Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Pathophysiology and Clinical Implications

 , , and
, , and
Abstract
:1. Fragile X Syndrome and Associated Disorders
2. Epidemiology of FXTAS
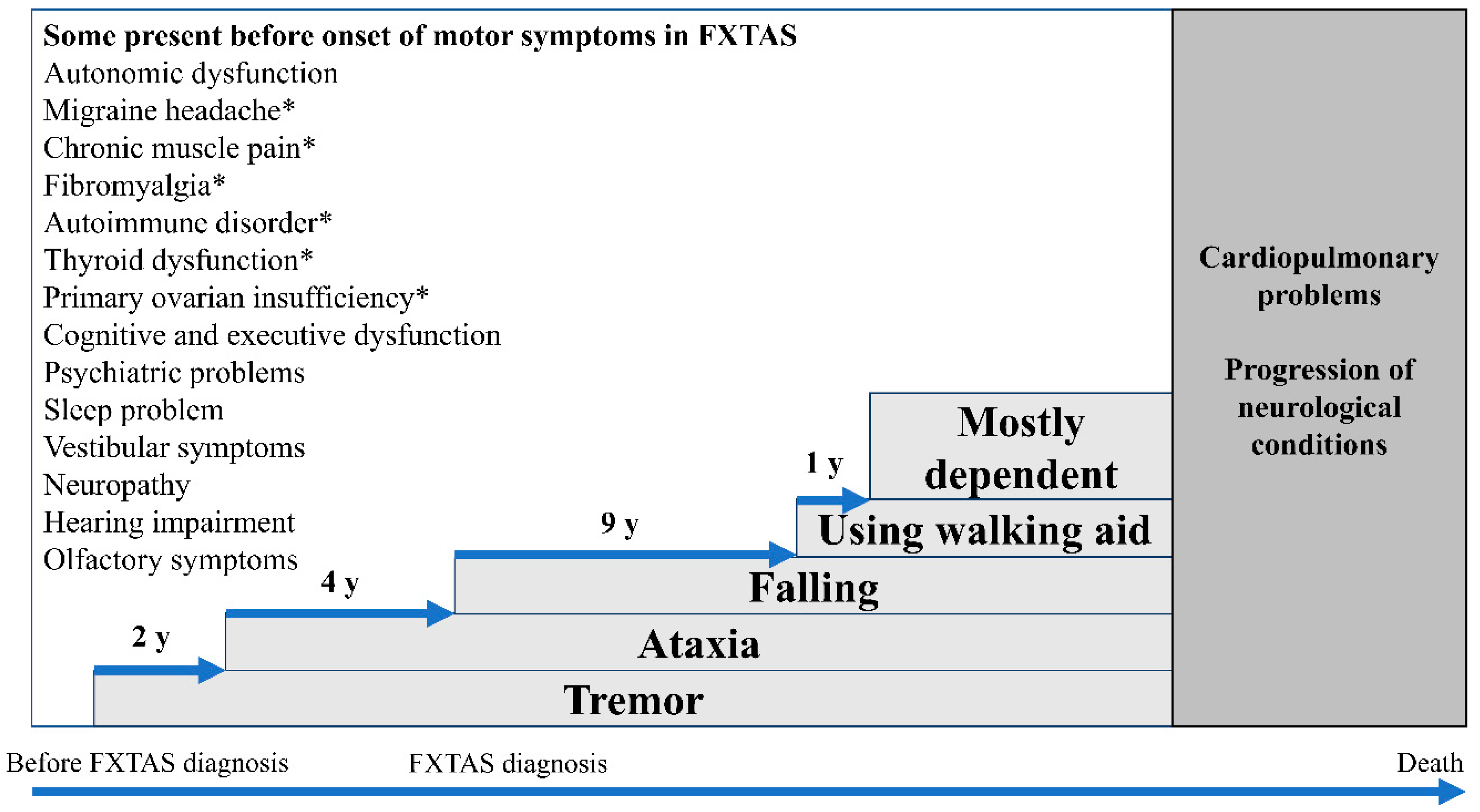
3. Clinical Presentation of FXTAS
3.1. Tremor
3.2. Cerebellar Gait Ataxia
3.3. Neuropathy
3.4. Parkinsonism
3.5. Eye Gaze Abnormalities
3.6. Cognitive Impairment
3.7. Other Coexisting Conditions
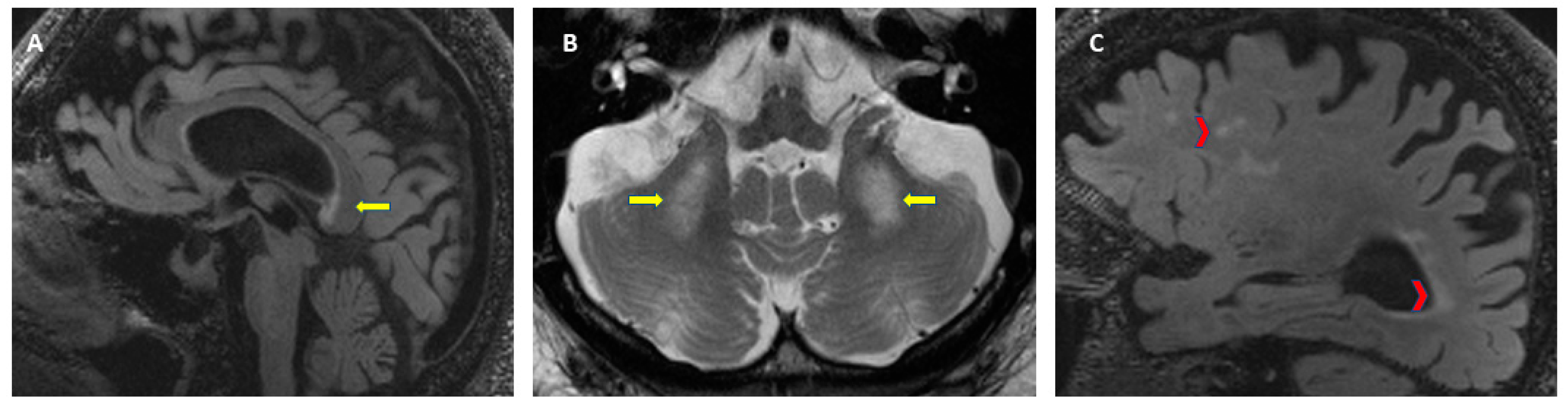
4. Neuroradiological Findings
5. Pathophysiology
5.1. Molecular Mechanisms
5.2. Pathology
6. Diagnosis
6.1. Diagnostic Criteria for FXTAS
6.2. Differential Diagnosis
7. Management and Ongoing Research
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| ASFMR1-TV2 | antisense FMR1 transcript/splice variant 2 |
| DGCR8 | DiGeorge Syndrome Critical Region 8 |
| FM | Full mutation |
| FMR1 | Fragile X Mental Retardation 1 gene |
| FMRP | Fragile X Mental Retardation Protein |
| FXAND | Fragile X-associated neuropsychiatric disorders |
| FXPOI | Fragile X-associated primary ovarian insufficiency |
| FXTAS | Fragile-X-associated tremor/ataxia syndrome |
| FXS | Fragile X syndrome |
| hnRNP A2/B1 | heterogeneous nuclear ribonucleoproteins A2/B1 |
| HP1 | heterochromatin protein 1 |
| LAP2β | Lamina-associated polypeptide 2 beta |
| MCP | Middle Cerebellar Peduncles |
| MRI | Magnetic Resonance Images |
| PD | Parkinson’s disease |
| PM | Premutation |
| PSP | Progressive supranuclear palsy |
| Purα | Pur-alpha |
| RANT | Repeat associated non-AUG translation |
References
- Hagerman, R.J.; Berry-Kravis, E.; Hazlett, H.C.; Bailey, D.B.; Moine, H.; Kooy, R.F.; Tassone, F.; Gantois, I.; Sonenberg, N.; Mandel, J.L.; et al. Fragile X syndrome. Nat. Rev. Dis. Primers 2017, 3, 17065. [Google Scholar] [CrossRef]
- Quartier, A.; Poquet, H.; Gilbert-Dussardier, B.; Rossi, M.; Casteleyn, A.S.; Des Portes, V.; Feger, C.; Nourisson, E.; Kuentz, P.; Redin, C.; et al. Intragenic FMR1 disease-causing variants: A significant mutational mechanism leading to Fragile-X syndrome. Eur. J. Hum. Genet. 2017, 25, 423–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myrick, L.K.; Nakamoto-Kinoshita, M.; Lindor, N.M.; Kirmani, S.; Cheng, X.; Warren, S.T. Fragile X syndrome due to a missense mutation. Eur. J. Hum. Genet. 2014, 22, 1185–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidorov, M.S.; Auerbach, B.D.; Bear, M.F. Fragile X mental retardation protein and synaptic plasticity. Mol. Brain 2013, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, K.M.; Gallagher, S.M.; Warren, S.T.; Bear, M.F. Altered synaptic plasticity in a mouse model of fragile X mental retardation. Proc. Natl. Acad. Sci. USA 2002, 99, 7746–7750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunamura, N.; Iwashita, S.; Enomoto, K.; Kadoshima, T.; Isono, F. Loss of the fragile X mental retardation protein causes aberrant differentiation in human neural progenitor cells. Sci. Rep. 2018, 8, 11585. [Google Scholar] [CrossRef] [Green Version]
- Monaghan, K.G.; Lyon, E.; Spector, E.B. ACMG standards and guidelines for fragile X testing: A revision to the disease-specific supplements to the standards and guidelines for Clinical Genetics Laboratories of the American College of Medical Genetics and Genomics. Genet. Med. 2013, 15, 575–586. [Google Scholar] [CrossRef] [Green Version]
- Sherman, S.; Allen, E.G.; Jesica, S. Clinical manifestation and management of FXPOI. In FXTAS, FXPOI, and Other Premutation Disorders; Tassone, F., Hall, D.A., Eds.; Springer Nature: Basel, Switzerland, 2016; pp. 199–224. ISBN 978-3-319-33896-5. [Google Scholar]
- Hagerman, R.J.; Protic, D.; Rajaratnam, A.; Salcedo-Arellano, M.J.; Aydin, E.Y.; Schneider, A. Fragile X-Associated Neuropsychiatric Disorders (FXAND). Front. Psychiatry 2018, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Salcedo-Arellano, M.J.; Hagerman, R.J.; Martinez-Cerdeno, V. Fragile X associated tremor/ataxia syndrome: Its clinical presentation, pathology, and treatment TT—Sindrome de temblor y ataxia asociado al X fragil: Presentacion clinica, patologia y tratamiento. Rev. Neurol. 2019, 68, 199–206. [Google Scholar]
- Hagerman, R.J.; Leehey, M.; Heinrichs, W.; Tassone, F.; Wilson, R.; Hills, J.; Grigsby, J.; Gage, B.; Hagerman, P.J. Intention tremor, parkinsonism, and generalized brain atrophy in male carriers of fragile X. Neurology 2001, 57, 127–130. [Google Scholar] [CrossRef]
- Hagerman, R.J.; Hagerman, P. Fragile X-associated tremor/ataxia syndrome—Features, mechanisms and management. Nat. Rev. Neurol. 2016, 12, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Winarni, T.; Zhang, L.; Tassone, F.; Hagerman, R.J. Fragile X-associated tremor/ataxia syndrome (FXTAS) in grey zone carriers. Clin. Genet. 2013, 84, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, D.; Tassone, F.; Klepitskaya, O.; Leehey, M. Fragile X–associated tremor ataxia syndrome in FMR1 gray zone allele carriers. Mov. Disord. 2012, 27, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Santa María, L.; Pugin, A.; Alliende, M.A.; Aliaga, S.; Curotto, B.; Aravena, T.; Tang, H.-T.; Mendoza-Morales, G.; Hagerman, R.; Tassone, F. FXTAS in an unmethylated mosaic male with fragile X syndrome from Chile. Clin. Genet. 2014, 86, 378–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loesch, D.Z.; Sherwell, S.; Kinsella, G.; Tassone, F.; Taylor, A.; Amor, D.; Sung, S.; Evans, A. Fragile X-associated tremor/ataxia phenotype in a male carrier of unmethylated full mutation in the FMR1 gene. Clin. Genet. 2012, 82, 88–92. [Google Scholar] [CrossRef]
- Pretto, D.I.; Hunsaker, M.R.; Cunningham, C.L.; Greco, C.M.; Hagerman, R.J.; Noctor, S.C.; Hall, D.A.; Hagerman, P.J.; Tassone, F. Intranuclear inclusions in a fragile X mosaic male. Transl. Neurodegener. 2013, 2, 10. [Google Scholar] [CrossRef] [Green Version]
- Jacquemont, S.; Hagerman, R.J.; Leehey, M.; Grigsby, J.; Zhang, L.; Brunberg, J.A.; Greco, C.; Des Portes, V.; Jardini, T.; Levine, R.; et al. Fragile X premutation tremor/ataxia syndrome: Molecular, clinical, and neuroimaging correlates. Am. J. Hum. Genet. 2003, 72, 869–878. [Google Scholar] [CrossRef] [Green Version]
- Hunter, J.; Rivero-Arias, O.; Angelov, A.; Kim, E.; Fotheringham, I.; Leal, J. Epidemiology of fragile X syndrome: A systematic review and meta-analysis. Am. J. Med. Genet. Part A 2014, 164, 1648–1658. [Google Scholar] [CrossRef]
