
CD28null and Regulatory T Cells Are Substantially Disrupted in Patients with End-Stage Renal Disease Due to Diabetes Mellitus


Abstract
:1. Introduction
2. Results
2.1. Alterations of T Lymphocytes and Their Subpopulations Patients at ESRD-T0
2.1.1. Differences in Neutrophils and Lymphocyte Cells
2.1.2. Differences in CD3+CD4+ and CD3+CD8+ Cells
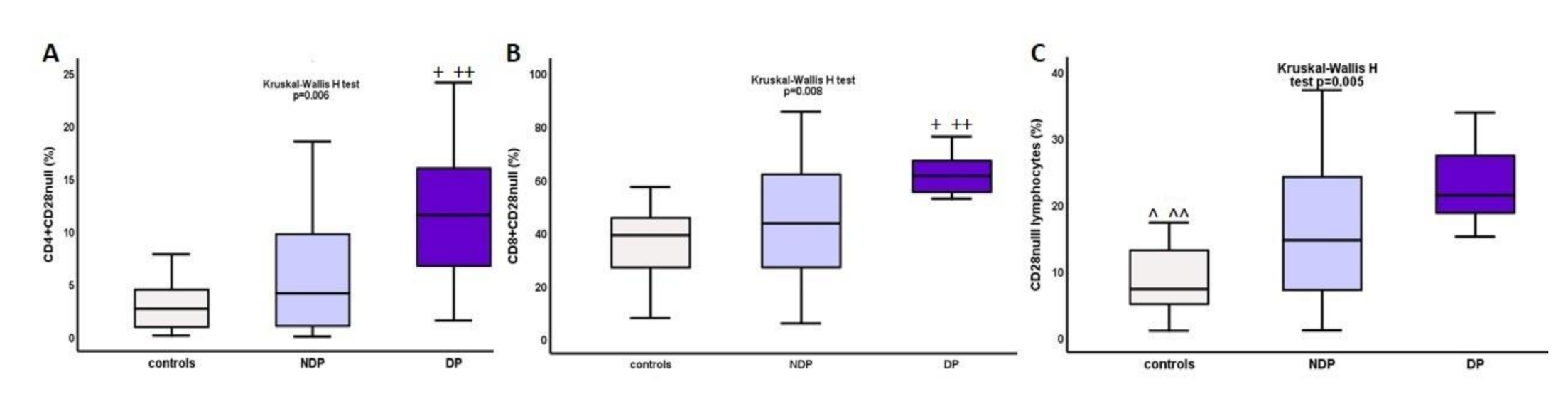
2.1.3. Increase in CD4+CD28null and CD8+CD28null Cells in ESRD and DM
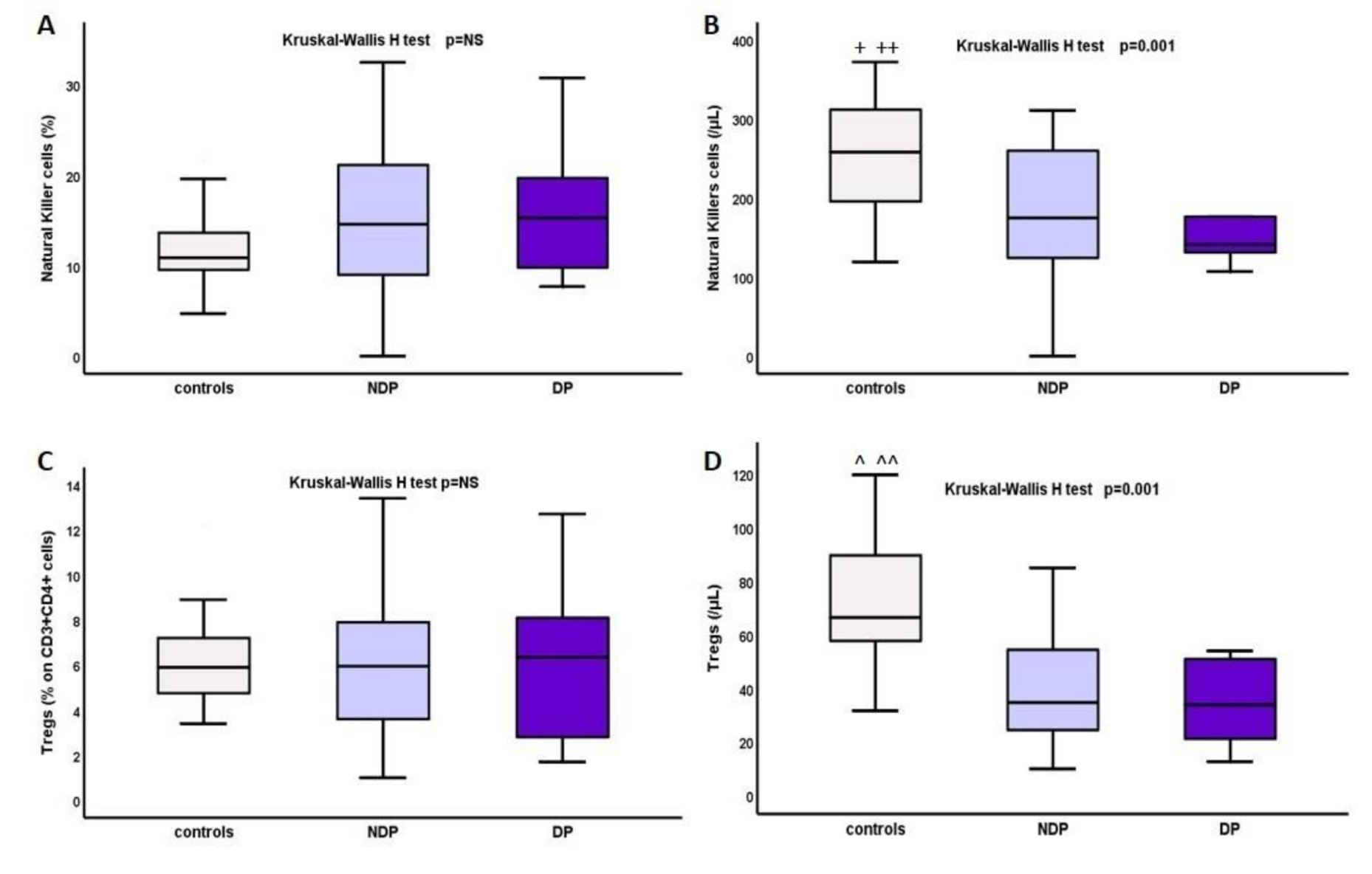
2.1.4. Changes in Natural Killer Cells and Tregs
2.2. Influence of Dialysis on T Lymphocytes—Different Effects after Applying HD or CAPD
3. Discussion
4. Materials and Methods
4.1. Study Schedule
4.2. Patients
4.3. Laboratory Measurements
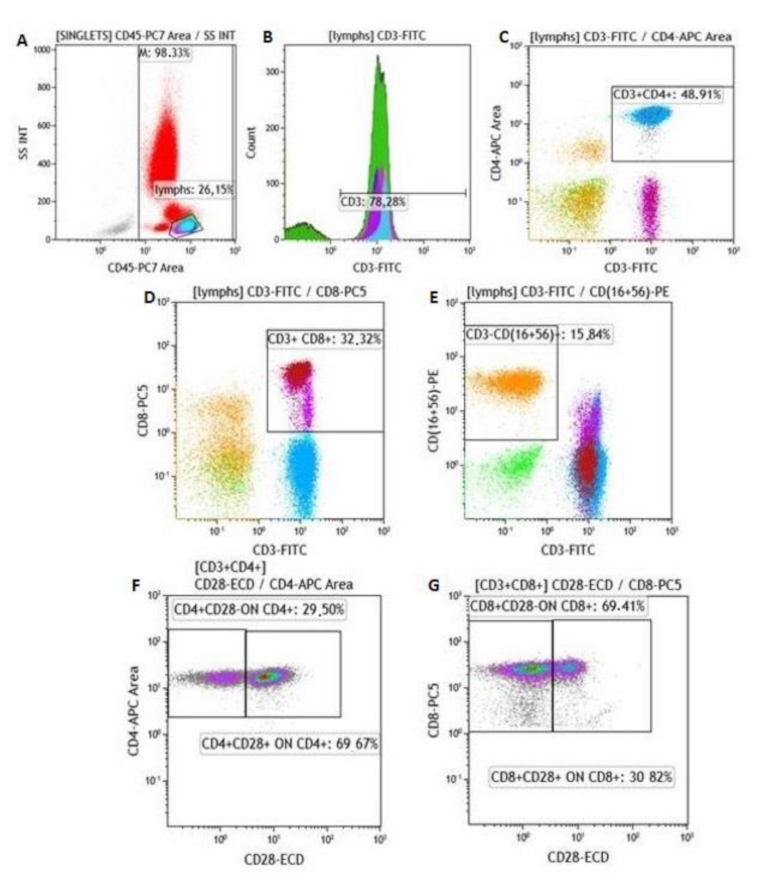
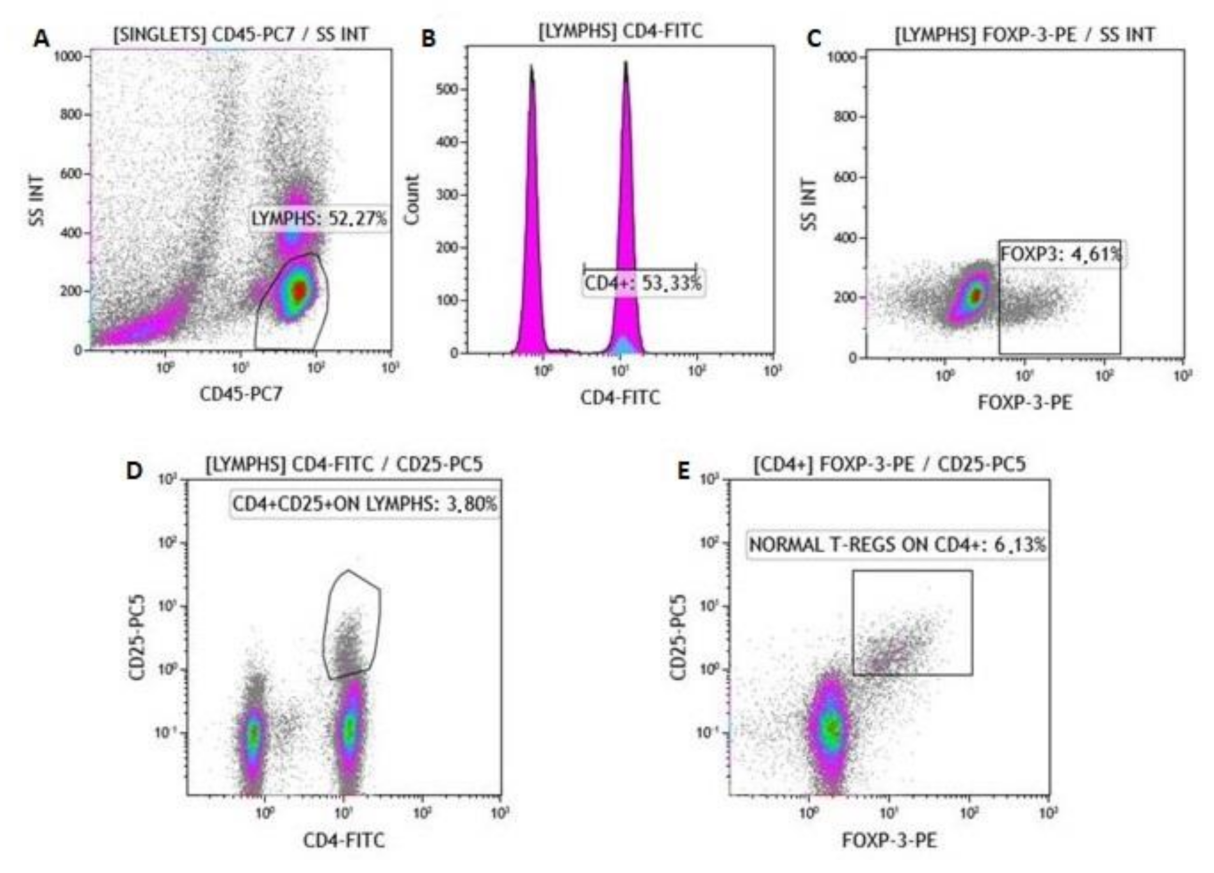
Flow Cytometry
5. Statistics
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, G. Immune dysfunction in Uremia 2020. Toxins 2020, 12, 439. [Google Scholar] [CrossRef]
- Dounousi, E.; Papavasiliou, E.; Makedou, A.; Ioannou, K.; Katopodis, K.P.; Tselepis, A.; Siamopoulos, K.C.; Tsakiris, D. Oxidative stress is progressively enhanced with advancing stages of CKD. Am. J. Kidney Dis. 2006, 48, 752–760. [Google Scholar] [CrossRef] [Green Version]
- Suvakov, S.; Jerotic, D.; Damjanovic, T.; Milic, N.; Pekmezovic, T.; Djukic, T.; Jelic-Ivanovic, Z.; SavicRadojevic, A.; Pljesa-Ercegovac, M.; Matic, M.; et al. Markers of Oxidative Stress and Endothelial Dysfunction Predict Haemodialysis Patients Survival. Am. J. Nephrol. 2019, 50, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Lioulios, G.; Fylaktou, M.; Papagianni, A.; Stangou, M. T cell markers recount the course of immunosenescence in healthy individuals and chronic kidney disease. Clin. Immunol. 2021, 108685. [Google Scholar] [CrossRef] [PubMed]
