Anti-Telomerase CD4+ Th1 Immunity and Monocytic-Myeloid-Derived-Suppressor Cells Are Associated with Long-Term Efficacy Achieved by Docetaxel, Cisplatin, and 5-Fluorouracil (DCF) in Advanced Anal Squamous Cell Carcinoma: Translational Study of Epitopes-HPV01 and 02 Trials

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Magnitude of Anti-Telomerase (hTERT)-Specific T Helper 1 (TH1) Response was Increased in SCCA Patients Following DCF Chemotherapy
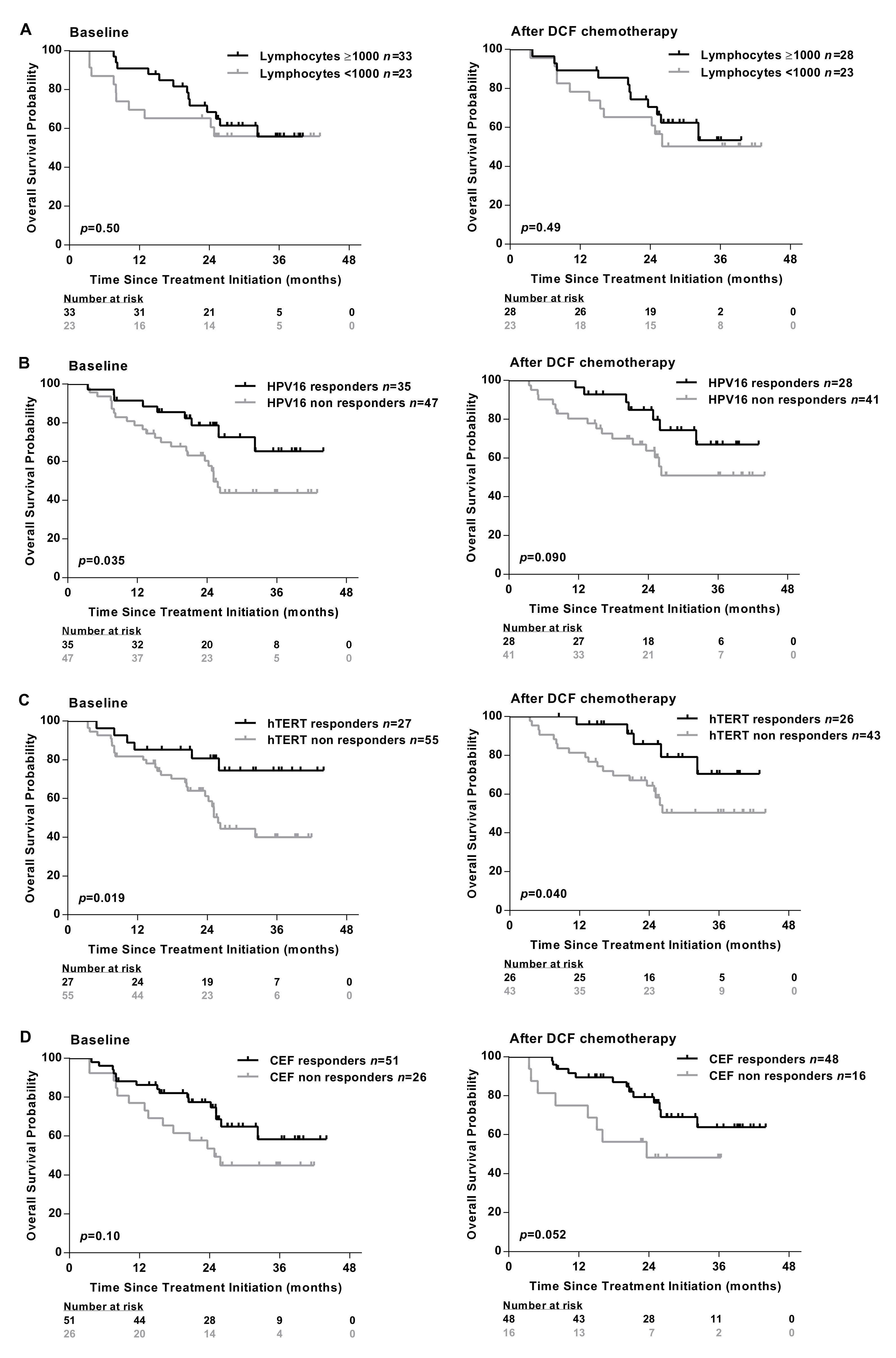
2.2. Peripheral Antigen-Specific T Cells Are Correlated with SCCA Patients’ Survival
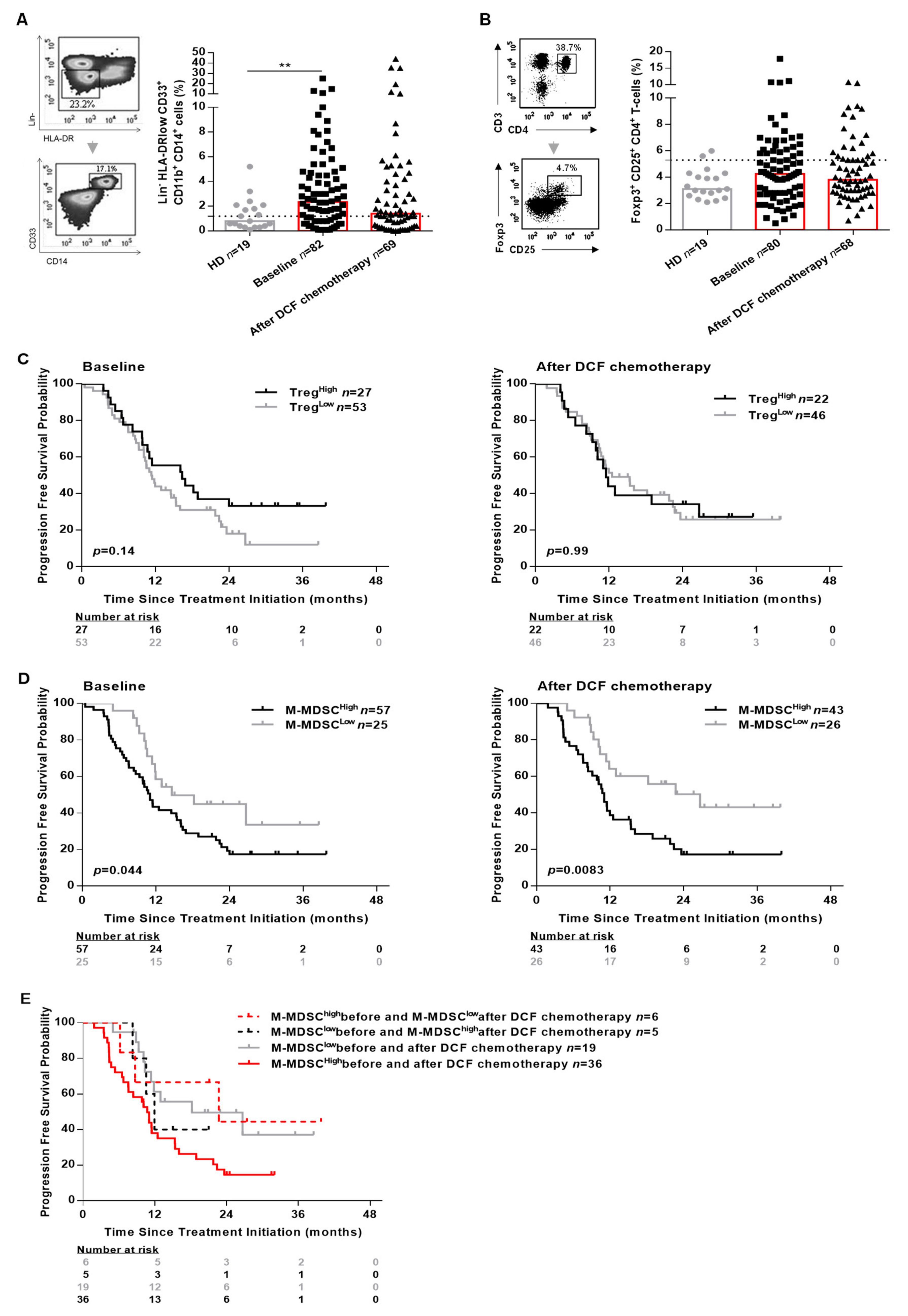
2.3. Influence of Peripheral Monocytic Myeloid-Derived Suppressive Cells (M-MDSC) and Regulatory CD4+ T-Cells (Treg) on the Clinical Outcomes of SCCA Patients
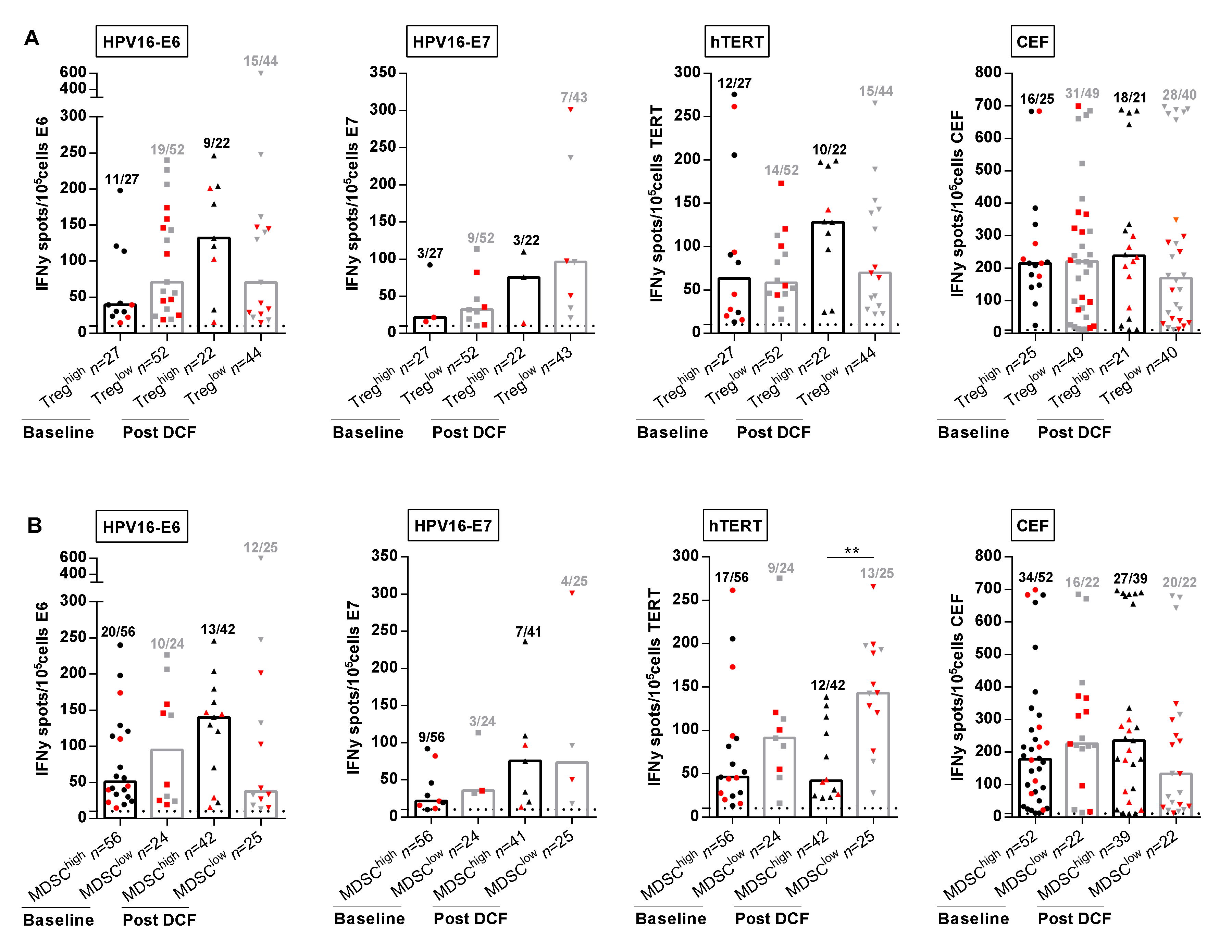
2.4. DCF Chemotherapy Alleviated M-MDSC Suppression of hTERT TH1 Immunity
3. Discussion
4. Methods
4.1. Study Design and Participants
4.2. Synthetic Peptides
4.3. Assessment of Antigen Specific T-Cell Responses in Healthy Donors and SCCA Patients
4.4. ELISpot Assay
4.5. Flow Cytometry
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Islami, F.; Ferlay, J.; Lortet-Tieulent, J.; Bray, F.; Jemal, A. International trends in anal cancer incidence rates. Int. J. Epidemiol. 2016, 46, dyw276. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Franceschi, S.; Clifford, G.M. Human papillomavirus types from infection to cancer in the anus, according to sex and HIV status: A systematic review and meta-analysis. Lancet Infect. Dis. 2018, 18, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.C.; François, E.; André, T.; Samalin, E.; Jary, M.; El Hajbi, F.; Baba-Hamed, N.; Pernot, S.; Kaminsky, M.-C.; Bouché, O.; et al. Docetaxel, cisplatin, and fluorouracil chemotherapy for metastatic or unresectable locally recurrent anal squamous cell carcinoma (Epitopes-HPV02): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 1094–1106. [Google Scholar] [CrossRef]
