Identification of Subclinical Lung Involvement in ACPA-Positive Subjects through Functional Assessment and Serum Biomarkers

 , , ,
, , ,
Abstract
:1. Introduction
- to evaluate the presence of subclinical lung involvement among ACPA-positive subjects without respiratory complains with and without confirmed diagnosis of RA;
- to assess pulmonary functional impairment at rest and during exercise through PFT and CPET, respectively;
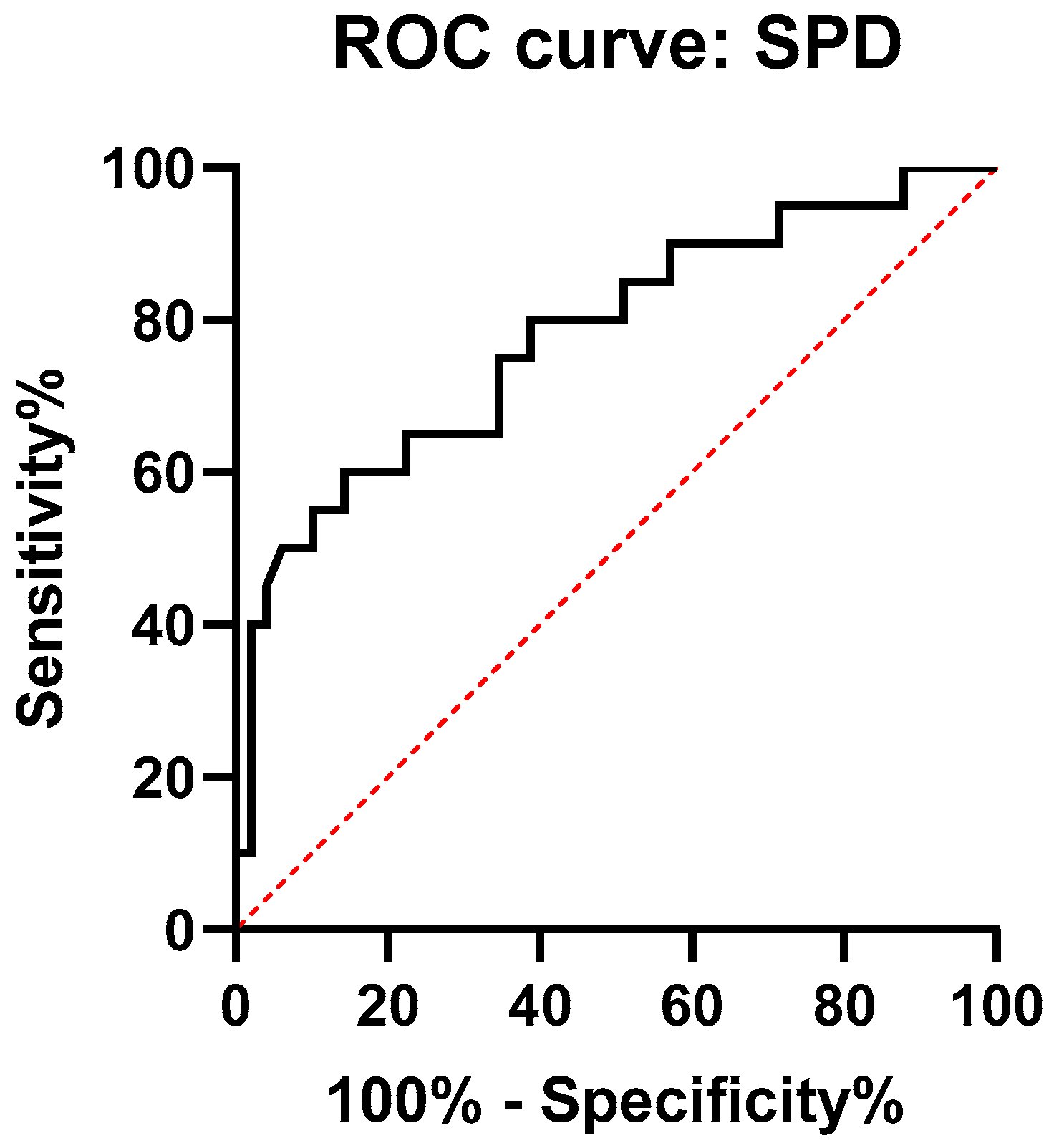
- to evaluate the diagnostic potential of serum autoantibodies and SPD levels, with regard to radiology findings of lung involvement.
