
Targeting the Autonomic Nervous System for Risk Stratification, Outcome Prediction and Neuromodulation in Ischemic Stroke

 , ,
, ,  , and
, and 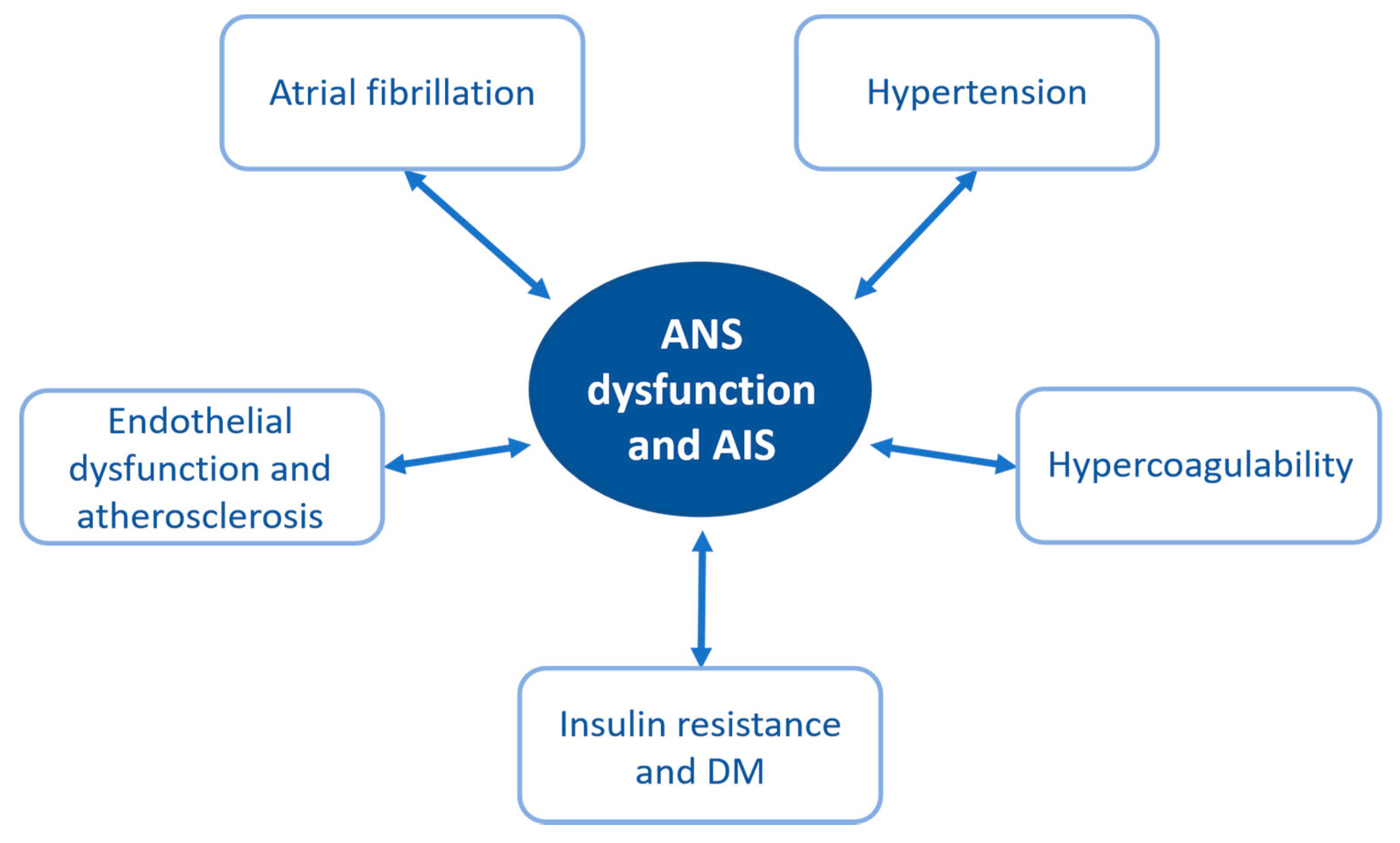{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. ANS Dysfunction and Ischemic Stroke: Running in Circles
2.1. ANS Dysfunction Can Increase the Risk of Ischemic Stroke
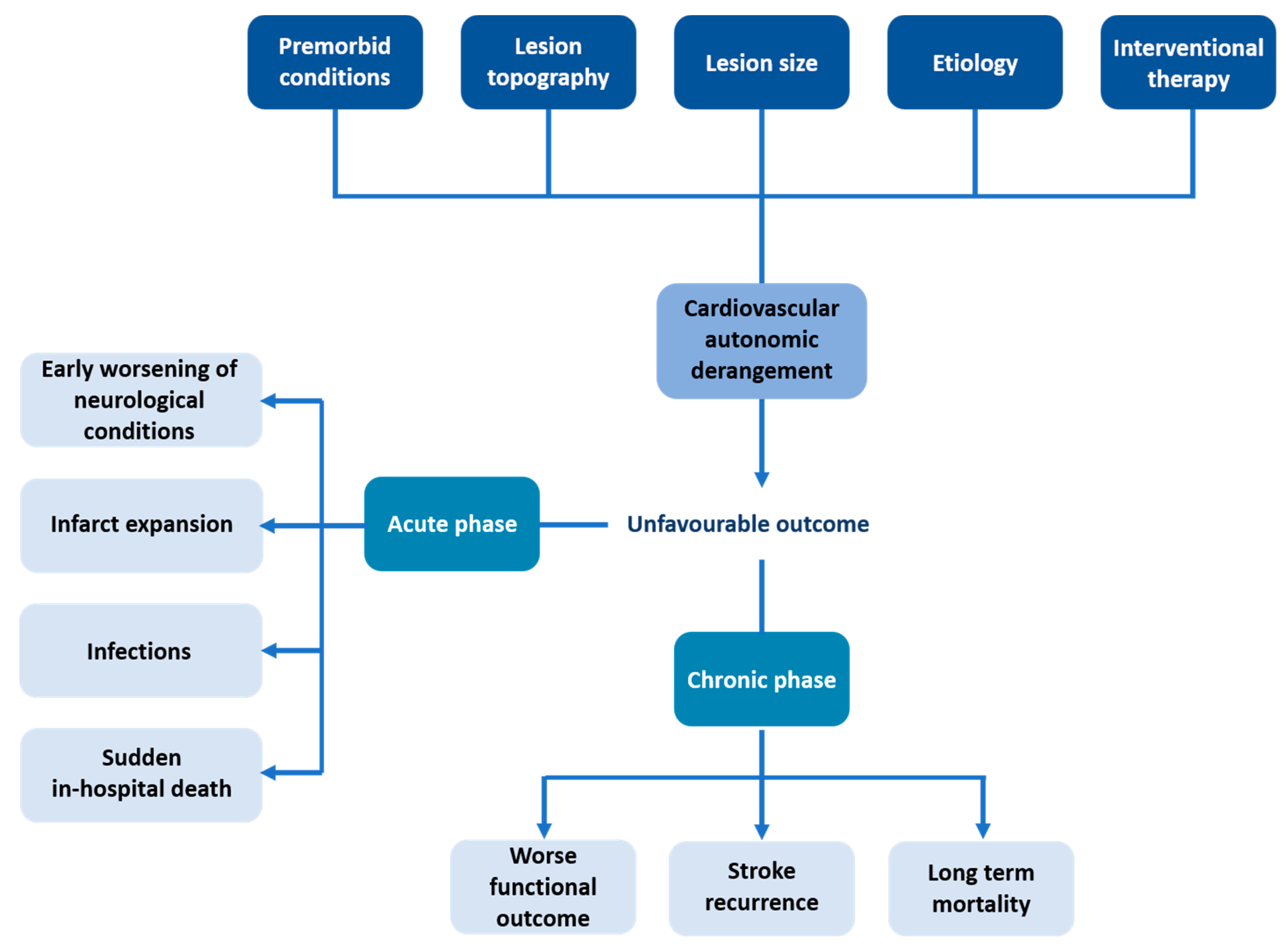
2.2. ANS Dysfunction after Ischemic Stroke
2.3. The Predictive Role of HRV
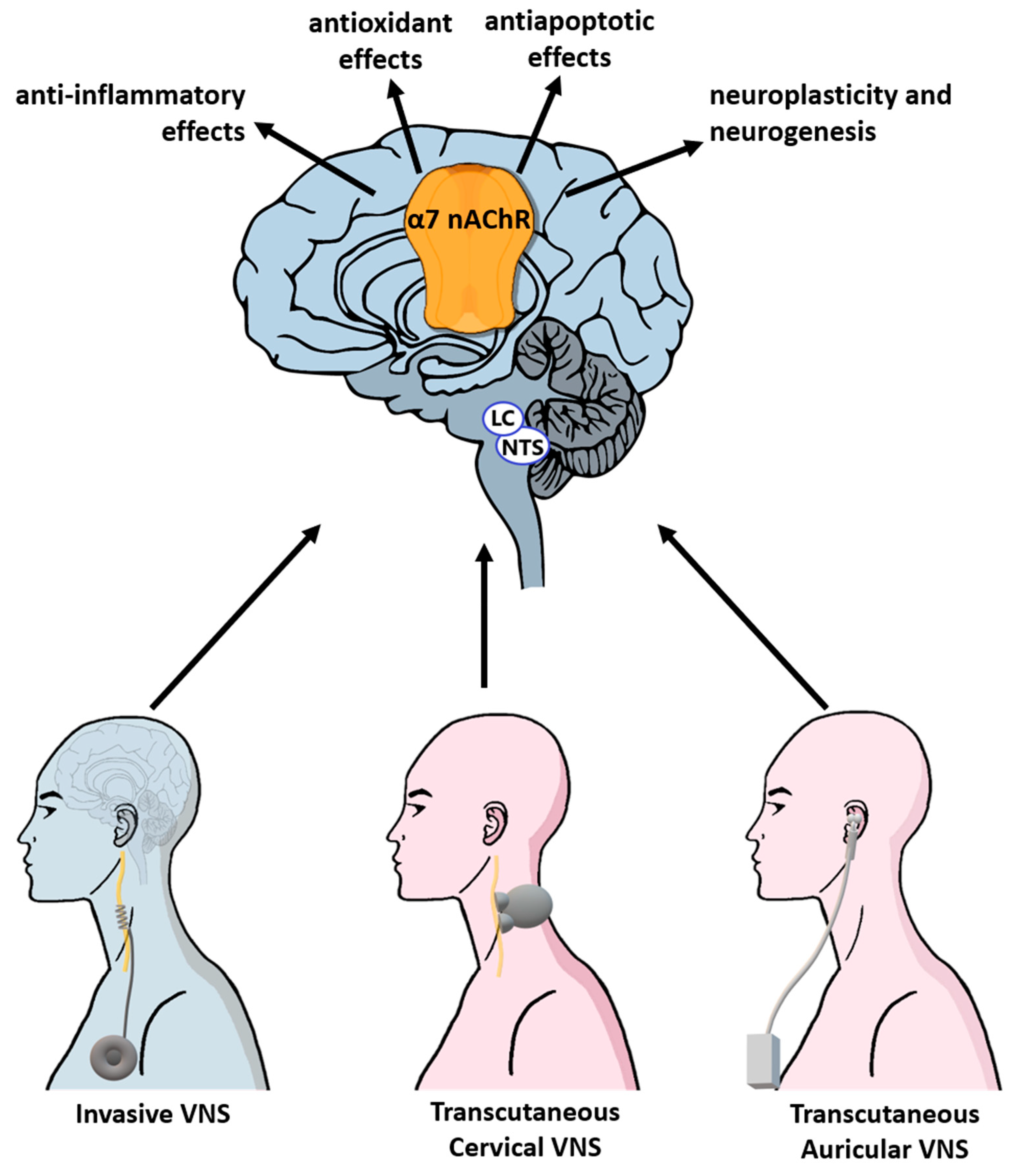
3. Targeting the Vagus Nerve: A Promising Multilevel Approach
3.1. The VNS Molecular Targets for Neuroprotection and Neuroplasticity in Stroke
3.1.1. Anti-Inflammatory Effects
3.1.2. Antioxidant Effects {XE “3.2.2. Antioxidant Effects”}
3.1.3. Antiapoptotic Effects {XE “3.2.3. Antiapoptotic Effects”}
3.1.4. Neuroplasticity and Neurogenesis {XE “3.2.3. Neuroplasticity and Neurogenesis”}
3.2. The Effects of VNS in Ischemic Stroke {XE “3.1. The Macro-Effects of VNS in Ischaemic Stroke”}
4. Conclusions
Funding
Conflicts of Interest
References
- Phipps, M.S.; Cronin, C.A. Management of acute ischemic stroke’. BMJ 2020, 368, 6983. [Google Scholar] [CrossRef] [Green Version]
- Vos, T. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Appelros, P.; Stegmayr, B.; Terént, A. Sex Differences in Stroke Epidemiology: A Systematic Review. Stroke 2009, 40, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Appelros, P.; Stegmayr, B.; Terént, A. A Review on Sex Differences in Stroke Treatment and Outcome. Acta Neurol. Scand. 2010, 121, 359–369. [Google Scholar] [CrossRef]
- Bushnell, C.D.; Chaturvedi, S.; Gage, K.R.; Herson, P.S.; Hurn, P.D.; Jiménez, M.C.; Kittner, S.J.; Madsen, T.E.; McCullough, L.D.; McDermott, M.; et al. Sex Differences in Stroke: Challenges and Opportunities. J. Cereb. Blood Flow Metab. 2018, 38, 2179–2191. [Google Scholar] [CrossRef] [PubMed]
- Micieli, G.; Cavallini, A. The Autonomic Nervous System and Ischemic Stroke: A Reciprocal Interdependence. Clin. Auton. Res. 2008, 18, 308–317. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J. Risk Factors for Ischaemic and Intracerebral Haemorrhagic Stroke in 22 Countries (the INTERSTROKE Study): A Case-Control Study’. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- Girijala, R.L.; Sohrabji, F.; Bush, R.L. Sex Differences in Stroke: Review of Current Knowledge and Evidence. Vasc. Med. 2017, 22, 135–145. [Google Scholar] [CrossRef]
- Lombardi, F.; Tarricone, D.; Tundo, F.; Colombo, F.; Belletti, S.; Fiorentini, C. Autonomic Nervous System and Paroxysmal Atrial Fibrillation: A Study Based on the Analysis of RR Interval Changes before, during and after Paroxysmal Atrial Fibrillation. Eur. Heart J. 2004, 25, 1242–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, J.P.; Paton, J.F.R. The Sympathetic Nervous System and Blood Pressure in Humans: Implications for Hypertension. J. Hum. Hypertens. 2012, 26, 463–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montano, N.; Porta, A.; Cogliati, C.; Costantino, G.; Tobaldini, E.; Casali, K.R.; Iellamo, F. Heart Rate Variability Explored in the Frequency Domain: A Tool to Investigate the Link between Heart and Behavior. Neurosci. Biobehav. Rev. 2009, 33, 71–80. [Google Scholar] [CrossRef]
- Goldstein, D.S.; Bentho, O.; Park, M.-Y.; Sharabi, Y. LF Power of Heart Rate Variability Is Not a Measure of Cardiac Sympathetic Tone but May Be a Measure of Modulation of Cardiac Autonomic Outflows by Baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The Relationship of Autonomic Imbalance, Heart Rate Variability and Cardiovascular Disease Risk Factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Binici, Z.; Mouridsen, M.R.; Køber, L.; Sajadieh, A. Decreased Nighttime Heart Rate Variability Is Associated with Increased Stroke Risk. Stroke 2011, 42, 3196–3201. [Google Scholar] [CrossRef] [Green Version]
- Bodapati, R.K.; Kizer, J.R.; Kop, W.J.; Kamel, H.; Stein, P.K. Addition of 24-Hour Heart Rate Variability Parameters to the Cardiovascular Health Study Stroke Risk Score and Prediction of Incident Stroke: The Cardiovascular Health Study. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Melillo, P. Automatic Prediction of Cardiovascular and Cerebrovascular Events Using Heart Rate Variability Analysis. PLoS ONE 2015, 10, 0118504. [Google Scholar] [CrossRef] [PubMed]
- Fyfe-Johnson, A.L.; Muller, C.J.; Alvaro, A.; Folsom, A.R.; Gottesman, R.F.; Rosamond, W.D.; Whitsel, E.A.; Agarwal, S.K.; MacLehose, R.F. Heart Rate Variability and Incident Stroke. Stroke 2016, 47, 1452–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, S.H. Cardiovascular Autonomic Dysfunction Predicts Acute Ischaemic Stroke in Patients with Type 2 Diabetes Mellitus: A 7-Year Follow-up Study. Diabet. Med. 2008, 25, 1171–1177. [Google Scholar] [CrossRef]
- Töyry, J.P.; Niskanen, L.K.; Länsimies, E.A.; Partanen, K.P.; Uusitupa, M.I. Autonomic Neuropathy Predicts the Development of Stroke in Patients with Non-Insulin-Dependent Diabetes Mellitus. Stroke 1996, 27, 1316–1318. [Google Scholar] [CrossRef]
- Feigin, V.L. Global Burden of Stroke and Risk Factors in 188 Countries, during 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef] [Green Version]
- Carthy, E.R. Autonomic Dysfunction in Essential Hypertension: A Systematic Review. Ann. Med. Surg. 2014, 3, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Malliani, A.; Montano, N. Emerging Excitatory Role of Cardiovascular Sympathetic Afferents in Pathophysiological Conditions. Hypertension 2002, 39, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Huikuri, H.V. Heart Rate Variability in Systemic Hypertension. Am. J. Cardiol. 1996, 77, 1073–1077. [Google Scholar] [CrossRef]
