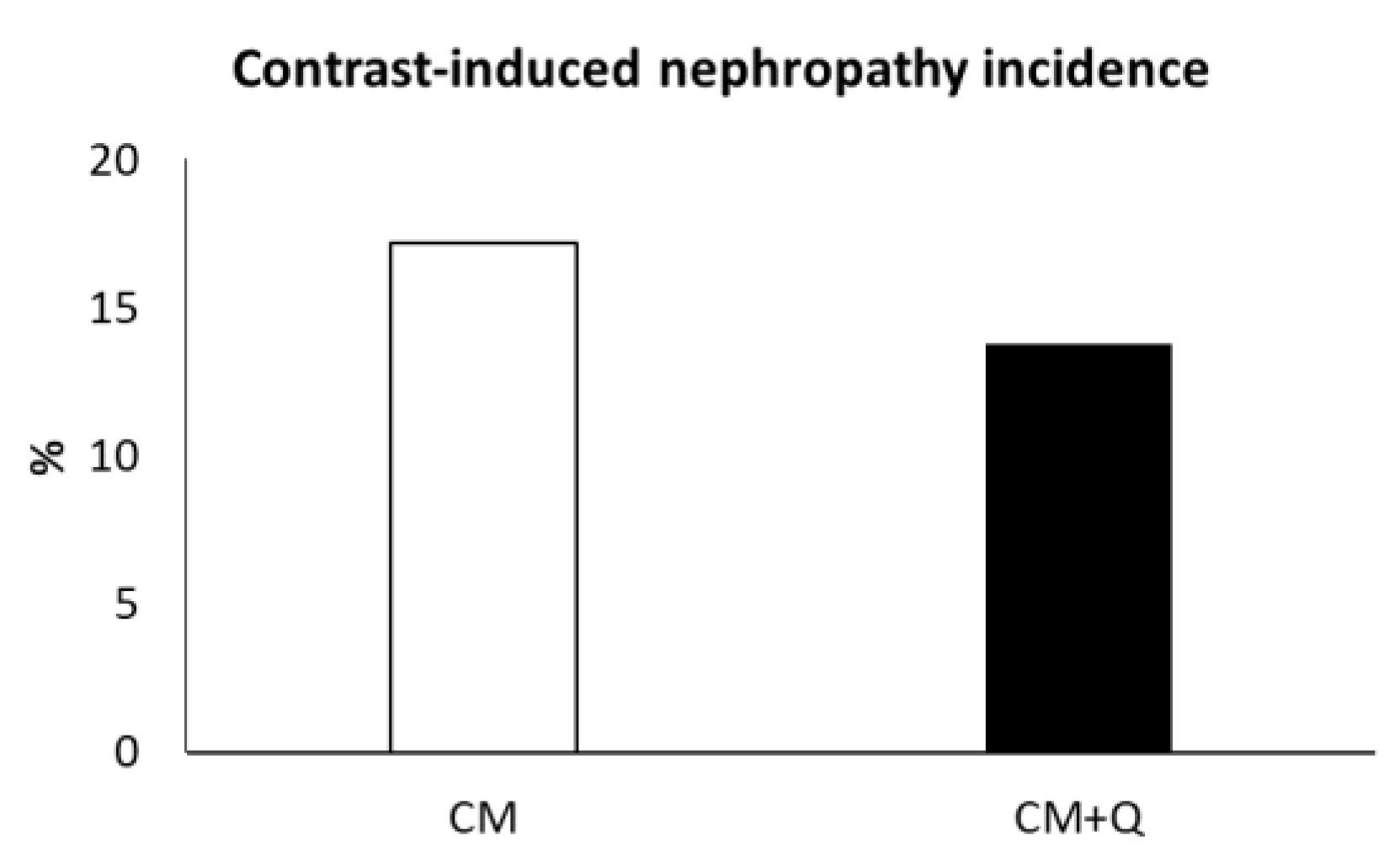
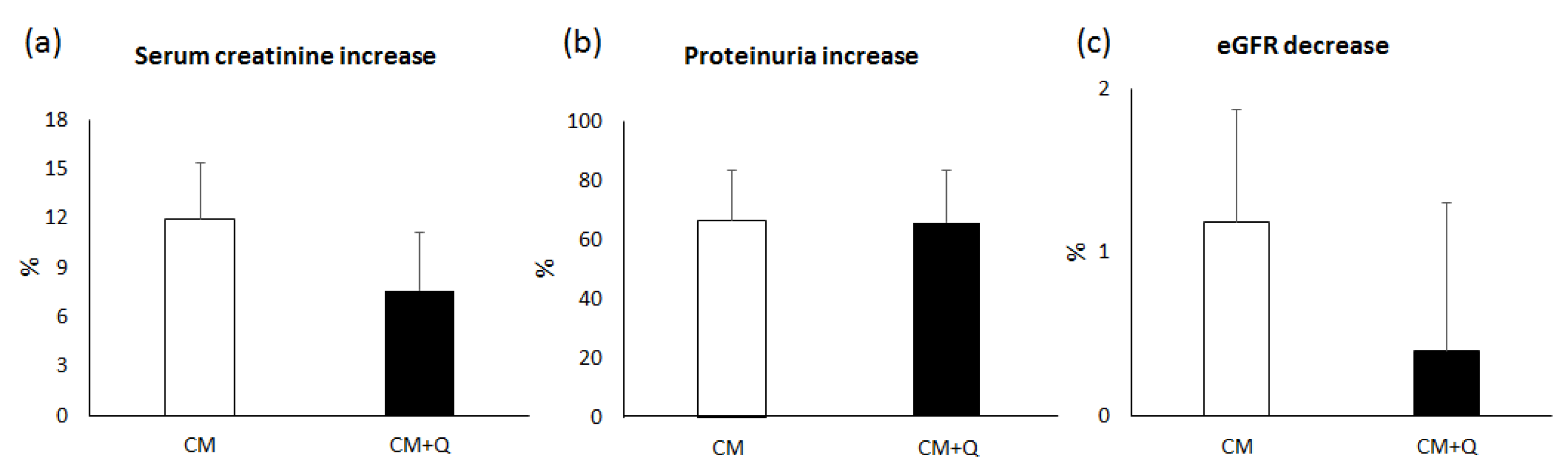
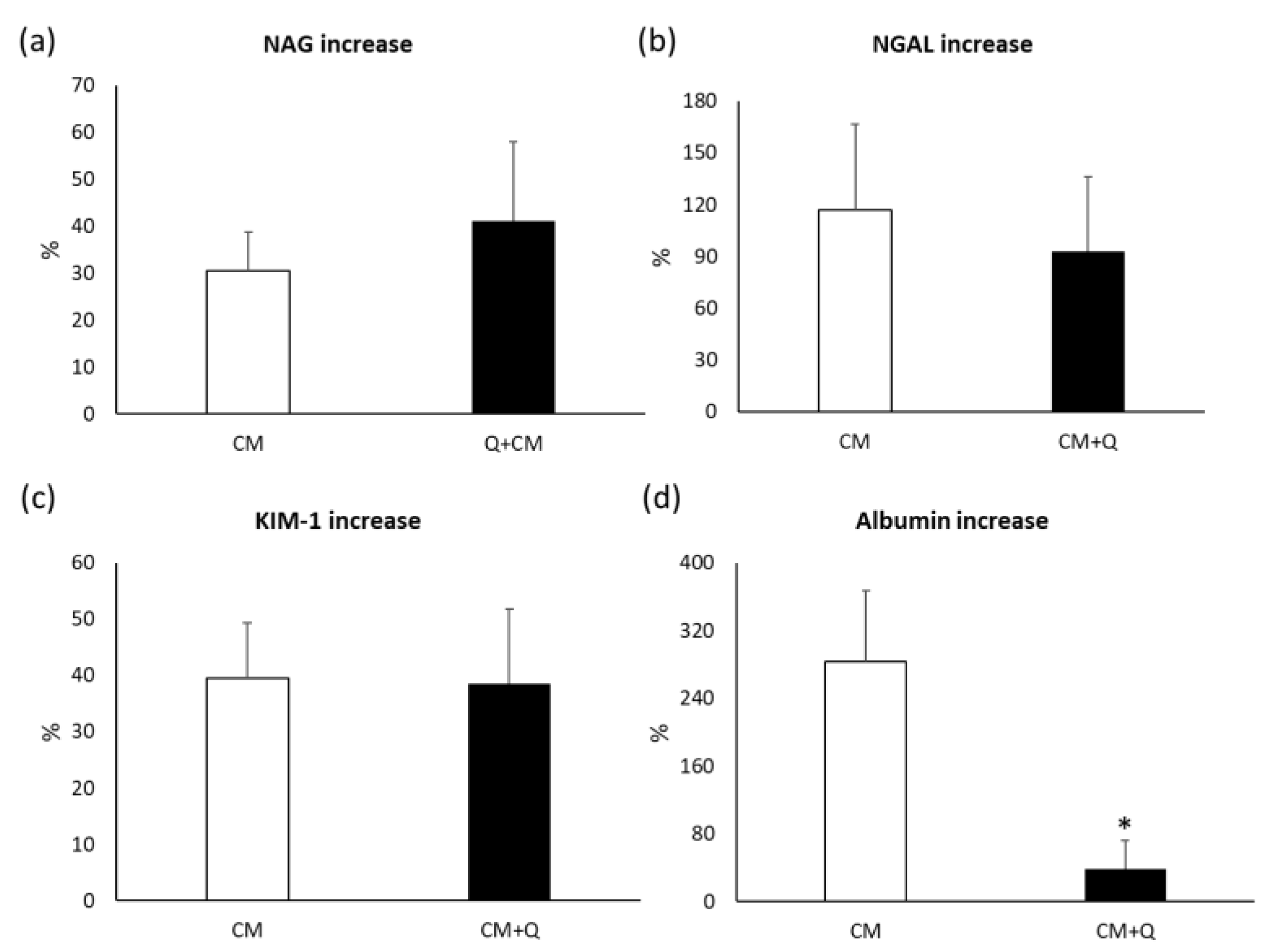
2.3. Quercetin Efficacy as Nephroprotector
2.4. Relative Risk of CIN from Each Risk Factor
2.5. Quercetin Safety
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Samples and Clinical Data Collection
4.3. Renal Function Evaluation
4.4. Statistical Analysis
4.5. Relative Risk (RR) of CIN Calculation
4.6. Quercetin Safety
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACE | Angiotensin converting enzyme |
| ARBs | Angiotensin II receptor blockers |
| ASA | Acetyl salicylic acid |
| BMI | Body mass index |
| CIN | Contrast-induced nephropathy |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration |
| CM | Contrast media |
| Crs | Serum creatinine |
| eGFR | Estimated glomerular filtration rate |
| GFR | Glomerular filtration rate |
| KIM-1 | Kidney injury molecule 1 |
| NAG | N-acetyl-β-D-glucosaminidase |
| NGAL | Neutrophil gelatinase-associated lipocalin |
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
| Q | Quercetin |
| RR | Relative risk |
| SEM | Standard error of the mean |
References
- Morcos, S.K.; Thomsen, H.S. European Society of Urogenital Radiology guidelines on administering contrast media. Abdom Imaging 2003, 28, 0187–0190. [Google Scholar] [CrossRef] [PubMed]
- Andreucci, M.; Faga, T.; Pisani, A.; Sabbatini, M.; Michael, A. Acute kidney injury by radiographic contrast media: Pathogenesis and prevention. Biomed. Res. Int. 2014, 2014, 362725. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Lauri, G.; Assanelli, E.; Campodonico, J.; Metrio, M.D.; Marana, I.; Grazi, M.; Veglia, F.; Bartorelli, A.L. Contrast-induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J. Am. Coll. Cardiol. 