
Kidney Disease in Diabetic Patients: From Pathophysiology to Pharmacological Aspects with a Focus on Therapeutic Inertia

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. DKD Epidemiology and Risk Factors
3. Pathophysiology of DKD
4. Management of Diabetes Mellitus in the Transition from DKD to ESRD
5. Pharmacological Management of DKD—New Insights and Old Confirmations
5.1. RAS Blockade
5.2. Antidiabetic Drugs
5.3. Dyslipidemia Management
5.4. Antiplatelet Therapy
6. Critical Issues on DKD Management: Evidence from Real-World Settings
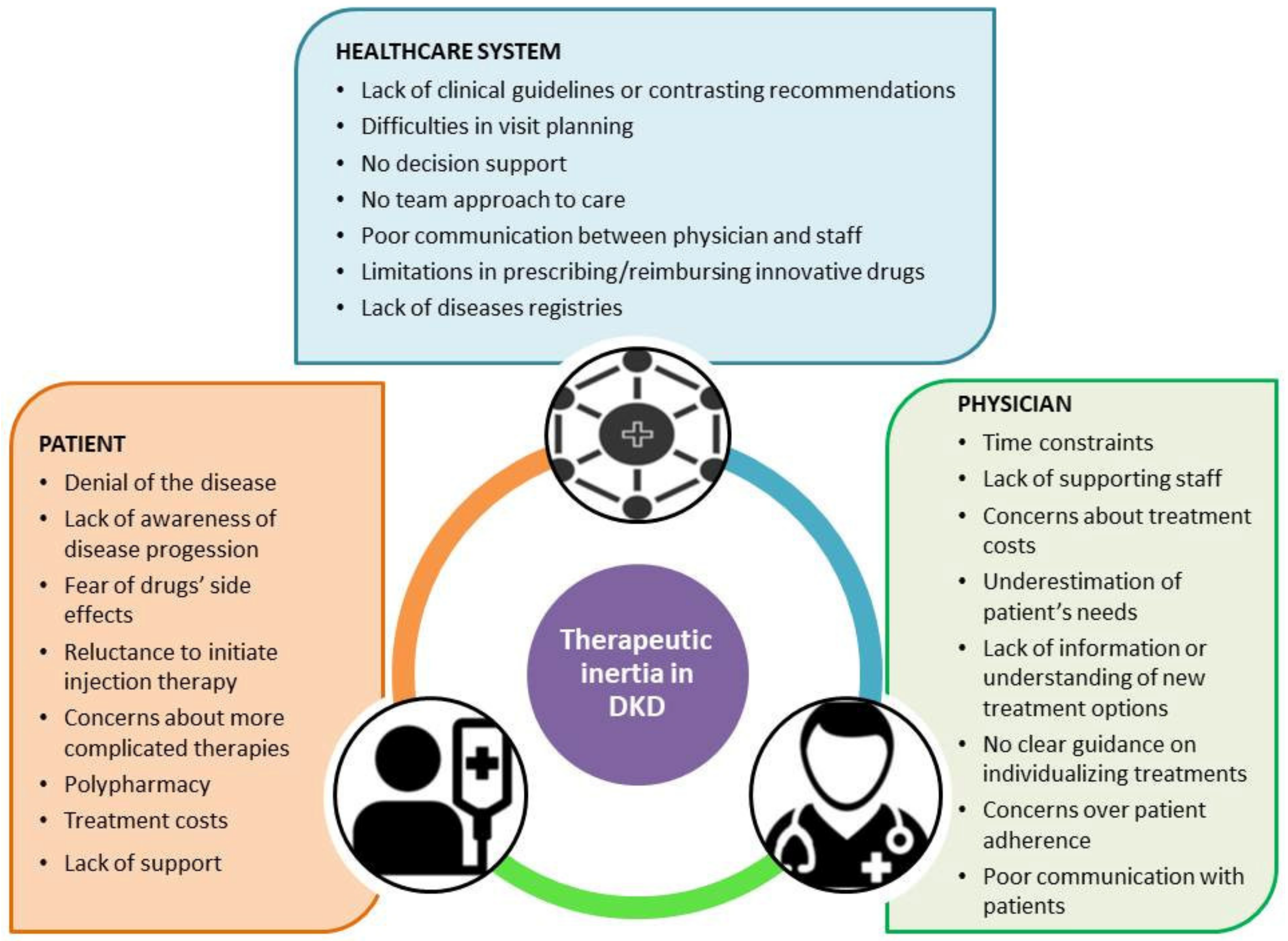
7. Factors Related to Therapeutic Inertia
8. Strategies to Optimize the Management of DKD Patients
9. Future Perspectives for DKD-Related Therapeutical Inertia Management
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DKD | Diabetes kidney disease |
| DM | Diabetes mellitus |
| WHO | World Health Organization |
| GFR | glomerular filtration rate |
| ESRD | end-stage renal disease |
| CV | cardiovascular |
| UACR | urine albumin/creatinine ratio |
| NDA | National Diabetes Audit |
| T1DM | Type 1 diabetes mellitus |
| T2DM | Type 2 diabetes mellitus |
| IAF | Institute for Alternative Futures |
| PKC | protein kinase C |
| NF-κB | nuclear factor kappa-light-chain enhancer of activated B cells |
| IL | interleukin |
| TNF | tumor necrosis factor |
| AGEs | advanced glycation end-products species |
| RAS | renin-angiotensin system |
| ACEi | angiotensin-converting enzyme inhibitors |
| ARB | angiotensin II receptor blockers |
| RR | relative risk |
| CI | confidence interval |
| AKI | acute kidney injury |
| ASCVD | atherosclerotic cardiovascular disease |
| MRA | mineralocorticoid receptor antagonists |
| HR | hazard ratio |
| SGLT2i | Sodium-glucose co-transporter-2 inhibitors |
| GLP-1 RA | glucagon-like peptide-1 receptor agonists |
| DPP-4i | dipeptidyl peptidase-4 inhibitors |
| PPAR | peroxisome proliferator-activated receptors |
| LDL-c | low-density lipoprotein—cholesterol |
| ADRs | adverse drug reactions |
| GPs | general practitioners |
References
- International Diabetes Federation (IDE). Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; Available online: https://www.diabetesatlas.org/en/sections/worldwide-toll-of-diabetes.html (accessed on 1 May 2021).
- World Health Organization. Diabetes-Health Impact. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes#:~:text=The%2520number%2520of%2520people%2520with,%2525%2520in%25202014%2520(1) (accessed on 15 March 2021).
- Gheith, O.; Farouk, N.; Nampoory, N.; Halim, M.A.; Al-Otaibi, T. Diabetic kidney disease: World wide difference of prevalence and risk factors. J. Nephropharmacol. 2016, 5, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Solini, A.; Penno, G.; Bonora, E.; Fondelli, C.; Orsi, E.; Arosio, M.; Trevisan, R.; Vedovato, M.; Cignarelli, M.; Andreozzi, F.; et al. Diverging association of reduced glomerular filtration rate and albuminuria with coronary and noncoronary events in patients with type 2 diabetes: The renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Diabetes Care 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugliese, G.; Solini, A.; Bonora, E.; Fondelli, C.; Orsi, E.; Nicolucci, A.; Penno, G. Chronic kidney disease in type 2 diabetes: Lessons from the Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicentre Study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; D′Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Correction to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2019, 62, 873. [Google Scholar] [CrossRef] [Green Version]