- Saldarriaga, W.; Forero-Forero, J.V.; González-Teshima, L.Y.; Fandiño-Losada, A.; Isaza, C.; Tovar-Cuevas, J.R.; Silva, M.; Choudhary, N.S.; Tang, H.T.; Aguilar-Gaxiola, S.; et al. Genetic cluster of fragile X syndrome in a Colombian district. J. Hum. Genet. 2018, 63, 509–516. [Google Scholar] [CrossRef]
- Otsuka, S.; Sakamoto, Y.; Siomi, H.; Itakura, M.; Yamamoto, K.; Matumoto, H.; Sasaki, T.; Kato, N.; Nanba, E. Fragile X carrier screening and FMR1 allele distribution in the Japanese population. Brain Dev. 2010, 32, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Jacquemont, S.; Hagerman, R.J.; Leehey, M.A.; Hall, D.A.; Levine, R.A.; Brunberg, J.A.; Jardini, T.; Gane, L.W.; Harris, S.W.; Herman, K.; et al. Penetrance of the Fragile X—Associated Tremor / Ataxia Syndrome in a Premutation Carrier Population. JAMA 2004, 291, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, D.; Mailick, M. The epidemiology of FXTAS. In FXTAS, FXPOI, and Other Premutation Disorders; Tassone, F., Ed.; Springer Nature: Basel, Switzerland, 2016; p. 25. ISBN 978-3-319-33898-9. [Google Scholar]
- Brussino, A.; Gellera, C.; Saluto, A.; Mariotti, C.; Arduino, C.; Castellotti, B.; Camerlingo, M.; de Angelis, V.; Orsi, L.; Tosca, P.; et al. FMR1 gene premutation is a frequent genetic cause of late-onset sporadic cerebellar ataxia. Neurology 2005, 64, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Van Esch, H.; Dom, R.; Bex, D.; Salden, I.; Caeckebeke, J.; Wibail, A.; Borghgraef, M.; Legius, E.; Fryns, J.-P.; Matthijs, G. Screening for FMR-1 premutations in 122 older Flemish males presenting with ataxia. Eur. J. Hum. Genet. 2005, 13, 121–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, S.A.; Steenblock, K.J.; Thibodeau, S.N.; Lindor, N.M. Premutations in the FMR1 Gene Are Uncommon in Men Undergoing Genetic Testing for Spinocerebellar Ataxia. J. Neurogenet. 2008, 22, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Biancalana, V.; Toft, M.; Le Ber, I.; Tison, F.; Scherrer, E.; Thibodeau, S.; Mandel, J.L.; Brice, A.; Farrer, M.J.; Dürr, A. FMR1 Premutations Associated With Fragile X–Associated Tremor/Ataxia Syndrome in Multiple System Atrophy. Arch. Neurol. 2005, 62, 962–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garland, E.M.; Vnencak-Jones, C.L.; Biaggioni, I.; Davis, T.L.; Montine, T.J.; Robertson, D. Fragile X gene premutation in multiple system atrophy. J. Neurol. Sci. 2004, 227, 115–118. [Google Scholar] [CrossRef]
- Yabe, I.; Soma, H.; Takei, A.; Fujik, N.; Sasaki, H. No association between FMR1 premutations and multiple system atrophy. J. Neurol. 2004, 251, 1411–1412. [Google Scholar] [CrossRef]
- Kraff, J.; Tang, H.-T.; Cilia, R.; Canesi, M.; Pezzoli, G.; Goldwurm, S.; Hagerman, P.J.; Tassone, F. Screen for Excess FMR1 Premutation Alleles Among Males With Parkinsonism. Arch. Neurol. 2007, 64, 1002–1006. [Google Scholar] [CrossRef] [Green Version]
- Cilia, R.; Kraff, J.; Canesi, M.; Pezzoli, G.; Goldwurm, S.; Amiri, K.; Tang, H.-T.; Pan, R.; Hagerman, P.J.; Tassone, F. Screening for the Presence of FMR1 Premutation Alleles in Women With Parkinsonism. Arch. Neurol. 2009, 66, 244–249. [Google Scholar] [CrossRef] [Green Version]
- Hall, D.A.; Berry-Kravis, E.; Zhang, W.; Tassone, F.; Spector, E.; Zerbe, G.; Hagerman, P.J.; Ouyang, B.; Leehey, M.A. FMR1 gray-zone alleles: Association with Parkinson’s disease in women? Mov. Disord. 2011, 26, 1900–1906. [Google Scholar] [CrossRef] [Green Version]
- Garcia Arocena, D.; Louis, E.D.; Tassone, F.; Gilliam, T.C.; Ottman, R.; Jacquemont, S.; Hagerman, P.J. Screen for expanded FMR1 alleles in patients with essential tremor. Mov. Disord. 2004, 19, 930–933. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Jang, W.; Youn, J.; Ki, C.-S.; Kim, B.J.; Kim, H.-T.; Louis, E.D.; Cho, J.W. Prevalence of fragile X-associated tremor/ataxia syndrome: A survey of essential tremor patients with cerebellar signs or extrapyramidal signs. Brain Behav. 2019, 9, e01337. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.N.; Ye, X.; Liu, X.; Louis, E.D. Genetic analysis of FMR1 repeat expansion in essential tremor. Neurosci. Lett. 2015, 593, 114–117. [Google Scholar] [CrossRef] [Green Version]
- Hall, D.A.; O’Keefe, J.A. Fragile x-associated tremor ataxia syndrome: The expanding clinical picture, pathophysiology, epidemiology, and update on treatment. Tremor Other Hyperkinetic Mov. 2012, 2, 2. [Google Scholar]
- Hall, D.A.; Berry-Kravis, E.; Jacquemont, S.; Rice, C.D.; Cogswell, J.; Zhang, L.; Hagerman, R.J.; Hagerman, P.J.; Leehey, M.A. Initial diagnoses given to persons with the fragile X associated tremor/ataxia syndrome (FXTAS). Neurology 2005, 65, 299–301. [Google Scholar] [CrossRef]
- Grigsby, J. The fragile X mental retardation 1 gene (FMR1): Historical perspective, phenotypes, mechanism, pathology, and epidemiology. Clin. Neuropsychol. 2016, 30, 815–833. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Revenga, L.; Madrigal, I.; Pagonabarraga, J.; Xunclà, M.; Badenas, C.; Kulisevsky, J.; Gomez, B.; Milà, M. Penetrance of FMR1 premutation associated pathologies in fragile X syndrome families. Eur. J. Hum. Genet. 2009, 17, 1359–1362. [Google Scholar] [CrossRef] [Green Version]
- Leehey, M.A.; Berry-Kravis, E.; Goetz, C.G.; Zhang, L.; Hall, D.A.; Li, L.; Rice, C.D.; Lara, R.; Cogswell, J.; Reynolds, A.; et al. FMR1 CGG repeat length predicts motor dysfunction in premutation carriers. Neurology 2008, 70, 1397–1402. [Google Scholar] [CrossRef]
- Tassone, F.; Adams, J.; Berry-Kravis, E.M.; Cohen, S.S.; Brusco, A.; Leehey, M.A.; Li, L.; Hagerman, R.J.; Hagerman, P.J. CGG repeat length correlates with age of onset of motor signs of the fragile X-associated tremor/ataxia syndrome (FXTAS). Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2007, 144, 566–569. [Google Scholar] [CrossRef]
- Leehey, M.A.; Berry-Kravis, E.; Min, S.-J.; Hall, D.A.; Rice, C.D.; Zhang, L.; Grigsby, J.; Greco, C.M.; Reynolds, A.; Lara, R.; et al. Progression of tremor and ataxia in male carriers of the FMR1 premutation. Mov. Disord. 2007, 22, 203–206. [Google Scholar] [CrossRef]
- Paul, R.; Pessah, I.N.; Gane, L.; Ono, M.; Hagerman, P.J.; Brunberg, J.A.; Tassone, F.; Bourgeois, J.A.; Adams, P.E.; Nguyen, D.V.; et al. Early onset of neurological symptoms in fragile X premutation carriers exposed to neurotoxins. Neurotoxicology 2010, 31, 399–402. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Cerdeño, V.; Lechpammer, M.; Lott, A.; Schneider, A.; Hagerman, R. Fragile X-associated tremor/ataxia syndrome in a man in his 30s. JAMA Neurol. 2015, 72, 1070–1073. [Google Scholar] [CrossRef] [PubMed]
