Type 1 FSHD with 6–10 Repeated Units: Factors Underlying Severity in Index Cases and Disease Penetrance in Their Relatives Attention

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Demographic Characteristics
2.2. Age of Onset, RUs, and CSS
2.3. Comparison of Clinical Data Between the Two Groups
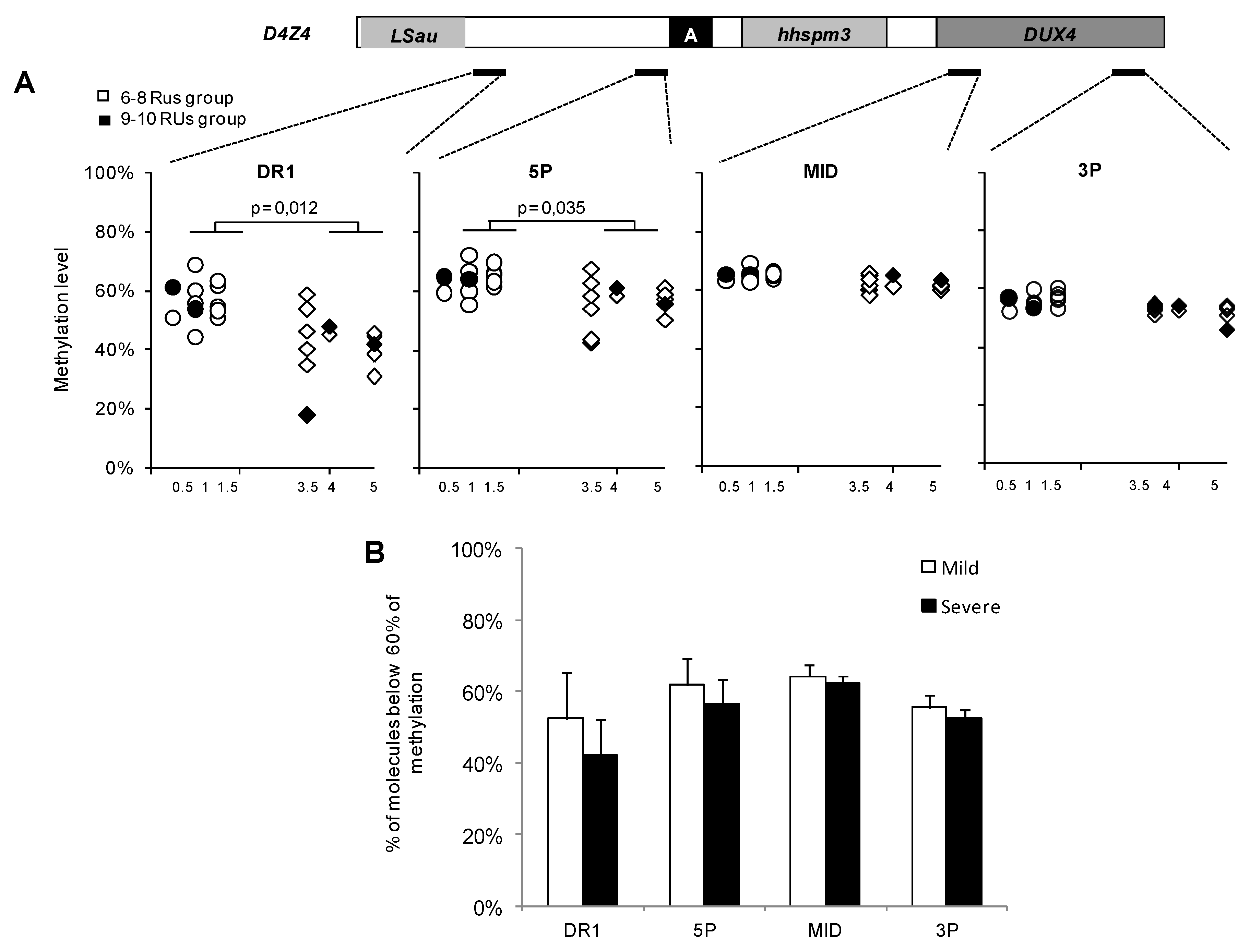
2.4. Association Between FSHD Severity DNA Methylation
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Clinical and Functional Evaluation
4.3. Genetic Testing/Methylation Profile Analysis
4.4. Statistical Analyses
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ABDUL | Left Upper Limb Abduction |
| ABDUL | Right Upper Abduction |
| ANTEL | Left Upper Limb Anterior Flexion |
| ANTER | Right Upper Limb Flexion |
| CSS | Clinical Severity Score |
| FSHD | Muscular Facioscapulohumeral Dystrophy |
| IC | Index case |
| MFM | Motor Function Measure |
| RU | Repeat Unit |
| SMMT | Mini Motor Test Sum |
References
- Lemmers, R.J.L.F.; Van Der Vliet, P.J.; Klooster, R.; Sacconi, S.; Camaño, P.; Dauwerse, J.G.; Snider, L.; Straasheijm, K.R.; Van Ommen, G.J.; Padberg, G.W.; et al. A Unifying Genetic Model for Facioscapulohumeral Muscular Dystrophy. Science 2010, 329, 1650–1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padberg, G.; Lunt, P.; Koch, M.; Fardeau, M. Diagnostic criteria for facioscapulohumeral muscular dystrophy. Neuromuscul. Disord. 1991, 1, 231–234. [Google Scholar] [CrossRef]
- Tawil, R.; Van Der Maarel, S.M.; Padberg, G.W.; Van Engelen, B. 171st ENMC International Workshop: Standards of care and management of facioscapulohumeral muscular dystrophy. Neuromuscul. Disord. 2010, 20, 471–475. [Google Scholar] [CrossRef]
- Deenen, J.C.; Arnts, H.; Van Der Maarel, S.M.; Padberg, G.W.; Verschuuren, J.J.; Bakker, E.; Weinreich, S.S.; Verbeek, A.L.; Van Engelen, B.G. Population-based incidence and prevalence of facioscapulohumeral dystrophy. Neurology 2014, 83, 1056–1059. [Google Scholar] [CrossRef] [Green Version]
- Mostacciuolo, M.; Pastorello, E.; Vazza, G.; Miorin, M.; Angelini, C.; Tomelleri, G.; Galluzzi, G.; Trevisan, C.P. Facioscapulohumeral muscular dystrophy: epidemiological and molecular study in a north-east Italian population sample. Clin. Genet. 2009, 75, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Ferri, G.; Huichalaf, C.H.; Caccia, R.; Gabellini, D. Direct interplay between two candidate genes in FSHD muscular dystrophy. Hum. Mol. Genet. 2014, 24, 1256–1266. [Google Scholar] [CrossRef] [Green Version]