- Trifirò, G.; Parrino, F.; Pizzimenti, V.; Giorgianni, F.; Sultana, J.; Muscianisi, M.; Troncone, C.; Tari, D.U.; Arcoraci, V.; Santoro, D.; et al. The Management of Diabetes Mellitus in Patients with Chronic Kidney Disease: A Population-Based Study in Southern Italy. Clin. Drug Investig. 2016. [Google Scholar] [CrossRef]
- Turner, R. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998. [Google Scholar] [CrossRef]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A.W. 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. N. Engl. J. Med. 2008. [Google Scholar] [CrossRef] [Green Version]
- Ray, K.K.; Seshasai, S.R.K.; Wijesuriya, S.; Sivakumaran, R.; Nethercott, S.; Preiss, D.; Erqou, S.; Sattar, N. Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: A meta-analysis of randomised controlled trials. Lancet 2009. [Google Scholar] [CrossRef]
- Khunti, K.; Millar-Jones, D. Clinical inertia to insulin initiation and intensification in the UK: A focused literature review. Prim. Care Diabetes 2017, 11, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Paul, S.K.; Klein, K.; Thorsted, B.L.; Wolden, M.L.; Khunti, K. Delay in treatment intensification increases the risks of cardiovascular events in patients with type 2 diabetes. Cardiovasc. Diabetol. 2015. [Google Scholar] [CrossRef] [Green Version]
- Khunti, K.; Davies, M.J. Clinical inertia—Time to reappraise the terminology? Prim. Care Diabetes 2017, 11, 105–106. [Google Scholar] [CrossRef]
- Phillips, L.S.; Branch, W.T.; Cook, C.B.; Doyle, J.P.; El-Kebbi, I.M.; Gallina, D.L.; Miller, C.D.; Ziemer, D.C.; Barnes, C.S. Clinical Inertia. Ann. Intern. Med. 2001, 135, 825. [Google Scholar] [CrossRef]
- Strain, W.D.; Blüher, M.; Paldánius, P. Clinical Inertia in Individualising Care for Diabetes: Is There Time to do More in Type 2 Diabetes? Diabetes Ther. 2014, 5, 347–354. [Google Scholar]
- Levey, A.S.; Eckardt, K.U.; Dorman, N.M.; Christiansen, S.L.; Hoorn, E.J.; Ingelfinger, J.R.; Inker, L.A.; Levin, A.; Mehrotra, R.; Palevsky, P.M.; et al. Nomenclature for kidney function and disease: Report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2020, 97, 1117–1129. [Google Scholar] [CrossRef]
- Papadopoulou-Marketou, N.; Kanaka-Gantenbein, C.; Marketos, N.; Chrousos, G.P.; Papassotiriou, I. Biomarkers of diabetic nephropathy: A 2017 update. Crit. Rev. Clin. Lab. Sci. 2017. [Google Scholar] [CrossRef]
- Min, T.Z.; Stephens, M.W.; Kumar, P.; Chudleigh, R.A. Renal complications of diabetes. Br. Med. Bull. 2012. [Google Scholar] [CrossRef]
- Delanaye, P.; Glassock, R.J.; De Broe, M.E. Epidemiology of chronic kidney disease: Think (at least) twice! Clin. Kidney J. 2017. [Google Scholar] [CrossRef] [Green Version]
- Colhoun, H.M.; Marcovecchio, M.L. Biomarkers of diabetic kidney disease. Diabetologia 2018, 61, 996–1011. [Google Scholar] [CrossRef] [Green Version]
- US Renal Data System. USRDS Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Available online: https://render.usrds.org/atlas04.aspx (accessed on 1 May 2021).