- Muzar, Z.; Adams, P.E.; Schneider, A.; Hagerman, R.J.; Lozano, R. Addictive substances may induce a rapid neurological deterioration in fragile X-associated tremor ataxia syndrome: A report of two cases. Intractable Rare Dis. Res. 2014, 3, 162–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saldarriaga, W.; Salcedo-Arellano, M.J.; Rodriguez-Guerrero, T.; Ríos, M.; Fandiño-Losada, A.; Ramirez-Cheyne, J.; Lein, P.J.; Tassone, F.; Hagerman, R.J. Increased severity of fragile X spectrum disorders in the agricultural community of Ricaurte, Colombia. Int. J. Dev. Neurosci. 2019, 72, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hall, D.A.; Robertson, E.; Shelton, A.L.; Losh, M.C.; Mila, M.; Moreno, E.G.; Gomez-Anson, B.; Martínez-Cerdeño, V.; Grigsby, J.; Lozano, R.; et al. Update on the Clinical, Radiographic, and Neurobehavioral Manifestations in FXTAS and FMR1 Premutation Carriers. Cerebellum 2016, 15, 578–586. [Google Scholar] [CrossRef]
- Gokden, M.; Al-Hinti, J.T.; Harik, S.I. Peripheral nervous system pathology in fragile X tremor/ataxia syndrome (FXTAS). Neuropathology 2009, 29, 280–284. [Google Scholar] [CrossRef]
- Hagerman, P.J.; Hagerman, R.J.; Ma, L.; Herren, A.W.; Espinal, G.; Randol, J.; McLaughlin, B.; Martinez-Cerdeño, V.; Pessah, I.N.; Hagerman, R.J.; et al. Neuropathology of fragile X-associated tremor/ataxia syndrome (FXTAS). Brain 2005, 129, 243–255. [Google Scholar]
- Hamlin, A.A.; Sukharev, D.; Campos, L.; Mu, Y.; Tassone, F.; Hessl, D.; Nguyen, D.V.; Loesch, D.; Hagerman, R.J. Hypertension in FMR1 premutation males with and without fragile X-associated tremor/ataxia syndrome (FXTAS). Am. J. Med. Genet. Part A 2012, 158, 1304–1309. [Google Scholar] [CrossRef] [Green Version]
- Coffey, S.M.; Cook, K.; Tartaglia, N.; Tassone, F.; Nguyen, D.V.; Pan, R.; Bronsky, H.E.; Yuhas, J.; Borodyanskaya, M.; Grigsby, J.; et al. Expanded clinical phenotype of women with the FMR1 premutation. Am. J. Med. Genet. Part A 2008, 146, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Hamlin, A.; Liu, Y.; Nguyen, D.V.; Tassone, F.; Zhang, L.; Hagerman, R.J. Sleep apnea in fragile X premutation carriers with and without FXTAS. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2011, 156, 923–928. [Google Scholar] [CrossRef] [Green Version]
- Summers, S.M.; Cogswell, J.; Goodrich, J.E.; Mu, Y.; Nguyen, D.V.; Brass, S.D.; Hagerman, R.J. Prevalence of restless legs syndrome and sleep quality in carriers of the fragile X premutation. Clin. Genet. 2014, 86, 181–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Au, J.; Akins, R.S.; Berkowitz-Sutherland, L.; Tang, H.-T.; Chen, Y.; Boyd, A.; Tassone, F.; Nguyen, D.V.; Hagerman, R. Prevalence and risk of migraine headaches in adult fragile X premutation carriers. Clin. Genet. 2013, 84, 546–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheeler, A.C.; Bailey, D.B.; Berry-Kravis, E.; Greenberg, J.; Losh, M.; Mailick, M.; Milà, M.; Olichney, J.M.; Rodriguez-Revenga, L.; Sherman, S.; et al. Associated features in females with an FMR1 premutation. J. Neurodev. Disord. 2014, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juncos, J.L.; Lazarus, J.T.; Graves-Allen, E.; Shubeck, L.; Rusin, M.; Novak, G.; Hamilton, D.; Rohr, J.; Sherman, S.L. New clinical findings in the fragile X-associated tremor ataxia syndrome (FXTAS). Neurogenetics 2011, 12, 123–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juncos, J.L.; Lazarus, J.T.; Rohr, J.; Allen, E.G.; Shubeck, L.; Hamilton, D.; Novak, G.; Sherman, S.L. Olfactory dysfunction in fragile X tremor ataxia syndrome. Mov. Disord. 2012, 27, 1556–1559. [Google Scholar] [CrossRef] [Green Version]
- Summers, S.M.; Cogswell, J.; Goodrich, J.E.; Mu, Y.; Nguyen, D.V.; Brass, S.D.; Hagerman, R.J. Fatigue and body mass index in the Fragile X premutation carrier. Fatigue Biomed. Health Behav. 2014, 2, 64–72. [Google Scholar] [CrossRef]
- Johnston, C.; Eliez, S.; Dyer-Friedman, J.; Hessl, D.; Glaser, B.; Blasey, C.; Taylor, A.; Reiss, A. Neurobehavioral phenotype in carriers of the fragile X premutation. Am. J. Med. Genet. 2001, 103, 314–319. [Google Scholar] [CrossRef]
- Bourgeois, J.A.; Cogswell, J.B.; Hessl, D.; Zhang, L.; Ono, M.Y.; Tassone, F.; Farzin, F.; Brunberg, J.A.; Grigsby, J.; Hagerman, R.J. Cognitive, anxiety and mood disorders in the fragile X-associated tremor/ataxia syndrome. Gen. Hosp. Psychiatry 2007, 29, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, J.A.; Seritan, A.L.; Casillas, E.M.; Hessl, D.; Schneider, A.; Yang, Y.; Kaur, I.; Cogswell, J.B.; Nguyen, D.V.; Hagerman, R.J. Lifetime prevalence of mood and anxiety disorders in fragile X premutation carriers. J. Clin. Psychiatry 2011, 72, 175–182. [Google Scholar] [CrossRef] [Green Version]
- Seritan, A.; Ortigas, M.; Seritan, S.; Bourgeois, J.; Hagerman, R. Psychiatric Disorders Associated with FXTAS. Curr. Psychiatry Rev. 2013, 9, 59–64. [Google Scholar]
- Leehey, M.A.; Legg, W.; Tassone, F.; Hagerman, R. Fibromyalgia in fragile X mental retardation 1 gene premutation carriers. Rheumatology 2011, 50, 2233–2236. [Google Scholar] [CrossRef] [Green Version]
- Winarni, T.I.; Chonchaiya, W.; Sumekar, T.A.; Ashwood, P.; Morales, G.M.; Tassone, F.; Nguyen, D.V.; Faradz, S.M.H.; Van de Water, J.; Cook, K.; et al. Immune-mediated disorders among women carriers of fragile X premutation alleles. Am. J. Med. Genet. Part A 2012, 158, 2473–2481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seritan, A.L.; Kim, K.; Benjamin, I.; Seritan, I.; Hagerman, R.J. Risk Factors for Cognitive Impairment in Fragile X-Associated Tremor/Ataxia Syndrome. J. Geriatr. Psychiatry Neurol. 2016, 29, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, R.J.; Leavitt, B.R.; Farzin, F.; Jacquemont, S.; Greco, C.M.; Brunberg, J.A.; Tassone, F.; Hessl, D.; Harris, S.W.; Zhang, L.; et al. Fragile-X–Associated Tremor/Ataxia Syndrome (FXTAS) in Females with the FMR1 Premutation. Am. J. Hum. Genet. 2004, 74, 1051–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassone, F.; Greco, C.M.; Hunsaker, M.R.; Seritan, A.L.; Berman, R.F.; Gane, L.W.; Jacquemont, S.; Basuta, K.; Jin, L.-W.; Hagerman, P.J.; et al. Neuropathological, clinical and molecular pathology in female fragile X premutation carriers with and without FXTAS. Genes, Brain Behav. 2012, 11, 577–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, D.A.; Robertson-Dick, E.E.; Keefe, J.A.; Hadd, A.G.; Zhou, L.; Berry-Kravis, E. X-inactivation in the clinical phenotype of fragile X premutation carrier sisters. Neurol. Genet. 2016, 2, e45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Mora, M.I.; Rodriguez-Revenga, L.; Feliu, A.; Badenas, C.; Madrigal, I.; Milà, M. Skewed X Inactivation in Women Carrying the FMR1 Premutation and Its Relation with Fragile-X-Associated Tremor/Ataxia Syndrome. Neurodegener. Dis. 2016, 16, 290–292. [Google Scholar] [CrossRef]
