The Prognostic Impact of Retinoid X Receptor and Thyroid Hormone Receptor alpha in Unifocal vs. Multifocal/Multicentric Breast Cancer

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Retinoid X Receptor (RXR)
2.1.1. Unifocal BC
2.1.2. Multifocal and/or Multicentric BC
2.2. Thyroid Hormone Receptor α1 (THRα1)
2.2.1. Unifocal BC
2.2.2. Multifocal and/or Multicentric BC
2.3. Thyroid Hormone Receptor α2 (THRα2)
2.3.1. Unifocal BC
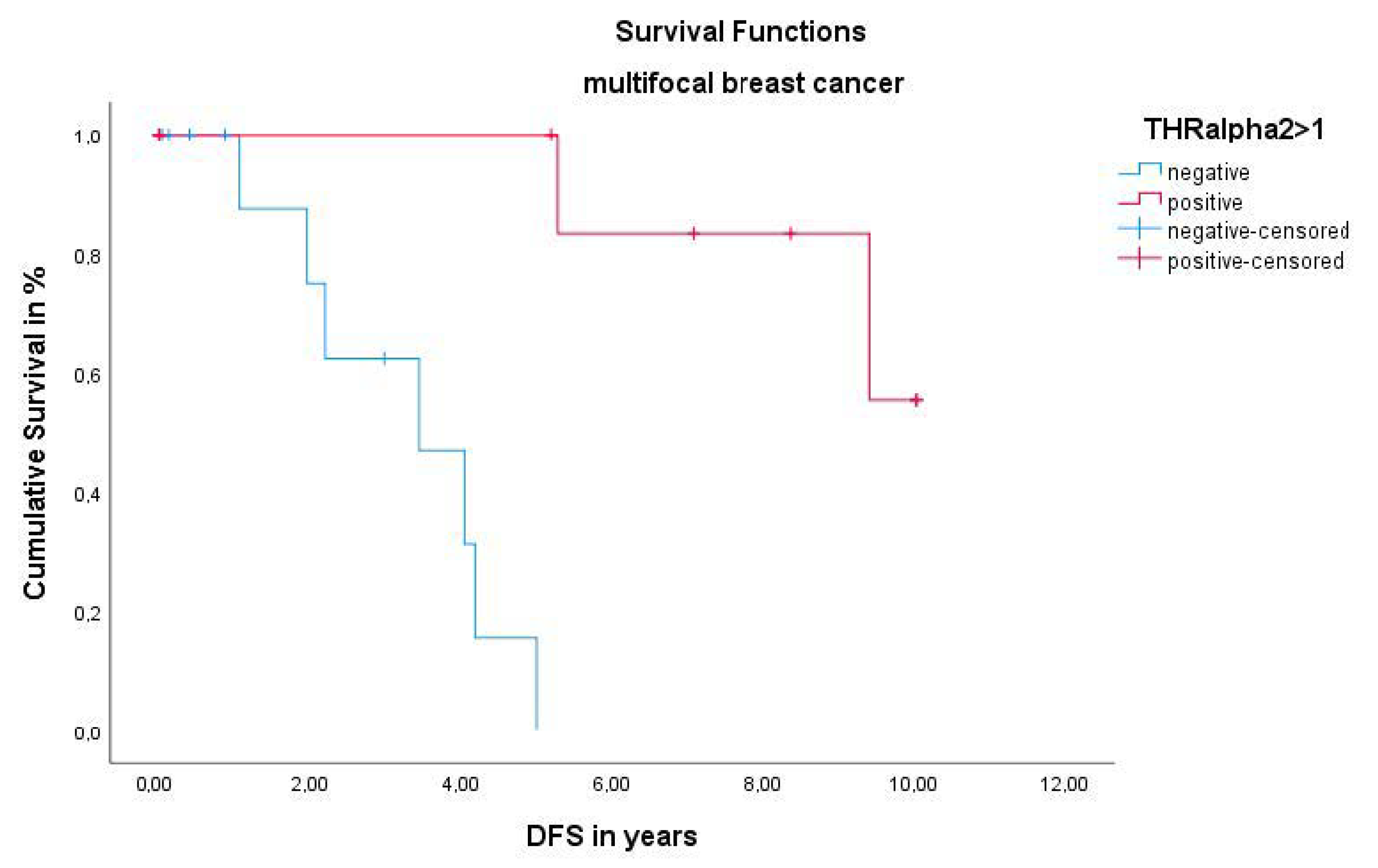
2.3.2. Multifocal and/or Multicentric BC
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunohistochemistry
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Approval and Consent to Participate
Abbreviations
| BC | Breast cancer |
| DFS | Disease-free survival |
| ER | Estrogen receptor |
| IRS | Immmunoreactive score |
| PR | Progesterone receptor |
| OS | Overall survival |
| RXR | Retinoid X receptor |
| TC | Total collective |
| TH | Thyroid hormone |
| THR | Thyroid hormone receptor |
| THRα | Thyroid hormone receptor alpha |
| THRα1 | Thyroid hormone receptor alpha 1 |
| THRα2 | Thyroid hormone receptor alpha 2 |
| VDR | Vitamin D receptor |
References
- Harbeck, N.; Gnant, M. Breast cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Cancer. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [CrossRef] [PubMed]
- McGuire, S. World Cancer Report 2014. Geneva, Switzerland: World Health Organization, International Agency for Research on Cancer, 2015. Adv. Nutr. 2016, 7, 418–419. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.; Costantino, J.P.; Wickerham, D.L.; Cecchini, R.S.; Cronin, W.M.; Robidoux, A.; Bevers, T.B.; Kavanah, M.T.; Atkins, J.N.; Margolese, R.G.; et al. Tamoxifen for the prevention of breast cancer: Current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J. Natl. Cancer Inst. 2005, 97, 1652–1662. [Google Scholar] [CrossRef] [Green Version]
