Age-Related Differences in the Time Course of Coagulation and Fibrinolytic Parameters in Patients with Traumatic Brain Injury

 , and
, and
Abstract
:1. Introduction
2. Results
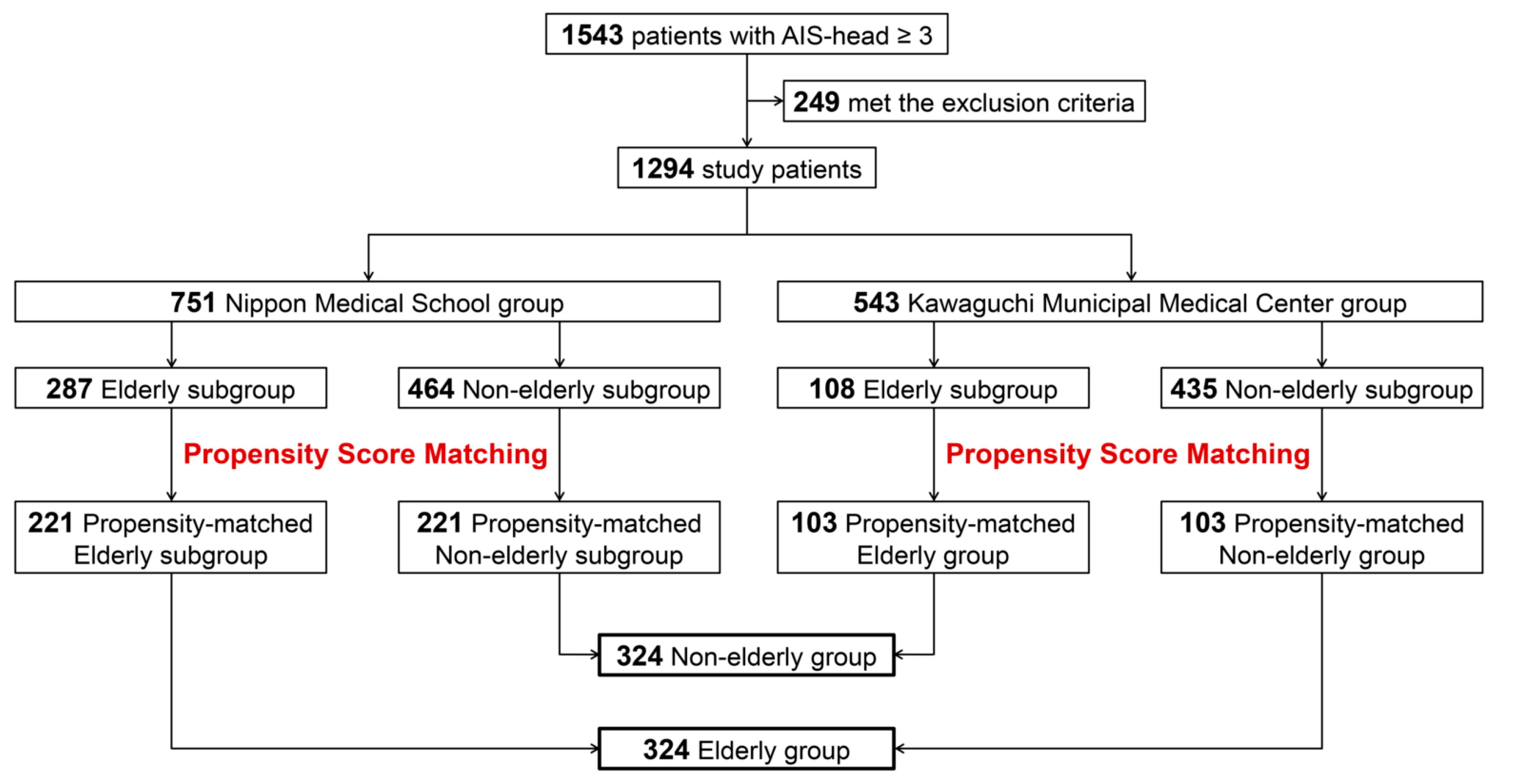
2.1. Case Selection
2.2. Relationship between Coagulation/Fibrinolytic Parameters and Age
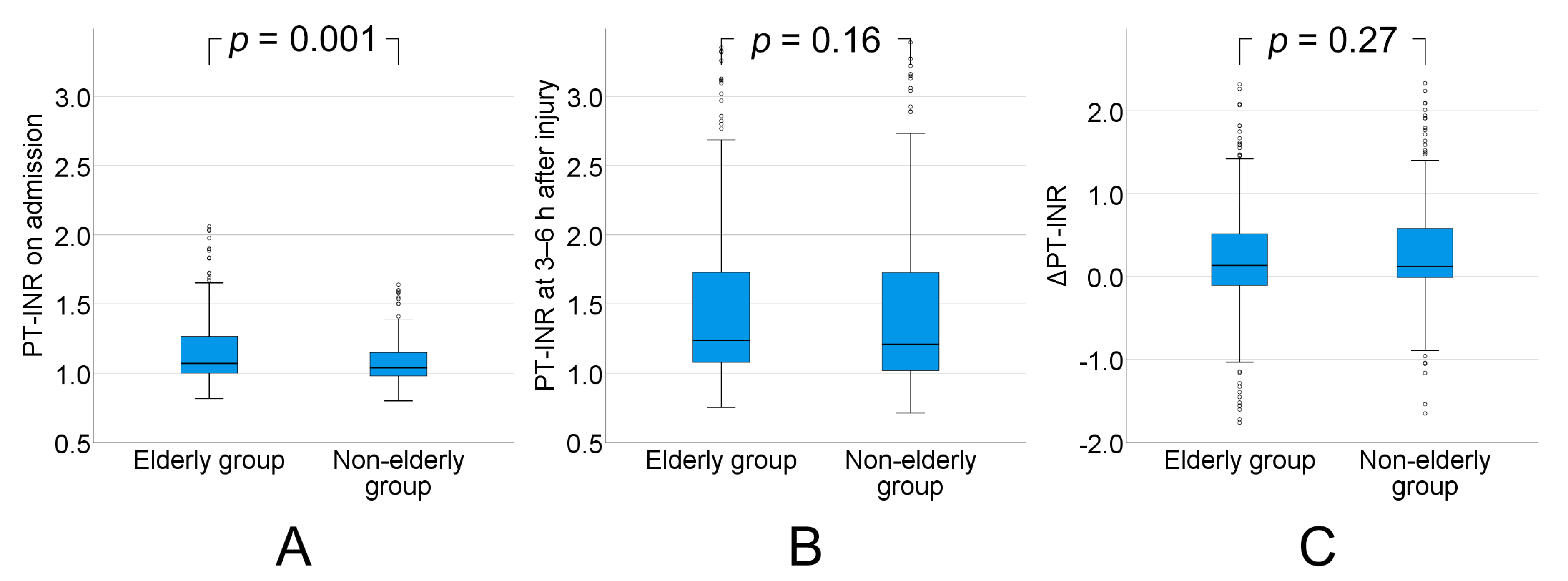
2.2.1. PT-INR
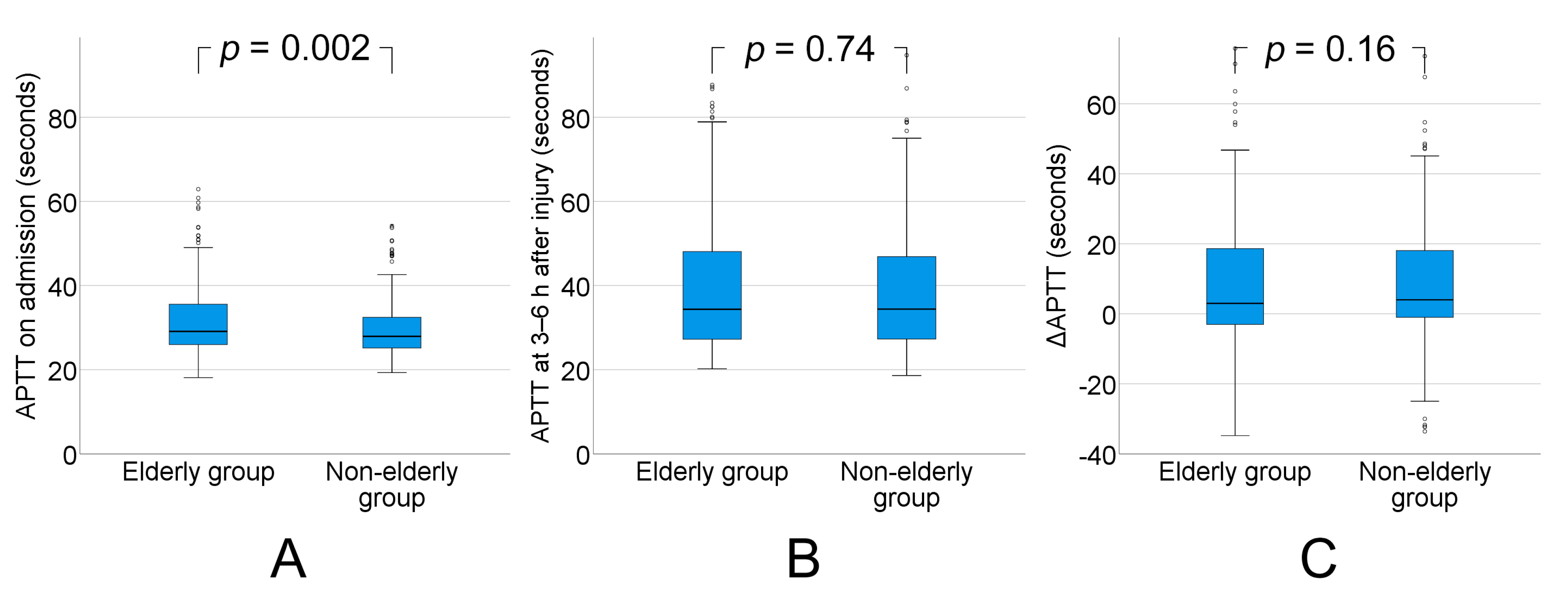
2.2.2. APTT
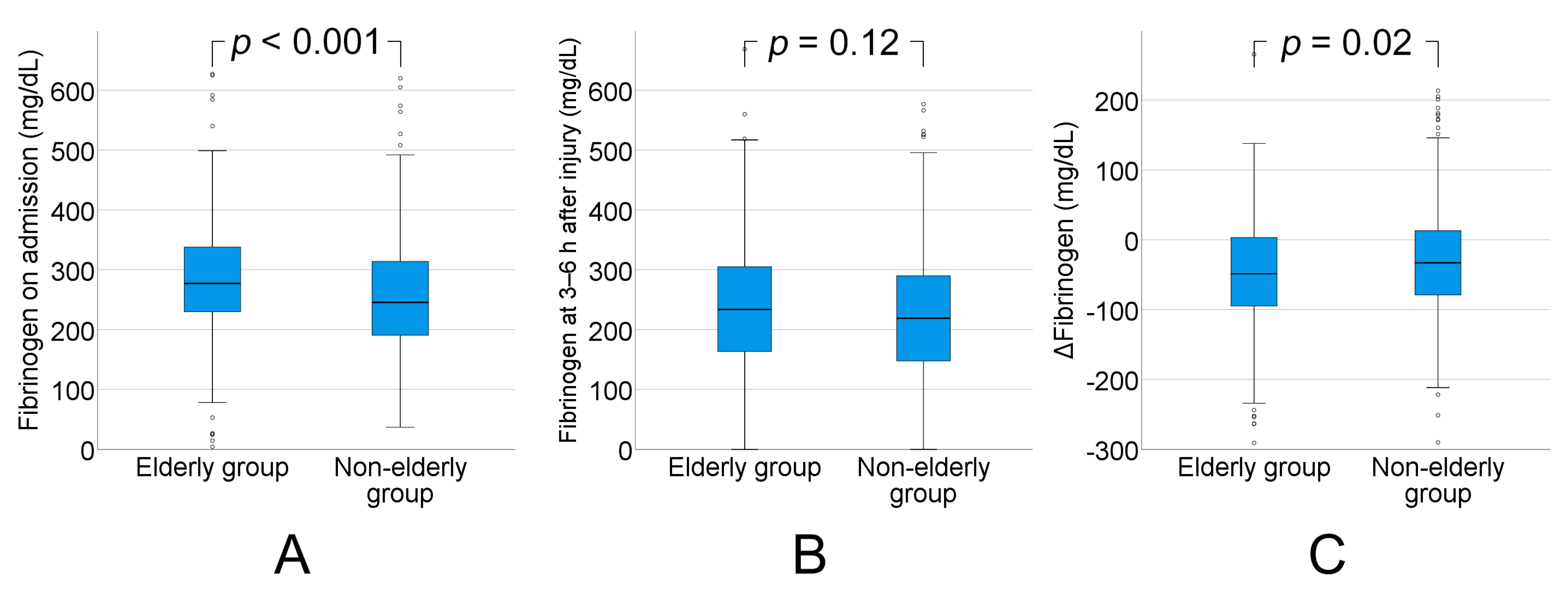
2.2.3. Fibrinogen
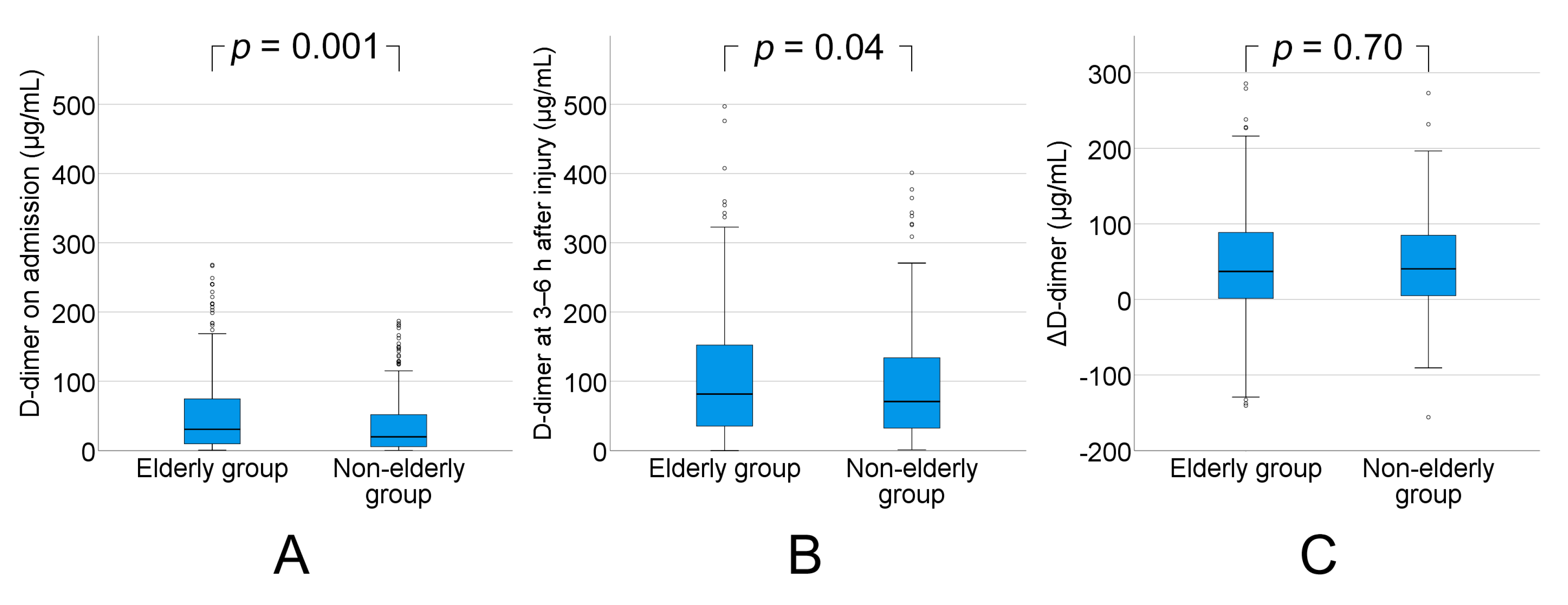
2.2.4. D-dimer
2.2.5. Correlation between Age and Outcome
2.2.6. Independent Risk Factors for Poor Prognosis at the Time of Admission
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Management of TBI
4.3. Assay of Coagulation/Fibrinolytic Parameters
4.4. Statistical Analysis
4.4.1. Propensity Score-Matched Analysis
4.4.2. Multivariate Logistic Regression Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| 95% CI | 95% confidence interval |
| AEDH | acute epidural hematoma |
| AIS | Abbreviated Injury Score |
| APTT | activated partial thromboplastin time |
| ASDH | acute subdural hematoma |
| CT | computed tomography |
| FFP | fresh frozen plasma |
| GCS | Glasgow Coma Scale |
| GOS | Glasgow Outcome Scale |
| IQR | interquartile range |
| ISS | Injury Severity Score |
| MRI | magnetic resonance imaging |
| PT-INR | prothrombin time-international normalized ratio |
| TBI | traumatic brain injury |
| TF | tissue factor |
| TICH | traumatic intracerebral hematoma/contusion |
| TSAH | traumatic subarachnoid hemorrhage |
| α2-PI | α2 plasmin inhibitor |
References
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Maegele, M.; Schochl, H.; Menovsky, T.; Marechal, H.; Marklund, N.; Buki, A.; Stanworth, S. Coagulopathy and haemorrhagic progression in traumatic brain injury: Advances in mechanisms, diagnosis, and management. Lancet Neurol. 2017, 16, 630–647. [Google Scholar] [CrossRef]
- Hukkelhoven, C.W.; Steyerberg, E.W.; Rampen, A.J.; Farace, E.; Habbema, J.D.; Marshall, L.F.; Murray, G.D.; Maas, A.I. Patient age and outcome following severe traumatic brain injury: An analysis of 5600 patients. J. Neurosurg. 2003, 99, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Epstein, D.S.; Mitra, B.; O’Reilly, G.; Rosenfeld, J.V.; Cameron, P.A. Acute traumatic coagulopathy in the setting of isolated traumatic brain injury: A systematic review and meta-analysis. Injury 2014, 45, 819–824. [Google Scholar] [CrossRef]