2004, 44, 1780–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rihal, C.S.; Textor, S.C.; Grill, D.E.; Berger, P.B.; Ting, H.H.; Best, P.J.; Singh, M.; Bell, M.R.; Barsness, G.W.; Mathew, V.; et al. Incidence and Prognostic Importance of Acute Renal Failure After Percutaneous Coronary Intervention. Circulation 2002, 105, 2259–2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, P.J.M.; Lennon, R.; Ting, H.H.; Bell, M.R.; Rihal, C.S.; Holmes, D.R.; Berger, P.B. The impact of renal insufficiency on clinical outcomes in patients undergoing percutaneous coronary interventions. J. Am. Coll. Cardiol. 2002, 39, 1113–1119. [Google Scholar] [CrossRef] [Green Version]
- Caiazza, A.; Russo, L.; Sabbatini, M.; Russo, D. Hemodynamic and Tubular Changes Induced by Contrast Media. Biomed Res. Int. 2014, 2014, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoungas, S.; Ninomiya, T.; Huxley, R.; Cass, A.; Jardine, M.; Gallagher, M.; Patel, A.; Vasheghani-Farahani, A.; Sadigh, G.; Perkovic, V. Systematic Review: Sodium Bicarbonate Treatment Regimens for the Prevention of Contrast-Induced Nephropathy. Ann. Intern. Med. 2009, 151, 631. [Google Scholar] [CrossRef]
- Solomon, R.; Werner, C.; Mann, D.; D’Elia, J.; Silva, P. Effects of Saline, Mannitol, and Furosemide on Acute Decreases in Renal Function Induced by Radiocontrast Agents. N. Engl. J. Med. 1994, 331, 1416–1420. [Google Scholar] [CrossRef]
- Linkermann, A.; Heller, J.-O.; Prókai, A.; Weinberg, J.M.; De Zen, F.; Himmerkus, N.; Szabó, A.J.; Bräsen, J.H.; Kunzendorf, U.; Krautwald, S. The RIP1-kinase inhibitor necrostatin-1 prevents osmotic nephrosis and contrast-induced AKI in mice. J. Am. Soc. Nephrol. 2013, 24, 1545–1557. [Google Scholar] [CrossRef]
- Quiros, Y.; Sánchez-González, P.D.; López-Hernández, F.J.; Morales, A.I.; López-Novoa, J.M. Cardiotrophin-1 Administration Prevents the Renal Toxicity of Iodinated Contrast Media in Rats. Toxicol. Sci. 2013, 132, 493–501. [Google Scholar] [CrossRef] [Green Version]
