Salivary MicroRNA for Diagnosis of Cancer and Systemic Diseases: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Results
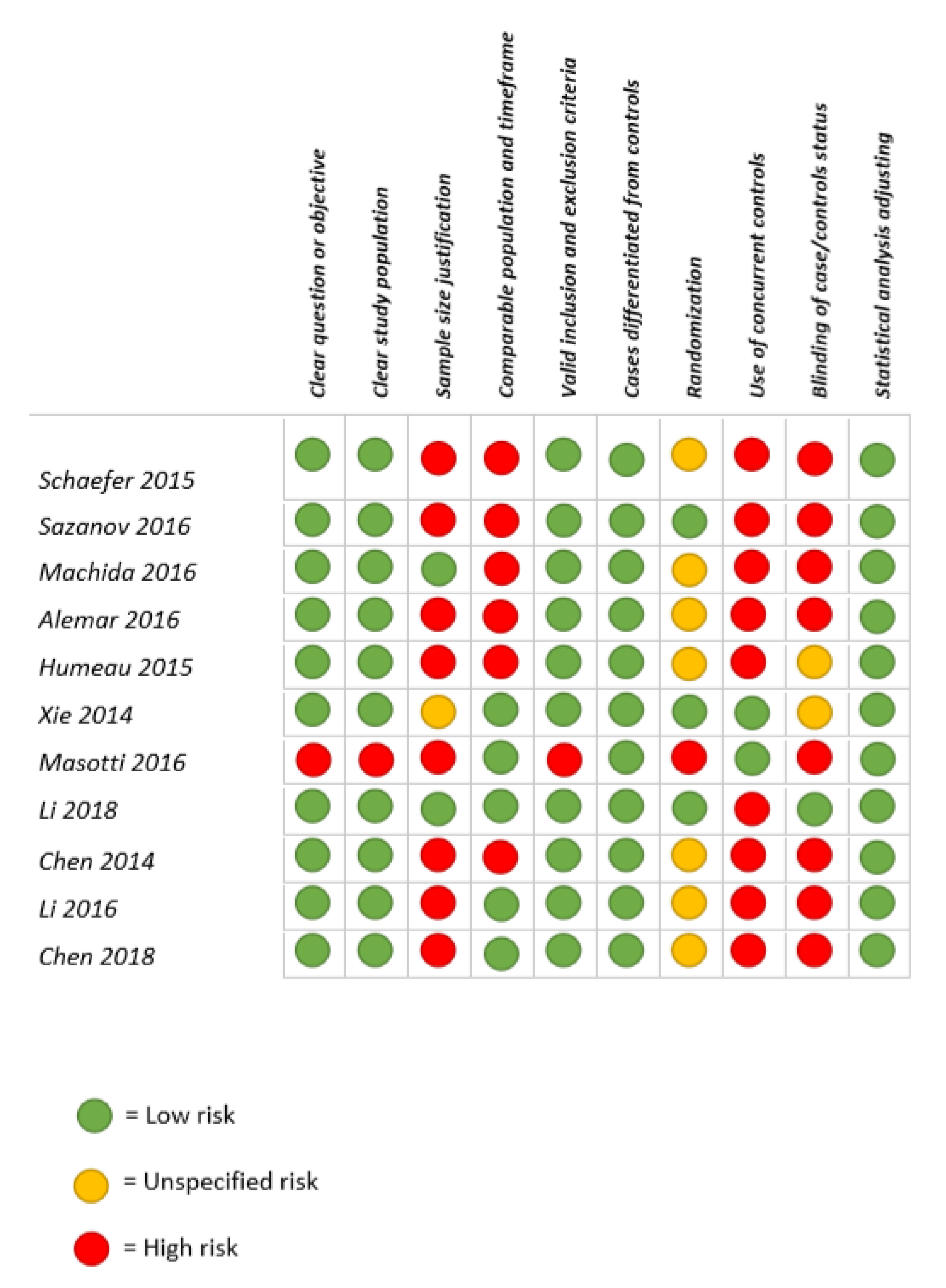
2.1. Quality Assessment
2.2. Level of Evidence
2.3. Disease Investigated
2.4. Type of Saliva and Analytical Techniques
3. Discussion
3.1. Pancreatic Cancer
3.2. Gastric Cancer and Gastric Ulcer
3.3. Colorectal Diseases
3.4. Others (Fibromyalgia, Gastritis, Traditional Chinese Medicine)
4. Materials and Methods
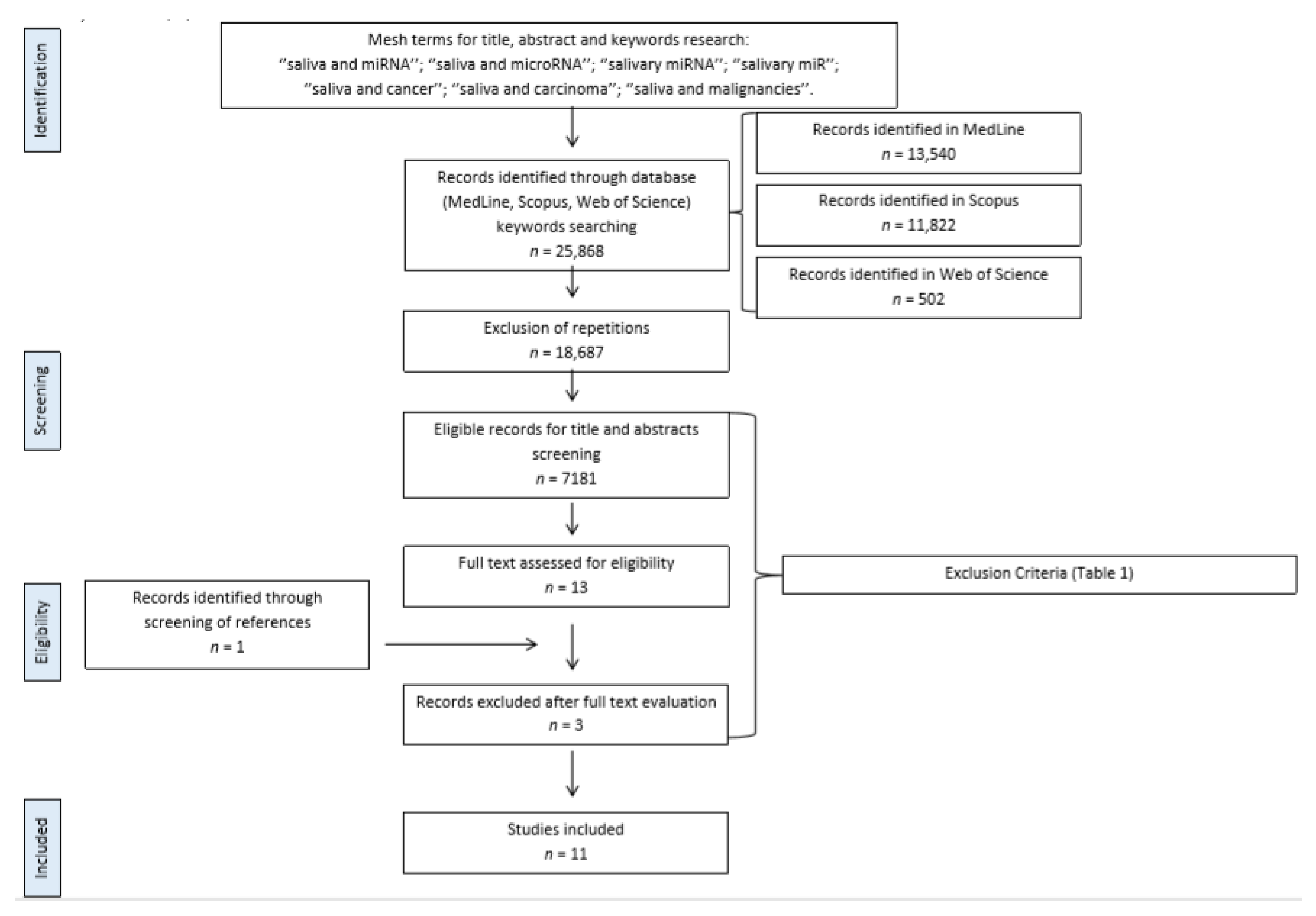
4.1. Search Strategy
4.2. Data Extraction, Quality Assessment, and Critical Appraisal
Author Contributions
Funding
Conflicts of Interest
References
- Lu, M.; Zhang, Q.; Deng, M.; Miao, J.; Guo, Y.; Gao, W.; Cui, Q. An analysis of human microRNA and disease associations. PLoS ONE 2008, 3, e3420. [Google Scholar] [CrossRef] [Green Version]
- Romano, G.; Veneziano, D.; Acunzo, M.; Croce, C.M. Small non-coding RNA and cancer. Carcinogenesis 2017, 38, 485–491. [Google Scholar] [CrossRef] [Green Version]
- Iorio, M.V.; Croce, C.M. microRNA involvement in human cancer. Carcinogenesis 2012, 33, 1126–1133. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrie, C.H.; Gal, S.; Dunlop, H.M.; Pushkaran, B.; Liggins, A.P.; Pulford, K.; Banham, A.H.; Pezzella, F.; Boultwood, J.; Wainscoat, J.S.; et al. Detection of elevated levels of tumour-associated microRNAs in serum of patients with diffuse large B-cell lymphoma. Br. J. Haematol. 2008, 141, 672–675. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Rubio, D.; Martin-Burriel, I.; Gil, A.; Cubero, P.; Forner, M.; Khalyfa, A.; Marin, J.M. Stability of Circulating Exosomal miRNAs in Healthy Subjects. Sci. Rep. 2018, 8, 10306. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.Z.; Cheng, X.Q.; Li, J.Y.; Zhang, P.; Yi, P.; Xu, X.; Zhou, X.D. Saliva in the diagnosis of diseases. Int. J. Oral Sci. 2016, 8, 133–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahn, J.H.; Zhang, Q.; Li, F.; Chan, T.M.; Lin, X.; Kim, Y.; Wong, D.T.; Xiao, X. The landscape of microRNA, Piwi-interacting RNA, and circular RNA in human saliva. Clin. Chem. 2015, 61, 221–230. [Google Scholar] [CrossRef] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, J.S.; Attumi, T.; Opekun, A.R.; Abraham, B.; Hou, J.; Shelby, H.; Graham, D.Y.; Streckfus, C.; Klein, J.R. MicroRNA signatures differentiate Crohn’s disease from ulcerative colitis. BMC Immunol. 2015, 16, 5. [Google Scholar] [CrossRef] [Green Version]
- Sazanov, A.A.; Kiselyova, E.V.; Zakharenko, A.A.; Romanov, M.N.; Zaraysky, M.I. Plasma and saliva miR-21 expression in colorectal cancer patients. J. Appl. Genet. 2017, 58, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Machida, T.; Tomofuji, T.; Maruyama, T.; Yoneda, T.; Ekuni, D.; Azuma, T.; Miyai, H.; Mizuno, H.; Kato, H.; Tsutsumi, K.; et al. miR-1246 and miR-4644 in salivary exosome as potential biomarkers for pancreatobiliary tract cancer. Oncol. Rep. 2016, 36, 2375–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alemar, B.; Izetti, P.; Gregorio, C.; Macedo, G.S.; Castro, M.A.; Osvaldt, A.B.; Matte, U.; Ashton-Prolla, P. miRNA-21 and miRNA-34a Are Potential Minimally Invasive Biomarkers for the Diagnosis of Pancreatic Ductal Adenocarcinoma. Pancreas 2016, 45, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Humeau, M.; Vignolle-Vidoni, A.; Sicard, F.; Martins, F.; Bournet, B.; Buscail, L.; Torrisani, J.; Cordelier, P. Salivary MicroRNA in Pancreatic Cancer Patients. PLoS ONE 2015, 10, e0130996. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Yin, X.; Gong, B.; Nie, W.; Wu, B.; Zhang, X.; Huang, J.; Zhang, P.; Zhou, Z.; Li, Z. Salivary microRNAs Show Potential as a Noninvasive Biomarker for Detecting Resectable Pancreatic Cancer. Cancer Prev. Res. 2015, 8, 165. [Google Scholar] [CrossRef] [Green Version]
- Masotti, A.; Baldassarre, A.; Guzzo, M.P.; Iannuccelli, C.; Barbato, C.; Di Franco, M. Circulating microRNA Profiles as Liquid Biopsies for the Characterization and Diagnosis of Fibromyalgia Syndrome. Mol. Neurobiol. 2017, 54, 7129–7136. [Google Scholar] [CrossRef]
- Li, F.; Yoshizawa, J.M.; Kim, K.M.; Kanjanapangka, J.; Grogan, T.R.; Wang, X.Y.; Elashoff, D.E.; Ishikawa, S.; Chia, D.; Liao, W.; et al. Discovery and Validation of Salivary Extracellular RNA Biomarkers for Noninvasive Detection of Gastric Cancer. Clin. Chem. 2018, 64, 1513–1521. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Chen, L.Y.; Wang, P.; Liu, L.M.; Chen, Z. MicroRNA expression in salivary supernatant of patients with pancreatic cancer and its relationship with ZHENG. Biomed. Res. Int. 2014, 2014, 756347. [Google Scholar] [CrossRef]
- Li, X.J.; Wang, L.P.; Li, G.; Zheng, X.F.; Duan, C.H. Expression of miR-204 and MMP-9 in Helicobacter pylori-associated gastric ulcer. Int. J. Clin. Exp. Med. 2016, 9, 7928–7936. [Google Scholar]
- Chen, Y.; Wu, Y.L.; Yao, H.Q.; Luo, H.; Lin, B.; Zhang, X.P.; Liang, X.; Sun, R.R.; Zhao, S.P.; Li, Y.S.; et al. miRNA Expression Profile of Saliva in Subjects of Yang Deficiency Constitution and Yin Deficiency Constitution. Cell. Physiol. Biochem. 2018, 49, 2088–2098. [Google Scholar] [CrossRef]
- Farah, R.; Haraty, H.; Salame, Z.; Fares, Y.; Ojcius, D.M.; Said Sadier, N. Salivary biomarkers for the diagnosis and monitoring of neurological diseases. Biomed. J. 2018, 41, 63–87. [Google Scholar] [CrossRef]
- Koizumi, T.; Shetty, V.; Yamaguchi, M. Salivary cytokine panel indicative of non-small cell lung cancer. J. Int. Med. Res. 2018, 46, 3570–3582. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Huang, S.; Lin, D.; Chen, G.; Xu, Y.; Li, Y.; Huang, Z.; Pan, J.; Chen, R.; Zeng, H. Surface-enhanced Raman spectroscopy of saliva proteins for the noninvasive differentiation of benign and malignant breast tumors. Int. J. Nanomed. 2015, 10, 537–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floriano, P.N.; Christodoulides, N.; Miller, C.S.; Ebersole, J.L.; Spertus, J.; Rose, B.G.; Kinane, D.F.; Novak, M.J.; Steinhubl, S.; Acosta, S.; et al. Use of Saliva-Based Nano-Biochip Tests for Acute Myocardial Infarction at the Point of Care: A Feasibility Study. Clin. Chem. 2009, 55, 1530–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapado-Gonzalez, O.; Majem, B.; Muinelo-Romay, L.; Alvarez-Castro, A.; Santamaria, A.; Gil-Moreno, A.; Lopez-Lopez, R.; Suarez-Cunqueiro, M.M. Human salivary microRNAs in Cancer. J. Cancer 2018, 9, 638–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, N.J.; Zhou, H.; Elashoff, D.; Henson, B.S.; Kastratovic, D.A.; Abemayor, E.; Wong, D.T. Salivary microRNA: Discovery, characterization, and clinical utility for oral cancer detection. Clin. Cancer Res. 2009, 15, 5473–5477. [Google Scholar] [CrossRef] [Green Version]