2. Results
2.1. Subjects’ Characteristics
2.2. Lung Function and Physiological Responses to Exercise
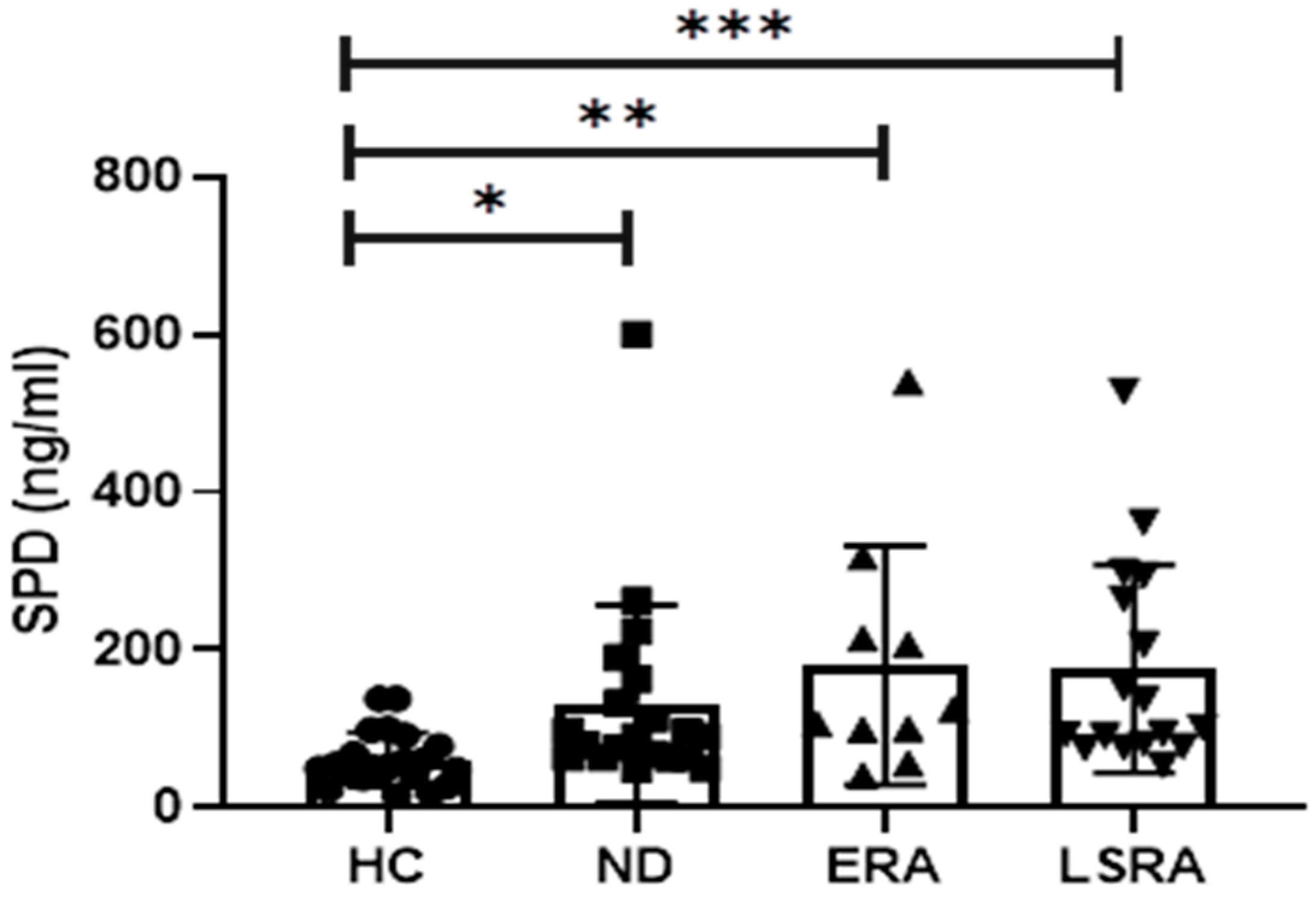
2.3. Laboratory Results
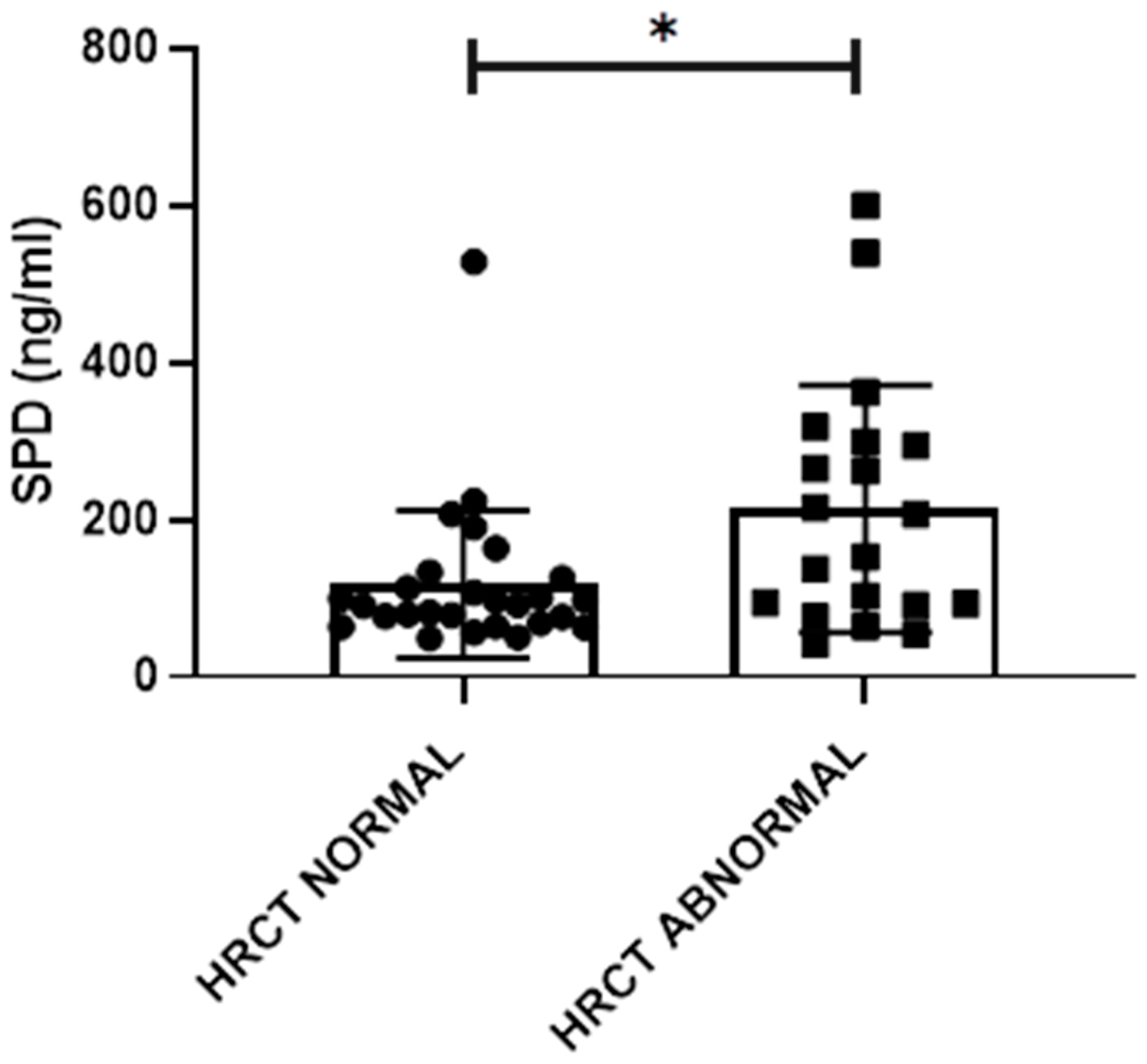
2.4. HRCT Abnormalities
2.5. Relations between Functional and Laboratory Data and the Presence of HRCT Abnormalities
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. Clinic and Clinimetric Evaluation
4.3. Laboratory Evaluation
4.4. Functional Evaluation
4.5. Imaging Evaluation
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scott, D.L.; Wolfe, F.; Huizinga, T.W. Rheumatoid arthritis. Lancet 2010, 376, 1094–1108. [Google Scholar] [CrossRef]
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Young, A.; Koduri, G.; Batley, M.; Kulinskaya, E.; Gough, A.; Norton, S.; Dixey, J. Mortality in rheumatoid arthritis. Increased in the early course of disease, in ischaemic heart disease and in pulmonary fibrosis. Rheumatology 2006, 46, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Steenbergen, H.W.; Aletaha, D.; Beaart-Van De Voorde, L.J.J.; Brouwer, E.; Codreanu, C.; Combe, B.; Fonseca, J.E.; Hetland, M.L.; Humby, F.; Kvien, T.K. EULAR definition of arthralgia suspicious for progression to rheumatoid arthritis. Ann. Rheum. Dis. 2017, 76, 491–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klareskog, L.; Malmström, V.; Lundberg, K.; Padyukov, L.; Alfredsson, L. Smoking, citrullination and genetic variability in the immunopathogenesis of rheumatoid arthritis. Semin. Immunol. 2011, 23, 92–98. [Google Scholar] [CrossRef]
- Lucchino, B.; Spinelli, F.R.; Iannuccelli, C.; Guzzo, M.P.; Conti, F.; Di Franco, M. Mucosa–Environment Interactions in the Pathogenesis of Rheumatoid Arthritis. Cells 2019, 8, 700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerardi, M.C.; Luca, N.D.; Alessandri, C.; Iannuccelli, C.; Valesini, G.; Di Franco, M. Frequency of antibodies to mutated citrullinated vimentin in chronic obstructive pulmonary disease: Comment on the article by Demoruelle et al. Arthritis Rheum. 2013, 65, 1672–1673. [Google Scholar] [CrossRef]
- Willis, V.C.; Demoruelle, M.K.; Derber, L.A.; Chartier-Logan, C.J.; Parish, M.C.; Pedraza, I.F.; Weisman, M.H.; Norris, J.M.; Holers, V.M.; Deane, K.D. Sputum autoantibodies in patients with established rheumatoid arthritis and subjects at risk of future clinically apparent disease. Arthritis Rheum. 2013, 65, 2545–2554. [Google Scholar] [PubMed]