- Cauley, J.A.; Norton, L.; Lippman, M.E.; Eckert, S.; Krueger, K.A.; Purdie, D.W.; Farrerons, J.; Karasik, A.; Mellstrom, D.; Ng, K.W.; et al. Continued breast cancer risk reduction in postmenopausal women treated with raloxifene: 4-year results from the MORE trial. Multiple outcomes of raloxifene evaluation. Breast Cancer Res. Treat. 2001, 65, 125–134. [Google Scholar] [CrossRef]
- Goss, P.E.; Ingle, J.N.; Ales-Martinez, J.E.; Cheung, A.M.; Chlebowski, R.T.; Wactawski-Wende, J.; McTiernan, A.; Robbins, J.; Johnson, K.C.; Martin, L.W.; et al. Exemestane for breast-cancer prevention in postmenopausal women. N. Engl. J. Med. 2011, 364, 2381–2391. [Google Scholar] [CrossRef] [Green Version]
- Muller, K.; Sixou, S.; Kuhn, C.; Jalaguier, S.; Mayr, D.; Ditsch, N.; Weissenbacher, T.; Harbeck, N.; Mahner, S.; Cavailles, V.; et al. Prognostic relevance of RIP140 and ERbeta expression in unifocal versus multifocal breast cancers: A preliminary report. Int. J. Mol. Sci. 2019, 20, 418. [Google Scholar] [CrossRef] [Green Version]
- Ataseven, B.; Lederer, B.; Blohmer, J.U.; Denkert, C.; Gerber, B.; Heil, J.; Kuhn, T.; Kummel, S.; Rezai, M.; Loibl, S.; et al. Impact of multifocal or multicentric disease on surgery and locoregional, distant and overall survival of 6,134 breast cancer patients treated with neoadjuvant chemotherapy. Ann. Surg. Oncol. 2015, 22, 1118–1127. [Google Scholar] [CrossRef]
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. (AWMF) Interdiszipliäre S3-Leitlinie für die Früherkennung, Diagnostik, Therapie und Nachsorge des Mammakarzinoms. Available online: https://www.awmf.org/uploads/tx_szleitlinien/032-045OLl_S3_Mammakarzinom_2017-12.pdf (accessed on 21 December 2020).