- Sattler, S. The Role of the ImmuneSystem Beyond the Fight Against Infection. Adv. Exp. Med. Biol. 2017, 1003, 3–14. [Google Scholar] [CrossRef]
- Parkin, J.; Cohen, B. An overview of the immunesystem. Lancet 2001, 357, 1777–1789. [Google Scholar] [CrossRef]
- Betjes, M.G. Immune cell dysfunction and inflammation in end-stagerenaldisease. Nat. Rev. Nephrol. 2013, 9, 255–265. [Google Scholar] [CrossRef]
- Litjens, N.H.; van Druningen, C.J.; Betjes, M.G. Progressive loss of renal function is associated with activation and depletion of naive T lymphocytes. Clin. Immunol. 2006, 118, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Betjes, M.G.; Litjens, N.H. Chronic kidney disease and premature ageing of the adaptive immune response. Curr. Urol. Rep. 2015, 16, 471. [Google Scholar] [CrossRef]
- Sampani, E.; Stangou, M.; Daikidou, D.V.; Nikolaidou, V.; Asouchidou, D.; Dimitriadis, C.; Lioulios, G.; Xochelli, A.; Fylaktou, A.; Papagianni, A. Influence of end stage renal disease on CD28 expression and T-cell immunity. Nephrology 2021, 26, 185–196. [Google Scholar] [CrossRef]
- Okba, A.M.; Raafat, M.; Farres, M.N.; Melek, N.; Amin, M.; Gendy, N. Expanded peripheral CD4 + CD28 null T cells and its association with atherosclerotic changes in patients with end stage renal disease on hemodialysis. Hum. Immunol. 2019, 80, 748–754. [Google Scholar] [CrossRef]
- Sun, Z.; Ye, H.; Tang, B.; Shen, X.; Wu, X.; Zhong, H.; Song, W. Prevalence of circulating CD4+CD28null T cells is associated with early atherosclerotic damage in patients with end-stage renal disease undergoing hemodialysis. Hum. Immunol. 2013, 74, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, A.; Turka, L.A. FOXP3-Positive Regulatory T Cells and Kidney Allograft Tolerance. Am. J. Kidney Dis. 2017, 69, 667–674. [Google Scholar] [CrossRef] [Green Version]