- De Boer, I.H. Kidney disease and related findings in the diabetes control and complications trial/ epidemiology of diabetes interventions and complications study. Diabetes Care 2014. [Google Scholar] [CrossRef] [Green Version]
- Cowie, C.C.; Port, F.K.; Wolfe, R.A.; Savage, P.J.; Moll, P.P.; Hawthorne, V.M. Disparities in Incidence of Diabetic End-Stage Renal Disease According to Race and Type of Diabetes. N. Engl. J. Med. 1989. [Google Scholar] [CrossRef]
- Rowley, W.R.; Bezold, C.; Arikan, Y.; Byrne, E.; Krohe, S. Diabetes 2030: Insights from Yesterday, Today, and Future Trends. Popul. Health Manag. 2017. [Google Scholar] [CrossRef] [Green Version]
- Gregg, E.W.; Li, Y.; Wang, J.; Rios Burrows, N.; Ali, M.K.; Rolka, D.; Williams, D.E.; Geiss, L. Changes in Diabetes-Related Complications in the United States, 1990–2010. N. Engl. J. Med. 2014. [Google Scholar] [CrossRef] [Green Version]
- Gembillo, G.; Cernaro, V.; Salvo, A.; Siligato, R.; Laudani, A.; Buemi, M.; Santoro, D. Role of vitamin D status in diabetic patients with renal disease. Medicina 2019, 55, 273. [Google Scholar] [CrossRef] [Green Version]
- Premaratne, E.; Verma, S.; Ekinci, E.I.; Theverkalam, G.; Jerums, G.; MacIsaac, R.J. The impact of hyperfiltration on the diabetic kidney. Diabetes Metab. 2015, 41, 5–17. [Google Scholar] [CrossRef]
- Thomas, B. The Global Burden of Diabetic Kidney Disease: Time Trends and Gender Gaps. Curr. Diab. Rep. 2019, 19, 1–7. [Google Scholar] [CrossRef]
- Carrero, J.J.; Hecking, M.; Chesnaye, N.C.; Jager, K.J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 151. [Google Scholar] [CrossRef]
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Stu. Lancet 2018. [Google Scholar] [CrossRef] [Green Version]
- Frayling, T.M.; Timpson, N.J.; Weedon, M.N.; Zeggini, E.; Freathy, R.M.; Lindgren, C.M.; Perry, J.R.B.; Elliott, K.S.; Lango, H.; Rayner, N.W.; et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 2007. [Google Scholar] [CrossRef] [Green Version]
- Scott, L.J.; Mohlke, K.L.; Bonnycastle, L.L.; Willer, C.J.; Li, Y.; Duren, W.L.; Erdos, M.R.; Stringham, H.M.; Chines, P.S.; Jackson, A.U.; et al. A genome-wide association study of type 2 diabetes in finns detects multiple susceptibility variants. Science 2007. [Google Scholar] [CrossRef] [Green Version]
- Zeggini, E.; Weedon, M.N.; Lindgren, C.M.; Frayling, T.M.; Elliott, K.S.; Lango, H.; Timpson, N.J.; Perry, J.R.B.; Rayner, N.W.; Freathy, R.M.; et al. Replication of genome-wide association signals in UK samples reveals risk loci for type 2 diabetes. Science 2007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köbberling, J. Empirical Risk Figures for First Degree Relatives of Non-Insulin Dependent diabetics. In The Genetics of Diabetes Mellitus; Springer: Berlin/Heidelberg, Germany, 1982; pp. 201–209. [Google Scholar]
- Kato, M.; Natarajan, R. Epigenetics and epigenomics in diabetic kidney disease and metabolic memory. Nat. Rev. Nephrol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, B.; Gulanick, M.; Lamendola, C. Risk factors for type 2 diabetes mellitus. J. Cardiovasc. Nurs. 2002. [Google Scholar] [CrossRef] [PubMed]
- Belkina, A.C.; Denis, G.V. Obesity genes and insulin resistance. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Report on Diabetes. Available online: https://apps.who.int/iris/handle/10665/204871 (accessed on 1 May 2021).