- Shaikh, T.; Tam, T.Y.; Li, T.; Hayes, S.B.; Goldstein, L.; Bleicher, R.; Boraas, M.; Sigurdson, E.; Ryan, P.D.; Anderson, P. Multifocal and multicentric breast cancer is associated with increased local recurrence regardless of surgery type. Breast J. 2015, 21, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Zati Zehni, A.; Jeschke, U.; Hester, A.; Kolben, T.; Ditsch, N.; Jacob, S.N.; Mumm, J.N.; Heidegger, H.H.; Mahner, S.; Vilsmaier, T. EP3 Is an Independent Prognostic Marker Only for Unifocal Breast Cancer Cases. Int. J. Mol. Sci. 2020, 21, 4418. [Google Scholar] [CrossRef] [PubMed]
- Weissenbacher, T.M.; Zschage, M.; Janni, W.; Jeschke, U.; Dimpfl, T.; Mayr, D.; Rack, B.; Schindlbeck, C.; Friese, K.; Dian, D. Multicentric and multifocal versus unifocal breast cancer: Is the tumor-node-metastasis classification justified? Breast Cancer Res. Treat. 2010, 122, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, Z.; Wu, Y.; Li, C.; Li, X.; Wang, X.; Qu, G. Multifocal and Multicentric Breast Carcinoma: A Significantly More Aggressive Tumor than Unifocal Breast Cancer. Anticancer Res. 2017, 37, 4593–4598. [Google Scholar]
- Boros, M.; Voidazan, S.; Moldovan, C.; Georgescu, R.; Toganel, C.; Moncea, D.; Molnar, C.V.; Podoleanu, C.; Eniu, A.; Stolnicu, S. Clinical implications of multifocality as a prognostic factor in breast carcinoma—A multivariate analysis study comprising 460 cases. Int. J. Clin. Exp. Med. 2015, 8, 9839–9846. [Google Scholar]
- Hua, S.; Kittler, R.; White, K.P. Genomic antagonism between retinoic acid and estrogen signaling in breast cancer. Cell 2009, 137, 1259–1271. [Google Scholar] [CrossRef] [Green Version]
- Muscat, G.E.; Eriksson, N.A.; Byth, K.; Loi, S.; Graham, D.; Jindal, S.; Davis, M.J.; Clyne, C.; Funder, J.W.; Simpson, E.R.; et al. Research resource: Nuclear receptors as transcriptome: Discriminant and prognostic value in breast cancer. Mol. Endocrinol. 2013, 27, 350–365. [Google Scholar] [CrossRef]
- Escriva, H.; Bertrand, S.; Laudet, V. The evolution of the nuclear receptor superfamily. Essays Biochem. 2004, 40, 11–26. [Google Scholar]
- Dawson, M.I.; Xia, Z. The retinoid X receptors and their ligands. Biochim. Biophys. Acta 2012, 1821, 21–56. [Google Scholar] [CrossRef] [Green Version]
- Zati Zehni, A.; Jacob, S.N.; Mumm, J.N.; Heidegger, H.H.; Ditsch, N.; Mahner, S.; Jeschke, U.; Vilsmaier, T. Hormone Receptor Expression in Multicentric/Multifocal versus Unifocal Breast Cancer: Especially the VDR Determines the Outcome Related to Focality. Int. J. Mol. Sci. 2019, 20, 5740. [Google Scholar] [CrossRef] [Green Version]
- Ditsch, N.; Vrekoussis, T.; Lenhard, M.; Ruhl, I.; Gallwas, J.; Weissenbacher, T.; Friese, K.; Mayr, D.; Makrigiannakis, A.; Jeschke, U. Retinoid X receptor alpha (RXRalpha) and peroxisome proliferator-activated receptor gamma (PPARgamma) expression in breast cancer: An immunohistochemical study. In Vivo 2012, 26, 87–92. [Google Scholar] [PubMed]
- Forman, B.M.; Umesono, K.; Chen, J.; Evans, R.M. Unique response pathways are established by allosteric interactions among nuclear hormone receptors. Cell 1995, 81, 541–550. [Google Scholar] [CrossRef] [Green Version]
- Koeffler, H.P. Peroxisome proliferator-activated receptor gamma and cancers. Clin. Cancer Res. 2003, 9, 1–9. [Google Scholar] [PubMed]
- Tang, X.H.; Gudas, L.J. Retinoids, retinoic acid receptors, and cancer. Annu. Rev. Pathol. 2011, 6, 345–364. [Google Scholar] [CrossRef] [PubMed]