- Michael, A.; Bajracharya, S.D.; Yuen, P.S.; Zhou, H.; Star, R.A.; Illei, G.G.; Alevizos, I. Exosomes from human saliva as a source of microRNA biomarkers. Oral Dis. 2010, 16, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.N.; Jia, L.F.; Zheng, Y.F.; Li, W.R. Salivary Exosomes: Emerging Roles in Systemic Disease. Int. J. Biol. Sci. 2018, 14, 633–643. [Google Scholar] [CrossRef]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T.W. Salivary Biomarkers: Toward Future Clinical and Diagnostic Utilities. Clin. Microbiol. Rev. 2013, 26, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Streckfus, C.F.; Mayorga-Wark, O.; Arreola, D.; Edwards, C.; Bigler, L.; Dubinsky, W.P. Breast cancer related proteins are present in saliva and are modulated secondary to ductal carcinoma in situ of the breast. Cancer Investig. 2008, 26, 159–167. [Google Scholar] [CrossRef]
- Pepe, M.S.; Feng, Z.D.; Janes, H.; Bossuyt, P.M.; Potter, J.D. Pivotal Evaluation of the Accuracy of a Biomarker Used for Classification or Prediction: Standards for Study Design. J. Natl. Cancer Inst. 2008, 100, 1432–1438. [Google Scholar] [CrossRef] [Green Version]
- Humprey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Edgar, C.; Dawes, D.; O’Mullane, D. Saliva and Oral Health, 4th ed.; Stephen Hancocks Ltd.: London, UK, 2012; pp. 1–154. [Google Scholar]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.J.; Xu, B.H. MicroRNA-21 Identified as Predictor of Cancer Outcome: A Meta-Analysis. PLoS ONE 2014, 9, e103373. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.L.; Li, L.W.; Li, S.Y. Circulating microRNA-21 as a biomarker for the detection of various carcinomas: An updated meta-analysis based on 36 studies. Tumor Biol. 2015, 36, 1973–1981. [Google Scholar] [CrossRef] [PubMed]
- Humeau, M.; Torrisani, J.; Cordelier, P. miRNA in clinical practice: Pancreatic cancer. Clin. Biochem. 2013, 46, 933–936. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.C.; Chin, T.M.; Yang, H.; Nga, M.E.; Lunny, D.P.; Lim, E.K.H.; Sun, L.L.; Pang, Y.H.; Leow, Y.N.; Malusay, S.R.Y.; et al. Tumour-initiating cell-specific miR-1246 and miR-1290 expression converge to promote non-small cell lung cancer progression. Nat. Commun. 2016, 7. [Google Scholar] [CrossRef]
- Zeng, X.J.; Tao, H.L. Diagnostic and prognostic serum marker of cholangiocarcinoma (Review). Oncol. Lett. 2015, 9, 3–8. [Google Scholar] [CrossRef]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [CrossRef]
- Lin, M.S.; Huang, J.X.; Yu, H. Elevated serum level of carbohydrate antigen 19-9 in benign biliary stricture diseases can reduce its value as a tumor marker. Int. J. Clin. Exp. Med. 2014, 7, 744–750. [Google Scholar]
- Ali, S.; Saleh, H.; Sethi, S.; Sarkar, F.H.; Philip, P.A. MicroRNA profiling of diagnostic needle aspirates from patients with pancreatic cancer. Br. J. Cancer 2012, 107, 1354–1360. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.W.; Liu, G.H.; Liu, Y.Q.; Zhao, H.C.; Yang, Z.; Zhao, C.L.; Zhang, X.F.; Ye, H. Over-expression of microRNA-940 promotes cell proliferation by targeting GSK3β and sFRP1 in human pancreatic carcinoma. Biomed. Pharmacother. 