- Liao, D. Association of Cardiac Autonomic Function and the Development of Hypertension: The ARIC Study. Am. J. Hypertens. 1996, 9, 1147–1156. [Google Scholar] [CrossRef]
- Takalo, R.; Korhonen, I.; Turjanmaa, V.; Majahalme, S.; Tuomisto, M.; Uusitalo, A. Short-Term Variability of Blood Pressure and Heart Rate in Borderline and Mildly Hypertensive Subjects. Hypertension 1994, 23, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Xu, Y.; Zhang, M.; Wang, Y.; Zou, W.; Gu, Y. Value of Assessing Autonomic Nervous Function by Heart Rate Variability and Heart Rate Turbulence in Hypertensive Patients. Int. J. Hypertens. 2018. [Google Scholar] [CrossRef]
- Singh, J.P.; Larson, M.G.; Tsuji, H.; Evans, J.C.; O’Donnell, C.J.; Levy, D. Reduced Heart Rate Variability and New-Onset Hypertension. Hypertension 1998, 32, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Chugh, S.S. Worldwide Epidemiology of Atrial Fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [Green Version]
- Kamel, H.; Okin, P.M.; Elkind, M.S.V.; Iadecola, C. Atrial Fibrillation and Mechanisms of Stroke. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef] [Green Version]
- Perera, K.S.; Vanassche, T.; Bosch, J.; Swaminathan, B.; Mundl, H.; Giruparajah, M.; Barboza, M.A.; O’Donnell, M.J.; Gomez-Schneider, M.; Hankey, G.J.; et al. Global Survey of the Frequency of Atrial Fibrillation–Associated Stroke. Stroke 2016, 47, 2197–2202. [Google Scholar] [CrossRef] [Green Version]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial Fibrillation as an Independent Risk Factor for Stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [Green Version]
- Andrade, J.G.; Macle, L.; Nattel, S.; Verma, A.; Cairns, J. Contemporary Atrial Fibrillation Management: A Comparison of the Current AHA/ACC/HRS, CCS, and ESC Guidelines. Can. J. Cardiol. 2017, 33, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; Alió, J. Cardioembolic Stroke: Clinical Features, Specific Cardiac Disorders and Prognosis. Curr. Cardiol. Rev. 2010, 6, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.-S.; Chen, L.S.; Fishbein, M.C.; Lin, S.-F.; Nattel, S. Role of the Autonomic Nervous System in Atrial Fibrillation: Pathophysiology and Therapy. Circ. Res. 2014, 114, 1500–1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettoni, M.; Zimmermann, M. Autonomic Tone Variations before the Onset of Paroxysmal Atrial Fibrillation. Circulation 2002, 105, 2753–2759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, S.K.; Norby, F.L.; Whitsel, E.A.; Soliman, E.Z.; Chen, L.Y.; Loehr, L.R.; Fuster, V.; Heiss, G.; Coresh, J.; Alonso, A. Cardiac Autonomic Dysfunction and Incidence of Atrial Fibrillation: Results From 20 Years Follow-Up. J. Am. Coll. Cardiol. 2017, 69, 291–299. [Google Scholar] [CrossRef]
- Sluyter, J.D.; Camargo, C.A.; Lowe, A.; Scragg, R.K.R. Pulse Rate Variability Predicts Atrial Fibrillation and Cerebrovascular Events in a Large, Population-Based Cohort. Int. J. Cardiol. 2019, 275, 83–88. [Google Scholar] [CrossRef]
- Rizzo, M.R. Autonomic Dysfunction Is Associated with Brief Episodes of Atrial Fibrillation in Type 2 Diabetes. J. Diabetes Its Complicat. 2015, 29, 88–92. [Google Scholar] [CrossRef]
- Watanabe, E. Multiscale Entropy of the Heart Rate Variability for the Prediction of an Ischemic Stroke in Patients with Permanent Atrial Fibrillation. PLoS ONE 2015, 10, 0137144. [Google Scholar] [CrossRef]
- Acampa, M.; Lazzerini, P.E.; Martini, G. Atrial Cardiopathy and Sympatho-Vagal Imbalance in Cryptogenic Stroke: Pathogenic Mechanisms and Effects on Electrocardiographic Markers. Front. Neurol 2018, 9. [Google Scholar] [CrossRef]
- Petty, G.W.; Brown, R.D.; Whisnant, J.P.; Sicks JoRean, D.; O’Fallon, W.M.; Wiebers, D.O. Ischemic Stroke Subtypes. Stroke 1999, 30, 2513–2516. [Google Scholar] [CrossRef] [Green Version]
- Libby, P. Atherosclerosis. Nat. Rev. Dis. Primers 2019, 5. [Google Scholar] [CrossRef]
- Mayerl, C.; Lukasser, M.; Sedivy, R.; Niederegger, H.; Seiler, R.; Wick, G. Atherosclerosis Research from Past to Present—On the Track of Two Pathologists with Opposing Views, Carl von Rokitansky and Rudolf Virchow. Virchows Arch 2006, 449, 96–103. [Google Scholar] [CrossRef]
- Amiya, E.; Watanabe, M.; Komuro, I. The Relationship between Vascular Function and the Autonomic Nervous System’. Ann. Vasc. Dis. 2014, 7, 109–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtor, T.; Davis, H.R.; Johns, L.; Vesselinovitch, D.; Wissler, R.W.; Mullan, S. The Sympathetic Nervous System and Atherosclerosis. J. Neurosurg. 1987, 67, 906–914. [Google Scholar] [CrossRef] [Green Version]
- Chao, A.C. Noninvasive Assessment of Spontaneous Baroreflex Sensitivity and Heart Rate Variability in Patients with Carotid Stenosis. CED 2003, 16, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Nasr, N.; Traon, A.P.-L.; Larrue, V. Baroreflex Sensitivity Is Impaired in Bilateral Carotid Atherosclerosis. Stroke 2005, 36, 1891–1895. [Google Scholar] [CrossRef] [Green Version]
- Ulleryd, M.A. The Association between Autonomic Dysfunction, Inflammation and Atherosclerosis in Men under Investigation for Carotid Plaques. PLoS ONE 2017, 12, 0174974. [Google Scholar] [CrossRef] [Green Version]
- Rupprecht, S. Association Between Systemic Inflammation, Carotid Arteriosclerosis, and Autonomic Dysfunction. Transl. Stroke Res. 2020, 11, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Lau, L.-H.; Lew, J.; Borschmann, K.; Thijs, V.; Ekinci, E.I. Prevalence of Diabetes and Its Effects on Stroke Outcomes: A Meta-Analysis and Literature Review. J. Diabetes Investig. 2019, 10, 780–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frontoni, S.; Bracaglia, D.; Gigli, F. Relationship between Autonomic Dysfunction, Insulin Resistance and Hypertension, in Diabetes. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 441–449. [Google Scholar] [CrossRef]