- Ulusoy, S.; Ozkan, G.; Mungan, S.; Orem, A.; Yulug, E.; Alkanat, M.; Yucesan, F.B. GSPE is superior to NAC in the prevention of contrast-induced nephropathy: Might this superiority be related to caspase 1 and calpain 1? Life Sci. 2014, 103, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Vicente, L.; Prieto, M.; Morales, A.I. Eficacia y seguridad de la quercetina como complemento alimenticio. Rev. De Toxicol. 2013, 30, 171–181. [Google Scholar]
- Morales, A.I.; Vicente-Sánchez, C.; Jerkic, M.; Santiago, J.M.; Sánchez-González, P.D.; Pérez-Barriocanal, F.; López-Novoa, J.M. Effect of quercetin on metallothionein, nitric oxide synthases and cyclooxygenase-2 expression on experimental chronic cadmium nephrotoxicity in rats. Toxicol. Appl. Pharmacol. 2006, 210, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Morales, A.I.; Vicente-Sánchez, C.; Sandoval, J.M.S.; Egido, J.; Mayoral, P.; Arévalo, M.A.; Fernández-Tagarro, M.; López-Novoa, J.M.; Pérez-Barriocanal, F. Protective effect of quercetin on experimental chronic cadmium nephrotoxicity in rats is based on its antioxidant properties. Food Chem. Toxicol. 2006, 44, 2092–2100. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Gonzalez, P.D.; Lopez-Hernandez, F.J.; Perez-Barriocanal, F.; Morales, A.I.; Lopez-Novoa, J.M. Quercetin reduces cisplatin nephrotoxicity in rats without compromising its anti-tumour activity. Nephrol. Dial. Transplant. 2011, 26, 3484–3495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlmann, M.K.; Burkhardt, G.; Horsch, E.; Wagner, M.; Köhler, H. Inhibition of oxidant-induced lipid peroxidation in cultured renal tubular epithelial cells (LLC-PK1) by quercetin. Free Radic. Res. 1998, 29, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Shoskes, D.A. Effect of bioflavonoids quercetin and curcumin on ischemic renal injury: A new class of renoprotective agents. Transplantation 1998, 66, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Askari, G.; Hajishafiee, M.; Ghiasvand, R.; Hariri, M.; Darvishi, L.; Ghassemi, S.; Iraj, B.; Hovsepian, V. Quercetin and Vitamin C Supplementation: Effects on Lipid Profile and Muscle Damage in Male Athletes. Int. J. Prev. Med. 2013, 4, S58–S62. [Google Scholar]