- Ren, T.; Xiong, J.; Liu, G.; Wang, S.; Tan, Z.; Fu, B.; Zhang, R.; Liao, X.; Wang, Q.; Guo, Z. Imbalance of Th22/Treg cells causes microinflammation in uremic patients undergoing hemodialysis. Biosci. Rep. 2019, 39, BSR20191585. [Google Scholar] [CrossRef] [Green Version]
- Mahajan, D.; Wang, Y.; Qin, X.; Wang, Y.; Zheng, G.; Wang, Y.M.; Alexander, S.; Harris, D. CD4+CD25+ regulatory T cells protect against injury in an innate murine model of chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 2731–2741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigal, L.H. Basic science for the clinician 56: Inducible T-cell costimulator--the world of costimulation gets more complicated…and interesting. J. Clin. Rheumatol. 2012, 18, 212–216. [Google Scholar] [CrossRef]
- Rochman, Y.; Yukawa, M.; Kartashov, A.V.; Barski, A. Functional characterization of human T cell hyporesponsiveness induced by CTLA4-Ig. PLoS ONE 2015, 10, e0122198. [Google Scholar] [CrossRef] [Green Version]
- Tesch, G.H. Diabetic nephropathy-is this an immune disorder? Clin. Sci. 2017, 131, 2183–2199. [Google Scholar] [CrossRef]
- Zoll, B.; Lefterova, P.; Ebert, O.; Huhn, D.; Von Ruecker, A. Schmidt-WolfI G Modulation of cell surface markers on NK-like T lymphocytes by using IL-2, IL-7 or IL-12 in vitro stimulation. Cytokine 2000, 12, 1385–1390. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.M.; Ghali, J.; Zhang, G.Y.; Hu, M.; Wang, Y.; Sawyer, A.; Zhou, J.J.; Hapudeniya, D.A.; Wang, Y.; Cao, Q.; et al. Development and function of Foxp3(+) regulatory T cells. Nephrology 2016, 21, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Bayati, F.; Mohammadi, M.; Valadi, M.; Jamshidi, S.; Foma, A.M.; Sharif-Paghaleh, E. The Therapeutic Potential of RegulatoryT Cells: Challenges and Opportunities. Front. Immunol. 2021, 11, 585819. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.C.; Zhang, L.X. Prevalence and Disease Burden of ChronicKidneyDisease. Adv. Exp. Med. Biol. 2019, 1165, 3–15. [Google Scholar] [PubMed]