- Vittal, P.; Pandya, S.; Sharp, K.; Berry-Kravis, E.; Zhou, L.; Ouyang, B.; Jackson, J.; Hall, D. ASFMR1 splice variant: A predictor of fragile X-associated tremor/ataxia syndrome. Neurol. Genet. 2018, 4, e246. [Google Scholar] [CrossRef] [Green Version]
- Ligsay, A.; El-Deeb, M.; Salcedo-Arellano, M.J.; Schloemerkemper, N.; Grayson, J.S.; Hagerman, R. General Anesthetic Use in Fragile X Spectrum Disorders. J. Neurosurg. Anesthesiol. 2019, 31, 285–290. [Google Scholar] [CrossRef]
- O’Dwyer, J.P.; Clabby, C.; Crown, J.; Barton, D.E.; Hutchinson, M. Fragile X-associated tremor/ataxia syndrome presenting in a woman after chemotherapy. Neurology 2005, 65, 331–332. [Google Scholar] [CrossRef]
- Muzar, Z.; Lozano, R.; Schneider, A.; Adams, P.E.; Faradz, S.M.H.; Tassone, F.; Hagerman, R.J. Methadone use in a male with the FMRI premutation and FXTAS. Am. J. Med. Genet. Part A 2015, 167, 1354–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Deeb, M.; Adams, P.; Schneider, A.; Salcedo-Arellano, M.J.; Tassone, F.; Hagerman, R. Fentanyl overdose in a female with the FMR1 premutation and FXTAS. J. Mol. Genet. 2018, 1, 101. [Google Scholar]
- Greco, C.M.; Berman, R.; Martin, R.; Tassone, F.; Schwartz, P.; Chang, A.; Trapp, B.D.; Iwahashi, C.; Brunberg, J.; Grigsby, J.; et al. Neuropathology of fragile X-associated tremor/ataxia syndrome (FXTAS). Brain 2006, 129, 243–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apartis, E.; Blancher, A.; Meissner, W.G.; Guyant-Maréchal, L.; Maltête, D.; De Broucker, T.; Legrand, A.-P.; Bouzenada, H.; Thanh, H.T.; Sallansonnet-Froment, M.; et al. FXTAS: New insights and the need for revised diagnostic criteria. Neurology 2012, 79, 1898–1907. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.-Q.; Yang, J.-C.; Hall, D.A.; Leehey, M.A.; Tassone, F.; Olichney, J.M.; Hagerman, R.J.; Zhang, L. Parkinsonism in fragile X-associated tremor/ataxia syndrome (FXTAS): Revisited. Parkinsonism Relat. Disord. 2014, 20, 456–459. [Google Scholar] [CrossRef] [Green Version]
- O’Keefe, J.A.; Robertson-Dick, E.E.; Hall, D.A.; Berry-Kravis, E. Gait and Functional Mobility Deficits in Fragile X-Associated Tremor/Ataxia Syndrome. Cerebellum 2016, 15, 475–482. [Google Scholar] [CrossRef]
- Hagerman, R.J.; Coffey, S.M.; Maselli, R.; Soontarapornchai, K.; Brunberg, J.A.; Leehey, M.A.; Zhang, L.; Gane, L.W.; Fenton-Farrell, G.; Tassone, F.; et al. Neuropathy as a presenting feature in fragile X-associated tremor/ataxia syndrome. Am. J. Med. Genet. Part A 2007, 143, 2256–2260. [Google Scholar] [CrossRef]
- Chanson, J.-B.; Boehm, N.; Samama, B.; Echaniz-Laguna, A.; Anheim, M. Small fiber neuropathy in a woman with fragile X-associated tremor/ataxia syndrome (FXTAS). J. Neurol. 2015, 262, 226–227. [Google Scholar] [CrossRef]
- Berry-Kravis, E.; Goetz, C.G.; Leehey, M.A.; Hagerman, R.J.; Zhang, L.; Li, L.; Nguyen, D.; Hall, D.A.; Tartaglia, N.; Cogswell, J.; et al. Neuropathic features in fragile X premutation carriers. Am. J. Med. Genet. Part A 2007, 143, 19–26. [Google Scholar] [CrossRef]
- Fraint, A.; Vittal, P.; Szewka, A.; Bernard, B.; Berry-Kravis, E.; Hall, D.A. New observations in the fragile X-associated tremor/ataxia syndrome (FXTAS) phenotype. Front. Genet. 2014, 5, 365. [Google Scholar] [CrossRef]
- Soontarapornchai, K.; Maselli, R.; Fenton-Farrell, G.; Tassone, F.; Hagerman, P.J.; Hessl, D.; Hagerman, R.J. Abnormal Nerve Conduction Features in Fragile X Premutation Carriers. Arch. Neurol. 2008, 65, 495–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunsaker, M.R.; Greco, C.M.; Tassone, F.; Berman, R.F.; Willemsen, R.; Hagerman, R.J.; Hagerman, P.J. Rare Intranuclear Inclusions in the Brains of 3 Older Adult Males With Fragile X Syndrome: Implications for the Spectrum of Fragile X-Associated Disorders. J. Neuropathol. Exp. Neurol. 2011, 70, 462–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglione, C.; Ginestroni, A.; Vella, A.; Dotti, M.T.; Della Nave, R.; Rizzo, G.; De Cristofaro, M.T.; De Stefano, N.; Piacentini, S.; Martinelli, P.; et al. MRI and SPECT of midbrain and striatal degeneration in fragile X-associated tremor/ataxia syndrome. J. Neurol. 2008, 255, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Klusek, J.; Hong, J.; Sterling, A.; Berry-Kravis, E.; Mailick, M.R. Inhibition deficits are modulated by age and CGG repeat length in carriers of the FMR1 premutation allele who are mothers of children with fragile X syndrome. Brain Cogn. 2020, 139, 105511. [Google Scholar] [CrossRef]
- Seritan, A.L.; Nguyen, D.V.; Farias, S.T.; Hinton, L.; Grigsby, J.; Bourgeois, J.A.; Hagerman, R.J. Dementia in fragile X-associated tremor/ataxia syndrome (FXTAS): Comparison with Alzheimer’s disease. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2008, 147, 1138–1144. [Google Scholar] [CrossRef] [Green Version]
- Grigsby, J.; Brega, A.G.; Jacquemont, S.; Loesch, D.Z.; Leehey, M.A.; Goodrich, G.K.; Hagerman, R.J.; Epstein, J.; Wilson, R.; Cogswell, J.B.; et al. Impairment in the cognitive functioning of men with fragile X-associated tremor/ataxia syndrome (FXTAS). J. Neurol. Sci. 2006, 248, 227–233. [Google Scholar] [CrossRef]
- Grigsby, J.; Brega, A.G.; Leehey, M.A.; Goodrich, G.K.; Jacquemont, S.; Loesch, D.Z.; Cogswell, J.B.; Epstein, J.; Wilson, R.; Jardini, T.; et al. Impairment of executive cognitive functioning in males with fragile X-associated tremor/ataxia syndrome. Mov. Disord. 2007, 22, 645–650. [Google Scholar] [CrossRef]
- Grigsby, J.; Brega, A.G.; Engle, K.; Leehey, M.A.; Hagerman, R.J.; Tassone, F.; Hessl, D.; Hagerman, P.J.; Cogswell, J.B.; Bennett, R.E.; et al. Cognitive profile of fragile X premutation carriers with and without fragile X-associated tremor/ataxia syndrome. Neuropsychology 2008, 22, 48–60. [Google Scholar] [CrossRef]