- Verrotti, A.; Prezioso, G.; Scattoni, R.; Chiarelli, F. Autonomic Neuropathy in Diabetes Mellitus. Front. Endocrinol. Lausanne 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.A.; Estacio, R.O.; Lundgren, R.A.; Esler, A.L.; Schrier, R.W. Diabetic autonomic neuropathy is associated with an increased incidence of strokes. Auton. Neurosci. 2003, 108, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.H.; Toft, E.; Christensen, M.S.; Schmidt, E.B. Heart Rate Variability and Plasma Lipids in Men with and without Ischaemic Heart Disease. Atherosclerosis 1999, 145, 181–186. [Google Scholar] [CrossRef]
- Pehlivanidis, A.N.; Athyros, V.G.; Demitriadis, D.S.; Papageorgiou, A.A.; Bouloukos, V.J.; Kontopoulos, A.G. Heart Rate Variability after Long-Term Treatment with Atorvastatin in Hypercholesterolaemic Patients with or without Coronary Artery Disease. Atherosclerosis 2001, 157, 463–469. [Google Scholar] [CrossRef]
- Chiasakul, T.; De Jesus, E.; Tong, J.; Chen, Y.; Crowther, M.; Garcia, D.; Chai-Adisaksopha, C.; Messé, S.R.; Cuker, A. Inherited Thrombophilia and the Risk of Arterial Ischemic Stroke: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012877. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Chung, J.-W.; Ahn, M.-J.; Kim, S.; Seok, J.M.; Jang, H.M.; Kim, G.-M.; Chung, C.-S.; Lee, K.H.; Bang, O.Y. Hypercoagulability and Mortality of Patients with Stroke and Active Cancer: The OASIS-CANCER Study. J. Stroke 2017, 19, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lau, L.M.; Leebeek, F.W.; de Maat, M.P.; Koudstaal, P.J.; Dippel, D.W. Screening for Coagulation Disorders in Patients with Ischemic Stroke. Expert Rev. Neurother. 2010, 10, 1321–1329. [Google Scholar] [CrossRef]
- Artoni, A.; Bucciarelli, P.; Martinelli, I. Cerebral Thrombosis and Myeloproliferative Neoplasms. Curr. Neurol. Neurosci. Rep. 2014, 14, 496. [Google Scholar] [CrossRef]
- Anker, M.S.; Frey, M.K.; Goliasch, G.; Bartko, P.E.; Prausmüller, S.; Gisslinger, H.; Kornek, G.; Strunk, G.; Raderer, M.; Zielinski, C.; et al. Increased Resting Heart Rate and Prognosis in Treatment-Naïve Unselected Cancer Patients: Results from a Prospective Observational Study. Eur. J. Heart Fail. 2020, 22, 1230–1238. [Google Scholar] [CrossRef] [Green Version]
- Bilora, F.; Biasiolo, M.; Zancan, A.; Zanon, E.; Veronese, F.; Manca, F.; Sartori, M.T. Autonomic Dysfunction and Primary Antiphospholipid Syndrome: A Frequent and Frightening Correlation? Int. J. Gen. Med. 2012, 5, 339–343. [Google Scholar] [CrossRef] [Green Version]
- Haft, J.I.; Kranz, P.D.; Albert, F.J.; Fani, K. Intravascular Platelet Aggregation in the Heart Induced by Norepinephrine. Microscopic Studies. Circulation 1972, 46, 698–708. [Google Scholar] [CrossRef] [Green Version]
- Känel, R.; Dimsdale, J.E. Effects of Sympathetic Activation by Adrenergic Infusions on Hemostasis in Vivo. Eur. J. Haematol. 2000, 65, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Meschia, J.F.; Bushnell, C.; Boden-Albala, B.; Braun, L.T.; Bravata, D.M.; Chaturvedi, S.; Creager, M.A.; Eckel, R.H.; Elkind Mitchell, S.V.; Fornage, M.; et al. Guidelines for the Primary Prevention of Stroke. Stroke 2014, 45, 3754–3832. [Google Scholar] [CrossRef] [Green Version]
- Oppenheimer, S.M.; Cechetto, D.F.; Hachinski, V.C. Cerebrogenic Cardiac Arrhythmias: Cerebral Electrocardiographic Influences and Their Role in Sudden Death. Arch. Neurol. 1990, 47, 513–519. [Google Scholar] [CrossRef]
- Talman, W.T. Cardiovascular regulation and lesions of the central nervous system. Ann. Neurol. 1985, 18, 1–12. [Google Scholar] [CrossRef]
- Kallmünzer, B.; Breuer, L.; Kahl, N.; Bobinger, T.; Raaz-Schrauder, D.; Huttner, H.B.; Schwab, S.; Köhrmann, M. Serious Cardiac Arrhythmias After Stroke. Stroke 2012, 43, 2892–2897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ay, H.; Koroshetz, W.J.; Benner, T.; Vangel, M.G.; Melinosky, C.; Arsava, E.M.; Ayata, C.; Zhu, M.; Schwamm, L.H.; Sorensen, A.G. Neuroanatomic Correlates of Stroke-Related Myocardial Injury. Neurology 2006, 66, 1325–1329. [Google Scholar] [CrossRef]
- Appleton, J.P.; Sprigg, N.; Bath, P.M. Blood Pressure Management in Acute Stroke. Stroke Vasc. Neurol. 2016, 1. [Google Scholar] [CrossRef]
- Ahmed, N.; Wahlgren, G. High Initial Blood Pressure after Acute Stroke Is Associated with Poor Functional Outcome. J. Intern. Med. 2001, 249, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Geeganage, C. Relationship between Baseline Blood Pressure Parameters (Including Mean Pressure, Pulse Pressure, and Variability) and Early Outcome after Stroke: Data from the Tinzaparin in Acute Ischaemic Stroke Trial (TAIST). Stroke 2011, 42, 491–493. [Google Scholar] [CrossRef] [Green Version]
- Sare, G.M.; Ali, M.; Shuaib, A.; Bath, P.M.W.; VISTA Collaboration. Relationship between Hyperacute Blood Pressure and Outcome after Ischemic Stroke: Data from the VISTA Collaboration. Stroke 2009, 40, 2098–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczudlik, A.; Słowik, A.; Dembińska-Kieć, A.; Zdzienicka, A.; Zwolińska, G.; Banach, M. Daily excretion of epinephrine and norepinephrine in acute phase of cerebral ischemia. Neurol. Neurochir. Pol. 1998, 32, 767–778. [Google Scholar] [PubMed]
- Capes, S.E.; Hunt, D.; Malmberg, K.; Pathak, P.; Gerstein, H.C. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: A systematic overview. Stroke 2001, 32, 2426–2432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamorro, Á. Catecholamines, Infection, and Death in Acute Ischemic Stroke. J. Neurol. Sci. 2007, 252, 29–35. [Google Scholar] [CrossRef]