- Kim, S.; Meurisse, A.; Stouvenot, M.; Jary, M.; Hon, T.N.T.; Francois, E.; Buecher, B.; Andre, T.; Samalin, E.; Boulbair, F.; et al. Updated data of epitopes-HPV02 trial and external validation of efficacy of DCF in prospective epitopes-HPV01 study in advanced anal squamous cell carcinoma. Pooled analysis of 115 patients. Ann. Oncol. 2019, 30, v203. [Google Scholar] [CrossRef]
- Bezu, L.; Da Silva, L.C.G.; Dewitte, H.; Breckpot, K.; Fučíková, J.; Spisek, R.; Galluzzi, L.; Kepp, O.; Kroemer, G. Combinatorial strategies for the induction of immunogenic cell death. Front. Immunol. 2015, 6, 187. [Google Scholar] [CrossRef]
- Galluzzi, L.; Buqué, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Yuan, H.; Fu, B.; Disbrow, G.L.; Apolinario, T.; Tomaić, V.; Kelley, M.L.; Baker, C.C.; Huibregtse, J.; Schlegel, R. The E6AP ubiquitin ligase is required for transactivation of the hTERT promoter by the human papillomavirus E6 oncoprotein. J. Biol. Chem. 2005, 280, 10807–10816. [Google Scholar] [CrossRef] [Green Version]
- Godet, Y.; Fabre, E.; Dosset, M.; Lamuraglia, M.; Levionnois, E.; Ravel, P.; Benhamouda, N.; Cazes, A.; Le Pimpec-Barthes, F.; Gaugler, B.; et al. Analysis of spontaneous tumor-specific CD4 T-cell immunity in lung cancer using promiscuous HLA-DR telomerase-derived epitopes: Potential synergistic effect with chemotherapy response. Clin. Cancer Res. 2012, 18, 2943–2953. [Google Scholar] [CrossRef] [Green Version]
- Mandruzzato, S.; Brandau, S.; Britten, C.M.; Bronte, V.; Damuzzo, V.; Gouttefangeas, C.; Maurer, D.; Ottensmeier, C.H.; Van Der Burg, S.H.; Welters, M.J.P.; et al. Toward harmonized phenotyping of human myeloid-derived suppressor cells by flow cytometry: Results from an interim study. Cancer Immunol. Immunother. 2016, 65, 161–169. [Google Scholar] [CrossRef]