- Lobo, T.F.; Borges, C.M.; Mattar, R.; Gomes, C.P.; de Angelo, A.G.S.; Pendeloski, K.P.T.; Daher, S. Impaired Treg and NK cells profile in overweight women with gestational diabetesmellitus. Am. J. Reprod. Immunol. 2018, 79. [Google Scholar] [CrossRef]
- Ighodaro, O.M. Molecular pathways associated with oxidative stress in diabetesmellitus. Biomed. Pharmacother. 2018, 108, 656–662. [Google Scholar] [CrossRef]
- Fiorentino, T.V.; Prioletta, A.; Zuo, P.; Folli, F. Hyperglycemia-induced oxidativestress and its role in diabetesmellitus related cardiovascular diseases. Curr. Pharm. Des. 2013, 19, 5695–5703. [Google Scholar] [CrossRef] [PubMed]
- Rask-Madsen, C.; King, G.L. Vascular complications of diabetes: Mechanisms of injury and protective factors. Cell Metab. 2013, 17, 20–33. [Google Scholar] [CrossRef] [Green Version]
- Hasnain, S.Z.; Prins, J.B.; McGuckin, M.A. Oxidative and endoplasmicreticulumstress in beta-cell dysfunction in diabetes. J. Mol. Endocrinol. 2016, 56, R33–R54. [Google Scholar] [CrossRef] [Green Version]
- Lampropoulou, I.T.; Stangou, M.; Papagianni, A.; Didangelos, T.; Iliadis, F.; Efstratiadis, G. TNF-α and microalbuminuria in patients with type 2 diabetes mellitus. J. Diabetes. Res. 2014, 2014, 394206. [Google Scholar] [CrossRef] [Green Version]
- Lampropoulou, I.T.; Stangou, Μ.; Sarafidis, P.; Gouliovaki, A.; Giamalis, P.; Tsouchnikas, I.; Didangelos, T.; Papagianni, A. TNF-α pathway and T-cell immunity are activated early during the development of diabetic nephropathy in Type II Diabetes Mellitus. Clin. Immunol. 2020, 215, 108423. [Google Scholar] [CrossRef]