- Harhangi, B.S.; Kompanje, E.J.; Leebeek, F.W.; Maas, A.I. Coagulation disorders after traumatic brain injury. Acta Neurochir. (Wien.) 2008, 150, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Wafaisade, A.; Lefering, R.; Tjardes, T.; Wutzler, S.; Simanski, C.; Paffrath, T.; Fischer, P.; Bouillon, B.; Maegele, M.; Trauma Registry of, D.G.U. Acute coagulopathy in isolated blunt traumatic brain injury. Neurocrit. Care 2010, 12, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Nakae, R.; Takayama, Y.; Kuwamoto, K.; Naoe, Y.; Sato, H.; Yokota, H. Time course of coagulation and fibrinolytic parameters in patients with traumatic brain injury. J. Neurotrauma 2016, 33, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Nakae, R.; Yokobori, S.; Takayama, Y.; Kanaya, T.; Fujiki, Y.; Igarashi, Y.; Suzuki, G.; Naoe, Y.; Fuse, A.; Yokota, H. A retrospective study of the effect of fibrinogen levels during fresh frozen plasma transfusion in patients with traumatic brain injury. Acta Neurochir. (Wien.) 2019, 161, 1943–1953. [Google Scholar] [CrossRef]
- Nakae, R.; Yokobori, S.; Takayama, Y.; Kuwamoto, K.; Naoe, Y.; Yokota, H. Age-related differences in fibrinolytic parameters in patients with acute traumatic brain injury. Surg. Neurol. Int. 2017, 8, 214. [Google Scholar] [CrossRef] [Green Version]
- Ouchi, Y.; Rakugi, H.; Arai, H.; Akishita, M.; Ito, H.; Toba, K.; Kai, I. Joint Committee of Japan Gerontological Society (JGLS) and Japan Geriatrics Society (JGS) on the definition and classification of the elderly. Redefining the elderly as aged 75 years and older: Proposal from the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society. Geriatr. Gerontol. Int. 2017, 17, 1045–1047. [Google Scholar] [CrossRef] [Green Version]
- Keimowitz, R.M.; Annis, B.L. Disseminated intravascular coagulation associated with massive brain injury. J. Neurosurg. 1973, 39, 178–180. [Google Scholar] [CrossRef] [PubMed]