- Visser, J.T.J.; Nijman, H.W.; Hoogenboom, B.; Jager, P.; Van Baarle, D.; Schuuring, E.; Abdulahad, W.; Miedema, F.; Van Der Zee, A.G.; Daemen, T. Frequencies and role of regulatory T cells in patients with (pre)malignant cervical neoplasia. Clin. Exp. Immunol. 2007, 150, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, V.K.; Salem, M.E.; Nimeiri, H.; Iqbal, S.; Singh, P.; Ciombor, K.; Polite, B.; Deming, D.; Chan, E.; Wade, J.L.; et al. Nivolumab for previously treated unresectable metastatic anal cancer (NCI9673): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Ott, P.A.; Piha-Paul, S.; Munster, P.; Pishvaian, M.J.; Van Brummelen, E.M.J.; Cohen, R.B.; Gomez-Roca, C.; Ejadi, S.; Stein, M.; Chan, E.; et al. Safety and antitumor activity of the anti-PD-1 antibody pembrolizumab in patients with recurrent carcinoma of the anal canal. Ann. Oncol. 2017, 28, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Galaine, J.; Turco, C.; Vauchy, C.; Royer, B.; Mercier-Letondal, P.; Queiroz, L.; Loyon, R.; Mouget, V.; Boidot, R.; Laheurte, C.; et al. CD4 T cells target colorectal cancer antigens upregulated by oxaliplatin. Int. J. Cancer 2019, 145, 3112–3125. [Google Scholar] [CrossRef] [PubMed]
- Laheurte, C.; Dosset, M.; Vernerey, D.; Boullerot, L.; Gaugler, B.; Gravelin, E.; Kaulek, V.; Jacquin, M.; Cuche, L.; Eberst, G.; et al. Distinct prognostic value of circulating anti-telomerase CD4+ Th1 immunity and exhausted PD-1+/TIM-3+ T cells in lung cancer. Br. J. Cancer 2019, 121, 405–416. [Google Scholar] [CrossRef] [Green Version]
- Zelba, H.; Weide, B.; Martens, A.; Derhovanessian, E.; Bailur, J.K.; Kyzirakos, C.; Pflugfelder, A.; Eigentler, T.; Di Giacomo, A.M.; Maio, M.; et al. Circulating CD4+ T cells that produce IL4 or IL17 when stimulated by melan-A but not by NY-ESO-1 have negative impacts on survival of patients with stage IV melanoma. Clin. Cancer Res. 2014, 20, 4390–4399. [Google Scholar] [CrossRef] [Green Version]
- Weide, B.; Zelba, H.; Derhovanessian, E.; Pflugfelder, A.; Eigentler, T.; Di Giacomo, A.M.; Maio, M.; Aarntzen, E.H.J.G.; De Vries, I.J.M.; Sucker, A.; et al. Functional T cells targeting NY-ESO-1 or Melan-A are predictive for survival of patients with distant melanoma metastasis. J. Clin. Oncol. 2012, 30, 1835–1841. [Google Scholar] [CrossRef]