- Donath, M.Y.; Shoelson, S.E. Type 2 diabetes as an inflammatory disease. Nat. Rev. Immunol. 2011, 11, 98–107. [Google Scholar] [CrossRef]
- Porrini, E.; Ruggenenti, P.; Mogensen, C.E.; Barlovic, D.P.; Praga, M.; Cruzado, J.M.; Hojs, R.; Abbate, M.; de Vries, A.P.J. Non-proteinuric pathways in loss of renal function in patients with type 2 diabetes. Lancet Diabetes Endocrinol. 2015, 3, 382–391. [Google Scholar] [CrossRef]
- Luis-Rodríguez, D. Pathophysiological role and therapeutic implications of inflammation in diabetic nephropathy. World J. Diabetes 2012. [Google Scholar] [CrossRef]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic kidney disease: Challenges, progress, and possibilities. Clin. J. Am. Soc. Nephrol. 2017. [Google Scholar] [CrossRef]
- Pieper, G.M.; Riaz-ul-Haq, M. Activation of nuclear factor-κb in cultured endothelial cells by increased glucose concentration: Prevention by calphostin C. J. Cardiovasc. Pharm. 1997. [Google Scholar] [CrossRef]
- Rayego-Mateos, S.; Morgado-Pascual, J.L.; Opazo-Ríos, L.; Guerrero-Hue, M.; García-Caballero, C.; Vázquez-Carballo, C.; Mas, S.; Sanz, A.B.; Herencia, C.; Mezzano, S.; et al. Pathogenic pathways and therapeutic approaches targeting inflammation in diabetic nephropathy. Int. J. Mol. Sci. 2020, 21, 3798. [Google Scholar] [CrossRef]
- Makino, H.; Yamasaki, Y.; Haramoto, T.; Shikata, K.; Hironaka, K.; Ota, Z.; Kanwar, Y.S. Ultrastructural changes of extracellular matrices in diabetic nephropathy revealed by high resolution scanning and immunoelectron microscopy. Lab. Investig. J. Tech. Methods Pathol. 1993, 68, 45–55. [Google Scholar]
- Conti, G.; Caccamo, D.; Siligato, R.; Gembillo, G.; Satta, E.; Pazzano, D.; Carucci, N.; Carella, A.; Del Campo, G.; Salvo, A.; et al. Association of higher advanced oxidation protein products (AOPPs) levels in patients with diabetic and hypertensive nephropathy. Medicina 2019, 55, 675. [Google Scholar] [CrossRef] [Green Version]
- Nowotny, K.; Jung, T.; Höhn, A.; Weber, D.; Grune, T. Advanced glycation end products and oxidative stress in type 2 diabetes mellitus. Biomolecules 2015, 5, 194–222. [Google Scholar] [CrossRef] [Green Version]
- Ighodaro, O.M. Molecular pathways associated with oxidative stress in diabetes mellitus. Biomed. Pharmacother. 2018. [Google Scholar] [CrossRef]
- Schleicher, E.D.; Weigert, C. Role of the hexosamine biosynthetic pathway in diabetic nephropathy. Kidney Int. 2000, 58, S13–S18. [Google Scholar] [CrossRef] [Green Version]
- Chung, S.S.M.; Ho, E.C.M.; Lam, K.S.L.; Chung, S.K. Contribution of polyol pathway to diabetes-induced oxidative stress. J. Am. Soc. Nephrol. 2003. [Google Scholar] [CrossRef] [Green Version]
- Surh, Y.-J.; Chun, K.-S.; Cha, H.-H.; Han, S.S.; Keum, Y.-S.; Park, K.-K.; Lee, S.S. Molecular mechanisms underlying chemopreventive activities of anti-inflammatory phytochemicals: Down-regulation of COX-2 and iNOS through suppression of NF-κB activation. Mutat. Res. 2001, 480, 243–268. [Google Scholar] [CrossRef]
- Suryavanshi, S.V.; Kulkarni, Y.A. NF-κβ: A potential target in the management of vascular complications of diabetes. Front. Pharmacol. 2017, 8, 798. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.C.; Brownlee, M.; Susztak, K.; Sharma, K.; Jandeleit-Dahm, K.A.M.; Zoungas, S.; Rossing, P.; Groop, P.-H.; Cooper, M.E. Diabetic kidney disease. Nat. Rev. Dis. Prim. 2015, 1, 15018. [Google Scholar] [CrossRef]
- Wada, J.; Makino, H. Inflammation and the pathogenesis of diabetic nephropathy. Clin. Sci. 2013. [Google Scholar] [CrossRef] [Green Version]