- Goodnight, S.H.; Kenoyer, G.; Rapaport, S.I.; Patch, M.J.; Lee, J.A.; Kurze, T. Defibrination after brain-tissue destruction: A serious complication of head injury. N. Engl. J. Med. 1974, 290, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Eddleston, M.; de la Torre, J.C.; Oldstone, M.B.; Loskutoff, D.J.; Edgington, T.S.; Mackman, N. Astrocytes are the primary source of tissue factor in the murine central nervous system. A role for astrocytes in cerebral hemostasis. J. Clin. Invest. 1993, 92, 349–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellino, F.J.; Chapman, M.P.; Donahue, D.L.; Thomas, S.; Moore, E.E.; Wohlauer, M.V.; Fritz, B.; Yount, R.; Ploplis, V.; Davis, P.; et al. Traumatic brain injury causes platelet adenosine diphosphate and arachidonic acid receptor inhibition independent of hemorrhagic shock in humans and rats. J. Trauma Acute Care Surg. 2014, 76, 1169–1176. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, M.; Monroe, D.M. Tissue factor in brain is not saturated with factor VIIa: Implications for factor VIIa dosing in intracerebral hemorrhage. Stroke 2009, 40, 2882–2884. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Xue, L.X.; Guo, Y.; Chen, S.W.; Wang, G.; Cao, H.L.; Chen, J.; Tian, H.L. The influence of hemocoagulation disorders on the development of posttraumatic cerebral infarction and outcome in patients with moderate or severe head trauma. Biomed. Res. Int. 2013, 2013, 685174. [Google Scholar] [CrossRef]
- Pahatouridis, D.; Alexiou, G.A.; Zigouris, A.; Mihos, E.; Drosos, D.; Voulgaris, S. Coagulopathy in moderate head injury. The role of early administration of low molecular weight heparin. Brain Inj. 2010, 24, 1189–1192. [Google Scholar] [CrossRef]
- Teraz-Orosz, A.; Csapo, A.; Bagoly, Z.; Szekely, E.G.; Toth, E.; Kovacs, B.; Bereczky, Z.; Muszbek, L.; Katona, E. A new ELISA method for the measurement of total alpha2-plasmin inhibitor level in human body fluids. J. Immunol. Methods 2019, 471, 27–33. [Google Scholar] [CrossRef]
- Kushimoto, S.; Yamamoto, Y.; Shibata, Y.; Sato, H.; Koido, Y. Implications of excessive fibrinolysis and alpha(2)-plasmin inhibitor deficiency in patients with severe head injury. Neurosurgery 2001, 49, 1084–1089. [Google Scholar] [CrossRef]
- Allard, C.B.; Scarpelini, S.; Rhind, S.G.; Baker, A.J.; Shek, P.N.; Tien, H.; Fernando, M.; Tremblay, L.; Morrison, L.J.; Pinto, R.; et al. Abnormal coagulation tests are associated with progression of traumatic intracranial hemorrhage. J. Trauma 2009, 67, 959–967. [Google Scholar] [CrossRef]