- Reynisdottir, G.; Karimi, R.; Joshua, V.; Olsen, H.; Hensvold, A.H.; Harju, A.; Engström, M.; Grunewald, J.; Nyren, S.; Eklund, A. Structural changes and antibody enrichment in the lungs are early features of anti–citrullinated protein antibody–positive rheumatoid arthritis. Arthritis Rheumatol. 2014, 66, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Demoruelle, M.K.; Weisman, M.H.; Simonian, P.L.; Lynch, D.A.; Sachs, P.B.; Pedraza, I.F.; Harrington, A.R.; Kolfenbach, J.R.; Striebich, C.C.; Pham, Q.N. Brief Report: Airways abnormalities and rheumatoid arthritis–related autoantibodies in subjects without arthritis: Early injury or initiating site of autoimmunity? Arthritis Rheum. 2012, 64, 1756–1761. [Google Scholar] [CrossRef]
- Shaw, M.; Collins, B.F.; Ho, L.A.; Raghu, G. Rheumatoid arthritis-associated lung disease. Eur. Respir. Rev. 2015, 24, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, Y.-J.; Lee, Y.J.; Kang, E.H. Lung involvements in rheumatic diseases: Update on the epidemiology, pathogenesis, clinical features, and treatment. BioMed Res. Int. 2018, 2018, 19. [Google Scholar] [CrossRef] [Green Version]
- Yamasaki, M. Long-Term Follow up of Subclinical Interstitial Lung Disease in Rheumatoid Arthritis. In Proceedings of the 2018 American College Rheumatology/Association of Rheumatology Professionals Annual Meeting, Chicago, IL, USA, 19–24 October 2018. [Google Scholar]
- Gochuico, B.R.; Avila, N.A.; Chow, C.K.; Novero, L.J.; Wu, H.-P.; Ren, P.; MacDonald, S.D.; Travis, W.D.; Stylianou, M.P.; Rosas, I.O. Progressive preclinical interstitial lung disease in rheumatoid arthritis. Arch. Intern. Med. 2008, 168, 159–166. [Google Scholar] [CrossRef]
- Solomon, J.J.; Chung, J.H.; Cosgrove, G.P.; Demoruelle, M.K.; Fernandez-Perez, E.R.; Fischer, A.; Frankel, S.K.; Hobbs, S.B.; Huie, T.J.; Ketzer, J. Predictors of mortality in rheumatoid arthritis-associated interstitial lung disease. Eur. Respir. J. 2016, 47, 588–596. [Google Scholar] [CrossRef]
- Yang, J.A.; Lee, J.S.; Park, J.K.; Lee, E.B.; Song, Y.W.; Lee, E.Y. Clinical characteristics associated with occurrence and poor prognosis of interstitial lung disease in rheumatoid arthritis. Korean J. Intern. Med. 2019, 34, 434. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Shi, Y.; Wang, X.; Huang, H.; Ascherman, D. Asymptomatic preclinical rheumatoid arthritis-associated interstitial lung disease. Clin. Dev. Immunol. 2013, 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guazzi, M.; Bandera, F.; Ozemek, C.; Systrom, D.; Arena, R. Cardiopulmonary exercise testing: What is its value? J. Am. Coll. Cardiol. 2017, 70, 1618–1636. [Google Scholar] [CrossRef] [PubMed]
- Palange, P.; Ward, S.A.; Carlsen, K.H.; Casaburi, R.; Gallagher, C.G.; Gosselink, R.; O’Donnell, D.E.; Puente-Maestu, L.; Schols, A.M.; Singh, S. Recommendations on the use of exercise testing in clinical practice. Eur. Respir. J. 2007, 29, 185–209. [Google Scholar] [CrossRef]