- Masterson, L.M.; Lechner, M.; Loewenbein, S.; Mohammed, H.; Davies-Husband, C.; Fenton, T.R.; Sudhoff, H.; Jani, P.; Goon, P.; Sterling, J. CD8 + T cell response to human papillomavirus 16 E7 is able to predict survival outcome in oropharyngeal cancer. Eur. J. Cancer 2016, 67, 141–151. [Google Scholar] [CrossRef]
- Zhang, Y.; Dakic, A.; Chen, R.; Dai, Y.; Schlegel, R.; Liu, X. Direct HPV E6/Myc interactions induce histone modifications, Pol II phosphorylation, and hTERT promoter activation. Oncotarget 2017, 8, 96323–96339. [Google Scholar] [CrossRef] [Green Version]
- Stevanovic, S.; Pasetto, A.; Helman, S.R.; Gartner, J.J.; Prickett, T.D.; Howie, B.; Robins, H.; Robbins, P.F.; Klebanoff, C.A.; Rosenberg, S.A.; et al. Landscape of immunogenic tumor antigens in successful immunotherapy of virally induced epithelial cancer. Science 2017, 356, 200–205. [Google Scholar] [CrossRef]
- Lyford-Pike, S.; Peng, S.; Young, G.D.; Taube, J.M.; Westra, W.H.; Akpeng, B.; Bruno, T.C.; Richmon, J.D.; Wang, H.; Bishop, J.A.; et al. Evidence for a role of the PD-1:PD-L1 pathway in immune resistance of HPV-associated head and neck squamous cell carcinoma. Cancer Res. 2013, 73, 1733–1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badoual, C.; Hans, S.; Merillon, N.; Van Ryswick, C.; Ravel, P.; Benhamouda, N.; Levionnois, E.; Nizard, M.; Si-Mohamed, A.; Besnier, N.; et al. PD-1–expressing tumor-infiltrating T cells are a favorable prognostic biomarker in HPV-associated head and neck cancer. Cancer Res. 2012, 73, 128–138. [Google Scholar] [CrossRef] [Green Version]
- Ichihara, F.; Kono, K.; Takahashi, A.; Kawaida, H.; Sugai, H.; Fujii, H. Increased populations of regulatory T cells in peripheral blood and tumor-infiltrating lymphocytes in patients with gastric and esophageal cancers. Clin. Cancer Res. 2003, 9, 4404–4408. [Google Scholar] [PubMed]