- Broman-Fulks, J.J.; Canu, W.H.; Trout, K.L.; Nieman, D.C. The effects of quercetin supplementation on cognitive functioning in a community sample: A randomized, placebo-controlled trial. Ther. Adv. Psychopharmacol. 2012, 2, 131–138. [Google Scholar] [CrossRef]
- Clifton, P.M. Effect of Grape Seed Extract and Quercetin on Cardiovascular and Endothelial Parameters in High-Risk Subjects. J. Biomed. Biotechnol. 2004, 2004, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Conquer, J.A.; Maiani, G.; Azzini, E.; Raguzzini, A.; Holub, B.J. Supplementation with quercetin markedly increases plasma quercetin concentration without effect on selected risk factors for heart disease in healthy subjects. J. Nutr. 1998, 128, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Daneshvar, P.; Hariri, M.; Ghiasvand, R.; Askari, G.; Darvishi, L.; Mashhadi, N.S.; Khosravi-boroujeni, H. Effect of eight weeks of quercetin supplementation on exercise performance, muscle damage and body muscle in male badminton players. Int. J. Prev. Med. 2013, 4, S53. [Google Scholar] [PubMed]
- Edwards, R.L.; Lyon, T.; Litwin, S.E.; Rabovsky, A.; Symons, J.D.; Jalili, T. Quercetin reduces blood pressure in hypertensive subjects. J. Nutr. 2007, 137, 2405–2411. [Google Scholar] [CrossRef] [PubMed]
- Egert, S.; Wolffram, S.; Bosy-Westphal, A.; Boesch-Saadatmandi, C.; Wagner, A.E.; Frank, J.; Rimbach, G.; Mueller, M.J. Daily quercetin supplementation dose-dependently increases plasma quercetin concentrations in healthy humans. J. Nutr. 2008, 138, 1615–1621. [Google Scholar] [CrossRef] [PubMed]
- Ferry, D.R.; Smith, A.; Malkhandi, J.; Fyfe, D.W.; deTakats, P.G.; Anderson, D.; Baker, J.; Kerr, D.J. Phase I clinical trial of the flavonoid quercetin: Pharmacokinetics and evidence for in vivo tyrosine kinase inhibition. Clin. Cancer Res. 1996, 2, 659–668. [Google Scholar]