- Sévin, M.; Kutalik, Z.; Bergman, S.; Vercelletto, M.; Renou, P.; Lamy, E.; Vingerhoets, F.J.; Di Virgilio, G.; Boisseau, P.; Bezieau, S.; et al. Penetrance of marked cognitive impairment in older male carriers of the <em>FMR1</em> gene premutation. J. Med. Genet. 2009, 46, 818–824. [Google Scholar]
- Movaghar, A.; Mailick, M.; Sterling, A.; Greenberg, J.; Saha, K. Automated screening for Fragile X premutation carriers based on linguistic and cognitive computational phenotypes. Sci. Rep. 2017, 7, 2674. [Google Scholar] [CrossRef] [Green Version]
- Nayar, K.; McKinney, W.; Hogan, A.L.; Martin, G.E.; La Valle, C.; Sharp, K.; Berry-Kravis, E.; Norton, E.S.; Gordon, P.C.; Losh, M. Language processing skills linked to FMR1 variation: A study of gaze-language coordination during rapid automatized naming among women with the FMR1 premutation. PLoS ONE 2019, 14, e0219924. [Google Scholar] [CrossRef] [Green Version]
- O’Keefe, J.A.; Robertson, E.E.; Ouyang, B.; Carns, D.; McAsey, A.; Liu, Y.; Swanson, M.; Bernard, B.; Berry-Kravis, E.; Hall, D.A. Cognitive function impacts gait, functional mobility and falls in fragile X-associated tremor/ataxia syndrome. Gait Posture 2018, 66, 288–293. [Google Scholar] [CrossRef]
- McKenzie, F.J.; Tassanakijpanich, N.; Epps, K.C.; March, S.K.; Hagerman, R.J. Spontaneous Coronary Artery Dissection in Females With the Fragile X FMR1 Premutation. JACC Case Rep. 2020, 2, 40–44. [Google Scholar] [CrossRef]
- Pugliese, P.; Annesi, G.; Cutuli, N.; Arabia, G.; Nicoletti, G.; Annesi, F.; Tarantino, P.; Gambardella, A.; Valentino, P.; Zappia, M.; et al. The fragile X premutation presenting as postprandial hypotension. Neurology 2004, 63, 2188–2189. [Google Scholar] [CrossRef]
- Louis, E.; Moskowitz, C.; Friez, M.; Amaya, M.; Vonsattel, J.P.G. Parkinsonism, dysautonomia, and intranuclear inclusions in a fragile X carrier: A clinical–pathological study. Mov. Disord. 2006, 21, 420–425. [Google Scholar] [CrossRef]
- Bacalman, S.; Farzin, F.; Bourgeois, J.; Cogswell, J.; Goodlin-Jones, B.; Gane, L.; Grigsby, J.; Leehey, M.; Tassone, F.; Hagerman, R. Psychiatric Phenotype of the Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS) in Males: Newly Described Fronto-Subcortical Dementia. J. Clin. Psychiatry 2006, 67, 87–94. [Google Scholar] [CrossRef]
- Capelli, L.P.; Gonçalves, M.R.R.; Kok, F.; Leite, C.C.; Nitrini, R.; Barbosa, E.R.; Vianna-Morgante, A.M. Fragile X-associated tremor/ataxia syndrome: Intrafamilial variability and the size of the FMR1 premutation CGG repeat. Mov. Disord. 2007, 22, 866–870. [Google Scholar] [CrossRef]
- Loesch, D.Z.; Cook, M.; Litewka, L.; Gould, E.; Churchyard, A.; Tassone, F.; Slater, H.R.; Storey, E. A low symptomatic form of neurodegeneration in younger carriers of the FMR1 premutation, manifesting typical radiological changes. J. Med. Genet. 2008, 45, 179–181. [Google Scholar] [CrossRef]
- Battistella, G.; Niederhauser, J.; Fornari, E.; Hippolyte, L.; Gronchi Perrin, A.; Lesca, G.; Forzano, F.; Hagmann, P.; Vingerhoets, F.J.G.; Draganski, B.; et al. Brain structure in asymptomatic FMR1 premutation carriers at risk for fragile X-associated tremor/ataxia syndrome. Neurobiol. Aging 2013, 34, 1700–1707. [Google Scholar] [CrossRef]
- Famula, J.L.; McKenzie, F.; McLennan, Y.A.; Grigsby, J.; Tassone, F.; Hessl, D.; Rivera, S.M.; Martinez-Cerdeno, V.; Hagerman, R.J. Presence of middle cerebellar peduncle sign in FMR1 premutation carriers without tremor and ataxia. Front. Neurol. 2018, 9, 1–6. [Google Scholar] [CrossRef]
- Renaud, M.; Perriard, J.; Coudray, S.; Sévin-Allouet, M.; Marcel, C.; Meissner, W.G.; Chanson, J.-B.; Collongues, N.; Philippi, N.; Gebus, O.; et al. Relevance of corpus callosum splenium versus middle cerebellar peduncle hyperintensity for FXTAS diagnosis in clinical practice. J. Neurol. 2015, 262, 435–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, J.S.; Adams, P.E.; Nguyen, D.; Brunberg, J.A.; Tassone, F.; Zhang, W.; Koldewyn, K.; Rivera, S.M.; Grigsby, J.; Zhang, L.; et al. Volumetric brain changes in females with fragile X-associated tremor/ataxia syndrome (FXTAS). Neurology 2007, 69, 851–859. [Google Scholar] [CrossRef]
- Brunberg, J.A.; Jacquemont, S.; Hagerman, R.J.; Berry-Kravis, E.M.; Grigsby, J.; Leehey, M.A.; Tassone, F.; Brown, W.T.; Greco, C.M.; Hagerman, P.J. Fragile X Premutation Carriers: Characteristic MR Imaging Findings of Adult Male Patients with Progressive Cerebellar and Cognitive Dysfunction. Am. J. Neuroradiol. 2002, 23, 1757–1766. [Google Scholar]
- Hashimoto, R.; Javan, A.K.; Tassone, F.; Hagerman, R.J.; Rivera, S.M. A voxel-based morphometry study of grey matter loss in fragile X-associated tremor/ataxia syndrome. Brain 2011, 134, 863–878. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.Y.; Hagerman, R.J.; Rivera, S.M. A multimodal imaging analysis of subcortical gray matter in fragile X premutation carriers. Mov. Disord. 2013, 28, 1278–1284. [Google Scholar] [CrossRef]
- Cohen, S.; Masyn, K.; Adams, J.; Hessl, D.; Rivera, S.; Tassone, F.; Brunberg, J.; DeCarli, C.; Zhang, L.; Cogswell, J.; et al. Molecular and imaging correlates of the fragile X–associated tremor/ataxia syndrome. Neurology 2006, 67, 1426–1431. [Google Scholar] [CrossRef]
- Wang, J.Y.; Hessl, D.; Hagerman, R.J.; Simon, T.J.; Tassone, F.; Ferrer, E.; Rivera, S.M. Abnormal trajectories in cerebellum and brainstem volumes in carriers of the fragile X premutation. Neurobiol. Aging 2017, 55, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.Y.; Hessl, D.; Tassone, F.; Kim, K.; Hagerman, R.J.; Rivera, S.M. Interaction between ventricular expansion and structural changes in the corpus callosum and putamen in males with FMR1 normal and premutation alleles. Neurobiol. Aging 2020, 86, 27–38. [Google Scholar] [CrossRef]
- Hashimoto, R.; Srivastava, S.; Tassone, F.; Hagerman, R.J.; Rivera, S.M. Diffusion tensor imaging in male premutation carriers of the fragile X mental retardation gene. Mov. Disord. 2011, 26, 1329–1336. [Google Scholar] [CrossRef]