- Zeng, C.; Yao, Y.; Jie, W.; Zhang, M.; Hu, X.; Zhao, Y.; Wang, S.; Yin, J.; Song, Y. Up-regulation of Foxp3 participates in progression of cervical cancer. Cancer Immunol. Immunother. 2012, 62, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Curiel, T.J.; Coukos, G.; Zou, L.; Alvarez, X.; Cheng, P.; Mottram, P.; Evdemon-Hogan, M.; Conejo-Garcia, J.R.; Zhang, L.; Burow, M.; et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat. Med. 2004, 10, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Parikh, F.; Duluc, D.; Imai, N.; Clark, A.; Misiukiewicz, K.; Bonomi, M.; Gupta, V.; Patsias, A.; Parides, M.; Demicco, E.G.; et al. Chemoradiotherapy-induced upregulation of PD-1 antagonizes immunity to HPV-related oropharyngeal cancer. Cancer Res. 2014, 74, 7205–7216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodge, J.W.; Garnett-Benson, C.; Farsaci, B.; Palena, C.; Tsang, K.-Y.; Ferrone, S.; Gameiro, S.R. Chemotherapy-induced immunogenic modulation of tumor cells enhances killing by cytotoxic T lymphocytes and is distinct from immunogenic cell death. Int. J. Cancer 2013, 133, 624–636. [Google Scholar] [CrossRef]
- Bruchard, M.; Mignot, G.; Dérangère, V.; Chalmin, F.; Chevriaux, A.; Végran, F.; Boireau, W.; Simon, B.; Ryffel, B.; Connat, J.L.; et al. Chemotherapy-triggered cathepsin B release in myeloid-derived suppressor cells activates the Nlrp3 inflammasome and promotes tumor growth. Nat. Med. 2012, 19, 57–64. [Google Scholar] [CrossRef]
- Limagne, E.; Euvrard, R.; Thibaudin, M.; Rébé, C.; Derangere, V.; Chevriaux, A.; Boidot, R.; Végran, F.; Bonnefoy, N.; Vincent, J.; et al. Accumulation of MDSC and Th17 cells in patients with metastatic colorectal cancer predicts the efficacy of a FOLFOX–bevacizumab drug treatment regimen. Cancer Res. 2016, 76, 5241–5252. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.C.; Buecher, B.; André, T.; Jary, M.; Bidard, F.-C.; Ghiringhelli, F.; François, É.; Taieb, J.; Smith, D.; De La Fouchardière, C.; et al. Atezolizumab plus modified docetaxel-cisplatin-5-fluorouracil (mDCF) regimen versus mDCF in patients with metastatic or unresectable locally advanced recurrent anal squamous cell carcinoma: A randomized, non-comparative phase II SCARCE GERCOR trial. BMC Cancer 2020, 20, 352. [Google Scholar] [CrossRef] [Green Version]