- Harms, H. Influence of Stroke Localization on Autonomic Activation, Immunodepression, and Post-Stroke Infection. Cereb. Dis. 2011, 32, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Sörös, P.; Hachinski, V. Cardiovascular and Neurological Causes of Sudden Death after Ischaemic Stroke. Lancet Neurol. 2012, 11, 179–188. [Google Scholar] [CrossRef]
- Benarroch, E.E. The Central Autonomic Network: Functional Organization, Dysfunction, and Perspective. Mayo Clin. Proc. 1993, 68, 988–1001. [Google Scholar] [CrossRef]
- Benarroch, E.E. Insular Cortex: Functional Complexity and Clinical Correlations. Neurology 2019, 93, 932–938. [Google Scholar] [CrossRef]
- Colivicchi, F.; Bassi, A.; Santini, M.; Caltagirone, C. Cardiac Autonomic Derangement and Arrhythmias in Right-Sided Stroke with Insular Involvement. Stroke 2004, 35, 2094–2098. [Google Scholar] [CrossRef] [Green Version]
- Hilz, M.J.; Dütsch, M.; Perrine, K.; Nelson, P.K.; Rauhut, U.; Devinsky, O. Hemispheric influence on autonomic modulation and baroreflex sensitivity. Ann. Neurol. 2001, 49, 575–584. [Google Scholar] [CrossRef]
- Oppenheimer, S.M.; Gelb, A.; Girvin, J.P.; Hachinski, V.C. Cardiovascular Effects of Human Insular Cortex Stimulation. Neurology 1992, 42, 1727–1732. [Google Scholar] [CrossRef]
- Barron, S.A.; Rogovski, Z.; Hemli, J. Autonomic Consequences of Cerebral Hemisphere Infarction. Stroke 1994, 25, 113–116. [Google Scholar] [CrossRef] [Green Version]
- Meyer, S.; Strittmatter, M.; Fischer, C.; Georg, T.; Schmitz, B. Lateralization in Autonomic Dysfunction in Ischemic Stroke Involving the Insular Cortex. Neuroreport 2004, 15, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Naver, H.K.; Blomstrand, C.; Wallin, B. Gunnar Reduced Heart Rate Variability After Right-Sided Stroke. Stroke 1996, 27, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Tokgözoglu, S.L.; Batur, M.K.; Topçuoglu, M.A.; Saribas, O.; Kes, S.; Oto, A. Effects of Stroke Localization on Cardiac Autonomic Balance and Sudden Death. Stroke 1999, 30, 1307–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korpelainen, J.T.; Sotaniemi, K.A.; Mäkikallio, A.; Huikuri, H.V.; Myllylä, V.V. Dynamic behavior of heart rate in ischemic stroke. Stroke 1999, 30, 1008–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korpelainen, J.T.; Sotaniemi, K.A.; Huikuri, H.V.; Myllylä, V.V. Circadian Rhythm of Heart Rate Variability Is Reversibly Abolished in Ischemic Stroke. Stroke 1997, 28, 2150–2154. [Google Scholar] [CrossRef]
- Korpelainen, J.T.; Sotaniemi, K.A.; Huikuri, H.V.; Myllyä, V.V. Abnormal Heart Rate Variability as a Manifestation of Autonomic Dysfunction in Hemispheric Brain Infarction. Stroke 1996, 27, 2059–2063. [Google Scholar] [CrossRef]
- Chen, C.-F.; Lin, H.-F.; Lin, R.-T.; Yang, Y.-H.; Lai, C.-L. Relationship between Ischemic Stroke Location and Autonomic Cardiac Function. J. Clin. Neurosci. 2013, 20, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Korpelainen, J.T.; Huikuri, H.V.; Sotaniemi, K.A.; Myllylä, V.V. Abnormal heart rate variability reflecting autonomic dysfunction in brainstem infarction. Acta Neurol. Scand. 1996, 94, 337–342. [Google Scholar] [CrossRef]
- Adams, H.P.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. Classification of Subtype of Acute Ischemic Stroke. Definitions for Use in a Multicenter Clinical Trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.-L.; Kuo, T.B.J.; Yang, C.C.H. Parasympathetic Activity Correlates with Early Outcome in Patients with Large Artery Atherosclerotic Stroke. J. Neurol. Sci. 2012, 314, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Kanai, M.; Kubo, H.; Kitamura, Y.; Izawa, K.P.; Ono, K.; Ando, H.; Nozoe, M.; Mase, K.; Shimada, S. Difference in Autonomic Nervous Activity in Different Subtypes of Noncardioembolic Ischemic Stroke. Int. J. Cardiol. 2015, 201, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Nayani, S.; Sreedharan, S.E.; Namboodiri, N.; Sarma, P.S.; Sylaja, P.N. Autonomic Dysfunction in First Ever Ischemic Stroke: Prevalence, Predictors and Short Term Neurovascular Outcome. Clin. Neurol. Neurosurg. 2016, 150, 54–58. [Google Scholar] [CrossRef]
- Gujjar, A.R.; Jaju, D.S.; Jacob, P.C.; Ganguly, S.S.; Al-Asmi, A.R. Serial Hemodynamic and Autonomic Changes in Acute Ischemic Stroke: Relation to Outcome, Stroke Type, and Location. J. Stroke Med. 2020. [Google Scholar] [CrossRef]
- Hilz, M.J. High NIHSS values predict impairment of cardiovascular autonomic control. Stroke 2011, 42, 1528–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuriyama, N.; Mizuno, T.; Niwa, F.; Watanabe, Y.; Nakagawa, M. Autonomic Nervous Dysfunction during Acute Cerebral Infarction. Neurol. Res. 2010, 32, 821–827. [Google Scholar] [CrossRef]
- Sander, D.; Klingelhöfer, J. Extent of Autonomic Activation Following Cerebral Ischemia Is Different in Hypertensive and Normotensive Humans. Arch. Neurol. 1996, 53, 890–894. [Google Scholar] [CrossRef]
- Xiong, L. Comprehensive Assessment for Autonomic Dysfunction in Different Phases after Ischemic Stroke. Int. J. Stroke 2013, 8, 645–651. [Google Scholar] [CrossRef]
- McLaren, A. Autonomic Function Is Impaired in Elderly Stroke Survivors. Stroke 2005, 36, 1026–1030. [Google Scholar] [CrossRef] [Green Version]
- Dütsch, M.; Burger, M.; Dörfler, C.; Schwab, S.; Hilz, M.J. Cardiovascular Autonomic Function in Poststroke Patients. Neurology 2007, 69, 2249–2255. [Google Scholar] [CrossRef]