- Kurland, D.; Hong, C.; Aarabi, B.; Gerzanich, V.; Simard, J.M. Hemorrhagic progression of a contusion after traumatic brain injury: A review. J. Neurotrauma 2012, 29, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Stein, S.C.; Spettell, C.; Young, G.; Ross, S.E. Delayed and progressive brain injury in closed-head trauma: Radiological demonstration. Neurosurgery 1993, 32, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Balleisen, L.; Bailey, J.; Epping, P.H.; Schulte, H.; van de Loo, J. Epidemiological study on factor VII, factor VIII and fibrinogen in an industrial population: I. Baseline data on the relation to age, gender, body-weight, smoking, alcohol, pill-using, and menopause. Thromb. Haemost. 1985, 54, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Hager, K.; Felicetti, M.; Seefried, G.; Platt, D. Fibrinogen and aging. Aging (Milano) 1994, 6, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.T.; Yeung, V.T.; Chan, J.C.; Chow, C.C.; Li, J.K.; So, W.Y.; Tsang, L.W.; Cockram, C.S. Plasma fibrinogen concentration in a Chinese population. Atherosclerosis 1997, 131, 211–217. [Google Scholar] [CrossRef]
- Krobot, K.; Hense, H.W.; Cremer, P.; Eberle, E.; Keil, U. Determinants of plasma fibrinogen: Relation to body weight, waist-to-hip ratio, smoking, alcohol, age, and sex. Results from the second MONICA Augsburg survey 1989-1990. Arter. Thromb. 1992, 12, 780–788. [Google Scholar] [CrossRef] [Green Version]
- Wilkerson, W.R.; Sane, D.C. Aging and thrombosis. Semin. Thromb. Hemost. 2002, 28, 555–568. [Google Scholar] [CrossRef]
- Cadroy, Y.; Pierrejean, D.; Fontan, B.; Sie, P.; Boneu, B. Influence of aging on the activity of the hemostatic system: Prothrombin fragment 1 + 2, thrombin-antithrombin III complexes and D-dimers in 80 healthy subjects with age ranging from 20 to 94 years. Nouv. Rev. Fr. Hematol. 1992, 34, 43–46. [Google Scholar]
- Hager, K.; Platt, D. Fibrin degeneration product concentrations (D-dimers) in the course of ageing. Gerontology 1995, 41, 159–165. [Google Scholar] [CrossRef]
- Mari, D.; Mannucci, P.M.; Coppola, R.; Bottasso, B.; Bauer, K.A.; Rosenberg, R.D. Hypercoagulability in centenarians: The paradox of successful aging. Blood 1995, 85, 3144–3149. [Google Scholar] [CrossRef]
- Pieper, C.F.; Rao, K.M.; Currie, M.S.; Harris, T.B.; Cohen, H.J. Age, functional status, and racial differences in plasma D-dimer levels in community-dwelling elderly persons. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M649–M657. [Google Scholar] [CrossRef] [PubMed]