- Sarfarazi, M.; Wijmenga, C.; Upadhyaya, M.; Weiffenbach, B.; Hyser, C.; Mathews, K.; Murray, J.; Gilbert, J.; Pericak-Vance, M.; Lunt, P.; et al. Regional mapping of facioscapulohumeral muscular dystrophy gene on 4q35: Combined analysis of an international consortium. Am. J. Hum. Genet. 1992, 51, 396–403. [Google Scholar]
- Feeney, S.J.; McGrath, M.J.; Sriratana, A.; Gehrig, S.M.; Lynch, G.S.; D’Arcy, C.E.; Price, J.T.; McLean, C.A.; Tupler, R.; Mitchell, C.A. FHL1 Reduces Dystrophy in Transgenic Mice Overexpressing FSHD Muscular Dystrophy Region Gene 1 (FRG1). PLoS ONE 2015, 10, e0117665. [Google Scholar] [CrossRef] [Green Version]
- Van Der Maarel, S.M.; Miller, D.; Tawil, R.; Filippova, G.N.; Tapscott, S.J. Facioscapulohumeral muscular dystrophy: consequences of chromatin relaxation. Curr. Opin. Neurol. 2012, 25, 614–620. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, M.; Lacey, M. Deciphering transcription dysregulation in FSH muscular dystrophy. J. Hum. Genet. 2012, 57, 477–484. [Google Scholar] [CrossRef]
- Statland, J.M.; Donlin-Smith, C.M.; Tapscott, S.J.; Lemmers, R.J.L.F.; van der Maarel, S.M.; Tawil, R. Milder phenotype in facioscapulohumeral dystrophy with 7–10 residual D4Z4 repeats. Neurology 2015, 85, 2147–2150. [Google Scholar]
- Ricci, G.; Scionti, I.; Sera, F.; Govi, M.; D’Amico, R.; Frambolli, I.; Mele, F.; Filosto, M.; Vercelli, L.; Ruggiero, L.; et al. Large scale genotype-phenotype analyses indicate that novel prognostic tools are required for families with facioscapulohumeral muscular dystrophy. Brain 2013, 136, 3408–3417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolic, A.; Ricci, G.; Sera, F.; Bucci, E.; Govi, M.; Mele, F.; Rossi, M.; Ruggiero, L.; Vercelli, L.; Ravaglia, S.; et al. Clinical expression of facioscapulohumeral muscular dystrophy in carriers of 1–3 D4Z4 reduced alleles: experience of the FSHD Italian National Registry. BMJ Open 2016, 6, e007798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scionti, I.; Greco, F.; Ricci, G.; Govi, M.; Arashiro, P.; Vercelli, L.; Berardinelli, A.; Angelini, C.; Antonini, G.; Cao, M.; et al. Large-Scale Population Analysis Challenges the Current Criteria for the Molecular Diagnosis of Fascioscapulohumeral Muscular Dystrophy. Am. J. Hum. Genet. 2012, 90, 628–635. [Google Scholar] [CrossRef] [Green Version]