- Wang, J.Y.; Hessl, D.; Iwahashi, C.; Cheung, K.; Schneider, A.; Hagerman, R.J.; Hagerman, P.J.; Rivera, S.M. Influence of the fragile X mental retardation (FMR1) gene on the brain and working memory in men with normal FMR1 alleles. Neuroimage 2013, 65, 288–298. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.S.G.; Stanfield, A.C. Fragile X premutation carriers: A systematic review of neuroimaging findings. J. Neurol. Sci. 2015, 352, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.Y.; Hessl, D.; Schneider, A.; Tassone, F.; Hagerman, R.J.; Rivera, S.M. Fragile X–Associated Tremor/Ataxia Syndrome: Influence of the FMR1 Gene on Motor Fiber Tracts in Males With Normal and Premutation AllelesFragile X–Associated Tremor/Ataxia Syndrome. JAMA Neurol. 2013, 70, 1022–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birch, R.C.; Hocking, D.R.; Cornish, K.M.; Menant, J.C.; Georgiou-Karistianis, N.; Godler, D.E.; Wen, W.; Hackett, A.; Rogers, C.; Trollor, J.N. Preliminary evidence of an effect of cerebellar volume on postural sway in FMR1 premutation males. Genes Brain Behav. 2015, 14, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, R.; Backer, K.C.; Tassone, F.; Hagerman, R.J.; Rivera, S.M. An fMRI study of the prefrontal activity during the performance of a working memory task in premutation carriers of the fragile X mental retardation 1 gene with and without fragile X-associated tremor/ataxia syndrome (FXTAS). J. Psychiatr. Res. 2011, 45, 36–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hocking, D.R.; Loesch, D.Z.; Trost, N.; Bui, M.Q.; Hammersley, E.; Francis, D.; Tassone, F.; Storey, E. Total and regional white matter lesions are correlated with motor and cognitive impairments in carriers of the FMR1 premutation. Front. Neurol. 2019, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, P.E.; Adams, J.S.; Nguyen, D.V.; Hessl, D.; Brunberg, J.A.; Tassone, F.; Zhang, W.; Koldewyn, K.; Rivera, S.M.; Grigsby, J.; et al. Psychological symptoms correlate with reduced hippocampal volume in fragile X premutation carriers. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2010, 153, 775–785. [Google Scholar] [CrossRef] [Green Version]
- Giulivi, C.; Napoli, E.; Tassone, F.; Halmai, J.; Hagerman, R. Plasma metabolic profile delineates roles for neurodegeneration, pro-inflammatory damage and mitochondrial dysfunction in the FMR1 premutation. Biochem. J. 2016, 473, 3871–3888. [Google Scholar] [CrossRef]
- Alvarez-Mora, M.I.; Rodriguez-Revenga, L.; Madrigal, I.; Guitart-Mampel, M.; Garrabou, G.; Milà, M. Impaired Mitochondrial Function and Dynamics in the Pathogenesis of FXTAS. Mol. Neurobiol. 2017, 54, 6896–6902. [Google Scholar] [CrossRef]
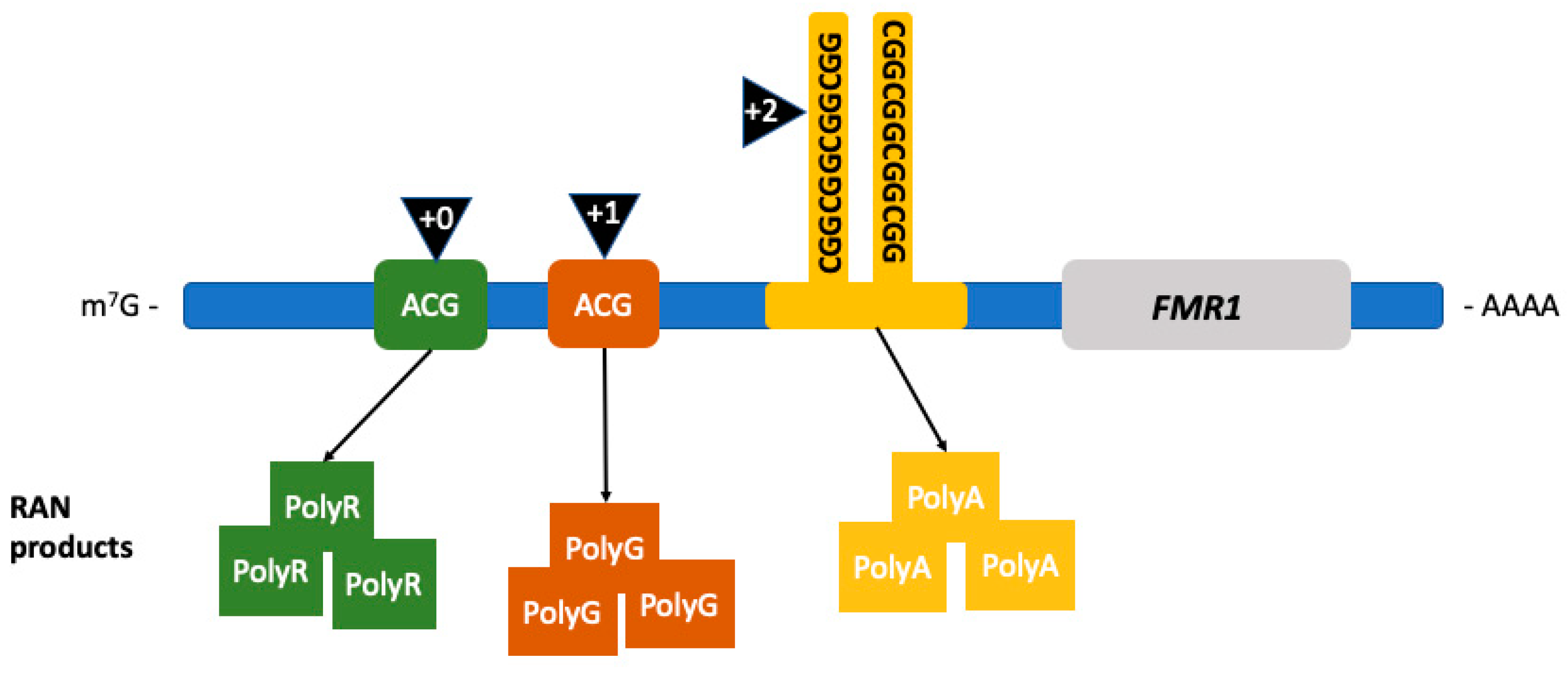
- Todd, P.K.; Oh, S.Y.; Krans, A.; He, F.; Sellier, C.; Frazer, M.; Renoux, A.J.; Chen, K.; Scaglione, K.M.; Basrur, V.; et al. CGG Repeat-Associated Translation Mediates Neurodegeneration in Fragile X Tremor Ataxia Syndrome. Neuron 2013, 78, 440–455. [Google Scholar] [CrossRef] [Green Version]
- Zu, T.; Gibbens, B.; Doty, N.S.; Gomes-Pereira, M.; Huguet, A.; Stone, M.D.; Margolis, J.; Peterson, M.; Markowski, T.W.; Ingram, M.A.C.; et al. Non-ATG–initiated translation directed by microsatellite expansions. Proc. Natl. Acad. Sci. USA 2011, 108, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Bañez-Coronel, M.; Ayhan, F.; Tarabochia, A.D.; Zu, T.; Perez, B.A.; Tusi, S.K.; Pletnikova, O.; Borchelt, D.R.; Ross, C.A.; Margolis, R.L.; et al. RAN Translation in Huntington Disease. Neuron 2015, 88, 667–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, J.D.; Ranum, L.P.W. New developments in RAN translation: Insights from multiple diseases. Curr. Opin. Genet. Dev. 2017, 44, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Cleary, J.D.; Pattamatta, A.; Ranum, L.P.W. Repeat-associated non-ATG (RAN) translation. J. Biol. Chem. 2018, 293, 16127–16141. [Google Scholar] [CrossRef] [Green Version]
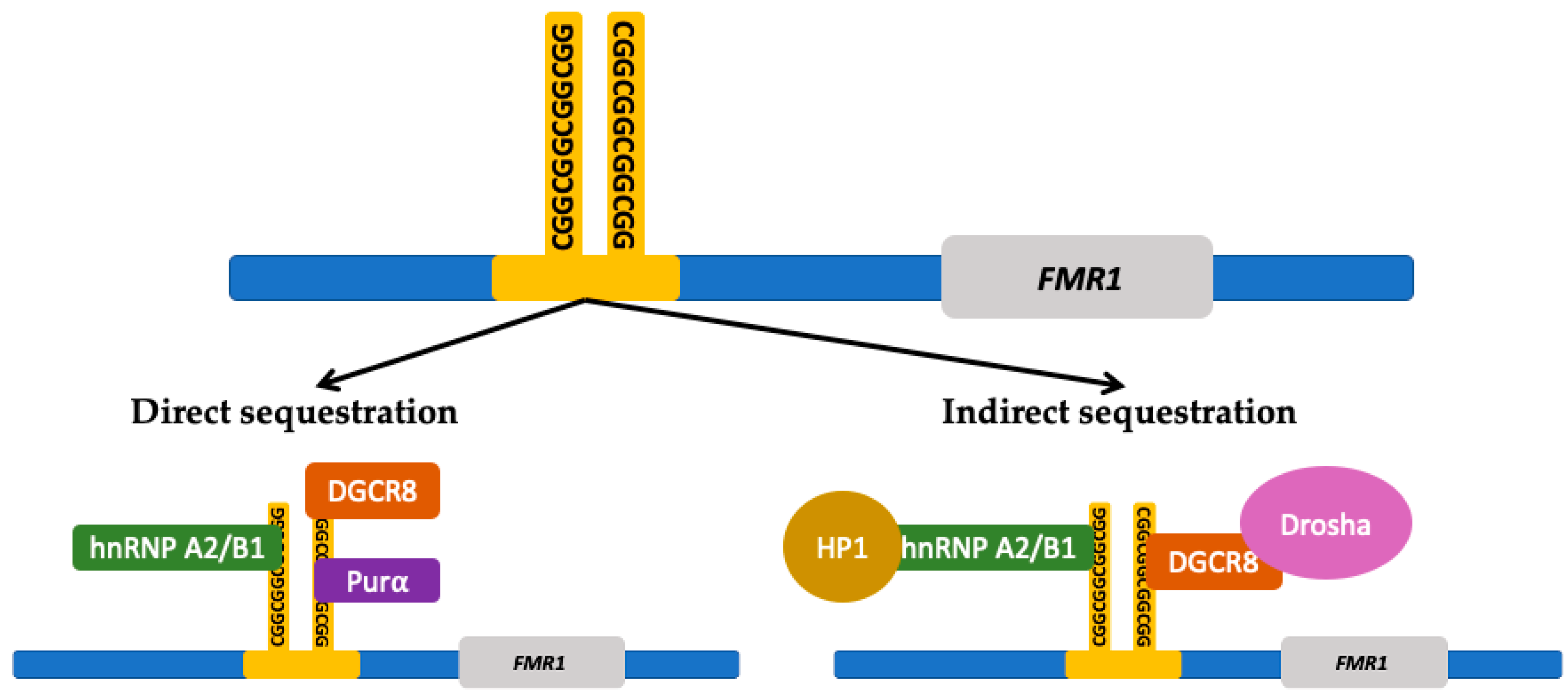
- Sellier, C.; Buijsen, R.A.M.; He, F.; Natla, S.; Jung, L.; Tropel, P.; Gaucherot, A.; Jacobs, H.; Meziane, H.; Vincent, A.; et al. Translation of Expanded CGG Repeats into FMRpolyG Is Pathogenic and May Contribute to Fragile X Tremor Ataxia Syndrome. Neuron 2017, 93, 331–347. [Google Scholar] [CrossRef] [Green Version]
- Glineburg, M.R.; Todd, P.K.; Charlet-Berguerand, N.; Sellier, C. Repeat-associated non-AUG (RAN) translation and other molecular mechanisms in Fragile X Tremor Ataxia Syndrome. Brain Res. 2018, 1693, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Sellier, C.; Freyermuth, F.; Tabet, R.; Tran, T.; He, F.; Ruffenach, F.; Alunni, V.; Moine, H.; Thibault, C.; Page, A.; et al. Sequestration of DROSHA and DGCR8 by Expanded CGG RNA Repeats Alters MicroRNA Processing in Fragile X-Associated Tremor/Ataxia Syndrome. Cell Rep. 2013, 3, 869–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, C.M.; Hagerman, R.J.; Tassone, F.; Chudley, A.E.; Del Bigio, M.R.; Jacquemont, S.; Leehey, M.; Hagerman, P.J. Neuronal intranuclear inclusions in a new cerebellar tremor/ataxia syndrome among fragile X carriers. Brain 2002, 125, 1760–1771. [Google Scholar] [CrossRef]
- Tassone, F.; Hagerman, R.J.; Garcia-Arocena, D.; Khandjian, E.W.; Greco, C.M.; Hagerman, P.J. Intranuclear inclusions in neural cells with premutation alleles in fragile X associated tremor/ataxia syndrome. J. Med. Genet. 2004, 41, e43. [Google Scholar] [CrossRef] [Green Version]
- Iwahashi, C.K.; Yasui, D.H.; An, H.-J.; Greco, C.M.; Tassone, F.; Nannen, K.; Babineau, B.; Lebrilla, C.B.; Hagerman, R.J.; Hagerman, P.J. Protein composition of the intranuclear inclusions of FXTAS. Brain 2005, 129, 256–271. [Google Scholar] [CrossRef]
- Ma, L.; Herren, A.W.; Espinal, G.; Randol, J.; McLaughlin, B.; Martinez-Cerdeño, V.; Pessah, I.N.; Hagerman, R.J.; Hagerman, P.J. Composition of the Intranuclear Inclusions of Fragile X-associated Tremor/Ataxia Syndrome. Acta Neuropathol. Commun. 2019, 7, 143. [Google Scholar] [CrossRef] [Green Version]
- Loomis, E.W.; Sanz, L.A.; Chédin, F.; Hagerman, P.J. Transcription-Associated R-Loop Formation across the Human FMR1 CGG-Repeat Region. PLoS Genet. 2014, 10, e1004294. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Lieber, M.R. G Clustering Is Important for the Initiation of Transcription-Induced R-Loops In Vitro, whereas High G Density without Clustering Is Sufficient Thereafter. Mol. Cell. Biol. 2009, 29, 3124–3133. [Google Scholar] [CrossRef] [Green Version]
- Belotserkovskii, B.P.; Liu, R.; Tornaletti, S.; Krasilnikova, M.M.; Mirkin, S.M.; Hanawalt, P.C. Mechanisms and implications of transcription blockage by guanine-rich DNA sequences. Proc. Natl. Acad. Sci. USA 2010, 107, 12816–12821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usdin, K.; House, N.C.M.; Freudenreich, C.H. Repeat instability during DNA repair: Insights from model systems. Crit. Rev. Biochem. Mol. Biol. 2015, 50, 142–167. [Google Scholar] [CrossRef] [PubMed]