- Luiza Caramori, M.; Kim, Y.; Huang, C.; Fish, A.J.; Rich, S.S.; Miller, M.E.; Russell, G.; Mauer, M. Cellular basis of diabetic nephropathy: 1. Study design and renal structural-functional relationships in patients with long-standing type 1 diabetes. Diabetes 2002. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Castelao, A.; Gorriz, J.L.; Bover, J.; Segura-de la Morena, J.; Cebollada, J.; Escalada, J.; Esmatjes, E.; Facila, L.; Gamarra, J.; Gracia, S.; et al. Consensus document for the detection and management of chronic kidney disease. Semergen 2014. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Castelao, A.; Soler, M.J.; Górriz Teruel, J.L.; Navarro-González, J.F.; Fernandez-Fernandez, B.; de Alvaro Moreno, F.; Ortiz, A. Optimizing the timing of nephrology referral for patients with diabetic kidney disease. Clin. Kidney J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.; Mohd Noor, F.S.; Draman, C.R.; Seman, M.R.; Ghani, A.S.A. A retrospective review of diabetic nephropathy patients during referral to the sub-urban nephrology clinic. Saudi J. Kidney Dis. Transpl. 2012. [Google Scholar] [CrossRef]
- Black, C.; Sharma, P.; Scotland, G.; McCullough, K.; McGurn, D.; Robertson, L.; Fluck, N.; MacLeod, A.; McNamee, P.; Prescott, G.; et al. Early referral strategies for management of people with markers of renal disease: A systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis. Health Technol. Assess. 2010. [Google Scholar] [CrossRef] [Green Version]
- Shrishrimal, K.; Hart, P.; Michota, F. Managing diabetes in hemodialysis patients: Observations and recommendations. Clevel. Clin. J. Med. 2009. [Google Scholar] [CrossRef]
- Joy, M.S.; Cefalu, W.T.; Hogan, S.L.; Nachman, P.H. Long-term glycemic control measurements in diabetic patients receiving hemodialysis. Am. J. Kidney Dis. 2002. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Lipska, K.J.; Mayo, H.; Bailey, C.J.; McGuire, D.K. Metformin in patientswith type 2 diabetes and kidney disease a systematic review. JAMA 2014. [Google Scholar] [CrossRef] [Green Version]
- Mak, R.H.K.; DeFronzo, R.A. Glucose and insulin metabolism in uremia. Nephron 1992, 61, 377–382. [Google Scholar] [CrossRef]
- Biesenbach, G.; Raml, A.; Schmekal, B.; Eichbauer-Sturm, G. Decreased insulin requirement in relation to GFR in nephropathic Type 1 and insulin-treated Type 2 diabetic patients. Diabet. Med. 2003. [Google Scholar] [CrossRef]
- American Diabetes Association. 11. Microvascular Complications and Foot Care: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S124–S138. [CrossRef] [Green Version]
- Fishbane, S.; Agoritsas, S.; Bellucci, A.; Halinski, C.; Shah, H.H.; Sakhiya, V.; Balsam, L. Augmented Nurse Care Management in CKD Stages 4 to 5: A Randomized Trial. Am. J. Kidney Dis. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlakis, M.; Kher, A. Pre-emptive Kidney Transplantation to Improve Survival in Patients with Type 1 Diabetes and Imminent Risk of ESRD. Semin. Nephrol. 2012. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Mezza, E.; Gino, M.; Grassi, G.; Soragna, G.; Fop, F.; Burdese, M.; Gai, M.; Motta, D.; Malfi, B.; et al. Referral of type 1 diabetic patients to a nephrology unit: Will pre-emptive transplantation change our life? J. Nephrol. 2004, 17, 275–283. [Google Scholar]
- Lewis, E.J.; Hunsicker, L.G.; Bain, R.P.; Rohde, R.D. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N. Engl. J. Med. 1993, 329, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.-H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2001. [Google Scholar] [CrossRef] [Green Version]
- Parving, H.-H.; Lehnert, H.; Bröchner-Mortensen, J.; Gomis, R.; Andersen, S.; Arner, P. The Effect of Irbesartan on the Development of Diabetic Nephropathy in Patients with Type 2 Diabetes. N. Engl. J. Med. 2001. [Google Scholar] [CrossRef]
- Lewis, E.J.; Hunsicker, L.G.; Clarke, W.R.; Berl, T.; Pohl, M.A.; Lewis, J.B.; Ritz, E.; Atkins, R.C.; Rohde, R.; Raz, I. Renoprotective Effect of the Angiotensin-Receptor Antagonist Irbesartan in Patients with Nephropathy Due to Type 2 Diabetes. N. Engl. J. Med. 2001. [Google Scholar] [CrossRef] [Green Version]