- Tita-Nwa, F.; Bos, A.; Adjei, A.; Ershler, W.B.; Longo, D.L.; Ferrucci, L. Correlates of D-dimer in older persons. Aging Clin. Exp. Res. 2010, 22, 20–23. [Google Scholar] [CrossRef]
- Yokota, H.; Atsumi, T.; Araki, T.; Fuse, A.; Sato, H.; Kushimoto, S.; Koido, Y.; Kawai, M.; Yamamoto, Y. Cerebral endothelial injury in elderly patients with severe head injury measured by serum thrombomodulin and von Willebrand factor. Neurol. Med. Chir. (Tokyo) 2007, 47, 383–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokota, H.; Naoe, Y.; Nakabayashi, M.; Unemoto, K.; Kushimoto, S.; Kurokawa, A.; Node, Y.; Yamamoto, Y. Cerebral endothelial injury in severe head injury: The significance of measurements of serum thrombomodulin and the von Willebrand factor. J. Neurotrauma 2002, 19, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.I.; Stensballe, J.; Rasmussen, L.S.; Ostrowski, S.R. A high admission syndecan-1 level, a marker of endothelial glycocalyx degradation, is associated with inflammation, protein C depletion, fibrinolysis, and increased mortality in trauma patients. Ann. Surg. 2011, 254, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Gando, S.; Nanzaki, S.; Kemmotsu, O. Coagulofibrinolytic changes after isolated head injury are not different from those in trauma patients without head injury. J. Trauma 1999, 46, 1070–1076. [Google Scholar] [CrossRef]
- Lustenberger, T.; Talving, P.; Kobayashi, L.; Inaba, K.; Lam, L.; Plurad, D.; Demetriades, D. Time course of coagulopathy in isolated severe traumatic brain injury. Injury 2010, 41, 924–928. [Google Scholar] [CrossRef]
- Association for the Advancement of Automotive Medicine. The Abbreviated Injury Scale (AIS) 1998 Revision; Association for the Advancement of Automotive Medicine: Des Plaines, IL, USA, 1998. [Google Scholar]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Guidelines Committee on the Management of Severe Head Injury, Japan Society of Neurotraumatology. Guidelines for the Management of Severe Head Injury, 3rd ed.; Igaku-Shoin Ltd.: Tokyo, Japan, 2013. (in Japanese) [Google Scholar]