2016, 83, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Li, M.J.; Wang, Q.Y.; Xue, F.Q.; Wu, Y.A. lncRNA-CYTOR Works as an Oncogene Through the CYTOR/miR-3679-5p/MACC1 Axis in Colorectal Cancer. DNA Cell Biol. 2019, 38, 572–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grieco, F.A.; Sebastiani, G.; Juan-Mateu, J.; Villate, O.; Marroqui, L.; Ladrière, L.; Tugay, K.; Regazzi, R.; Bugliani, M.; Marchetti, P.; et al. MicroRNAs miR-23a-3p, miR-23b-3p, and miR-149-5p Regulate the Expression of Proapoptotic BH3-Only Proteins DP5 and PUMA in Human Pancreatic β-Cells. Diabetes 2017, 66, 100–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Z.; Yin, S.; Sun, R.C.; Zhang, S.X.; Fu, M.; Wu, Y.L.; Zhang, T.; Khaliq, J.; Li, Y.X. miR-140-5p suppresses the proliferation, migration and invasion of gastric cancer by regulating YES1. Mol. Cancer. 2017, 16, 139. [Google Scholar] [CrossRef]
- Zheng, J.Z.; Huang, Y.N.; Yao, L.; Liu, Y.R.; Liu, S.; Hu, X.; Liu, Z.B.; Shao, Z.M. Elevated miR-301a expression indicates a poor prognosis for breast cancer patients. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.D.; He, X.J.; Tao, H.Q.; Zhang, W.; Wang, Y.Y.; Ye, Z.Y.; Zhao, Z.S. Abnormal expression of miR-301a in gastric cancer associated with progression and poor prognosis. J. Surg. Oncol. 2013, 108, 197–202. [Google Scholar] [CrossRef]
- Mera, R.M.; Bravo, L.E.; Camargo, M.C.; Bravo, J.C.; Delgado, A.G.; Romero-Gallo, J.; Yepez, M.C.; Realpe, J.L.; Schneider, B.G.; Morgan, D.R.; et al. Dynamics of Helicobacter pylori infection as a determinant of progression of gastric precancerous lesions: 16-year follow-up of an eradication trial. Gut 2018, 67, 1239–1246. [Google Scholar] [CrossRef]
- Li, T.Q.; Pan, H.J.; Li, R.S. The dual regulatory role of miR-204 in cancer. Tumor Biol. 2016, 37, 11667–11677. [Google Scholar] [CrossRef] [Green Version]
- Sacconi, A.; Biagioni, F.; Canu, V.; Mori, F.; Di Benedetto, A.; Lorenzon, L.; Ercolani, C.; Di Agostino, S.; Cambria, A.M.; Germoni, S.; et al. miR-204 targets Bcl-2 expression and enhances responsiveness of gastric cancer. Cell Death Dis. 2012, 3, e423. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Zhang, M.Y.; Zhong, M.; Zhang, Y.Y.; Lv, K. MicroRNA-204, a direct negative regulator of ezrin gene expression, inhibits glioma cell migration and invasion. Mol. Cell. Biochem. 2014, 396, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.B.; Yin, Y.; Hu, Y.L.; Zhang, J.W.; Bian, Z.H.; Song, M.X.; Hua, D.; Huang, Z.H. MicroRNA-204-5p inhibits gastric cancer cell proliferation by downregulating USP47 and RAB22A. Med. Oncol. 2015, 32, 331. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.H.; Wang, X.Q.; Chen, P.S. MiR-204 down regulates SIRT1 and reverts SIRT1-induced epithelial-mesenchymal transition, anoikis resistance and invasion in gastric cancer cells. BMC Cancer 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Li, L.; Su, J.; Zhang, G. Decreased miR-204 in H. pylori-Associated Gastric Cancer Promotes Cancer Cell Proliferation and Invasion by Targeting SOX4. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Nunes, P.B.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohns Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef] [Green Version]