- Robinson, T.G.; Dawson, S.L.; Eames, P.J.; Panerai, R.B.; Potter, J.F. Cardiac Baroreceptor Sensitivity Predicts Long-Term Outcome after Acute Ischemic Stroke. Stroke 2003, 34, 705–712. [Google Scholar] [CrossRef]
- Toledo, M.E.G. Atrial Fibrillation Detected after Acute Ischemic Stroke: Evidence Supporting the Neurogenic Hypothesis. J. Stroke Cereb. Dis. 2013, 22, 486–491. [Google Scholar] [CrossRef]
- Graff, B. Heart Rate Variability and Functional Outcome in Ischemic Stroke: A Multiparameter Approach. J. Hypertens. 2013, 31, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.-C. Complexity of Heart Rate Variability Predicts Outcome in Intensive Care Unit Admitted Patients with Acute Stroke. J. Neurol. Neurosurg. Psychiatry 2015, 86, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Tobaldini, E. Cardiac Autonomic Derangement Is Associated with Worse Neurological Outcome in the Very Early Phases of Ischemic Stroke. J. Clin. Med. 2019, 8, 852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X. Autonomic Dysfunction Predicts Clinical Outcomes After Acute Ischemic Stroke. Stroke 2018, 49, 215–218. [Google Scholar] [CrossRef]
- Xiong, L. Preliminary Findings of the Effects of Autonomic Dysfunction on Functional Outcome after Acute Ischemic Stroke. Clin. Neurol. Neurosurg. 2012, 114, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H. Complexity of Heart Rate Variability Can Predict Stroke-In-Evolution in Acute Ischemic Stroke Patients. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef]
- Günther, A. Heart Rate Variability—A Potential Early Marker of Sub-Acute Post-Stroke Infections. Acta Neurol. Scand. 2012, 126, 189–196. [Google Scholar] [CrossRef]
- He, L.; Li, C.; Luo, Y.; Dong, W.; Yang, H. Clinical Prognostic Significance of Heart Abnormality and Heart Rate Variability in Patients with Stroke. Neurol. Res. 2010, 32, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Colivicchi, F.; Bassi, A.; Santini, M.; Caltagirone, C. Prognostic Implications of Right-Sided Insular Damage, Cardiac Autonomic Derangement, and Arrhythmias After Acute Ischemic Stroke. Stroke 2005, 36, 1710–1715. [Google Scholar] [CrossRef]
- Mäkikallio, A.M.; Mäkikallio, T.H.; Korpelainen, J.T.; Sotaniemi, K.A.; Huikuri, H.V.; Myllylä, V.V. Heart Rate Dynamics Predict Poststroke Mortality. Neurology 2004, 62, 1822–1826. [Google Scholar] [CrossRef]
- Bassi, A.; Colivicchi, F.; Santini, M.; Caltagirone, C. Cardiac Autonomic Dysfunction and Functional Outcome after Ischaemic Stroke. Eur. J. Neurol. 2007, 14, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Bassi, A.; Colivicchi, F.; Santini, M.; Caltagirone, C. Gender-Specific Predictors of Functional Outcome after Stroke Rehabilitation: Potential Role of the Autonomic Nervous System. Eur. Neurol. 2010, 63, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Arad, M.; Abboud, S.; Radai, M.M.; Adunsky, A. Heart Rate Variability Parameters Correlate with Functional Independence Measures in Ischemic Stroke Patients. J. Electrocardiol. 2002, 35, 243–246. [Google Scholar] [CrossRef]
- Lees, T.; Shad-Kaneez, F.; Simpson, A.M.; Nassif, N.T.; Lin, Y.; Lal, S. Heart Rate Variability as a Biomarker for Predicting Stroke, Post-Stroke Complications and Functionality. Biomarker Insights 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Demaerschalk, B.M.; Kleindorfer, D.O.; Adeoye, O.M.; Demchuk, A.M.; Fugate, J.E.; Grotta, J.C.; Khalessi, A.A.; Levy, E.I.; Palesch, Y.Y.; Prabhakaran, S.; et al. Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke. Stroke 2016, 47, 581–641. [Google Scholar] [CrossRef] [PubMed]
- Gomis, M.; Dávalos, A. Recanalization and Reperfusion Therapies of Acute Ischemic Stroke: What Have We Learned, What Are the Major Research Questions, and Where Are We Headed? Front. Neurol. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Lahr, M.M.H.; Luijckx, G.-J.; Vroomen, P.C.A.J.; van der Zee, D.-J.; Buskens, E. Proportion of Patients Treated With Thrombolysis in a Centralized Versus a Decentralized Acute Stroke Care Setting. Stroke 2012, 43, 1336–1340. [Google Scholar] [CrossRef] [PubMed]
- Béjot, Y.; Bailly, H.; Durier, J.; Giroud, M. Epidemiology of Stroke in Europe and Trends for the 21st Century. Presse Médicale 2016, 45, e391–e398. [Google Scholar] [CrossRef]
- Nour, M.; Scalzo, F.; Liebeskind, D.S. Ischemia-Reperfusion Injury in Stroke. Interv. Neurol. 2013, 1, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Chamorro, Á.; Dirnagl, U.; Urra, X.; Planas, A.M. Neuroprotection in Acute Stroke: Targeting Excitotoxicity, Oxidative and Nitrosative Stress, and Inflammation. Lancet Neurol. 2016, 15, 869–881. [Google Scholar] [CrossRef]
- Mravec, B. The Role of the Vagus Nerve in Stroke. Auton. Neurosci. 2010, 158, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Akdemir, B.; Benditt, D.G. Vagus Nerve Stimulation: An Evolving Adjunctive Treatment for Cardiac Disease. Anatol. J. Cardiol. 2016, 16, 804–810. [Google Scholar] [CrossRef]
- Chakravarthy, K.; Chaudhry, H.; Williams, K.; Christo, P.J. Review of the Uses of Vagal Nerve Stimulation in Chronic Pain Management. Curr. Pain. Headache Rep. 2015, 19, 54. [Google Scholar] [CrossRef] [PubMed]
- Farrand, A.Q.; Helke, K.L.; Aponte-Cofresí, L.; Gooz, M.B.; Gregory, R.A.; Hinson, V.K.; Boger, H.A. Effects of Vagus Nerve Stimulation Are Mediated in Part by TrkB in a Parkinson’s Disease Model. Behav. Brain Res. 2019, 373, 112080. [Google Scholar] [CrossRef] [PubMed]