- Auwerx, J.; Baulieu, E.; Beato, M.; Becker-Andre, M.; Burbach, P.H.; Camerino, G.; Chambon, P.; Cooney, A.; Dejean, A.; Dreyer, C.; et al. A unified nomenclature system for the nuclear receptor superfamily. Cell 1999, 97, 161–163. [Google Scholar]
- Raffo, P.; Emionite, L.; Colucci, L.; Belmondo, F.; Moro, M.G.; Bollag, W.; Toma, S. Retinoid receptors: Pathways of proliferation inhibition and apoptosis induction in breast cancer cell lines. Anticancer Res. 2000, 20, 1535–1543. [Google Scholar] [PubMed]
- Friedrich, M.; Axt-Fliedner, R.; Villena-Heinsen, C.; Tilgen, W.; Schmidt, W.; Reichrath, J. Analysis of vitamin D-receptor (VDR) and retinoid X-receptor alpha in breast cancer. Histochem. J. 2002, 34, 35–40. [Google Scholar] [CrossRef]
- Elstner, E.; Williamson, E.A.; Zang, C.; Fritz, J.; Heber, D.; Fenner, M.; Possinger, K.; Koeffler, H.P. Novel therapeutic approach: Ligands for PPARgamma and retinoid receptors induce apoptosis in bcl-2-positive human breast cancer cells. Breast Cancer Res. Treat. 2002, 74, 155–165. [Google Scholar] [CrossRef]
- Crowe, D.L.; Chandraratna, R.A. A retinoid X receptor (RXR)-selective retinoid reveals that RXR-alpha is potentially a therapeutic target in breast cancer cell lines, and that it potentiates antiproliferative and apoptotic responses to peroxisome proliferator-activated receptor ligands. Breast Cancer Res. 2004, 6, R546–R555. [Google Scholar] [CrossRef] [Green Version]
- Suh, N.; Wang, Y.; Williams, C.R.; Risingsong, R.; Gilmer, T.; Willson, T.M.; Sporn, M.B. A new ligand for the peroxisome proliferator-activated receptor-gamma (PPAR-gamma), GW7845, inhibits rat mammary carcinogenesis. Cancer Res. 1999, 59, 5671–5673. [Google Scholar]
- Zanardi, S.; Serrano, D.; Argusti, A.; Barile, M.; Puntoni, M.; Decensi, A. Clinical trials with retinoids for breast cancer chemoprevention. Endocr. Relat. Cancer 2006, 13, 51–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross-Innes, C.S.; Stark, R.; Holmes, K.A.; Schmidt, D.; Spyrou, C.; Russell, R.; Massie, C.E.; Vowler, S.L.; Eldridge, M.; Carroll, J.S. Cooperative interaction between retinoic acid receptor-alpha and estrogen receptor in breast cancer. Genes Dev. 2010, 24, 171–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heublein, S.; Mayr, D.; Meindl, A.; Kircher, A.; Jeschke, U.; Ditsch, N. Vitamin D receptor, Retinoid X receptor and peroxisome proliferator-activated receptor gamma are overexpressed in BRCA1 mutated breast cancer and predict prognosis. J. Exp. Clin. Cancer Res. 2017, 36, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonofiglio, D.; Cione, E.; Vizza, D.; Perri, M.; Pingitore, A.; Qi, H.; Catalano, S.; Rovito, D.; Genchi, G.; Ando, S. Bid as a potential target of apoptotic effects exerted by low doses of PPARgamma and RXR ligands in breast cancer cells. Cell Cycle 2011, 10, 2344–2354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasmin, R.; Kannan-Thulasiraman, P.; Kagechika, H.; Dawson, M.I.; Noy, N. Inhibition of mammary carcinoma cell growth by RXR is mediated by the receptor’s oligomeric switch. J. Mol. Biol. 2010, 397, 1121–1131. [Google Scholar] [CrossRef] [Green Version]