- Fakhoury, M.; Negrulj, R.; Mooranian, A.; Al-Salami, H. Inflammatory bowel disease: Clinical aspects and treatments. J. Inflamm. Res. 2014, 7, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Shivashankar, R.; Tremaine, W.; Harmsen, S.; Zinsmeister, A.; Loftus, E. Updated Incidence and Prevalence of Crohn’s Disease and Ulcerative Colitis in Olmsted County, Minnesota (1970–2010). Am. J. Gastroenterol. 2014, 109, 499. [Google Scholar] [CrossRef]
- Palmieri, O.; Creanza, T.M.; Bossa, F.; Latiano, T.; Corritore, G.; Palumbo, O.; Martino, G.; Biscaglia, G.; Scimeca, D.; Carella, M.; et al. Functional Implications of MicroRNAs in Crohn’s Disease Revealed by Integrating MicroRNA and Messenger RNA Expression Profiling. Int. J. Mol. Sci. 2017, 18, 1580. [Google Scholar] [CrossRef] [Green Version]
- Tian, Y.H.; Ma, X.H.; Lv, C.; Sheng, X.L.; Li, X.; Zhao, R.; Song, Y.L.; Andl, T.; Plikus, M.V.; Sun, J.Y.; et al. Stress responsive miR-31 is a major modulator of mouse intestinal stem cells during regeneration and tumorigenesis. Elife 2017, 6, e29538. [Google Scholar] [CrossRef]
- Strillacci, A.; Valerii, M.C.; Sansone, P.; Caggiano, C.; Sgromo, A.; Vittori, L.; Fiorentino, M.; Poggioli, G.; Rizzello, F.; Campieri, M.; et al. Loss of miR-101 expression promotes Wnt/β-catenin signalling pathway activation and malignancy in colon cancer cells. J. Pathol. 2013, 229, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Yu, W.; Han, X. Overexpression of microRNA-101 causes anti-tumor effects by targeting CREB1 in colon cancer. Mol. Med. Rep. 2019, 19, 3159–3167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.G.; Xia, Y.J.; Cui, Y. Upregulation of miR-101 enhances the cytotoxic effect of anticancer drugs through inhibition of colon cancer cell proliferation. Oncol. Rep. 2017, 38, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, X.; Xu, W.; Lu, T.; Zhou, J.; Ge, X.; Hua, D. MicroRNA-142-3p Promotes Cellular Invasion of Colorectal Cancer Cells by Activation of RAC1. Technol. Cancer Res. Treat. 2018, 17, 1533033818790508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Sun, Z.; Liu, B.; Shan, Y.J.; Zhao, L.F.; Jia, L. Tumor-suppressive miR-26a and miR-26b inhibit cell aggressiveness by regulating FUT4 in colorectal cancer. Cell Death Dis. 2017, 8, e2892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häuser, W.; Fitzcharles, M.-A. Facts and myths pertaining to fibromyalgia. Dialogues Clin. Neurosci. 2018, 20, 53–62. [Google Scholar]
- Wang, Q.; Zhu, Y. Epidemiological investigation of constitutional types of Chinese medicine in general population: Based on 21,948 epidemiological investigation data of nine provinces in China. China J. Tradit. Chin. Med. Pharm. 2009, 24, 7–12. [Google Scholar]
- Qi, Y.; Zhou, Y.; Chen, X.; Ye, L.; Zhang, Q.; Huang, F.; Cui, B.; Lin, D.; Ning, G.; Wang, W.; et al. MicroRNA-4443 Causes CD4+ T Cells Dysfunction by Targeting TNFR-Associated Factor 4 in Graves’ Disease. Front. Immunol. 2017, 8, 1440. [Google Scholar] [CrossRef] [Green Version]
- Shefler, I.; Salamon, P.; Levi-Schaffer, F.; Mor, A.; Hershko, A.Y.; Mekori, Y.A. MicroRNA-4443 regulates mast cell activation by T cell-derived microvesicles. J. Allergy Clin. Immunol. 2018, 141, 2132–2141. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- NIH—NHLBI—Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 20 December 2019).
- OCEBM Levels of Evidence Working Group. The Oxford Levels of Evidence 2. Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/index.aspx?o=5653 (accessed on 20 December 2019).