- Tzilas, V.; Bouros, D. Cardiopulmonary Exercise Testing in Systemic Sclerosis: ‘Ars longa, vita brevis’. Respiration 2016, 91, 202–203. [Google Scholar] [CrossRef] [Green Version]
- Rosato, E.; Romaniello, A.; Magrì, D.; Bonini, M.; Sardo, L.; Gigante, A.; Quarta, S.; Digiulio, M.A.; Viola, G.; Di Paolo, M. Exercise tolerance in systemic sclerosis patients without pulmonary impairment: Correlation with clinical variables. Clin. Exp. Rheumatol. 2014, 32, 103–108. [Google Scholar]
- Doyle, T.J.; Patel, A.S.; Hatabu, H.; Nishino, M.; Wu, G.; Osorio, J.C.; Golzarri, M.F.; Traslosheros, A.; Chu, S.G.; Frits, M.L. Detection of rheumatoid arthritis–interstitial lung disease is enhanced by serum biomarkers. Am. J. Respir. Crit. Care Med. 2015, 191, 1403–1412. [Google Scholar] [CrossRef] [Green Version]
- Madsen, J.; Kliem, A.; Tornøe, I.; Skjødt, K.; Koch, C.; Holmskov, U. Localization of lung surfactant protein D on mucosal surfaces in human tissues. J. Immunol. 2000, 164, 5866–5870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, J.R. Immunoregulatory functions of surfactant proteins. Nat. Rev. Immunol. 2005, 5, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.L.; Husby, S.; Holmskov, U. Surfactant protein A and surfactant protein D variation in pulmonary disease. Immunobiology 2007, 212, 381–416. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Solomon, J.J.; du Bois, R.M.; Deane, K.D.; Olson, A.L.; Fernandez-Perez, E.R.; Huie, T.J.; Stevens, A.D.; Gill, M.B.; Rabinovitch, A.M. Lung disease with anti-CCP antibodies but not rheumatoid arthritis or connective tissue disease. Respir. Med. 2012, 106, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, E.J.; Barr, R.G.; Austin, J.H.M.; Kawut, S.M.; Raghu, G.; Sell, J.L.; Hoffman, E.A.; Newell, J.D.; Watts, J.R.; Nath, P.H. Rheumatoid arthritis-associated autoantibodies and subclinical interstitial lung disease: The Multi-Ethnic Study of Atherosclerosis. Thorax 2016, 71, 1082–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynisdottir, G.; Olsen, H.; Joshua, V.; Engström, M.; Forsslund, H.; Karimi, R.; Sköld, C.M.; Nyren, S.; Eklund, A.; Grunewald, J. Signs of immune activation and local inflammation are present in the bronchial tissue of patients with untreated early rheumatoid arthritis. Ann. Rheum. Dis. 2016, 75, 1722–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyldgaard, C.; Hilberg, O.; Pedersen, A.B.; Ulrichsen, S.P.; Løkke, A.; Bendstrup, E.; Ellingsen, T. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: Comorbidity and mortality. Ann. Rheum. Dis. 2017, 76, 1700–1706. [Google Scholar] [CrossRef]