- Shigemori, M.; Abe, T.; Aruga, T.; Ogawa, T.; Okudera, H.; Ono, J.; Onuma, T.; Katayama, Y.; Kawai, N.; Kawamata, T.; et al. Guidelines for the Management of Severe Head Injury, 2nd Edition guidelines from the Guidelines Committee on the Management of Severe Head Injury, the Japan Society of Neurotraumatology. Neurol. Med. Chir. (Tokyo) 2012, 52, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. The use of propensity score methods with survival or time-to-event outcomes: Reporting measures of effect similar to those used in randomized experiments. Stat. Med. 2014, 33, 1242–1258. [Google Scholar] [CrossRef] [Green Version]
- Meredith, J.W.; Evans, G.; Kilgo, P.D.; MacKenzie, E.; Osler, T.; McGwin, G.; Cohn, S.; Esposito, T.; Gennarelli, T.; Hawkins, M.; et al. A comparison of the abilities of nine scoring algorithms in predicting mortality. J. Trauma 2002, 53, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, S.C.; Langley, J.D.; Civil, I.D. Comparing measures of injury severity for use with large databases. J. Trauma 2002, 53, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Anglin, C.O.; Spence, J.S.; Warner, M.A.; Paliotta, C.; Harper, C.; Moore, C.; Sarode, R.; Madden, C.; Diaz-Arrastia, R. Effects of platelet and plasma transfusion on outcome in traumatic brain injury patients with moderate bleeding diatheses. J. Neurosurg. 2013, 118, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.M.; Li, R.; Zhao, X.C.; Zhang, Q.; Luo, X.L. Increased transfusion of fresh frozen plasma is associated with mortality or worse functional outcomes after severe traumatic brain injury: A retrospective study. World Neurosurg. 2017, 104, 381–389. [Google Scholar] [CrossRef]
- Katz, M.H. Multivariable analysis: A primer for readers of medical research. Ann. Intern. Med. 2003, 138, 644–650. [Google Scholar] [CrossRef]
- Kucuk, U.; Kucuk, H.O.; Eyuboglu, M.; Dogan, M. eComment. The importance of choosing a proper predictor variable selection method in logistic regression analyses. Interact. Cardiovasc. Thorac. Surg. 2016, 22, 258. [Google Scholar] [CrossRef] [Green Version]
- Jennett, B.; Snoek, J.; Bond, M.R.; Brooks, N. Disability after severe head injury: Observations on the use of the Glasgow Outcome Scale. J. Neurol. Neurosurg. Psychiatry 1981, 44, 285–293. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Unmatched Subgroups | Matched Subgroups | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Elderly Subgroup (n = 287) | Non-Elderly Subgroup (n = 464) | Standardized Mean difference | Elderly Subgroup (n = 221) | Non-Elderly Subgroup (n = 221) | Standardized Mean Difference | |||||