- Barzilai, A. DNA damage, neuronal and glial cell death and neurodegeneration. Apoptosis 2010, 15, 1371–1381. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.S.; Cao, Z.; Hulsizer, S.; Tassone, F.; Berman, R.F.; Hagerman, P.J.; Pessah, I.N. Early mitochondrial abnormalities in hippocampal neurons cultured from Fmr1 pre-mutation mouse model. J. Neurochem. 2012, 123, 613–621. [Google Scholar] [CrossRef] [Green Version]
- Ross-Inta, C.; Omanska-Klusek, A.; Wong, S.; Barrow, C.; Garcia-Arocena, D.; Iwahashi, C.; Berry-Kravis, E.; Hagerman, R.J.; Hagerman, P.J.; Giulivi, C. Evidence of mitochondrial dysfunction in fragile X-associated tremor/ataxia syndrome. Biochem. J. 2010, 429, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Napoli, E.; Ross-Inta, C.; Wong, S.; Omanska-Klusek, A.; Barrow, C.; Iwahashi, C.; Garcia-Arocena, D.; Sakaguchi, D.; Berry-Kravis, E.; Hagerman, R.; et al. Altered zinc transport disrupts mitochondrial protein processing/import in fragile X-associated tremor/ataxia syndrome. Hum. Mol. Genet. 2011, 20, 3079–3092. [Google Scholar] [CrossRef] [Green Version]
- Song, G.; Napoli, E.; Wong, S.; Hagerman, R.; Liu, S.; Tassone, F.; Giulivi, C. Altered Redox Mitochondrial Biology in the Neurodegenerative Disorder Fragile X-Tremor/Ataxia Syndrome: Use of Antioxidants in Precision Medicine. Mol. Med. 2016, 22, 548–559. [Google Scholar] [CrossRef] [Green Version]
- Hagerman, P.J.; Hagerman, R.J. The fragile-X premutation: A maturing perspective. Am. J. Hum. Genet. 2004, 74, 805–816. [Google Scholar] [CrossRef] [Green Version]
- Salcedo-Arellano, M.J.; Dufour, B.; McLennan, Y.; Martinez-Cerdeno, V.; Hagerman, R. Fragile X syndrome and associated disorders: Clinical aspects and pathology. Neurobiol. Dis. 2020, 136, 104740. [Google Scholar] [CrossRef] [PubMed]
- Greco, C.M.; Soontrapornchai, K.; Wirojanan, J.; Gould, J.E.; Hagerman, P.J.; Hagerman, R.J. Testicular and Pituitary Inclusion Formation in Fragile X Associated Tremor/Ataxia Syndrome. J. Urol. 2007, 177, 1434–1437. [Google Scholar] [CrossRef] [PubMed]
- Tassone, F.; Iwahashi, C.; Hagerman, P.J. FMR1 RNA within the Intranuclear Inclusions of Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS). RNA Biol. 2004, 1, 103–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ariza, J.; Rogers, H.; Hartvigsen, A.; Snell, M.; Dill, M.; Judd, D.; Hagerman, P.; Martínez-Cerdeño, V. Iron accumulation and dysregulation in the putamen in fragile X-associated tremor/ataxia syndrome. Mov. Disord. 2017, 32, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Ariza, J.; Steward, C.; Rueckert, F.; Widdison, M.; Coffman, R.; Afjei, A.; Noctor, S.C.; Hagerman, R.; Hagerman, P.; Martínez-Cerdeño, V. Dysregulated iron metabolism in the choroid plexus in fragile X-associated tremor/ataxia syndrome. Brain Res. 2015, 1598, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Rogers, H.; Ariza, J.; Monterrubio, A.; Hagerman, P.; Martínez-Cerdeño, V. Cerebellar Mild Iron Accumulation in a Subset of FMR1 Premutation Carriers with FXTAS. Cerebellum 2016, 15, 641–644. [Google Scholar] [CrossRef]
- Cunningham, C.L.; Martínez Cerdeño, V.; Navarro Porras, E.; Prakash, A.N.; Angelastro, J.M.; Willemsen, R.; Hagerman, P.J.; Pessah, I.N.; Berman, R.F.; Noctor, S.C. Premutation CGG-repeat expansion of the Fmr1 gene impairs mouse neocortical development. Hum. Mol. Genet. 2010, 20, 64–79. [Google Scholar] [CrossRef]
- Martínez Cerdeño, V.; Hong, T.; Amina, S.; Lechpammer, M.; Ariza, J.; Tassone, F.; Noctor, S.C.; Hagerman, P.; Hagerman, R. Microglial cell activation and senescence are characteristic of the pathology FXTAS. Mov. Disord. 2018, 33, 1887–1894. [Google Scholar] [CrossRef]
- Salcedo-Arellano, M.J.; Wolf-Ochoa, M.W.; Hong, T.; Amina, S.; Tassone, F.; Lechpammer, M.; Hagerman, R.; Martínez-Cerdeño, V. Parkinsonism versus concomitant Parkinson’s disease in Fragile X-associated Tremor/Ataxia Syndrome. Mov. Disord. Clin. Pract. 2020, 7, 413–418. [Google Scholar] [CrossRef]
- Aydin, E.Y.; Schneider, A.; Protic, D.; Wang, J.Y.; Martínez-Cerdeño, V.; Tassone, F.; Tang, H.-T.; Perlman, S.; Hagerman, R.J. Rapidly Progressing Neurocognitive Disorder in a Male with FXTAS and Alzheimer’s Disease. Clin. Interv. Aging 2020, 15, 285–292. [Google Scholar] [CrossRef] [Green Version]
- De Pablo-Fernandez, E.; Doherty, K.M.; Holton, J.L.; Revesz, T.; Djamshidian, A.; Limousin, P.; Bhatia, K.P.; Warner, T.T.; Lees, A.J.; Ling, H. Concomitant fragile X-associated tremor ataxia syndrome and Parkinson’s disease: A clinicopathological report of two cases. J. Neurol. Neurosurg. Psychiatry 2015, 86, 934–936. [Google Scholar] [CrossRef] [Green Version]
- Loesch, D.Z.; Litewka, L.; Brotchie, P.; Huggins, R.M.; Tassone, F.; Cook, M. Magnetic resonance imaging study in older fragile X premutation male carriers. Ann. Neurol. 2005, 58, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Hall, D.A.; Birch, R.C.; Anheim, M.; Jønch, A.E.; Pintado, E.; O’Keefe, J.; Trollor, J.N.; Stebbins, G.T.; Hagerman, R.J.; Fahn, S.; et al. Emerging topics in FXTAS. J. Neurodev. Disord. 2014, 6, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry-Kravis, E.; Abrams, L.; Coffey, S.M.; Hall, D.A.; Greco, C.; Gane, L.W.; Grigsby, J.; Bourgeois, J.A.; Finucane, B.; Jacquemont, S.; et al. Fragile X-associated tremor/ataxia syndrome: Clinical features, genetics, and testing guidelines. Mov. Disord. 2007, 22, 2018–2030. [Google Scholar] [CrossRef] [PubMed]
- Robertson, E.; Hall, D.; McAsey, A.; O’Keefe, J.A. Fragile X-associated tremor/ataxia syndrome: Phenotypic comparisons with other movement disorders. Clin. Neuropsychol. 2016, 30, 849–900. [Google Scholar] [CrossRef]
- Polussa, J.; Schneider, A.; Hagerman, R. Molecular Advances Leading to Treatment Implications for Fragile X Premutation Carriers. Brain Disord. Ther. 2014, 3, 1–14. [Google Scholar]
- Johnson, J.W.; Kotermanski, S.E. Mechanism of action of memantine. Curr. Opin. Pharmacol. 2006, 6, 61–67. [Google Scholar] [CrossRef]
- Seritan, A.L.; Nguyen, D.V.; Mu, Y.; Tassone, F.; Bourgeois, J.A.; Schneider, A.; Cogswell, J.B.; Cook, K.R.; Leehey, M.A.; Grigsby, J.; et al. Memantine for Fragile X–Associated Tremor/Ataxia Syndrome. J. Clin. Psychiatry 2014, 75, 264–271. [Google Scholar] [CrossRef]