- Patatanian, E.; Thompson, D.F. A review of methotrexate-induced accelerated nodulosis. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2002, 22, 1157–1162. [Google Scholar] [CrossRef]
- Kiely, P.; Busby, A.D.; Nikiphorou, E.; Sullivan, K.; Walsh, D.A.; Creamer, P.; Dixey, J.; Young, A. Is incident rheumatoid arthritis interstitial lung disease associated with methotrexate treatment? Results from a multivariate analysis in the ERAS and ERAN inception cohorts. BMJ Open 2019, 9, e028466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, C.A.; Saravanan, V.; Nisar, M.; Arthanari, S.; Woodhead, F.A.; Price-Forbes, A.N.; Dawson, J.; Sathi, N.; Ahmad, Y.; Koduri, G. Rheumatoid arthritis-related interstitial lung disease: Associations, prognostic factors and physiological and radiological characteristics—A large multicentre UK study. Rheumatology 2014, 53, 1676–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roubille, C.; Haraoui, B. Interstitial lung diseases induced or exacerbated by DMARDS and biologic agents in rheumatoid arthritis: A systematic literature review. Semin. Arthritis Rheum. 2014, 43, 613–626. [Google Scholar] [CrossRef] [PubMed]
- Geri, G.; Dadoun, S.; Bui, T.; Pinol, N.D.C.; Paternotte, S.; Dougados, M.; Gossec, L. Risk of infections in bronchiectasis during disease-modifying treatment and biologics for rheumatic diseases. BMC Infect. Dis. 2011, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hamblin, M.J.; Horton, M.R. Rheumatoid arthritis-associated interstitial lung disease: Diagnostic dilemma. Pulm. Med. 2011, 2011, 12. [Google Scholar] [CrossRef]
- Wang, T.; Zheng, X.-J.; Liang, B.-M.; Liang, Z.-A. Clinical features of rheumatoid arthritis-associated interstitial lung disease. Sci. Rep. 2015, 5, 14897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podolanczuk, A.J.; Oelsner, E.C.; Barr, R.G.; Hoffman, E.A.; Armstrong, H.F.; Austin, J.H.M.; Basner, R.C.; Bartels, M.N.; Christie, J.D.; Enright, P.L. High attenuation areas on chest computed tomography in community-dwelling adults: The MESA study. Eur. Respir. J. 2016, 48, 1442–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, T.J.; Hunninghake, G.M.; Rosas, I.O. Subclinical interstitial lung disease: Why you should care. Am. J. Respire. Crit. Care Med. 2012, 185, 1147–1153. [Google Scholar] [CrossRef]
- Rosas, I.O.; Ren, P.; Avila, N.A.; Chow, C.K.; Franks, T.J.; Travis, W.D.; McCoy, J.P., Jr.; May, R.M.; Wu, H.-P.; Nguyen, D.M. Early interstitial lung disease in familial pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2007, 176, 698–705. [Google Scholar] [CrossRef] [Green Version]