- Laheurte, C.; Galaine, J.; Beziaud, L.; Dosset, M.; Kerzerho, J.; Jacquemard, C.; Gaugler, B.; Ferrand, C.; Dormoy, A.; Aubin, F.; et al. Immunoprevalence and magnitude of HLA-DP4 versus HLA-DR-restricted spontaneous CD4+ Th1 responses against telomerase in cancer patients. OncoImmunology 2016, 5, e1137416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hothorn, T.; Lausen, B. On the exact distribution of maximally selected rank statistics. Comput. Stat. Data Anal. 2003, 43, 121–137. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population n = 82 | HPV Non Responders n = 47 | HPV Responders n = 35 | p-Value * | hTERT Non Responders n = 55 | hTERT Responders n = 27 | p-Value ** | |
|---|---|---|---|---|---|---|---|
| Genre | |||||||
| Female | 63 (76.8%) | 37 (78.7%) | 26 (74.3%) | 0.64 | 42 (76.4%) | 21 (77.8%) | 0.88 |
| Male | 19 (23.2%) | 10 (21.3%) | 9 (25.7%) | 13 (23.6%) | 6 (22.2%) | ||
| Age | |||||||
| Median [IQR] | 60.0 [38.6–84.0] | 59.4 [38.6–78.4] | 61.7 [41.1–84.0] | 0.27 | 60.1 [38.6–84.0] | 59.5 [44.2–78.4] | 0.81 |
| ECOG | |||||||
| 0 | 53 (64.6%) | 31 (66.0%) | 22 (62.9%) | 0.89 | 36 (65.4%) | 17 (63.0%) | 0.87 |
| 1 | 28 (34.2%) | 15 (31.9%) | 13 (37.1%) | 18 (32.7%) | 10 (37.0%) | ||
| 2 | 1 (1.2%) | 1 (2.1%) | 0 (0.0%) | 1 (1.8%) | 0 (0.0%) | ||
| HIV positif | |||||||
| Positive | 78 (95.1%) | 44 (93.6%) | 34 (97.1%) | 0.63 | 52 (94.5%) | 26 (96.3%) | 1.0 |
| Negative | 4 (4.9%) | 3 (6.4%) | 1 (2.9%) | 3 (5.6%) | 1 (3.7%) | ||
| Stage | |||||||
| Locally advanced | 17 (20.7%) | 10 (21.3%) | 7 (20.0%) | 0.71 | 12 (21.8%) | 5 (18.5%) | 0.34 |
| Synchronous metastases | 22 (26.8%) | 11 (23.4%) | 11 (31.4%) | 12 (21.8%) | 10 (37.0%) | ||
| Metachronous metastases | 43 (52.4%) | 26 (55.3%) | 17 (48.6%) | 31 (56.4%) | 12 (44.4%) | ||