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| English literature Studies published between 2000 and 2019 Studies considering human saliva samples for miRNAs identification Studies using miRNAs as diagnostic biomarkers | Publication type: case reports, conference proceedings, personal communications, letters to editor, reviews Studies considering salivary miRNAs for diagnostic tools engineering, testing, and validation Studies on the diagnostic use of salivary miRNAs in patients with: • Pharyngeal, esophageal, and oral cavity diseases • oral manifestations of systemic disease • oral microbial infections • drug/hormone dosages • aging • psychiatric and cognitive diseases |
| Study Number | Title | Authors | Year of Publication | Disease Investigated | Number of Involved Patients | Biomarkers (miRNAs) |
|---|---|---|---|---|---|---|
| 1 [10] | MicroRNA signatures differentiate Crohn’s disease from ulcerative colitis | Schaefer et al. | 2015 | CD vs. UC | 35 HC, 42 CD, 41 UC, 5 saliva samples/group | miR-101 |
| 2 [11] | Plasma and saliva miR-21 expression in colorectal cancer patients | Sazanov et al. | 2016 | CRC | 31 peripheral blood and 34 saliva samples (CRC stages II–IV) + 34 HC | miR-21 |
| 3 [12] | miR-1246 and miR-4644 in salivary exosome as potential biomarkers for pancreatic-biliary tract cancer | Machida et al. | 2016 | PC | 12 PC and 13 HC | miR-1246 and miR-4644 |
| 4 [13] | miRNA-21 and miRNA-34a Are Potential Minimally Invasive Biomarkers for the Diagnosis of Pancreatic Ductal Adenocarcinoma | Alemar et al. | 2016 | PC | serum and saliva 24 PC + HC saliva, 10 PC, and 10 saliva HC | saliva: miR-21, -34a, -155, -200b, and -376a |
| 5 [14] | Salivary MicroRNA in Pancreatic Cancer Patients | Humeau et al. | 2015 | PC | saliva from PC (7), pancreatitis (4), IPMN (2), and HC (4) | miR-21, miR-23a, miR-23b, and miR-29c |
| 6 [15] | Salivary microRNAs Show Potential as a Non-invasive Biomarker for Detecting Resectable Pancreatic Cancer | Xie et al. | 2014 | PC | 40 PC, 20 BPT, and 40 HC | miR-940 and miR-3679-5p |
| 7 [16] | Circulating microRNA Profiles as Liquid Biopsies for the Characterization and Diagnosis of Fibromyalgia Syndrome | Masotti et al. | 2016 | FM | Blood and saliva, 14 FM, and 14 HC | miR-23a-3p, miR-346, and miR-320b |
| 8 [17] | Discovery and Validation of Salivary Extracellular RNA Biomarkers for Non-invasive Detection of Gastric Cancer | Li et al. | 2018 | GC | Saliva, 63 GC, and 31 HC | miR140-5p, miR374a, miR454 4.61, miR15b, miR28–5p, and miR301a |
| 9 [18] | MicroRNA Expression in Salivary Supernatant of Patients with Pancreatic Cancer and Its Relationship with ZHENG | Gao et al. | 2014 | PC and ZHENG | 30 PC and 32 HC | 5 miRNA candidates miR-17, miR-21, miR-181a, miR-181b, and miR-196a |
| 10 [19] | Expression of miR-204 and MMP-9 in Helicobacter pylori-associated gastric ulcer | Li et al. | 2016 | Helicobacter pylori-associated GU | Ulcer, blood, and saliva samples of 46 patients with H. pylori-associated gastritis; normal stomach mucosa, blood, and saliva in 29 HC | miRNA-204 |
| 11 [20] | miRNA Expression Profile of Saliva in Subjects of Yang Deficiency Constitution and Yin Deficiency Constitution | Chen et al. | 2018 | Constitution deficit and miRNA | Saliva from 5 balanced individuals, 5 Yin deficiencies, and 5 Yang deficiencies | 81 miRNA Yang deficiency 98 miRNA Yin deficiency |