- Crisafulli, E.; Alfieri, V.; Silva, M.; Aiello, M.; Tzani, P.; Milanese, G.; Bertorelli, G.; Sverzellati, N.; Chetta, A. Relationships between emphysema and airways metrics at high-resolution computed tomography (HRCT) and ventilatory response to exercise in mild to moderate COPD patients. Respir. Med. 2016, 117, 207–214. [Google Scholar] [CrossRef]
- Paoletti, P.; De Filippis, F.; Fraioli, F.; Cinquanta, A.; Valli, G.; Laveneziana, P.; Vaccaro, F.; Martolini, D.; Palange, P. Cardiopulmonary exercise testing (CPET) in pulmonary emphysema. Respir. Physiol. Neurobiol. 2011, 179, 167–173. [Google Scholar] [CrossRef]
- Crisafulli, E.; Teopompi, E.; Luceri, S.; Longo, F.; Tzani, P.; Pagano, P.; Ielpo, A.; Longo, C.; Di Paolo, M.; Sverzellati, N. The value of high-resolution computed tomography (HRCT) to determine exercise ventilatory inefficiency and dynamic hyperinflation in adult patients with cystic fibrosis. Respir. Res. 2019, 20, 78. [Google Scholar] [CrossRef]
- Ju, C.-R.; Liu, W.; Chen, R.-C. Serum surfactant protein D: Biomarker of chronic obstructive pulmonary disease. Dis. Markers 2012, 32, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Giles, J.T.; Danoff, S.K.; Sokolove, J.; Wagner, C.A.; Winchester, R.; Pappas, D.A.; Siegelman, S.; Connors, G.; Robinson, W.H.; Bathon, J.M. Association of fine specificity and repertoire expansion of anticitrullinated peptide antibodies with rheumatoid arthritis associated interstitial lung disease. Ann. Rheum. Dis. 2014, 73, 1487–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demoruelle, M.K.; Harrall, K.K.; Ho, L.; Purmalek, M.M.; Seto, N.L.; Rothfuss, H.M.; Weisman, M.H.; Solomon, J.J.; Fischer, A.; Okamoto, Y. Anti–citrullinated protein antibodies are associated with neutrophil extracellular traps in the sputum in relatives of rheumatoid arthritis patients. Arthritis Rheumatol. 2017, 69, 1165–1175. [Google Scholar] [CrossRef]
- Weatherald, J.; Sattler, C.; Garcia, G.; Laveneziana, P. Ventilatory response to exercise in cardiopulmonary disease: The role of chemosensitivity and dead space. Eur. Respir. J. 2018, 51, 1700860. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Wanger, J.; Clausen, J.L.; Coates, A.; Pedersen, O.F.; Brusasco, V.; Burgos, F.; Casaburi, R.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M. Standardisation of the measurement of lung volumes. Eur. Respir. J. 2005, 26, 511–522. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Eur. Respir. Soc. 1993, 6, 5–40. [Google Scholar] [CrossRef]
- Cotes, J.E.; Chinn, D.J.; Quanjer, P.H.; Roca, J.; Yernault, J.C. Standardization of the measurement of transfer factor (diffusing capacity). Eur. Respir. Soc. 1993, 6, 41–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Thoracic, S. ATS/ACCP statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 2003, 167, 211–277. [Google Scholar]