| Number of sites involved | |||||||
| Median [IQR] | 2.0 [1.0–8.0] | 2.0 [1.0–8.0] | 2.0 [1.0–5.0] | 0.84 | 2.0 [1.0–8.0] | 2.0 [1.0–5.0] | 0.65 |
| Previous Chemoradiotherapy | (n = 48) | (n = 29) | (n = 19) | (n = 36) | (n = 11) | ||
| MMC + Cape/5FU | 36 (78.3%) | 22 (75.9%) | 14 (82.3%) | 0.34 | 26 (74.3%) | 10 (90.9%) | 0.38 |
| CDDP + 5FU | 6 (13.0%) | 5 (17.2%) | 1 (5.9%) | 6 (17.1%) | 0 (0.0%) | ||
| Capecitabine | 1 (2.2%) | 1 (3.4%) | 0 (0.0%) | 1 (2.9%) | 0 (0.0%) | ||
| Missing | 2 | 0 | 2 | 1 | 1 | ||
| RT without CT | |||||||
| No | 73 (93.6%) | 41 (93.2%) | 32 (94.1%) | 1.0 | 51 (96.2%) | 22 (88.0%) | 0.32 |
| Yes | 5 (6.4%) | 3 (6.8%) | 2 (5.9%) | 2 (3.8%) | 3 (12.0%) | ||
| Missing | 4 | 3 | 1 | 2 | 2 | ||
| Absolute lymphocyte count | (n = 59) | (n = 35) | (n = 21) | (n = 37) | (n = 19) | ||
| Median [IQR] | 1086.0 [860.0–1700.0] | 1159.0 [875.0–1927.0] | 1019.0 [850.0–1411.0] | 0.28 | 1159.0 [820.0–1869.0] | 1019.0 [875.0–1600.0] | 0.56 |
| Immune checkpoints expression on CD4 T-cells | |||||||
| OX40 | 14.5 [9.6–24.1] | 13.7 [7.4–20.8] | 17.6 [9.5–26.7] | 0.27 | 13.2 [7.9–23.3] | 17.6 [9.5–26.6] | 0.35 |
| CD226+ TIGIT− | 34.1 [24.1–44.3] | 32.8 [23.9–42.8] | 35.0 [24.1–44.8] | 0.79 | 34.4 [24.2–42.4] | 31.5 [23.6–45.1] | 0.81 |
| CD226+ TIGIT+ | 12.2 [7.9–17.0] | 11.5 [7.8–15.8] | 14.5 [8.8–18.9] | 0.12 | 12.1 [7.9–13.2] | 14.2 [7.4–20.6] | 0.36 |
| CD226− TIGIT+ | 8.1 [5.6–10.6] | 7.8 [5.4–9.8] | 8.3 [6.4–11.3] | 0.27 | 8.1 [5.6–10.8] | 7.7 [6.4–10.1] | 0.93 |
| PD-1 | 8.6 [6.0–13.0] | 8.9 [5.8–14.2] | 8.9 [6.7–12.3] | 0.79 | 9.4 [6.1–13.5] | 8.1 [5.0–11.8] | 0.37 |
| Missing | 0 | 1 | 1 | 1 | 1 | ||
| Immune checkpoints expression on CD8 T-cells | |||||||
| 4-1BB | 0.1 [0.0–0.3] | 0.1 [0.0–0.4] | 0.1 [0.0–0.2] | 0.41 | 0.1 [0.0–0.4] | 0.1 [0.0–0.2] | 0.18 |
| CD226+ TIGIT− | 36.6 [22.0–49.1] | 39.3 [23.0–47.3] | 35.9 [21.0–52.4] | 0.82 | 39.7 [23.3–54.2] | 27.4 [21.0–42.4] | 0.05 |