- Daxinger, L.; Tapscott, S.J.; Van Der Maarel, S.M. Genetic and epigenetic contributors to FSHD. Curr. Opin. Genet. Dev. 2015, 33, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaillard, M.-C.; Roche, S.; Dion, C.; Tasmadjian, A.; Bouget, G.; Salort-Campana, E.; Vovan, C.; Chaix, C.; Broucqsault, N.; Morère, J.; et al. Differential DNA methylation of the D4Z4 repeat in patients with FSHD and asymptomatic carriers. Neurology 2014, 83, 733–742. [Google Scholar] [CrossRef]
- Sacconi, S.; Lemmers, R.J.; Balog, J.; Van Der Vliet, P.J.; Lahaut, P.; Van Nieuwenhuizen, M.P.; Straasheijm, K.R.; Debipersad, R.D.; Vos-Versteeg, M.; Salviati, L.; et al. The FSHD2 Gene SMCHD1 Is a Modifier of Disease Severity in Families Affected by FSHD1. Am. J. Hum. Genet. 2013, 93, 744–751. [Google Scholar] [CrossRef] [Green Version]
- Emmanuelle, S.; Nguyen, K.; Bernard, R.; Jouve, E.; Solé, G.; Nadaj-Pakleza, A.; Niederhauser, J.; Charles, E.; Ollagnon, E.; Bouhour, F.; et al. Low penetrance in facioscapulohumeral muscular dystrophy type 1 with large pathological D4Z4 alleles: a cross-sectional multicenter study. Orphanet J. Rare Dis. 2015, 10, 2. [Google Scholar]
- Roche, S.; Dion, C.; Broucqsault, N.; Laberthonnière, C.; Gaillard, M.-C.; Robin, J.D.; Lagarde, A.; Puppo, F.; Vovan, C.; Chaix, C.; et al. Methylation hotspots evidenced by deep sequencing in patients with facioscapulohumeral dystrophy and mosaicism. Neurol. Genet. 2019, 5, e372. [Google Scholar] [CrossRef] [Green Version]
- Ricci, E.; Galluzzi, G.; Deidda, G.; Cacurri, S.; Colantoni, L.; Merico, B.; Piazzo, N.; Servidei, S.; Vigneti, E.; Pasceri, V.; et al. Progress in the molecular diagnosis of facioscapulohumeral muscular dystrophy and correlation between the number of KpnI repeats at the 4q35 locus and clinical phenotype. Ann. Neurol. 1999, 45, 751–757. [Google Scholar] [CrossRef]
- Tawil, R.; Forrester, J.; Griggs, R.; Mendell, J.; Kissel, J.; McDermott, M.; King, W.; Weiffenbach, B.; Figlewicz, D. The Fsh-Dy Group Evidence for anticipation and association of deletion size with severity in facioscapulohumerd muscular dystrophy. Ann. Neurol. 1996, 39, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Lunt, P.W.; Jardine, P.E.; Koch, M.; Maynard, J.; Osborn, M.; Williams, M.; Harper, P.S.; Upadhyaya, M. Phenotypic-genotypic correlation will assist genetic counseling in 4q35-facioscapulohumeral muscular dystrophy. Muscle Nerve 1995, 18, S103–S109. [Google Scholar] [CrossRef]