- Wasserman, K.; Hansen, J.; Sue, D.; Stringer, W.; Whipp, B. Principles of Exercise Testing and Interpretation, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- Koch, B.; Schäper, C.; Ittermann, T.; Spielhagen, T.; Dörr, M.; Völzke, H.; Opitz, C.F.; Ewert, R.; Gläser, S. Reference values for cardiopulmonary exercise testing in healthy volunteers: The SHIP study. Eur. Respir. J. 2009, 33, 389–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 48) | ND (n = 21) | ERA (n = 10) | LSRA (n = 17) | HC (n = 22) | p | |
|---|---|---|---|---|---|---|
| Age, years | 49.8 ± 11 | 50.38 ± 13.6 | 48.5 ± 10.8 | 53.06 ± 7.3 | 47.3 ± 10.5 | 0.49 |
| Sex, M/F | 11/37 | 3/18 | 3/7 | 5/12 | 7/15 | 0.45 |
| BMI, kg/m2 | 24.1 ± 4 | 23.3 ± 3.01 | 25.5 ± 5.6 | 25.5 ± 5.6 | 24.9 ± 2.8 | 0.28 |
| Smoking, current/former/never | 14/12/22 | 7/1/13 | 2/5/3 | 5/6/6 | 8/4/10 | 0.1 |
| Disease duration, months | 13.78 ± 11.02 | - | 3.6 ± 1.5 | 19.97 ± 9.6 † | - | <0.0001 |
| DAS28 | 3.6 ± 1.5 | - | 4.21 ± 1.7 | 3.2 ± 1.45 | - | 0.2 |
| ACPA, UI/L | 321.3 ± 394.9 | 342 ± 429.6 | 298.8 ± 202.2 | 309 ± 450.8 | - | 0.73 |
| RF, UI/L | 139.9 ±179.2 | 101.2 ± 138.8 | 182.2 ± 195.4 | 163 ± 212.5 | - | 0.46 |
| Overall (n = 48) | ND (n = 21) | ERA (n = 10) | LSRA (n = 17) | p | |
|---|---|---|---|---|---|
| FEV1, % pred. | 102.6 ± 11.9 | 104.3 ± 11.0 | 100.5 ± 14.7 | 101.9 ± 11.5 | 0.56 |
| FVC, % pred. | 107.8 ± 12.8 | 108.3 ± 13.8 | 105.4 ± 9.3 | 108.7 ± 13.7 | 0.81 |
| FEV1/FVC, % | 80.2 ± 7.0 | 81.4 ± 6.9 | 80.0 ± 7.6 | 78.8 ± 6.9 | 0.7 |
| TLC, % pred. | 99.3 ± 12.1 | 98.5 ± 13.5 | 97.9 ± 11.9 | 101.3 ± 11.3 | 0.5 |
| DLCO, % pred. | 81.5 ± 16.6 | 83.7 ± 18.7 | 82.5 ± 19.4 | 78.5 ± 13.0 | 0.76 |
| KCO, % pred. | 84.3 ± 17.5 | 85.8 ± 17.8 | 90.2 ± 20.4 | 79.6 ± 15.3 | 0.21 |
| Reduced DLCO, n (%) | 28 (58.3) | 12 (57.1) | 5 (50.0) | 11 (64.7) | 0.71 |
| Work rate peak, % pred. | 76.1 ± 15.4 | 71.4 ± 14.2 | 71.1 ± 12.7 | 84.4 ± 15.4 | 0.35 |
| V’O2 peak, mL/min/kg | 22.7 ± 4.4 | 23.1 ± 3.9 | 23.6 ± 5.6 | 21.8 ± 4.3 | 0.81 |
| V’O2 peak, % pred. | 90.1 ± 15.9 | 92.6 ± 17.8 | 90.7 ± 14.5 | 86.7 ± 14.6 | 0.63 |
| Reduced exercise tolerance, n (%) | 19 (39.6) | 7 (33.3) | 3 (30.0) | 9 (52.9) | 0.53 |
| V’O2 at θL, % pred. V’O2 peak | 52.7 ± 10.6 | 55.2 ± 9.6 | 47.3 ± 11.7 | 53.0 ± 10.6 | 0.2 |
| V’E peak, l/min | 57.3 ± 18.9 | 54.0 ± 10.1 | 65.0 ± 20.3 | 56.7 ± 24.9 | 0.39 |
| V’E peak, %eMVV | 49.8 ± 12.0 | 49.3 ± 11.8 | 54.5 ± 11.9 | 47.6 ± 12.2 | 0.63 |
| SpO2 peak, % | 97.3 ± 1.4 | 97.7 ± 1.1 | 97.6 ± 1.2 | 96.8 ± 1.7 * | 0.017 |