| Male, n (%) | 167 | (58.2) | 374 | (80.6) | −0.512 | 150 | (67.9) | 153 | (69.2) | −0.022 |
| GCS Score | 13 | (9–15) | 13 | (7–14) | 0.119 | 13 | (9–15) | 13 | (8–15) | 0.024 |
| ASDH, n (%) | 197 | (68.6) | 252 | (54.3) | 0.305 | 147 | (66.5) | 139 | (62.9) | 0.084 |
| AEDH, n (%) | 33 | (11.5) | 78 | (16.8) | −0.169 | 27 | (12.2) | 24 | (10.9) | 0.031 |
| TICH, n (%) | 137 | (47.7) | 237 | (51.1) | −0.060 | 107 | (48.4) | 98 | (42.1) | 0.080 |
| TSAH, n (%) | 156 | (54.4) | 298 | (64.2) | −0.204 | 129 | (58.4) | 132 | (59.7) | −0.041 |
| AIS-head | 4 | (4–5) | 4 | (3–5) | 0.170 | 4 | (4–5) | 4 | (4–5) | 0.013 |
| AIS-face | 0 | (0–0) | 0 | (0–0) | −0.333 | 0 | (0–0) | 0 | (0–0) | 0.028 |
| AIS-chest | 0 | (0–0) | 0 | (0–3) | −0.414 | 0 | (0–0) | 0 | (0–0) | −0.024 |
| AIS-abdomen | 0 | (0–0) | 0 | (0–0) | −0.333 | 0 | (0–0) | 0 | (0–0) | 0.000 |
| AIS-extremities | 0 | (0–0) | 0 | (0–2) | −0.236 | 0 | (0–0) | 0 | (0–1) | −0.058 |
| AIS-external | 0 | (0–1) | 0 | (0–1) | 0.021 | 0 | (0–1) | 0 | (0–1) | 0.087 |
| ISS | 20 | (16–25) | 25 | (16–29) | −0.288 | 20 | (16–25) | 21 | (16–26) | −0.042 |
| FFP (mL) | 0 | (0–0) | 0 | (0–0) | −0.010 | 0 | (0–0) | 0 | (0–0) | −0.020 |
| Variable | Unmatched Subgroups | Matched Subgroups | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Elderly Subgroup (n = 108) | Non-Elderly Subgroup (n = 435) | Standardized Mean difference | Elderly Subgroup (n = 103) | Non-Elderly Subgroup (n = 103) | Standardized Mean Difference | |||||
| Male, n (%) | 55 | (50.9) | 330 | (75.9) | −0.549 | 55 | (53.4) | 55 | (53.4) | 0.000 |
| GCS Score | 8 | (4–14) | 10 | (6–14) | −0.125 | 8 | (4–14) | 9 | (6–13) | −0.098 |
| ASDH, n (%) | 85 | (78.7) | 255 | (58.6) | 0.413 | 80 | (77.7) | 78 | (75.7) | 0.047 |
| AEDH, n (%) | 7 | (6.5) | 92 | (21.1) | −0.389 | 7 | (6.8) | 6 | (5.8) | 0.041 |
| TICH, n (%) | 81 | (75.0) | 324 | (74.5) | 0.023 | 77 | (74.8) | 80 | (77.7) | −0.070 |
| TSAH, n (%) | 91 | (84.3) | 357 | (82.1) | 0.053 | 86 | (83.5) | 88 | (85.4) | −0.055 |
| AIS-head | 4 | (4–5) | 4 | (3–5) | 0.282 | 4 | (4–5) | 4 | (4–5) | −0.056 |
| AIS-face | 0 | (0–0) | 0 | (0–0) | −0.234 | 0 | (0–0) | 0 | (0–0) | −0.077 |
| AIS-chest | 0 | (0–3) | 0 | (0–3) | 0.025 | 0 | (0–3) | 0 | (0–3) | −0.080 |
| AIS-abdomen | 0 | (0–0) | 0 | (0–0) | −0.137 | 0 | (0–0) | 0 | (0–0) | −0.051 |