- Strippoli, G.F.M.; Bonifati, C.; Craig, M.; Navaneethan, S.D.; Craig, J.C. Angiotensin converting enzyme inhibitors and angiotensin II receptor antagonists for preventing the progression of diabetic kidney disease. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group; de Boer, I.H.; Caramori, M.L.; Chan, J.C.N.; Heerspink, H.J.L.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; et al. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2020. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Chan, J.C.; Cooper, M.E.; Gansevoort, R.T.; Haller, H.; Remuzzi, G.; Rossing, P.; Schmieder, R.E.; Nowack, C.; et al. Effect of finerenone on albuminuria in patients with diabetic nephropathy a randomized clinical trial. JAMA 2015. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ruilope, L.M.; Agarwal, R.; Anker, S.D.; Bakris, G.L.; Filippatos, G.; Nowack, C.; Kolkhof, P.; Joseph, A.; Mentenich, N.; Pitt, B. Design and baseline characteristics of the finerenone in reducing cardiovascular mortality and morbidity in diabetic kidney disease trial. Am. J. Nephrol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Anker, S.D.; Bakris, G.; Filippatos, G.; Pitt, B.; Rossing, P.; Ruilope, L.; Gebel, M.; Kolkhof, P.; Nowack, C.; et al. Investigating new treatment opportunities for patients with chronic kidney disease in type 2 diabetes: The role of finerenone. Nephrol. Dial. Transpl. 2020. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association (ADA). Standards of Medical Care in Diabetes—2018. Available online: https://diabetesed.net/wp-content/uploads/2017/12/2018-ADA-Standards-of-Care.pdf (accessed on 1 May 2021).
- National Kidney Foundation; Nelson, R.G.; Tuttle, K.R.; Bilous, R.W.; Gonzalez-Campoy, J.M.; Mauer, M.; Molitch, M.E.; Sharma, K.; Fradkin, J.E.; Narva, A.S.; et al. KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 Update. Am. J. Kidney Dis. 2012, 60, 850–886. [Google Scholar] [CrossRef]
- Maruthur, N.M.; Tseng, E.; Hutfless, S.; Wilson, L.M.; Suarez-Cuervo, C.; Berger, Z.; Chu, Y.; Iyoha, E.; Segal, J.B.; Bolen, S. Diabetes medications as monotherapy or metformin-based combination therapy for type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 2016, 164, 740–751. [Google Scholar] [CrossRef]
- Crowley, M.J.; Diamantidis, C.J.; McDuffie, J.R.; Cameron, C.B.; Stanifer, J.W.; Mock, C.K.; Wang, X.; Tang, S.; Nagi, A.; Kosinski, A.S.; et al. Clinical outcomes of metformin use in populations with chronic kidney disease, congestive heart failure, or chronic liver disease: A systematic review. Ann. Intern. Med. 2017, 166, 191–200. [Google Scholar] [CrossRef]
- Vasilakou, D.; Karagiannis, T.; Athanasiadou, E.; Mainou, M.; Liakos, A.; Bekiari, E.; Sarigianni, M.; Matthews, D.R.; Tsapas, A. Sodium-glucose cotransporter 2 inhibitors for type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 262–274. [Google Scholar] [CrossRef]
- Zelniker, T.A.; Wiviott, S.D.; Raz, I.; Im, K.; Goodrich, E.L.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Furtado, R.H.M.; et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet 2019. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Rørth, R.; Jhund, P.S.; Docherty, K.F.; Sattar, N.; Preiss, D.; Køber, L.; Petrie, M.C.; McMurray, J.J.V. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019. [Google Scholar] [CrossRef]
- Coppolino, G.; Leporini, C.; Rivoli, L.; Ursini, F.; di Paola, E.D.; Cernaro, V.; Arturi, F.; Bolignano, D.; Russo, E.; De Sarro, G.; et al. Exploring the effects of DPP-4 inhibitors on the kidney from the bench to clinical trials. Pharmacol. Res. 2018, 129, 274–294. [Google Scholar] [CrossRef]
- Yamashita, H.; Nagai, Y.; Takamura, T.; Nohara, E.; Kobayashi, K. Thiazolidinedione derivatives ameliorate albuminuria in streptozotocin-induced diabetic spontaneous hypertensive rat. Metabolism 2002. [Google Scholar] [CrossRef]
- Buckingham, R.E.; Al-Barazanji, K.A.; Toseland, C.D.N.; Slaughter, M.; Connor, S.C.; West, A.; Bond, B.; Turner, N.C.; Clapham, J.C. Peroxisome Proliferator-Activated Receptor- Agonist, Rosiglitazone, Protects Against Nephropathy and Pancreatic Islet Abnormalities in Zucker Fatty Rats. Diabetes 1998, 47, 1326–1334. [Google Scholar] [CrossRef]
- Davidson, M.A.; Mattison, D.R.; Azoulay, L.; Krewski, D. Thiazolidinedione drugs in the treatment of type 2 diabetes mellitus: Past, present and future. Crit. Rev. Toxicol. 2018. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Work Group Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease. Available online: https://kdigo.org/guidelines/lipids-in-ckd/ (accessed on 1 May 2021).