| ΔSpO2, % | -0.3 ± 1.3 | -0.2 ± 1.2 | 0 ± 0.9 | -0.7 ± 1.5 | 0.26 |
| V’E/V’CO2 at θL | 30.6 ± 4.6 | 29.9 ± 5.0 | 31.6 ± 5.6 | 30.7 ± 4.6 | 0.72 |
| V’E/V’CO2 slope | 27.8 ± 4.6 | 27.0 ± 5.0 | 29.0 ± 3.8 | 28.0 ± 4.5 | 0.5 |
| Impaired ventilatory efficiency, n (%) | 15 (31.2) | 6 (28.6) | 2 (20.0) | 7 (41.2) | 0.5 |
| Overall (n = 48) | ND (n = 21) | ERA (n = 10) | LSRA (n = 17) | p | |
|---|---|---|---|---|---|
| Total, % | 62.5 | 38 | 60 | 94.1 *,† | 0.001 |
| Parenchymal, % | 62.5 | 38 | 60 | 94.1 *,† | 0.001 |
| Airways, % | 16.6 | 14.3 | 10 | 23.5 | 0.98 |
| Emphysema, % | 16.6 | - | 30 * | 29.4 * | 0.02 |
| Fibrosis, % | 29.1 | 14.3 | 10 | 58.8 *,† | 0.003 |
| Ground glass, % | 6.25 | - | - | 17.6 | 0.054 |
| Consolidations, % | 10.4 | 4.7 | 10 | 17.6 | 0.43 |
| Nodules, % | 50 | 28 | 60 | 76.4 * | 0.004 |
| Bronchiectasis, % | 12.5 | 4.7 | 20 | 17.6 | 0.43 |
| Airways thickening, % | 16.6 | 14.3 | 10 | 23.5 | 0.61 |
| Air trapping, % | 8.3 | - | 10 | 11.8 | 0.14 |
| Dependent Variable | Predictors | B | SE | OR | 95% CI | p | R2 |
|---|---|---|---|---|---|---|---|
| HRCT Abnormal (Yes) | SPD | 0.009 | 0.05 | 1.009 | 1.000–1.018 | 0.041 | |
| Reduced DLCO (No) | −2.94 | 1.26 | 0.053 | 0.04–0.63 | 0.02 | ||
| ACPA | 0.001 | 0.001 | 1.001 | 0.998–1.003 | 0.44 | ||
| V’E/V’CO2 at θL Impaired (No) | −0.65 | 1.32 | 0.52 | 0.039–6.9 | 0.62 | ||
| Constant | −0.629 | 1.477 | 0.53 | 0.67 | |||
| 0.506 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucchino, B.; Di Paolo, M.; Gioia, C.; Vomero, M.; Diacinti, D.; Mollica, C.; Alessandri, C.; Diacinti, D.; Palange, P.; Di Franco, M. Identification of Subclinical Lung Involvement in ACPA-Positive Subjects through Functional Assessment and Serum Biomarkers. Int. J. Mol. Sci. 2020, 21, 5162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21145162
Lucchino B, Di Paolo M, Gioia C, Vomero M, Diacinti D, Mollica C, Alessandri C, Diacinti D, Palange P, Di Franco M. Identification of Subclinical Lung Involvement in ACPA-Positive Subjects through Functional Assessment and Serum Biomarkers. International Journal of Molecular Sciences. 2020; 21(14):5162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21145162
Chicago/Turabian StyleLucchino, Bruno, Marcello Di Paolo, Chiara Gioia, Marta Vomero, Davide Diacinti, Cristina Mollica, Cristiano Alessandri, Daniele Diacinti, Paolo Palange, and Manuela Di Franco. 2020. "Identification of Subclinical Lung Involvement in ACPA-Positive Subjects through Functional Assessment and Serum Biomarkers" International Journal of Molecular Sciences 21, no. 14: 5162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21145162