- Katske, F.; Shoskes, D.A.; Sender, M.; Poliakin, R.; Gagliano, K.; Rajfer, J. Treatment of interstitial cystitis with a quercetin supplement. Tech. Urol. 2001, 7, 44–46. [Google Scholar]
- Lee, K.-H.; Park, E.; Lee, H.-J.; Kim, M.-O.; Cha, Y.-J.; Kim, J.-M.; Lee, H.; Shin, M.-J. Effects of daily quercetin-rich supplementation on cardiometabolic risks in male smokers. Nutr. Res. Pract. 2011, 5, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Lozoya, X.; Reyes-Morales, H.; Chávez-Soto, M.A.; Martínez-García, M.d.C.; Soto-González, Y.; Doubova, S.V. Intestinal anti-spasmodic effect of a phytodrug of Psidium guajava folia in the treatment of acute diarrheic disease. J. Ethnopharmacol. 2002, 83, 19–24. [Google Scholar] [CrossRef]
- Shoskes, D.A.; Zeitlin, S.I.; Shahed, A.; Rajfer, J. Quercetin in men with category III chronic prostatitis: A preliminary prospective, double-blind, placebo-controlled trial. Urology 1999, 54, 960–963. [Google Scholar] [CrossRef]
- Rear, R.; Bell, R.M.; Hausenloy, D.J. Contrast-induced nephropathy following angiography and cardiac interventions. Heart 2016, 102, 638–648. [Google Scholar] [CrossRef] [Green Version]
- Martens, R.J.H.; Houben, A.J.H.M.; Kooman, J.P.; Berendschot, T.T.J.M.; Dagnelie, P.C.; van der Kallen, C.J.H.; Kroon, A.A.; Leunissen, K.M.L.; van der Sande, F.M.; Schaper, N.C.; et al. Microvascular endothelial dysfunction is associated with albuminuria: The Maastricht Study. J. Hypertens. 2018, 36, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, Y.; Yuksel, R.; Yagmurca, M.; Haltas, H.; Erdamar, H.; Toktas, M.; Ozcan, O. Effects of quercetin on methotrexate-induced nephrotoxicity in rats. Hum. Exp. Toxicol. 2017, 36, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Pate, G.E.; Shalansky, S.; Al-Shamari, A.; Webb, J.G.; Buller, C.E.; Humphries, K.H. N-acetylcysteine reduces urinary albumin excretion following contrast administration: Evidence of biological effect. Nephrol. Dial. Transplant. 2007, 22, 2520–2524. [Google Scholar] [CrossRef] [PubMed]