- Kumaria, A.; Tolias, C.M. Is There a Role for Vagus Nerve Stimulation Therapy as a Treatment of Traumatic Brain Injury? Br. J. Neurosurg. 2012, 26, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Merrill, C.A.; Jonsson, M.A.G.; Minthon, L.; Ejnell, H.; Silander, H.C.; Blennow, K.; Karlsson, M.; Nordlund, A.; Rolstad, S.; Warkentin, S.; et al. Vagus Nerve Stimulation in Patients with Alzheimer’s Disease: Additional Follow-up Results of a Pilot Study through 1 Year. J. Clin. Psychiatry 2006, 67, 1171–1178. [Google Scholar] [CrossRef]
- Zhao, M.; Guan, L.; Wang, Y. The Association of Autonomic Nervous System Function with Ischemic Stroke, and Treatment Strategies. Front. Neurol. 2020, 10, 1411. [Google Scholar] [CrossRef]
- Tobaldini, E.; Toschi-Dias, E.; Appratto de Souza, L.; Rabello Casali, K.; Vicenzi, M.; Sandrone, G.; Cogliati, C.; La Rovere, M.T.; Pinna, G.D.; Montano, N. Cardiac and Peripheral Autonomic Responses to Orthostatic Stress During Transcutaneous Vagus Nerve Stimulation in Healthy Subjects. J. Clin. Med. 2019, 8, 496. [Google Scholar] [CrossRef] [Green Version]
- Duris, K.; Lipkova, J.; Jurajda, M. Cholinergic Anti-Inflammatory Pathway and Stroke. Curr. Drug Deliv. 2017, 14, 449–457. [Google Scholar] [CrossRef]
- Jiang, Y.; Li, L.; Liu, B.; Zhang, Y.; Chen, Q.; Li, C. Vagus Nerve Stimulation Attenuates Cerebral Ischemia and Reperfusion Injury via Endogenous Cholinergic Pathway in Rat. PLoS ONE 2014, 9, e102342. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Q.; Li, S.; Niu, L.; Ma, J.; Wen, L.; Zhang, L.; Li, C. A7nAchR Mediates Transcutaneous Auricular Vagus Nerve Stimulation-Induced Neuroprotection in a Rat Model of Ischemic Stroke by Enhancing Axonal Plasticity. Neurosci. Lett. 2020, 730, 135031. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.-X.; Hong, Z.-Q.; Tan, Z.; Sui, M.-H.; Zhuang, Z.-Q.; Liu, H.-H.; Zheng, X.-Y.; Yan, T.-B.; Geng, D.-F.; Jin, D.-M. Nicotinic Acetylcholine Receptor Alpha7 Subunit Mediates Vagus Nerve Stimulation-Induced Neuroprotection in Acute Permanent Cerebral Ischemia by A7nAchR/JAK2 Pathway. Med. Sci. Monit. 2017, 23, 6072–6081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, R.; Yang, G.; Li, G. Inflammatory Mechanisms in Ischemic Stroke: Role of Inflammatory Cells. J. Leukoc. Biol. 2010, 87, 779–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakhan, S.E.; Kirchgessner, A.; Hofer, M. Inflammatory Mechanisms in Ischemic Stroke: Therapeutic Approaches. J. Transl. Med. 2009, 7, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Li, L.; Liu, B.; Zhang, Y.; Chen, Q.; Li, C. PPARγ Upregulation Induced by Vagus Nerve Stimulation Exerts Anti-Inflammatory Effect in Cerebral Ischemia/Reperfusion Rats. Med. Sci. Monit. 2015, 21, 268–275. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.; Wang, W.; Xue, Z.; Zhu, L.; Wang, S.; Sun, Z. Electrical Stimulation of the Vagus Nerve Protects against Cerebral Ischemic Injury through an Anti-Infammatory Mechanism. Neural Regen. Res. 2015, 10, 576. [Google Scholar] [CrossRef]
- El Kasmi, K.C.; Holst, J.; Coffre, M.; Mielke, L.; de Pauw, A.; Lhocine, N.; Smith, A.M.; Rutschman, R.; Kaushal, D.; Shen, Y.; et al. General Nature of the STAT3-Activated Anti-Inflammatory Response. J. Immunol. 2006, 177, 7880–7888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchins, A.P.; Diez, D.; Miranda-Saavedra, D. The IL-10/STAT3-Mediated Anti-Inflammatory Response: Recent Developments and Future Challenges. Brief Funct. Genom. 2013, 12, 489–498. [Google Scholar] [CrossRef] [Green Version]
- Neumann, S.; Shields, N.J.; Balle, T.; Chebib, M.; Clarkson, A.N. Innate Immunity and Inflammation Post-Stroke: An A7-Nicotinic Agonist Perspective. Int. J. Mol. Sci. 2015, 16, 29029–29046. [Google Scholar] [CrossRef] [Green Version]
- De Jonge, W.J.; van der Zanden, E.P.; The, F.O.; Bijlsma, M.F.; van Westerloo, D.J.; Bennink, R.J.; Berthoud, H.-R.; Uematsu, S.; Akira, S.; van den Wijngaard, R.M.; et al. Stimulation of the Vagus Nerve Attenuates Macrophage Activation by Activating the Jak2-STAT3 Signaling Pathway. Nat. Immunol. 2005, 6, 844–851. [Google Scholar] [CrossRef]
- Xia, C.-Y.; Zhang, S.; Gao, Y.; Wang, Z.-Z.; Chen, N.-H. Selective Modulation of Microglia Polarization to M2 Phenotype for Stroke Treatment. Int. Immunopharmacol. 2015, 25, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Li, P.; Guo, Y.; Wang, H.; Leak, R.K.; Chen, S.; Gao, Y.; Chen, J. Microglia/Macrophage Polarization Dynamics Reveal Novel Mechanism of Injury Expansion After Focal Cerebral Ischemia. Stroke 2012, 43, 3063–3070. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.-P.; Zhao, Y.; Qin, X.-Y.; Wan, L.-Y.; Fan, X.-X. Non-Invasive Vagus Nerve Stimulation Protects Against Cerebral Ischemia/Reperfusion Injury and Promotes Microglial M2 Polarization Via Interleukin-17A Inhibition. J. Mol. Neurosci. 2019, 67, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Ekici, F.; Karson, A.; Dillioglugil, M.O.; Gurol, G.; Kir, H.M.; Ates, N. The Effects of Vagal Nerve Stimulation in Focal Cerebral Ischemia and Reperfusion Model. Turk. Neurosurg. 2013, 23, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Han, Z.; Shen, F.; He, Y.; Degos, V.; Camus, M.; Maze, M.; Young, W.L.; Su, H. Activation of α-7 Nicotinic Acetylcholine Receptor Reduces Ischemic Stroke Injury through Reduction of Pro-Inflammatory Macrophages and Oxidative Stress. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Parada, E.; Egea, J.; Buendia, I.; Negredo, P.; Cunha, A.C.; Cardoso, S.; Soares, M.P.; López, M.G. The Microglial A7-Acetylcholine Nicotinic Receptor Is a Key Element in Promoting Neuroprotection by Inducing Heme Oxygenase-1 via Nuclear Factor Erythroid-2-Related Factor 2. Antioxid. Redox Signal. 2013, 19, 1135–1148. [Google Scholar] [CrossRef] [Green Version]