- Yang, J.-C.; Niu, Y.-Q.; Simon, C.; Seritan, A.L.; Chen, L.; Schneider, A.; Moghaddam, S.T.; Hagerman, P.J.; Hagerman, R.J.; Olichney, J.M. Memantine Effects on Verbal Memory in Fragile X-associated Tremor/Ataxia Syndrome (FXTAS): A Double-Blind Brain Potential Study. Neuropsychopharmacology 2014, 39, 2760–2768. [Google Scholar] [CrossRef]
- Yang, J.-C.; Rodriguez, A.; Royston, A.; Niu, Y.-Q.; Avar, M.; Brill, R.; Simon, C.; Grigsby, J.; Hagerman, R.J.; Olichney, J.M. Memantine Improves Attentional Processes in Fragile X-Associated Tremor/Ataxia Syndrome: Electrophysiological Evidence from a Randomized Controlled Trial. Sci. Rep. 2016, 6, 21719. [Google Scholar] [CrossRef] [Green Version]
- Napoli, E.; Schneider, A.; Wang, J.Y.; Trivedi, A.; Carrillo, N.R.; Tassone, F.; Rogawski, M.; Hagerman, R.J.; Giulivi, C. Allopregnanolone Treatment Improves Plasma Metabolomic Profile Associated with GABA Metabolism in Fragile X-Associated Tremor/Ataxia Syndrome: A Pilot Study. Mol. Neurobiol. 2019, 56, 3702–3713. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Trivedi, A.M.; Carrillo, N.R.; Yang, J.; Schneider, A.; Giulivi, C.; Adams, P.; Tassone, F.; Kim, K.; Rivera, S.M.; et al. Open-Label Allopregnanolone Treatment of Men with Fragile X-Associated Tremor/Ataxia Syndrome. Neurotherapeutics 2017, 14, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Secades, J.; Frontera, G. CDP-Choline: Pharmacological and clinical review. Methods Find. Exp. Clin. Pharmacol. 1995, 17, 1–54. [Google Scholar]
- Hall, D.A.; Robertson, E.E.; Leehey, M.; McAsey, A.; Ouyang, B.; Berry-Kravis, E.; O’Keefe, J.A. Open-label pilot clinical trial of citicoline for fragile X-associated tremor/ataxia syndrome (FXTAS). PLoS ONE 2020, 15, e0225191. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.K.; Khan, E.; Mishra, S.K.; Mishra, A.; Charlet-Berguerand, N.; Kumar, A. Curcumin Regulates the r(CGG)exp RNA Hairpin Structure and Ameliorate Defects in Fragile X-Associated Tremor Ataxia Syndrome. Front. Neurosci. 2020, 14, 295. [Google Scholar] [CrossRef] [PubMed]
- Verma, A.K.; Khan, E.; Mishra, S.K.; Jain, N.; Kumar, A. Piperine Modulates Protein Mediated Toxicity in Fragile X-Associated Tremor/Ataxia Syndrome through Interacting Expanded CGG Repeat (r(CGG)exp) RNA. ACS Chem. Neurosci. 2019, 10, 3778–3788. [Google Scholar] [CrossRef] [PubMed]
- Qurashi, A.; Liu, H.; Ray, L.; Nelson, D.L.; Duan, R.; Jin, P. Chemical screen reveals small molecules suppressing fragile X premutation rCGG repeat-mediated neurodegeneration in Drosophila. Hum. Mol. Genet. 2012, 21, 2068–2075. [Google Scholar] [CrossRef] [Green Version]
- Seritan, A.; Nguyen, D.; Mu, Y.; Tassone, F.; Bourgeois, J.; Schneider, A.; Cogswell, J.; Cook, K.; Leehey, M.; Grigsby, J.; et al. Memantine for Fragile X-Associated Tremor/Ataxia Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Psychiatry 2013, 75, 264. [Google Scholar] [CrossRef]
- Trivedi, A.; Wang, J.Y.; Carrillo, N.; Hagerman, R. Allopregnanolone improves neuropsychiatric symptoms in elderly men with Fragile X-associated tremor/ataxia syndrome (FXTAS): Results from an open label study. Neurology 2019, 92. [Google Scholar]
- Sayeed, I.; Parvez, S.; Wali, B.; Siemen, D.; Stein, D.G. Direct inhibition of the mitochondrial permeability transition pore: A possible mechanism for better neuroprotective effects of allopregnanolone over progesterone. Brain Res. 2009, 1263, 165–173. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Criteria | ||
|---|---|---|
| Molecular | Required | FMR1 Mutation * |
| Clinical | Major | Intention tremor |
| Cerebellar gait ataxia | ||
| Minor | Parkinsonism | |
| Neuropathy | ||
| Memory and executive function deficits | ||
| Neuroradiological | Major | White matter lesions in the middle cerebellar peduncles (MCP sign) or brainstem |
| Minor | White matter lesions in the splenium of the corpus callosum | |
| Cerebral white matter lesions | ||
| Moderate–severe brain atrophy | ||
| Neuropathological | Major | Ubiquitin-positive intranuclear inclusions |
| Diagnostic categories | ||
| Definite | 1 clinical major AND 1 neuroradiological major OR 1 neuropathological major | |
| Probable | 2 clinical major OR 1 clinical minor + 1 radiological minor | |
| Possible | 1 clinical major + 1 clinical minor | |
| Medication/Compound | Molecular Mechanism | Clinical Trial Phases Completed | Reference |
|---|---|---|---|
| Curcumin | Decreases RANT and FMRpolyG production, reducing its accumulation. | Preclinical | [167] |
| Selectively binds CGG RNA repeats potentially reducing RNA binding proteins sequestration and reducing CGG repeats-induced cell toxicity. | |||
| Cytidine 5′diphospho-choline (Citicoline) | Inhibition of phospholipase A2 (PLA2) leading to suppression of CGG repeats-induced cell toxicity. | Phase 2 | [166,169] |
| Memantine | Noncompetitive antagonist of N-methyl-d-aspartate (NMDA) proposed to normalize premutation associated abnormal neuronal response to glutamate. | Phase 2 | [161,170] |
| Piperine | Selectively binds CGG RNA repeats potentially reducing RNA binding proteins sequestration and reducing CGG repeats-induced cell toxicity. | Preclinical | [168] |
| Allopregnanolone | Positive allosteric modulator of GABA receptors. | Phase 2 | [163,164,171,172] |
| Reduction of caspase-3 protein expression leading to reduced apoptosis. | |||
| Inhibition of mitochondrial permeability transition pore which is implicated in the intrinsic pathway of apoptosis. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabal-Herrera, A.M.; Tassanakijpanich, N.; Salcedo-Arellano, M.J.; Hagerman, R.J. Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Pathophysiology and Clinical Implications. Int. J. Mol. Sci. 2020, 21, 4391. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21124391
Cabal-Herrera AM, Tassanakijpanich N, Salcedo-Arellano MJ, Hagerman RJ. Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Pathophysiology and Clinical Implications. International Journal of Molecular Sciences. 2020; 21(12):4391. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21124391
Chicago/Turabian StyleCabal-Herrera, Ana Maria, Nattaporn Tassanakijpanich, Maria Jimena Salcedo-Arellano, and Randi J. Hagerman. 2020. "Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Pathophysiology and Clinical Implications" International Journal of Molecular Sciences 21, no. 12: 4391. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21124391