| Study Number | Authors | Type of Saliva and Methods of Collection | Setting of Collection | Handling, Centrifugation, and Storing | Method of Analysis |
|---|---|---|---|---|---|
| 1 [10] | Schaefer et al. | Whole Unstimulated | NR | Preservation: RNAprotect® saliva reagent (Quiagen) Centrifugation: NR Storing: NR | RT-qPCR + microarray |
| 2 [11] | Sazanov et al. | Whole NR | In the morning, empty stomach, after oral rinsing with sterile water | Preservation: NR Centrifugation: 12,000 rpm, 2 min Storing: NR | RT-qPCR |
| 3 [12] | Machida et al. | Whole Unstimulated accumulation on the floor of the mouth and spit through a funnel | Collection between 7–12 am; Collection tube kept on ice at 4 °C | Preservation: NR Centrifugation: NR Storing: at 4 °C for 6 h, then at –80 °C | RT-qPCR |
| 4 [13] | Alemar et al. | Whole Unstimulated | Collection between 9–11 am; No drinking, eating, smoking, or oral hygiene for at least 1 h before collection | Preservation: RNA Oragene® RE-100 Centrifugation: NR Storing: NR | RT-qPCR |
| 5 [14] | Humeau et al. | Whole Unstimulated, collected by micro-pipette | No toothbrushing 45 min before collection | Preservation: RNAprotect® saliva reagent (Quiagen) Centrifugation: NR Storing: –80 °C | RT-qPCR |
| 6 [15] | Xie et al. | Whole Continuous citric acid solution tongue stimulation for 5 s every 30 s | No eating, drinking, smoking, or oral hygiene procedures for at least 2 h before collection | Preservation: NR Centrifugation: 3 mL centrifuged (3000× g, 15 min, 4 °C) and re-centrifugation (12,000× g, 10 min, 4 °C) Storing: –80 °C | qPCR |
| 7 [16] | Masotti et al. | Whole NR | NR | NR | qPCR |
| 8 [17] | Li et al. | Whole Unstimulated | No eating or drinking except water for 30 min collection | Preservation: SUPERase-In RNase inhibitor® Centrifugation: 5mL saliva (2600× g for 15 min at 4 °C). Storing: –80 °C | RT-qPCR |
| 9 [18] | Gao et al. | whole NR | NR | Preservation: NR Centrifugation: saliva (2500× g for 10 min at 4 °C) and supernatant centrifuged (10,000× g for 1 min) Storing: −80 °C | RT-qPCR |
| 10 [19] | Li et al. | whole Continuous 2% citric acid tongue stimulation | No eating, drinking, smoking, or oral hygiene procedures for at least 2 h before collection | NR | qPCR + microarray + ELISA |
| 11 [20] | Chen et al. | whole Swabbing for 15 min | No eating, drinking, smoking, or oral hygiene procedures for at least 2 h before collection | NR | microarray |
| Study | Disease Investigated and Location | Salivary miRNAs | Subjects | Status | Sensitivity | Specificity | Statistical Significance |
|---|---|---|---|---|---|---|---|
| 1 [10] | Intestinal bowel disease | miR-101 | CD vs. HC | overexpressed | NR | NR | p < 0.05 |
| miR-21, miR-31, miR-142-3p | UC vs. HC | overexpressed | NR | NR | p < 0.05 | ||
| miR-142-5p | UC vs. HC | underexpressed | NR | NR | p <0.05 | ||
| 2 [11] | Colon-rectal cancer | miR-21 | CRC stages II/III/IV vs. HC | overexpressed | 97% | 91% | p = 5 × 10−12 |
| 3 [12] | Pancreatic cancer | miR-1246 | PC vs. HC | overexpressed | 66,70% | 100% | p = 0.008 |
| miR-4644 | PC vs. HC | overexpressed | 75% | 76,90% | p = 0.026 | ||
| miR-1246 + miR-4644 | PC vs. HC | overexpressed | NR | NR | p = 0.005 | ||