- Kuijpens, J.L.; Nyklictek, I.; Louwman, M.W.; Weetman, T.A.; Pop, V.J.; Coebergh, J.W. Hypothyroidism might be related to breast cancer in post-menopausal women. Thyroid 2005, 15, 1253–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turken, O.; NarIn, Y.; DemIrbas, S.; Onde, M.E.; Sayan, O.; KandemIr, E.G.; Yaylac, I.M.; Ozturk, A. Breast cancer in association with thyroid disorders. Breast Cancer Res. 2003, 5, R110–R113. [Google Scholar] [CrossRef]
- Ditsch, N.; Liebhardt, S.; Von Koch, F.; Lenhard, M.; Vogeser, M.; Spitzweg, C.; Gallwas, J.; Toth, B. Thyroid function in breast cancer patients. Anticancer Res. 2010, 30, 1713–1717. [Google Scholar]
- Tremmel, E.; Hofmann, S.; Kuhn, C.; Heidegger, H.; Heublein, S.; Hermelink, K.; Wuerstlein, R.; Harbeck, N.; Mayr, D.; Mahner, S.; et al. Thyronamine regulation of TAAR1 expression in breast cancer cells and investigation of its influence on viability and migration. Breast Cancer 2019, 11, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.C.; Yeh, C.T.; Lin, K.H. Molecular Functions of Thyroid Hormone Signaling in Regulation of Cancer Progression and Anti-Apoptosis. Int. J. Mol. Sci. 2019, 20, 4986. [Google Scholar] [CrossRef] [Green Version]
- Mitsuhashi, T.; Tennyson, G.E.; Nikodem, V.M. Alternative splicing generates messages encoding rat c-erbA proteins that do not bind thyroid hormone. Proc. Natl. Acad. Sci. USA 1988, 85, 5804–5808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakurai, A.; Nakai, A.; DeGroot, L.J. Expression of three forms of thyroid hormone receptor in human tissues. Mol. Endocrinol. 1989, 3, 392–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual, A.; Aranda, A. Thyroid hormone receptors, cell growth and differentiation. Biochim. Biophys. Acta 2013, 1830, 3908–3916. [Google Scholar] [CrossRef] [PubMed]
- Perlmann, T.; Rangarajan, P.N.; Umesono, K.; Evans, R.M. Determinants for selective RAR and TR recognition of direct repeat HREs. Genes Dev. 1993, 7, 1411–1422. [Google Scholar] [CrossRef] [Green Version]
- Heublein, S.; Mayr, D.; Meindl, A.; Angele, M.; Gallwas, J.; Jeschke, U.; Ditsch, N. Thyroid Hormone Receptors Predict Prognosis in BRCA1 Associated Breast Cancer in Opposing Ways. PLoS ONE 2015, 10, e0127072. [Google Scholar] [CrossRef]
- Han, S.; Roman, J. Peroxisome proliferator-activated receptor gamma: A novel target for cancer therapeutics? Anticancer Drugs 2007, 18, 237–244. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Joseph, C.; Al-Izzi, S.; Alsaleem, M.; Kurozumi, S.; Toss, M.S.; Arshad, M.; Goh, F.Q.; Alshankyty, I.M.; Aleskandarany, M.A.; Ali, S.; et al. Retinoid X receptor gamma (RXRG) is an independent prognostic biomarker in ER-positive invasive breast cancer. Br. J. Cancer 2019, 121, 776–785. [Google Scholar] [CrossRef]
- Roszer, T.; Menendez-Gutierrez, M.P.; Cedenilla, M.; Ricote, M. Retinoid X receptors in macrophage biology. Trends Endocrinol. Metab. 2013, 24, 460–468. [Google Scholar] [CrossRef]
- Leal, A.S.; Zydeck, K.; Carapellucci, S.; Reich, L.A.; Zhang, D.; Moerland, J.A.; Sporn, M.B.; Liby, K.T. Retinoid X receptor agonist LG100268 modulates the immune microenvironment in preclinical breast cancer models. NPJ Breast Cancer 2019, 5, 39. [Google Scholar] [CrossRef]