| CD226+ TIGIT+ | 17.6 [10.4–27.5] | 17.8 [10.3–26.3] | 16.1 [10.3–24.6] | 0.71 | 14.7 [8.7–28.6] | 17.2 [14.0–29.4] | 0.24 |
| CD226− TIGIT+ | 15.9 [9.5–28.8] | 14.7 [9.3–28.0] | 19.0 [10.7–28.8] | 0.28 | 16.3 [9.6–23.0] | 19.3 [12.9–34.4] | 0.06 |
| PD-1 | 5.0 [3.3–8.7] | 5.3 [3.8–9.4] | 4.8 [2.6–7.9] | 0.12 | 5.0 [3.6–8.8] | 5.1 [2.9–8.9] | 0.83 |
| Missing | 0 | 1 | 1 | 1 | 1 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spehner, L.; Kim, S.; Vienot, A.; François, E.; Buecher, B.; Adotevi, O.; Vernerey, D.; Abdeljaoued, S.; Meurisse, A.; Borg, C. Anti-Telomerase CD4+ Th1 Immunity and Monocytic-Myeloid-Derived-Suppressor Cells Are Associated with Long-Term Efficacy Achieved by Docetaxel, Cisplatin, and 5-Fluorouracil (DCF) in Advanced Anal Squamous Cell Carcinoma: Translational Study of Epitopes-HPV01 and 02 Trials. Int. J. Mol. Sci. 2020, 21, 6838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186838
Spehner L, Kim S, Vienot A, François E, Buecher B, Adotevi O, Vernerey D, Abdeljaoued S, Meurisse A, Borg C. Anti-Telomerase CD4+ Th1 Immunity and Monocytic-Myeloid-Derived-Suppressor Cells Are Associated with Long-Term Efficacy Achieved by Docetaxel, Cisplatin, and 5-Fluorouracil (DCF) in Advanced Anal Squamous Cell Carcinoma: Translational Study of Epitopes-HPV01 and 02 Trials. International Journal of Molecular Sciences. 2020; 21(18):6838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186838
Chicago/Turabian StyleSpehner, Laurie, Stefano Kim, Angélique Vienot, Eric François, Bruno Buecher, Olivier Adotevi, Dewi Vernerey, Syrine Abdeljaoued, Aurélia Meurisse, and Christophe Borg. 2020. "Anti-Telomerase CD4+ Th1 Immunity and Monocytic-Myeloid-Derived-Suppressor Cells Are Associated with Long-Term Efficacy Achieved by Docetaxel, Cisplatin, and 5-Fluorouracil (DCF) in Advanced Anal Squamous Cell Carcinoma: Translational Study of Epitopes-HPV01 and 02 Trials" International Journal of Molecular Sciences 21, no. 18: 6838. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186838