- Goto, K.; Lee, J.; Matsuda, C.; Hirabayashi, K.; Kojo, T.; Nakamura, A.; Mitsunaga, Y.; Furukawa, T.; Sahashi, K.; Arahata, K. DNA rearrangements in Japanese facioscapulohumeral muscular dystrophy patients: clinical correlations. Neuromuscul. Disord. 1995, 5, 201–208. [Google Scholar] [CrossRef]
- Brouwer, O.F.; Padberg, G.W.; Wijmenga, C.; Frants, R.R. Facioscapulohumeral Muscular Dystrophy in Early Childhood. Arch. Neurol. 1994, 51, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Sakellariou, P.; Kekou, K.; Fryssira, H.; Sofocleous, C.; Manta, P.; Panousopoulou, A.; Gounaris, K.; Kanavakis, E. Mutation spectrum and phenotypic manifestation in FSHD Greek patients. Neuromuscul. Disord. 2012, 22, 339–349. [Google Scholar] [CrossRef]
- Rudnik-Schöneborn, S.; Weis, J.; Kress, W.; Häusler, M.; Zerres, K. Becker’s muscular dystrophy aggravating facioscapulohumeral muscular dystrophy–double trouble as an explanation for an atypical phenotype. Neuromuscul. Disord. 2008, 18, 881–885. [Google Scholar] [CrossRef]
- Korngut, L.; Siu, V.M.; Venance, S.L.; Levin, S.; Ray, P.; Lemmers, R.J.; Keith, J.; Campbell, C. Phenotype of combined Duchenne and facioscapulohumeral muscular dystrophy. Neuromuscul. Disord. 2008, 18, 579–582. [Google Scholar] [CrossRef]
- Lin, F.; Wang, Z.-Q.; Lin, M.-T.; Murong, S.-X.; Wang, N. New Insights into Genotype-phenotype Correlations in Chinese Facioscapulohumeral Muscular Dystrophy: A Retrospective Analysis of 178 Patients. Chin. Med. J. 2015, 128, 1707–1713. [Google Scholar] [CrossRef]
- Dion, C.; Roche, S.; Laberthonnière, C.; Broucqsault, N.; Mariot, V.; Xue, S.; Gurzau, A.D.; Nowak, A.; Gordon, C.T.; Gaillard, M.-C.; et al. SMCHD1 is involved in de novo methylation of the DUX4-encoding D4Z4 macrosatellite. Nucleic Acids Res. 2019, 47, 2822–2839. [Google Scholar] [CrossRef] [Green Version]
- Jansz, N.; Chen, K.; Murphy, J.M.; Blewitt, M.E. The Epigenetic Regulator SMCHD1 in Development and Disease. Trends Genet. 2017, 33, 233–243. [Google Scholar] [CrossRef]
- Lemmers, R.J.; Goeman, J.J.; Van Der Vliet, P.J.; Van Nieuwenhuizen, M.P.; Balog, J.; Vos-Versteeg, M.; Camaño, P.; Arroyo, M.A.R.; Jerico, I.; Rogers, M.T.; et al. Inter-individual differences in CpG methylation at D4Z4 correlate with clinical variability in FSHD1 and FSHD2. Hum. Mol. Genet. 2014, 24, 659–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Greef, J.C.; Frants, R.R.; Van Der Maarel, S.M. Epigenetic mechanisms of facioscapulohumeral muscular dystrophy. Mutat. Res. Mol. Mech. Mutagen. 2008, 647, 94–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bérard, C.; Payan, C.; Hodgkinson, I.; Fermanian, J. A motor function measure for neuromuscular diseases. Construction and validation study. Neuromuscul. Disord. 2005, 15. [Google Scholar] [CrossRef] [PubMed]