| AIS-extremities | 0 | (0–2) | 0 | (0–1) | 0.051 | 0 | (0–1) | 0 | (0–1) | 0.025 |
| AIS-external | 0 | (0–1) | 1 | (0–1) | −0.176 | 0 | (0–1) | 0 | (0–1) | −0.080 |
| ISS | 25 | (18–29) | 25 | (16–30) | 0.116 | 25 | (17–29) | 25 | (18–33) | −0.097 |
| FFP (mL) | 0 | (0–770) | 0 | (0–0) | 0.246 | 0 | (0–560) | 0 | (0–0) | 0.080 |
| GOS | Elderly Group (n = 324) | Non-Elderly Group (n = 324) | p Value | ||
|---|---|---|---|---|---|
| 4–5, n (%) | 166 | (51.2) | 202 | (62.3) | 0.004 |
| 1–3, n (%) | 158 | (48.8) | 122 | (37.7) | |
| Factor | Odds Ratio (95% CI) | p Value | |
|---|---|---|---|
| Age (10-y increments) | 1.46 | (1.26–1.69) | <0.001 |
| Male | 1.02 | (0.62–1.68) | 0.93 |
| GCS score (1-point decrements) | 1.38 | (1.29–1.48) | <0.001 |
| AIS-head (1-point increments) | 2.42 | (1.52–3.86) | <0.001 |
| ISS (1-point increments) | 1.09 | (1.05–1.12) | <0.001 |
| ASDH | 1.85 | (0.96–3.57) | 0.07 |
| AEDH | 0.41 | (0.19–0.92) | 0.03 |
| TICH | 1.69 | (1.03–2.79) | 0.04 |
| TSAH | 1.42 | (0.85–2.35) | 0.18 |
| PT (0.1-INR increments) | 1.01 | (0.99–1.02) | 0.30 |
| APTT (1-s increments) | 1.01 | (0.99–1.04) | 0.36 |
| Fibrinogen (10-mg/dL decrements) | 1.04 | (1.01–1.06) | 0.001 |
| D-dimer (10-μg/mL increments) | 1.08 | (1.02–1.13) | 0.006 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakae, R.; Fujiki, Y.; Takayama, Y.; Kanaya, T.; Igarashi, Y.; Suzuki, G.; Naoe, Y.; Yokobori, S. Age-Related Differences in the Time Course of Coagulation and Fibrinolytic Parameters in Patients with Traumatic Brain Injury. Int. J. Mol. Sci. 2020, 21, 5613. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21165613
Nakae R, Fujiki Y, Takayama Y, Kanaya T, Igarashi Y, Suzuki G, Naoe Y, Yokobori S. Age-Related Differences in the Time Course of Coagulation and Fibrinolytic Parameters in Patients with Traumatic Brain Injury. International Journal of Molecular Sciences. 2020; 21(16):5613. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21165613
Chicago/Turabian StyleNakae, Ryuta, Yu Fujiki, Yasuhiro Takayama, Takahiro Kanaya, Yutaka Igarashi, Go Suzuki, Yasutaka Naoe, and Shoji Yokobori. 2020. "Age-Related Differences in the Time Course of Coagulation and Fibrinolytic Parameters in Patients with Traumatic Brain Injury" International Journal of Molecular Sciences 21, no. 16: 5613. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21165613