- Nunez, V.; Alameda, D.; Rico, D.; Mota, R.; Gonzalo, P.; Cedenilla, M.; Fischer, T.; Bosca, L.; Glass, C.K.; Arroyo, A.G.; et al. Retinoid X receptor alpha controls innate inflammatory responses through the up-regulation of chemokine expression. Proc. Natl. Acad. Sci. USA 2010, 107, 10626–10631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, R.S.; Bapat, S.A. Expression proteomics predicts loss of RXR-gamma during progression of epithelial ovarian cancer. PLoS ONE 2013, 8, e70398. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Lee, J.Y.; Choi, J.E.; Lee, S.Y.; Park, J.Y.; Kim, D.S. Epigenetic inactivation of retinoid X receptor genes in non-small cell lung cancer and the relationship with clinicopathologic features. Cancer Genet. Cytogenet. 2010, 197, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Liby, K.; Rendi, M.; Suh, N.; Royce, D.B.; Risingsong, R.; Williams, C.R.; Lamph, W.; Labrie, F.; Krajewski, S.; Xu, X.; et al. The combination of the rexinoid, LG100268, and a selective estrogen receptor modulator, either arzoxifene or acolbifene, synergizes in the prevention and treatment of mammary tumors in an estrogen receptor-negative model of breast cancer. Clin. Cancer Res. 2006, 12, 5902–5909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, K.; Kim, H.T.; Rodriquez, J.L.; Hilsenbeck, S.G.; Mohsin, S.K.; Xu, X.C.; Lamph, W.W.; Kuhn, J.G.; Green, J.E.; Brown, P.H. Suppression of mammary tumorigenesis in transgenic mice by the RXR-selective retinoid, LGD1069. Cancer Epidemiol. Biomark. Prev. 2002, 11, 467–474. [Google Scholar]
- Kong, G.; Kim, H.T.; Wu, K.; DeNardo, D.; Hilsenbeck, S.G.; Xu, X.C.; Lamph, W.W.; Bissonnette, R.; Dannenberg, A.J.; Brown, P.H. The retinoid X receptor-selective retinoid, LGD1069, down-regulates cyclooxygenase-2 expression in human breast cells through transcription factor crosstalk: Implications for molecular-based chemoprevention. Cancer Res. 2005, 65, 3462–3469. [Google Scholar] [CrossRef] [Green Version]
- Wu, K.; DuPre, E.; Kim, H.; Tin, U.C.; Bissonnette, R.P.; Lamph, W.W.; Brown, P.H. Receptor-selective retinoids inhibit the growth of normal and malignant breast cells by inducing G1 cell cycle blockade. Breast Cancer Res. Treat. 2006, 96, 147–157. [Google Scholar] [CrossRef]
- Esteva, F.J.; Glaspy, J.; Baidas, S.; Laufman, L.; Hutchins, L.; Dickler, M.; Tripathy, D.; Cohen, R.; DeMichele, A.; Yocum, R.C.; et al. Multicenter phase II study of oral bexarotene for patients with metastatic breast cancer. J. Clin. Oncol. 2003, 21, 999–1006. [Google Scholar] [CrossRef]
- Alvarado-Pisani, A.R.; Chacon, R.S.; Betancourt, L.J.; Lopez-Herrera, L. Thyroid hormone receptors in human breast cancer: Effect of thyroxine administration. Anticancer Res. 1986, 6, 1347–1351. [Google Scholar]
- Cestari, S.H.; Figueiredo, N.B.; Conde, S.J.; Clara, S.; Katayama, M.L.; Padovani, C.R.; Brentani, M.M.; Nogueira, C.R. Influence of estradiol and triiodothyronine on breast cancer cell lines proliferation and expression of estrogen and thyroid hormone receptors. Arq. Bras. Endocrinol. Metab. 2009, 53, 859–864. [Google Scholar] [CrossRef] [Green Version]
- Hall, L.C.; Salazar, E.P.; Kane, S.R.; Liu, N. Effects of thyroid hormones on human breast cancer cell proliferation. J. Steroid. Biochem. Mol. Biol. 2008, 109, 57–66. [Google Scholar] [CrossRef]