- Brooke, M.H.; Griggs, R.; Mendell, J.R.; Fenichel, G.M.; Shumate, J.B.; Pellegrino, R.J. Clinical trial in duchenne dystrophy. I. The design of the protocol. Muscle Nerve 1981, 4, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Vignos, P.J., Jr.; Archibald, K.C. Maintenance of ambulation in childhood muscular dystrophy. J. Chronic Dis. 1960, 12, 273–290. [Google Scholar] [CrossRef]
- Hartweck, L.M.; Anderson, L.J.; Lemmers, R.J.; Dandapat, A.; Toso, E.A.; Dalton, J.C.; Tawil, R.; Day, J.W.; Van Der Maarel, S.M.; Kyba, M. A focal domain of extreme demethylation within D4Z4 in FSHD2. Neurology 2013, 80, 392–399. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| 6–8 RUs (n = 74) | 9–10 RUs (n = 25) | Z | p | |
|---|---|---|---|---|
| Adjusted SMMT | 0.67 (0.32–1.07) | 0.52 (0.28–0.99) | −0.38 | 0.70 |
| CSS | 2.5 (1.4–3.5) | 2.5 (1.0–3.3) | −0.51 | 0.61 |
| Brooke | 2 (1–3) | 2 (1–2.75) | −0.09 | 0.93 |
| Gardner | 2 (0–3) | 1 (0–2) | −1.37 | 0.17 |
| Brooke/Gardner sum-score | 4 (2–5) | 3 (2–4) | −1.2 | 0.23 |
| MFM score | 92.5 (81.5–99) | 95.5 (86.25–98) | −0.56 | 0.58 |
| Time to Walk 10 m | 7 (6–11) | 8 (6–9.75) | −0.34 | 0.74 |
| Time to climb 4 steps | 3 (2–5) | 3.5 (2–7) | −023 | 0.82 |
| Time of Barré (s) | 60 (30–143) | 92 (30–150) | −99 | 0.32 |
| Time of Mingazzini (s) | 60 (26.25–124.75) | 75 (60–132) | −1.6 | 0.12 |
| ABDUR | 90 (80–180) | 120 (80–180) | −0.64 | 0.52 |
| ABDUL | 90 (80–180) | 170 (75–180) | −0.41 | 0.68 |
| ANTER | 110 (88.75–180) | 120 (75–180) | −0.12 | 0.92 |
| ANTEL | 110 (90–180) | 170 (75–180) | −0.47 | 0.64 |
| Percentage of Methylation | Percentage of Hypomethylation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| DR1 | 5P | Mid | 3P | DR1 | 5P | Mid | 3P | ||
| SMMT | r | −0.31 | −0.26 | −0.35 | −0.33 | 0.27 | 0.31 | 0.21 | 0.30 |
| p | 0.12 | 0.12 | 0.08 | 0.10 | 0.18 | 0.12 | 0.30 | 0.14 | |
| CSS | r | −0.47 | −.042 | −0.51 | −0.43 | 0.42 | 0.31 | 0.23 | 0.29 |
| p | 0.01 | 0.03 | 0.01 | 0.03 | 0.03 | 0.12 | 0.26 | 0.14 | |
| Brooke | r | −0.22 | −0.15 | −0.21 | −0.12 | 0.15 | 0.09 | −0.06 | 0 |
| p | 0.26 | 0.45 | 0.29 | 0.55 | 0.45 | 0.65 | 0.78 | 0.99 | |
| Gardner | r | −0.37 | −0.29 | −0.37 | −0.34 | 0.33 | 0.18 | 0.17 | 0.2 |