- Li, T.; Yu, Z.; Qu, Z.; Zhang, N.; Crew, R.; Jiang, Y. Decreased number of CD19+CD24hiCD38hi regulatory B cells in Diabetic nephropathy. Mol. Immunol. 2019, 112, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Lavoz, C.; Matus, Y.S.; Orejudo, M.; Carpio, J.D.; Droguett, A.; Egido, J.; Mezzano, S.; Ruiz-Ortega, M. Interleukin-17A blockade reduces albuminuria and kidney injury in an accelerated model of diabeticnephropathy. Kidney Int. 2019, 95, 1418–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzman-Flores, J.M.; Ramírez-Emiliano, J.; Pérez-Vázquez, V.; López-Briones, S. Th17 and regulatory T cells in patients with different time of progression of type 2 diabetes mellitus. Cent. Eur. J. Immunol. 2020, 45, 29–36. [Google Scholar] [CrossRef] [PubMed]
- El-Samahy, M.; Tantawy, A.; Adly, A.; Habeeb, N.; Ismail, E.; Hamed, G.; Eladawy, R. Expression of CD4+CD28null T lymphocytes in children and adolescents with type 1 diabetes mellitus: Relation to microvascular complications, aortic elastic properties, and carotid intima media thickness. Pediatr. Diabetes 2017, 18, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Crépin, T.; Legendre, M.; Carron, C.; Vachey, C.; Courivaud, C.; Rebibou, J.M.; Ferrand, C.; Laheurte, C.; Vauchy, C.; Gaiffe, E.; et al. Uraemia-induced immune senescence and clinical outcomes in chronic kidney disease patients. Nephrol. Dial. Transplant. 2020, 35, 624–632. [Google Scholar] [CrossRef] [Green Version]
- Caprara, C.; Corradi, V.; Scalzotto, E.; Frigo, A.C.; Proglio, M.; Sharma, R.; Ronco, C. Differential effects of peritoneal and hemodialysis on circulating regulatory T cells one month post initiation of renal replacement therapy. Clin. Nephrol. 2021, 95, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Jiao, X.; Chen, R.; Cao, X.; Zou, J.; Ji, J.; Ding, X.; Yu, X. The difference of T cell phenotypes in end stage renal disease patients under different dialysis modality. BMC Nephrol. 2019, 20, 301. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DM | NDM | p | |