- Bolisetty, S.; Agarwal, A. Urine albumin as a biomarker in acute kidney injury. Am. J. Physiol. Ren. Physiol. 2011, 300, F626–F627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudnick, M.R.; Goldfarb, S.; Wexler, L.; Ludbrook, P.A.; Murphy, M.J.; Halpern, E.F.; Hill, J.A.; Winniford, M.; Cohen, M.B.; VanFossen, D.B. Nephrotoxicity of ionic and nonionic contrast media in 1196 patients: A randomized trial. Kidney Int. 1995, 47, 254–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwab, S.J.; Hlatky, M.A.; Pieper, K.S.; Davidson, C.J.; Morris, K.G.; Skelton, T.N.; Bashore, T.M. Contrast nephrotoxicity: A randomized controlled trial of a nonionic and an ionic radiographic contrast agent. N. Engl. J. Med. 1989, 320, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Jungbauer, C.G.; Uecer, E.; Stadler, S.; Birner, C.; Buchner, S.; Maier, L.S.; Luchner, A. N-acteyl-\s s-D-glucosaminidase and kidney injury molecule-1: New predictors for long-term progression of chronic kidney disease in patients with heart failure. Nephrology 2016, 21, 490–498. [Google Scholar] [CrossRef]
- Sheira, G.; Noreldin, N.; Tamer, A.; Saad, M. Urinary biomarker N-acetyl-β-D-glucosaminidase can predict severity of renal damage in diabetic nephropathy. J. Diabetes Metab. Disord. 2015, 14, 4. [Google Scholar] [CrossRef] [PubMed]
- Han, W.K.; Waikar, S.S.; Johnson, A.; Betensky, R.A.; Dent, C.L.; Devarajan, P.; Bonventre, J.V. Urinary biomarkers in the early diagnosis of acute kidney injury. Kidney Int. 2008, 73, 863–869. [Google Scholar] [CrossRef] [Green Version]
- Sirota, J.C.; Klawitter, J.; Edelstein, C.L. Biomarkers of Acute Kidney Injury. Available online: https://www.hindawi.com/journals/jt/2011/328120/ (accessed on 10 April 2019).