- Jerzak, K.J.; Cockburn, J.; Pond, G.R.; Pritchard, K.I.; Narod, S.A.; Dhesy-Thind, S.K.; Bane, A. Thyroid hormone receptor alpha in breast cancer: Prognostic and therapeutic implications. Breast Cancer Res. Treat. 2015, 149, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Conde, I.; Paniagua, R.; Zamora, J.; Blanquez, M.J.; Fraile, B.; Ruiz, A.; Arenas, M.I. Influence of thyroid hormone receptors on breast cancer cell proliferation. Ann. Oncol. 2006, 17, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.M.; Dominguez, G.; Gonzalez-Sancho, J.M.; Garcia, J.M.; Silva, J.; Garcia-Andrade, C.; Navarro, A.; Munoz, A.; Bonilla, F. Expression of thyroid hormone receptor/erbA genes is altered in human breast cancer. Oncogene 2002, 21, 4307–4316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhlen, M.; Oksvold, P.; Fagerberg, L.; Lundberg, E.; Jonasson, K.; Forsberg, M.; Zwahlen, M.; Kampf, C.; Wester, K.; Hober, S.; et al. Towards a knowledge-based Human Protein Atlas. Nat. Biotechnol. 2010, 28, 1248–1250. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Meng, Z.H.; Chandrasekaran, R.; Kuo, W.L.; Collins, C.C.; Gray, J.W.; Dairkee, S.H. Biallelic inactivation of the thyroid hormone receptor beta1 gene in early stage breast cancer. Cancer Res. 2002, 62, 1939–1943. [Google Scholar] [PubMed]
- Ditsch, N.; Toth, B.; Himsl, I.; Lenhard, M.; Ochsenkuhn, R.; Friese, K.; Mayr, D.; Jeschke, U. Thyroid hormone receptor (TR)alpha and TRbeta expression in breast cancer. Histol. Histopathol. 2013, 28, 227–237. [Google Scholar] [PubMed]
- Ribeiro, R.C.; Apriletti, J.W.; Wagner, R.L.; Feng, W.; Kushner, P.J.; Nilsson, S.; Scanlan, T.S.; West, B.L.; Fletterick, R.J.; Baxter, J.D. X-ray crystallographic and functional studies of thyroid hormone receptor. J. Steroid Biochem. Mol. Biol. 1998, 65, 133–141. [Google Scholar] [CrossRef]
- Lazar, J.; Desvergne, B.; Zimmerman, E.C.; Zimmer, D.B.; Magnuson, M.A.; Nikodem, V.M. A role for intronic sequences on expression of thyroid hormone receptor alpha gene. J. Biol. Chem. 1994, 269, 20352–20359. [Google Scholar] [CrossRef]
- Izumo, S.; Mahdavi, V. Thyroid hormone receptor alpha isoforms generated by alternative splicing differentially activate myosin HC gene transcription. Nature 1988, 334, 539–542. [Google Scholar] [CrossRef]
- Hercbergs, A.; Johnson, R.E.; Ashur-Fabian, O.; Garfield, D.H.; Davis, P.J. Medically induced euthyroid hypothyroxinemia may extend survival in compassionate need cancer patients: An observational study. Oncologist 2015, 20, 72–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hercbergs, A.A.; Goyal, L.K.; Suh, J.H.; Lee, S.; Reddy, C.A.; Cohen, B.H.; Stevens, G.H.; Reddy, S.K.; Peereboom, D.M.; Elson, P.J.; et al. Propylthiouracil-induced chemical hypothyroidism with high-dose tamoxifen prolongs survival in recurrent high grade glioma: A phase I/II study. Anticancer Res. 2003, 23, 617–626. [Google Scholar] [PubMed]
- Dinda, S.; Sanchez, A.; Moudgil, V. Estrogen-like effects of thyroid hormone on the regulation of tumor suppressor proteins, p53 and retinoblastoma, in breast cancer cells. Oncogene 2002, 21, 761–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabnis, G.J.; Goloubeva, O.; Chumsri, S.; Nguyen, N.; Sukumar, S.; Brodie, A.M. Functional activation of the estrogen receptor-alpha and aromatase by the HDAC inhibitor entinostat sensitizes ER-negative tumors to letrozole. Cancer Res. 2011, 71, 1893–1903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cserni, G.; Chmielik, E.; Cserni, B.; Tot, T. The new TNM-based staging of breast cancer. Virchows Arch. 2018, 472, 697–703. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Edge, S.B.; Giuliano, A. New and Important Changes in the TNM Staging System for Breast Cancer. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 457–467. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 2002, 41, 151–152. [Google Scholar] [CrossRef]