- National Kidney Foundation. How to Classify CKD. Available online: https://www.kidney.org/professionals/explore-your-knowledge/how-to-classify-ckd (accessed on 1 May 2021).
- Joint British Societies′ JBS3 Board; Deanfield, J.; Sattar, N.; Simpson, I.; Wood, D.; Bradbury, K.; Fox, K.; Boon, N.; Winocour, P.; Feher, M.; et al. Consensus recommendations for the prevention of cardiovascular disease (JBS3). Heart 2014, 100, ii1–ii67. [Google Scholar] [CrossRef]
- Stanton, R.C. Clinical challenges in diagnosis and management of diabetic kidney disease. Am. J. Kidney Dis. 2014. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.E.; Garg, R. Glycemic management in ESRD and earlier stages of CKD. Am. J. Kidney Dis. 2014. [Google Scholar] [CrossRef] [Green Version]
- Gerich, J.E.; Woerle, H.J.; Meyer, C.; Stumvoll, M. Renal gluconeogenesis: Its importance in human glucose homeostasis. Diabetes Care 2001. [Google Scholar] [CrossRef] [Green Version]
- Meyers, J.L.; Candrilli, S.D.; Kovacs, B. Type 2 diabetes mellitus and renal impairment in a large outpatient electronic medical records database: Rates of diagnosis and antihyperglycemic medication dose adjustment. Postgrad. Med. 2011. [Google Scholar] [CrossRef]
- Penfornis, A.; Blicklé, J.F.; Fiquet, B.; Quéré, S.; Dejager, S. How are patients with type 2 diabetes and renal disease monitored and managed? Insights from the observational OREDIA study. Vasc. Health Risk Manag. 2014. [Google Scholar] [CrossRef] [Green Version]
- Min, T.; Davies, G.I.; Rice, S.; Chess, J.; Stephens, J.W. Treatment choices for the glycaemic management of patients with type 2 diabetes and chronic kidney disease: Analysis of the SAIL patient linked dataset. Diabetes Metab. Syndr. Clin. Res. Rev. 2018. [Google Scholar] [CrossRef]
- Muller, C.; Dimitrov, Y.; Imhoff, O.; Richter, S.; Ott, J.; Krummel, T.; Bazin-Kara, D.; Chantrel, F.; Hannedouche, T. Oral antidiabetics use among diabetic type 2 patients with chronic kidney disease. Do nephrologists take account of recommendations? J. Diabetes Complicat. 2016. [Google Scholar] [CrossRef]
- Ingrasciotta, Y.; Bertuccio, M.P.; Crisafulli, S.; Ientile, V.; Muscianisi, M.; L′abbate, L.; Pastorello, M.; Provenzano, V.; Scorsone, A.; Scondotto, S.; et al. Real world use of antidiabetic drugs in the years 2011–2017: A population-based study from Southern Italy. Int. J. Environ. Res. Public Health 2020, 17, 9514. [Google Scholar] [CrossRef]
- De Cosmo, S.; Viazzi, F.; Pacilli, A.; Giorda, C.; Ceriello, A.; Gentile, S.; Russo, G.; Rossi, M.C.; Nicolucci, A.; Guida, P.; et al. Achievement of therapeutic targets in patients with diabetes and chronic kidney disease: Insights from the Associazione Medici Diabetologi Annals initiative. Nephrol. Dial. Transpl. 2015. [Google Scholar] [CrossRef]
- Xie, X.; Atkins, E.; Lv, J.; Bennett, A.; Neal, B.; Ninomiya, T.; Woodward, M.; MacMahon, S.; Turnbull, F.; Hillis, G.S.; et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: Updated systematic review and meta-analysis. Lancet 2016. [Google Scholar] [CrossRef] [Green Version]
- De Cosmo, S.; Viazzi, F.; Piscitelli, P.; Giorda, C.; Ceriello, A.; Genovese, S.; Russo, G.; Guida, P.; Fioretto, P.; Pontremoli, R. Blood pressure status and the incidence of diabetic kidney disease in patients with hypertension and type 2 diabetes. J. Hypertens. 2016. [Google Scholar] [CrossRef]