- Li, W.-H.; Wang, L.; He, H.-Y.; Chen, J.; Yu, Y.-R. Expression of neutrophil gelatinase-associated lipocalin in low osmolar contrast-induced nephropathy in rats and the effect of N-acetylcysteine. Exp. Ther. Med. 2016, 12, 3175–3180. [Google Scholar] [CrossRef] [Green Version]
- Bonventre, J.V. Kidney injury molecule-1 (KIM-1): A urinary biomarker and much more. Nephrol. Dial. Transpl. 2009, 24, 3265–3268. [Google Scholar] [CrossRef] [PubMed]
- Huxley, R.R.; Neil, H.A.W. The relation between dietary flavonol intake and coronary heart disease mortality: A meta-analysis of prospective cohort studies. Eur. J. Clin. Nutr. 2003, 57, 904. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-H. Renal Effects of Prostaglandins and Cyclooxygenase-2 Inhibitors. Electrolytes Blood Press. 2008, 6, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollman, P.C.; de Vries, J.H.; van Leeuwen, S.D.; Mengelers, M.J.; Katan, M.B. Absorption of dietary quercetin glycosides and quercetin in healthy ileostomy volunteers. Am. J. Clin. Nutr. 1995, 62, 1276–1282. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Laskey, W.K.; Jenkins, C.; Selzer, F.; Marroquin, O.C.; Wilensky, R.L.; Glaser, R.; Cohen, H.A.; Holmes, D.R.; Investigators, N.D.R. Volume-to-creatinine clearance ratio: A pharmacokinetically based risk factor for prediction of early creatinine increase after percutaneous coronary intervention. J. Am. Coll. Cardiol. 2007, 50, 584–590. [Google Scholar] [CrossRef]
- Yamamoto, M.; Hayashida, K.; Mouillet, G.; Chevalier, B.; Meguro, K.; Watanabe, Y.; Dubois-Rande, J.-L.; Morice, M.-C.; Lefèvre, T.; Teiger, E. Renal function–based contrast dosing predicts acute kidney injury following transcatheter aortic valve implantation. JACC Cardiovasc. Interv. 2013, 6, 479–486. [Google Scholar] [CrossRef]
- Sadat, U.; Usman, A.; Boyle, J.R.; Hayes, P.D.; Solomon, R.J. Contrast medium-induced acute kidney injury. Cardiorenal Med. 2015, 5, 219–228. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | ||
|---|---|---|
| CM Group | CM+Q Group | |
| Anthropometric Characteristics | ||
| Men (%) | 77.6 | 67.3 |
| Women (%) | 22.4 | 32.7 |
| Age (years; mean ± SEM) (minimum-maximum) | 71.4 ± 1.1 (39–91) | 68.5 ± 1.4 (46–88) |
| BMI (mean ± SEM) | 27.6 ± 0.4 | 31.8 ± 3.7 |
| Risk Factors | ||
| Diabetes mellitus (%) | 27.6 | 31.0 |
| Dyslipidemia (%) | 44.0 | 51.7 |
| Arterial hypertension (%) | 56.7 | 53.4 |
| Smoking (%) | 20.1 | 36.2 * |
| Type of Contrast Agent | ||
| CM administered (%)/ | ||
| Volume mL (mean ± SEM) | ||
| Iodixanol | 70.1/ 295.0 ± 15.0 | 63.8/ 274.1 ± 18.7 |
| Iohexol | 22.4/ 260.0 ± 21.7 | 25.9/ 308.4 ± 28.0 |
| Iodine (not specified) | 0.8/ 100.0 ± 0.0 | 3.5/ 600.0 ± 0.0 |