| 4 [13] | Pancreatic cancer | miR-21 | PC vs. HC | overexpressed | NR | NR | NR |
| miR-34a, miR-155, miR-200b, miR-376a | PC vs. HC | NR | NR | NR | NR | ||
| 5 [14] | Pancreatic cancer | miR-21 | PC vs. HC | overexpressed | 71% | 100% | p = 0.012 |
| miR-23a | PC vs. HC and pre-cancerous | overexpressed | 85,70% | 100% | p = 0.001 | ||
| miR-23b | PC vs. HC and pre-cancerous | overexpressed | 85,70% | 100% | p = 0.014 | ||
| miR-29c | PC vs. HC | overexpressed | 57% | 100% | p = 0.03 | ||
| miR-210 | Pancreatitis vs. HC | overexpressed | 100% | 100% | p = 0.000014 | ||
| let-7c | Pancreatitis vs. HC | overexpressed | 75% | 80% | p = 0.033 | ||
| miR-216 | PC vs. Pancreatitis | overexpressed | 50% | 100% | p = 0.024 | ||
| 6 [15] | Pancreatic cancer | miR-940 | PC vs. HC | overexpressed | 90% | 40% | p < 0.006 |
| PC vs. BPT | overexpressed | 62,50% | 75% | p < 0.004 | |||
| PC vs. HC + BPT | overexpressed | 90% | 41,70% | p < 0.001 | |||
| miR-3679-5p | PC vs. HC | underexpressed | 83% | 45% | p < 0.008 | ||
| PC vs. BPT | underexpressed | 90% | 45% | p < 0.007 | |||
| PC vs. HC + BPT | underexpressed | 85% | 45% | p < 0.002 | |||
| 7 [16] | Fibromyalgia | miR-23a-3p | FM vs. HC | NR | NR | NR | NR |
| miR-346 | NR | NR | NR | NR | |||
| miR-320b | NR | NR | NR | NR | |||
| 8 [17] | Gastric Cancer | miR140-5p | GC vs. HC | underexpressed | 75% | 83% | p < 0.05 |
| miR301a | underexpressed | ||||||
| miR374a | underexpressed | NR | NR | ||||
| miR454 | underexpressed | NR | NR | ||||
| miR15b | underexpressed | NR | NR | ||||
| miR28-5p | underexpressed | NR | NR | ||||
| 9 [18] | Pancreatic Cancer/ZHENG | miR-17 | PC vs. HC | NR | NR | NR | NR |
| miR-21 | NR | NR | NR | NR | |||
| miR-181 | NR | NR | NR | NR | |||
| miR-196a | NR | NR | NR | NR | |||
| 10 [19] | Helicobacter pylori-associated Gastric Ulcer | miRNR-204 | GU vs. HC | NR | NR | NR | p < 0.01 |
| 11 [20] | Constitution deficit/yin yang | miR-4443 | Yang deficiency constitution | underexpressed | NR | NR | NR |
| miR-2681-3p | overexpressed | NR | NR | NR | |||
| miR-4455 | Yin deficiency constitution | underexpressed | NR | NR | NR | ||
| miR-1343-3p | overexpressed | NR | NR | NR |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Setti, G.; Pezzi, M.E.; Viani, M.V.; Pertinhez, T.A.; Cassi, D.; Magnoni, C.; Bellini, P.; Musolino, A.; Vescovi, P.; Meleti, M. Salivary MicroRNA for Diagnosis of Cancer and Systemic Diseases: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 907. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21030907
Setti G, Pezzi ME, Viani MV, Pertinhez TA, Cassi D, Magnoni C, Bellini P, Musolino A, Vescovi P, Meleti M. Salivary MicroRNA for Diagnosis of Cancer and Systemic Diseases: A Systematic Review. International Journal of Molecular Sciences. 2020; 21(3):907. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21030907
Chicago/Turabian StyleSetti, Giacomo, Margherita E. Pezzi, Maria Vittoria Viani, Thelma A. Pertinhez, Diana Cassi, Cristina Magnoni, Pierantonio Bellini, Antonino Musolino, Paolo Vescovi, and Marco Meleti. 2020. "Salivary MicroRNA for Diagnosis of Cancer and Systemic Diseases: A Systematic Review" International Journal of Molecular Sciences 21, no. 3: 907. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21030907