|---|---|---|---|
| N | 28 | 28 | |
| Systolic blood pressure (SBP) | 144 ± 26 | 140 ± 25 | NS |
| Diastolic dlood pressure (DBP) | 85 ± 23 | 74 ± 31 | NS |
| Intimal–medial thickness (IMT) | 0.06 ± 0.01 | 0.05 ± 0.01 | NS |
| IMTmax | 0.16 ± 0.23 | 0.06 ± 0.01 | NS |
| Comorbid conditions or habits | |||
| Smoking (%) | 14 (50) | 13 (46.42) | NS |
| Coronary artery disease (%) | 19 (67.85) | 16 (57.14) | NS |
| Peripheral artery disease (%) | 13 (46.42) | 4 (14.28) | NS |
| Stroke (%) | 2 (7.14) | 1 (3.5) | NS |
| Dyslipidemia (%) | 19 (67.85) | 16 (57.14) | NS |
| DM | NDM | Controls | p | p (DM vs. NDM) | |
|---|---|---|---|---|---|
| N | 28 | 28 | 25 | ||
| WCC (K/μL) | 7600 ± 2076 | 7399 ± 2365 | 6726 ± 1314 | NS | NS |
| Neutrophils (K/μL) | 5927 ± 1729 | 5029 ± 1985 | 4061 ± 1444 | 0.02 | NS |
| Neutrophils (%) | 72 ± 10 | 68 ± 7.5 | 59 ± 13 | 0.008 | NS |
| Lymphocytes (K/μL) | 1212 ± 564 | 1435 ± 596 | 2198 ± 556 | 0.0001 | NS |
| Lymphocytes (%) | 16.5 ± 9.4 | 19.5 ± 6 | 33.6 ± 9.4 | 0.0001 | NS |
| NLR | 6 ± 4.9 | 3.9 ± 2 | 2 ± 1.1 | 0.0001 | NS |
| T-cell subtypes | |||||
| CD3+CD4+ cells | 622(150–1412) | 693.9(224–1579) | 943(584–1876) | 0.001 | NS |
| CD3+CD4+ cells (%) | 43(30–71) | 48.7(27–63) | 49.6(36–66) | NS | NS |
| CD3+CD8+ cells | 235(135–600) | 352(102–149) | 406(263–775) | NS | NS |
| CD3+CD8+ cells (%) | 23(11–44) | 23(11–47) | 22(9–33) | NS | NS |
| CD4+/CD8+ | 1.6(0.7–4.8) | 1.9(0.7–4.3) | 2.3(1–7) | NS | NS |
| CD28null cells | 206.8(61–500) | 162.5(12.6–1209) | 155(26–430) | NS | NS |
| CD28null (%) | 21.3(4.4–34) | 14.6(1–50) | 7.2(1–17) | 0.005 | 0.02 |
| CD4+CD28null | 34.7(14–279) | 20.9(0–550) | 32(0.9–76) | NS | NS |