| p | 0.06 | 0.15 | 0.06 | 0.08 | 0.09 | 0.38 | 0.39 | 0.31 | |
| Time to Walk 10 m | r | −0.04 | 0.1 | −0.16 | −0.1 | −0.07 | −0.08 | 0.17 | 0.09 |
| p | 0.86 | 0.63 | 0.42 | 0.63 | 0.74 | 0.7 | 0.4 | 0.67 | |
| Time to climb 4 steps | r | −0.04 | 0.08 | −0.03 | −0.02 | −0.08 | 0 | 0.3 | 0.23 |
| p | 0.86 | 0.71 | 0.89 | 0.93 | 0.72 | 0.99 | 0.15 | 0.27 | |
| Time of Barré | r | 0.48 | 0.46 | 0.5 | 0.39 | −0.52 | −0.08 | −0.33 | −0.01 |
| p | 0.01 | 0.02 | 0.01 | 0.05 | 0.01 | 0.7 | 0.1 | 0.95 | |
| Time of Mingazzini | r | 0.19 | 0.17 | 0.17 | 0.17 | −0.22 | −0.26 | −0.22 | −0.07 |
| p | 0.39 | 0.44 | 0.44 | 0.44 | 0.31 | 0.23 | 0.32 | 0.74 | |
| ABDUR | r | 0.01 | 0 | 0.05 | 0.13 | 0.04 | 0.03 | 0.15 | 0.02 |
| p | 0.95 | 0.99 | 0.8 | 0.54 | 0.86 | 0.89 | 0.48 | 0.92 | |
| ABDUL | r | 0.06 | 0.08 | 0.06 | 0.24 | −0.09 | −0.14 | −0.04 | −0.28 |
| p | 0.78 | 0.7 | 0.75 | 0.25 | 0.66 | 0.48 | 0.86 | 0.16 | |
| ANTER | r | 0.12 | 0.09 | 0.15 | 0.3 | −0.06 | −0.01 | 0 | −0.19 |
| p | 0.57 | 0.66 | 0.47 | 0.14 | 0.76 | 0.97 | 0.99 | 0.36 | |
| ANTEL | r | 0.14 | 0.13 | 0.12 | 0.34 | −0.14 | −0.16 | −0.18 | −0.47 |
| p | 0.51 | 0.54 | 0.54 | 0.09 | 0.48 | 0.44 | 0.38 | 0.02 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salort-Campana, E.; Fatehi, F.; Beloribi-Djefaflia, S.; Roche, S.; Nguyen, K.; Bernard, R.; Cintas, P.; Solé, G.; Bouhour, F.; Ollagnon, E.; et al. Type 1 FSHD with 6–10 Repeated Units: Factors Underlying Severity in Index Cases and Disease Penetrance in Their Relatives Attention. Int. J. Mol. Sci. 2020, 21, 2221. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21062221
Salort-Campana E, Fatehi F, Beloribi-Djefaflia S, Roche S, Nguyen K, Bernard R, Cintas P, Solé G, Bouhour F, Ollagnon E, et al. Type 1 FSHD with 6–10 Repeated Units: Factors Underlying Severity in Index Cases and Disease Penetrance in Their Relatives Attention. International Journal of Molecular Sciences. 2020; 21(6):2221. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21062221
Chicago/Turabian StyleSalort-Campana, Emmanuelle, Farzad Fatehi, Sadia Beloribi-Djefaflia, Stéphane Roche, Karine Nguyen, Rafaelle Bernard, Pascal Cintas, Guilhem Solé, Françoise Bouhour, Elisabeth Ollagnon, and et al. 2020. "Type 1 FSHD with 6–10 Repeated Units: Factors Underlying Severity in Index Cases and Disease Penetrance in Their Relatives Attention" International Journal of Molecular Sciences 21, no. 6: 2221. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21062221