| Without data | 6.7 | 5.2 |
| Pharmacological Group | CM Group | CM+Q Group |
|---|---|---|
| Hypertension Treatment | ||
| ACE inhibitors | 26.9 | 27.6 |
| Aldosterone receptor antagonists | 0.8 | 2.12 |
| Alpha blockers | 4.1 | 10.6 |
| ARBs | 15.4 | 17.0 |
| Beta blockers | 26.9 | 19.1 |
| Calcium channels antagonists | 17.9 | 4.2 |
| Diuretics | 28.5 | 23.4 |
| Dyslipidemia Treatment | ||
| Statins | 38.2 | 31.9 |
| Diabetes Mellitus Treatment | ||
| Antidiabetics | 21.1 | 21.3 |
| Thrombus Prevention Treatment | ||
| ASA | 35.8 | 31.9 |
| Antiplatelet agents | 25.2 | 12.8 |
| Others | ||
| NSAIDs | 7.3 | 17.0 |
| CM Group | CM+Q Group | |
|---|---|---|
| Crs (mg/dL) | 1.08 ± 0.04 | 0.96 ± 0.04 |
| Serum urea (mg/dL) | 52.20 ± 2.54 | 48.91 ± 3.00 |
| eGFR CKD-EPI (mL/min/1.73 m2) | 82.61 ± 1.09 | 85.93 ± 1.44 |
| Risk Factor | CM | CM+Q | ||||
|---|---|---|---|---|---|---|
| RR | 95% Confidence Interval | RR | 95% Confidence Interval | |||
| Lower Limit | Upper Limit | Lower Limit | Upper Limit | |||
| Arterial hypertension | 1.19 | 0.83 | 1.68 | 0.87 | 0.41 | 3.85 |
| Diabetes mellitus | 1.15 | 0.57 | 2.29 | 0.74 | 0.21 | 2.63 |
| Dyslipidemia | 0.73 | 0.41 | 1.32 | 1.56 | 0.85 | 2.82 |
| Smoking | 1.17 | 0.50 | 2.71 | 1.06 | 0.40 | 2.78 |
| CM volume >350 mL | 1.83 * | 1.07 | 3.14 | 0.80 | 0.22 | 2.86 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicente-Vicente, L.; González-Calle, D.; Casanova, A.G.; Hernández-Sánchez, M.T.; Prieto, M.; Rama-Merchán, J.C.; Martín-Moreiras, J.; Martín-Herrero, F.; Sánchez, P.L.; López-Hernández, F.J.; et al. Quercetin, a Promising Clinical Candidate for The Prevention of Contrast-Induced Nephropathy. Int. J. Mol. Sci. 2019, 20, 4961. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194961
Vicente-Vicente L, González-Calle D, Casanova AG, Hernández-Sánchez MT, Prieto M, Rama-Merchán JC, Martín-Moreiras J, Martín-Herrero F, Sánchez PL, López-Hernández FJ, et al. Quercetin, a Promising Clinical Candidate for The Prevention of Contrast-Induced Nephropathy. International Journal of Molecular Sciences. 2019; 20(19):4961. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194961
Chicago/Turabian StyleVicente-Vicente, Laura, David González-Calle, Alfredo Ginés Casanova, María Teresa Hernández-Sánchez, Marta Prieto, Juan Carlos Rama-Merchán, Javier Martín-Moreiras, Francisco Martín-Herrero, Pedro Luis Sánchez, Francisco J. López-Hernández, and et al. 2019. "Quercetin, a Promising Clinical Candidate for The Prevention of Contrast-Induced Nephropathy" International Journal of Molecular Sciences 20, no. 19: 4961. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194961