- Ditsch, N.; Mayr, D.; Lenhard, M.; Strauss, C.; Vodermaier, A.; Gallwas, J.; Stoeckl, D.; Graeser, M.; Weissenbacher, T.; Friese, K.; et al. Correlation of thyroid hormone, retinoid X, peroxisome proliferator-activated, vitamin D and oestrogen/progesterone receptors in breast carcinoma. Oncol. Lett. 2012, 4, 665–671. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable. | Coefficient | HR (95% CI) | p Value |
|---|---|---|---|
| Age | −0.001 | 0.999 (0.970–1.0301) | 0.967 |
| Grading | −0.008 | 0.992 (0.985–0.999) | 0.034 |
| pT | 0.215 | 1.240 (0.833–1.845) | 0.290 |
| pN | −0.003 | 0.997 (0.982–1.012) | 0.695 |
| pM | 2.353 | 10.516 (4.694–23.559) | 0.000 |
| RXR | 0.437 | 1.547 (0.687–3.483) | 0.292 |
| Variable | Coefficient | HR (95% CI) | p Value |
|---|---|---|---|
| Age | 0.010 | 1.010 (0.975–1.046) | 0.575 |
| Grading | 0.418 | 1.159 (0.761–3.033) | 0.236 |
| pT | 0.115 | 1.122 (0.784–1.605) | 0.530 |
| pN | 0.022 | 1.022 (0.795–1.314) | 0.867 |
| pM | 2.079 | 7.993 (3.007–21.248) | 0.000 |
| THRα1 | 0.486 | 1.626 (0.532–4.973) | 0.394 |
| Variable | Coefficient | HR (95% CI) | p Value |
|---|---|---|---|
| Age | 0.005 | 1.005 (0.978–1.033) | 0.721 |
| Grading | −0.008 | 0.984 (0.984–0.999) | 0.033 |
| pT | 0.201 | 1.222 (0.841–1.776) | 0.293 |
| pN | −0.001 | 0.999 (0.984–1.014) | 0.880 |
| pM | 2.550 | 12.812 (5.662–28.988) | 0.000 |
| THRα2 | −0.299 | 0.742 (0.370–1.486) | 0.399 |
| Patient Characteristics | n (%) |
|---|---|
| Age (years) | Median 59.09 Range 69 |
| Tumor foci | Unifocal 173 (54.2) Multifocal 146 (45.7) |
| Histology | NST 188 (61.4) Non-NST 118 (38.5) |
| Tumor grade | G1 or G2 165 (52.2) G3 151 (47.7) |
| pT | pT1 197 (64.3) pT2-pT4 109 (35.6) |
| pN | pN0 166 (54.2) pN1-pN3 140 (45.7) |
| pM | pM0 239 (78.1) pM1 67 (21.8) |
| RXR | negative 186 (58.3) positive 133 (41.6) |
| THRα1 | negative 120 (37.6) positive 199 (62.3) |
| THRα2 | negative 172 (53.9) positive 147 (46.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zehni, A.Z.; Batz, F.; Vattai, A.; Kaltofen, T.; Schrader, S.; Jacob, S.-N.; Mumm, J.-N.; Heidegger, H.H.; Ditsch, N.; Mahner, S.; et al. The Prognostic Impact of Retinoid X Receptor and Thyroid Hormone Receptor alpha in Unifocal vs. Multifocal/Multicentric Breast Cancer. Int. J. Mol. Sci. 2021, 22, 957. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020957
Zehni AZ, Batz F, Vattai A, Kaltofen T, Schrader S, Jacob S-N, Mumm J-N, Heidegger HH, Ditsch N, Mahner S, et al. The Prognostic Impact of Retinoid X Receptor and Thyroid Hormone Receptor alpha in Unifocal vs. Multifocal/Multicentric Breast Cancer. International Journal of Molecular Sciences. 2021; 22(2):957. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020957
Chicago/Turabian StyleZehni, Alaleh Zati, Falk Batz, Aurelia Vattai, Till Kaltofen, Svenja Schrader, Sven-Niclas Jacob, Jan-Niclas Mumm, Helene Hildegard Heidegger, Nina Ditsch, Sven Mahner, and et al. 2021. "The Prognostic Impact of Retinoid X Receptor and Thyroid Hormone Receptor alpha in Unifocal vs. Multifocal/Multicentric Breast Cancer" International Journal of Molecular Sciences 22, no. 2: 957. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020957