| CD4+CD28null (%) | 11.5(1.5–24) | 4.1(0–42.3) | 2.6(0.1–7.8) | 0.006 | 0.02 |
| CD8+CD28null | 132(47–400) | 114(12–735) | 116(25–391) | NS | NS |
| CD8+CD28null (%) | 61.3(24–76) | 43(5.7–85) | 39(7.8–57) | 0.008 | 0.04 |
| Natural killer cells | 141(56–460) | 174.6(0–617) | 258(119–1060) | 0.01 | NS |
| Naural killer cells (%) | 15.3(7.7–31) | 14.6(0–32.5) | 10.9(4.7–40) | NS | NS |
| Treg cells | 33.7(12–102) | 34.7(9.9–130) | 66.3(31–119) | 0.001 | NS |
| Treg cells (%) | 3.1(1.1–6.7) | 2.8(0.62–8.5) | 2.9(1.6–5.7) | NS | NS |
| IRP | 3(1–4) | 3(1–4) | 2(0–4) | 0.006 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampani, E.; Daikidou, D.-V.; Lioulios, G.; Xochelli, A.; Mitsoglou, Z.; Nikolaidou, V.; Dimitriadis, C.; Fylaktou, A.; Papagianni, A.; Stangou, M. CD28null and Regulatory T Cells Are Substantially Disrupted in Patients with End-Stage Renal Disease Due to Diabetes Mellitus. Int. J. Mol. Sci. 2021, 22, 2975. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22062975
Sampani E, Daikidou D-V, Lioulios G, Xochelli A, Mitsoglou Z, Nikolaidou V, Dimitriadis C, Fylaktou A, Papagianni A, Stangou M. CD28null and Regulatory T Cells Are Substantially Disrupted in Patients with End-Stage Renal Disease Due to Diabetes Mellitus. International Journal of Molecular Sciences. 2021; 22(6):2975. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22062975
Chicago/Turabian StyleSampani, Erasmia, Dimitra-Vasilia Daikidou, George Lioulios, Aliki Xochelli, Zoi Mitsoglou, Vasiliki Nikolaidou, Chrysostomos Dimitriadis, Asimina Fylaktou, Aikaterini Papagianni, and Maria Stangou. 2021. "CD28null and Regulatory T Cells Are Substantially Disrupted in Patients with End-Stage Renal Disease Due to Diabetes Mellitus" International Journal of Molecular Sciences 22, no. 6: 2975. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22062975