- Egea, J.; Martín-de-Saavedra, M.D.; Parada, E.; Romero, A.; del Barrio, L.; Rosa, A.O.; García, A.G.; López, M.G. Galantamine Elicits Neuroprotection by Inhibiting INOS, NADPH Oxidase and ROS in Hippocampal Slices Stressed with Anoxia/Reoxygenation. Neuropharmacology 2012, 62, 1082–1090. [Google Scholar] [CrossRef]
- Jiang, Y.; Li, L.; Tan, X.; Liu, B.; Zhang, Y.; Li, C. MiR-210 Mediates Vagus Nerve Stimulation-Induced Antioxidant Stress and Anti-Apoptosis Reactions Following Cerebral Ischemia/Reperfusion Injury in Rats. J. Neurochem. 2015, 134, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Mutharasan, R.K.; Nagpal, V.; Ichikawa, Y.; Ardehali, H. MicroRNA-210 Is Upregulated in Hypoxic Cardiomyocytes through Akt- and P53-Dependent Pathways and Exerts Cytoprotective Effects. Am. J. Physiol. Heart Circ. Physiol. 2011, 301, H1519–H1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Ma, J.; Jin, X.; Jia, G.; Jiang, Y.; Li, C. L-PGDS Mediates Vagus Nerve Stimulation-Induced Neuroprotection in a Rat Model of Ischemic Stroke by Suppressing the Apoptotic Response. Neurochem. Res. 2017, 42, 644–655. [Google Scholar] [CrossRef]
- Saleem, S.; Shah, Z.A.; Urade, Y.; Doré, S. Lipocalin-Prostaglandin D Synthase Is a Critical Beneficial Factor in Transient and Permanent Focal Cerebral Ischemia. Neuroscience 2009, 160, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Engineer, N.D.; Kimberley, T.J.; Prudente, C.N.; Dawson, J.; Tarver, W.B.; Hays, S.A. Targeted Vagus Nerve Stimulation for Rehabilitation After Stroke. Front. Neurosci. 2019, 13, 280. [Google Scholar] [CrossRef] [Green Version]
- Meyers, E.C.; Solorzano, B.R.; James, J.; Ganzer, P.D.; Lai, E.S.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Vagus Nerve Stimulation Enhances Stable Plasticity and Generalization of Stroke Recovery. Stroke 2018, 49, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Hays, S.A.; Rennaker, R.L.; Kilgard, M.P. Targeting Plasticity with Vagus Nerve Stimulation to Treat Neurological Disease. Prog. Brain Res. 2013, 207, 275–299. [Google Scholar] [CrossRef] [Green Version]
- Pabst, M.; Braganza, O.; Dannenberg, H.; Hu, W.; Pothmann, L.; Rosen, J.; Mody, I.; van Loo, K.; Deisseroth, K.; Becker, A.J.; et al. Astrocyte Intermediaries of Septal Cholinergic Modulation in the Hippocampus. Neuron 2016, 90, 853–865. [Google Scholar] [CrossRef] [Green Version]
- Palacios-Filardo, J.; Mellor, J.R. Neuromodulation of Hippocampal Long-Term Synaptic Plasticity. Curr. Opin. Neurobiol. 2019, 54, 37–43. [Google Scholar] [CrossRef]
- Papouin, T.; Dunphy, J.; Tolman, M.; Dineley, K.T.; Haydon, P.G. Septal Cholinergic Neuromodulation Tunes the Astrocyte-Dependent Gating of Hippocampal NMDA Receptors to Wakefulness. Neuron 2017, 94, 840–854. [Google Scholar] [CrossRef] [Green Version]
- Hays, S.A.; Khodaparast, N.; Ruiz, A.; Sloan, A.M.; Hulsey, D.R.; Rennaker, R.L.; Kilgard, M.P. The Timing and Amount of Vagus Nerve Stimulation during Rehabilitative Training Affect Poststroke Recovery of Forelimb Strength. Neuroreport 2014, 25, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Kilgard, M.P. Harnessing Plasticity to Understand Learning and Treat Disease. Trends Neurosci. 2012, 35, 715–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khodaparast, N.; Hays, S.A.; Sloan, A.M.; Fayyaz, T.; Hulsey, D.R.; Rennaker, R.L.; Kilgard, M.P. Vagus Nerve Stimulation Delivered during Motor Rehabilitation Improves Recovery in a Rat Model of Stroke. Neurorehabil. Neural Repair 2014, 28, 698–706. [Google Scholar] [CrossRef] [Green Version]
- Dawson, J.; Pierce, D.; Dixit, A.; Kimberley, T.J.; Robertson, M.; Tarver, B.; Hilmi, O.; McLean, J.; Forbes, K.; Kilgard, M.P.; et al. Safety, Feasibility, and Efficacy of Vagus Nerve Stimulation Paired with Upper-Limb Rehabilitation After Ischemic Stroke. Stroke 2016, 47, 143–150. [Google Scholar] [CrossRef]
- Kimberley, T.J.; Pierce, D.; Prudente, C.N.; Francisco, G.E.; Yozbatiran, N.; Smith, P.; Tarver, B.; Engineer, N.D.; Alexander, D.D.; Kline, D.K.; et al. Vagus Nerve Stimulation Paired with Upper Limb Rehabilitation After Chronic Stroke. Stroke 2018, 49, 2789–2792. [Google Scholar] [CrossRef] [Green Version]
- Morrison, R.A.; Danaphongse, T.T.; Pruitt, D.T.; Adcock, K.S.; Mathew, J.K.; Abe, S.T.; Abdulla, D.M.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. A Limited Range of Vagus Nerve Stimulation Intensities Produce Motor Cortex Reorganization When Delivered during Training. Behav. Brain Res. 2020, 391, 112705. [Google Scholar] [CrossRef] [PubMed]
- Pruitt, D.T.; Danaphongse, T.T.; Lutchman, M.; Patel, N.; Reddy, P.; Wang, V.; Parashar, A.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Optimizing Dosing of Vagus Nerve Stimulation for Stroke Recovery. Transl. Stroke Res. 2020. [Google Scholar] [CrossRef]
- Hulsey, D.R.; Riley, J.R.; Loerwald, K.W.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Parametric Characterization of Neural Activity in the Locus Coeruleus in Response to Vagus Nerve Stimulation. Exp. Neurol. 2017, 289, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Morrison, R.A.; Hulsey, D.R.; Adcock, K.S.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Vagus Nerve Stimulation Intensity Influences Motor Cortex Plasticity. Brain Stimul. 2019, 12, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Gainetdinov, R.R.; Premont, R.T.; Bohn, L.M.; Lefkowitz, R.J.; Caron, M.G. Desensitization of g Protein–Coupled Receptors and Neuronal Functions. Annu. Rev. Neurosci. 2004, 27, 107–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salgado, H.; Köhr, G.; Treviño, M. Noradrenergic ‘Tone’ Determines Dichotomous Control of Cortical Spike-Timing-Dependent Plasticity. Sci. Rep. 2012, 2, 417. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Li, L.; Ma, J.; Zhang, L.; Niu, F.; Feng, T.; Li, C. Auricular Vagus Nerve Stimulation Promotes Functional Recovery and Enhances the Post-Ischemic Angiogenic Response in an Ischemia/Reperfusion Rat Model. Neurochem. Int. 2016, 97, 73–82. [Google Scholar] [CrossRef]
- Li, J.; Zhang, K.; Zhang, Q.; Zhou, X.; Wen, L.; Ma, J.; Niu, L.; Li, C. PPAR-γ Mediates Ta-VNS-Induced Angiogenesis and Subsequent Functional Recovery after Experimental Stroke in Rats. Biomed. Res. Int. 2020, 2020, 8163789. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Zhang, L.; Niu, T.; Ai, C.; Jia, G.; Jin, X.; Wen, L.; Zhang, K.; Zhang, Q.; Li, C. Growth Differentiation Factor 11 Improves Neurobehavioral Recovery and Stimulates Angiogenesis in Rats Subjected to Cerebral Ischemia/Reperfusion. Brain Res. Bull. 2018, 139, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Ay, I.; Sorensen, A.G.; Ay, H. Vagus Nerve Stimulation Reduces Infarct Size in Rat Focal Cerebral Ischemia: An Unlikely Role for Cerebral Blood Flow. Brain Res. 2011, 1392, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Ay, I.; Lu, J.; Ay, H.; Gregory, S.A. Vagus Nerve Stimulation Reduces Infarct Size in Rat Focal Cerebral Ischemia. Neurosci. Lett. 2009, 459, 147–151. [Google Scholar] [CrossRef]
- Hiraki, T.; Baker, W.; Greenberg, J.H. Effect of Vagus Nerve Stimulation during Transient Focal Cerebral Ischemia on Chronic Outcome in Rats. J. Neurosci. Res. 2012, 90, 887–894. [Google Scholar] [CrossRef] [Green Version]
- Sun, Z.; Baker, W.; Hiraki, T.; Greenberg, J.H. The Effect of Right Vagus Nerve Stimulation on Focal Cerebral Ischemia: An Experimental Study in the Rat. Brain Stimul. 2012, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ay, I.; Nasser, R.; Simon, B.; Ay, H. Transcutaneous Cervical Vagus Nerve Stimulation Ameliorates Acute Ischemic Injury in Rats. Brain Stimul. 2016, 9, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Ay, I.; Napadow, V.; Ay, H. Electrical Stimulation of the Vagus Nerve Dermatome in the External Ear Is Protective in Rat Cerebral Ischemia. Brain Stimul. 2015, 8, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Yang, L.Y.; Orban, L.; Cuylear, D.; Thompson, J.; Simon, B.; Yang, Y. Non-Invasive Vagus Nerve Stimulation Reduces Blood-Brain Barrier Disruption in a Rat Model of Ischemic Stroke. Brain Stimul. 2018, 11, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Zhang, L.; He, G.; Tan, X.; Jin, X.; Li, C. Transcutaneous Auricular Vagus Nerve Stimulation Regulates Expression of Growth Differentiation Factor 11 and Activin-like Kinase 5 in Cerebral Ischemia/Reperfusion Rats. J. Neurol. Sci. 2016, 369, 27–35. [Google Scholar] [CrossRef]
- Khodaparast, N.; Hays, S.A.; Sloan, A.M.; Hulsey, D.R.; Ruiz, A.; Pantoja, M.; Rennaker, R.L.; Kilgard, M.P. Vagus Nerve Stimulation during Rehabilitative Training Improves Forelimb Strength Following Ischemic Stroke. Neurobiol. Dis. 2013, 60, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Khodaparast, N.; Kilgard, M.P.; Casavant, R.; Ruiz, A.; Qureshi, I.; Ganzer, P.D.; Rennaker, R.L.; Hays, S.A. Vagus Nerve Stimulation During Rehabilitative Training Improves Forelimb Recovery After Chronic Ischemic Stroke in Rats. Neurorehabil. Neural Repair 2016, 30, 676–684. [Google Scholar] [CrossRef] [Green Version]
- Dawson, J.; Engineer, N.D.; Prudente, C.N.; Pierce, D.; Francisco, G.; Yozbatiran, N.; Tarver, W.B.; Casavant, R.; Kline, D.K.; Cramer, S.C.; et al. Vagus Nerve Stimulation Paired with Upper-Limb Rehabilitation After Stroke: One-Year Follow-Up. Neurorehabil. Neural Repair 2020, 34, 609–615. [Google Scholar] [CrossRef]
- Capone, F.; Miccinilli, S.; Pellegrino, G.; Zollo, L.; Simonetti, D.; Bressi, F.; Florio, L.; Ranieri, F.; Falato, E.; Di Santo, A.; et al. Transcutaneous Vagus Nerve Stimulation Combined with Robotic Rehabilitation Improves Upper Limb Function after Stroke. Available online: https://www.hindawi.com/journals/np/2017/7876507/ (accessed on 16 July 2020).
- Baig, S.S.; Falidas, K.; Laud, P.J.; Snowdon, N.; Farooq, M.U.; Ali, A.; Majid, A.; Redgrave, J.N. Transcutaneous Auricular Vagus Nerve Stimulation with Upper Limb Repetitive Task Practice May Improve Sensory Recovery in Chronic Stroke. J. Stroke Cereb. Dis. 2019, 28, 104348. [Google Scholar] [CrossRef]
- Redgrave, J.N.; Moore, L.; Oyekunle, T.; Ebrahim, M.; Falidas, K.; Snowdon, N.; Ali, A.; Majid, A. Transcutaneous Auricular Vagus Nerve Stimulation with Concurrent Upper Limb Repetitive Task Practice for Poststroke Motor Recovery: A Pilot Study. J. Stroke Cerebrovasc. Dis. 2018, 27, 1998–2005. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carandina, A.; Lazzeri, G.; Villa, D.; Di Fonzo, A.; Bonato, S.; Montano, N.; Tobaldini, E. Targeting the Autonomic Nervous System for Risk Stratification, Outcome Prediction and Neuromodulation in Ischemic Stroke. Int. J. Mol. Sci. 2021, 22, 2357. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22052357
Carandina A, Lazzeri G, Villa D, Di Fonzo A, Bonato S, Montano N, Tobaldini E. Targeting the Autonomic Nervous System for Risk Stratification, Outcome Prediction and Neuromodulation in Ischemic Stroke. International Journal of Molecular Sciences. 2021; 22(5):2357. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22052357
Chicago/Turabian StyleCarandina, Angelica, Giulia Lazzeri, Davide Villa, Alessio Di Fonzo, Sara Bonato, Nicola Montano, and Eleonora Tobaldini. 2021. "Targeting the Autonomic Nervous System for Risk Stratification, Outcome Prediction and Neuromodulation in Ischemic Stroke" International Journal of Molecular Sciences 22, no. 5: 2357. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22052357