- Braga, M.F.B.; Casanova, A.; Teoh, H.; Gerstein, H.C.; Fitchett, D.H.; Honos, G.; McFarlane, P.A.; Ur, E.; Yale, J.F.; Langer, A.; et al. Poor achievement of guidelines-recommended targets in type 2 diabetes: Findings from a contemporary prospective cohort study. Int. J. Clin. Pract. 2012. [Google Scholar] [CrossRef]
- Ali, M.K.; Bullard, K.M.; Saaddine, J.B.; Cowie, C.C.; Imperatore, G.; Gregg, E.W. Achievement of Goals in U.S. Diabetes Care, 1999–2010. N. Engl. J. Med. 2013. [Google Scholar] [CrossRef] [Green Version]
- Bayram, F.; Sonmez, A.; Haymana, C.; Sabuncu, T.; Dizdar, O.S.; Gurkan, E.; Carlioglu, A.K.; Agbaht, K.; Ozdemir, D.; Demirci, I.; et al. Utilization of statins and LDL-cholesterol target attainment in Turkish patients with type 2 diabetes—A nationwide cross-sectional study (TEMD dyslipidemia study). Lipids Health Dis. 2020. [Google Scholar] [CrossRef]
- José Gagliardino, J.; Arechavaleta, R.; Goldberg Eliaschewitz, F.; Iglay, K.; Brodovicz, K.; Gonzalez, C.D.; Yu, S.; Ravi Shankar, R.; Heisel, O.; Keown, P.; et al. Dyslipidemia: The untreated metabolic dysfunction in people with type 2 diabetes in Latin America. ARETAEUS study outcomes. J. Clin. Transl. Endocrinol. 2019. [Google Scholar] [CrossRef]
- Nicolucci, A. Therapeutic Inertia: How Can We Measure it? The AMD Annals Experience. Available online: https://www.jamd.it/wp-content/uploads/2020/04/2020_01_14_bis.pdf (accessed on 1 May 2021).
- Fu, H.; Liu, S.; Bastacky, S.I.; Wang, X.; Tian, X.J.; Zhou, D. Diabetic kidney diseases revisited: A new perspective for a new era. Mol. Metab. 2019, 30, 250–263. [Google Scholar] [CrossRef]
- Schetz, M.; Dasta, J.; Goldstein, S.; Golper, T. Drug-induced acute kidney injury. Curr. Opin. Crit. Care 2005. [Google Scholar] [CrossRef] [PubMed]
- Wong, N.A. An analysis of discharge drug prescribing amongst elderly patients with renal impairment. Postgrad. Med. J. 1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, F.; O′Hare, A.M.; Miao, Y.; Steinman, M.A. Use of renally inappropriate medications in older veterans: A national study. J. Am. Geriatr. Soc. 2015, 63, 2290–2297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingrasciotta, Y.; Sultana, J.; Giorgianni, F.; Caputi, A.P.; Arcoraci, V.; Tari, D.U.; Linguiti, C.; Perrotta, M.; Nucita, A.; Pellegrini, F.; et al. The burden of nephrotoxic drug prescriptions in patients with chronic kidney disease: A Retrospective population-based study in Southern Italy. PLoS ONE 2014. [Google Scholar] [CrossRef] [Green Version]
- Roux-Marson, C.; Baranski, J.B.; Fafin, C.; Exterman, G.; Vigneau, C.; Couchoud, C.; Moranne, O.; P.S.P.A. Investigators. Medication burden and inappropriate prescription risk among elderly with advanced chronic kidney disease. BMC Geriatr. 2020. [Google Scholar] [CrossRef] [Green Version]
- Del Prato, S.; Penno, G.; Miccoli, R. Changing the treatment paradigm for type 2 diabetes. Diabetes Care 2009, 32 (Suppl. S2), S217–S222. [Google Scholar] [CrossRef] [Green Version]
- Kurlander, J.E.; Kerr, E.A.; Krein, S.; Heisler, M.; Piette, J.D. Cost-related nonadherence to medications among patients with diabetes and chronic pain: Factors beyond finances. Diabetes Care 2009. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association (ADA). 12. Older Adults: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S139–S147. [CrossRef] [Green Version]
- Hua, X.; Carvalho, N.; Tew, M.; Huang, E.S.; Herman, W.H.; Clarke, P. Expenditures and prices of antihyperglycemic medications in the United States: 2002–2013. JAMA 2016. [Google Scholar] [CrossRef] [Green Version]
- Peyrot, M.; Rubin, R.R.; Lauritzen, T.; Skovlund, S.E.; Snoek, F.J.; Matthews, D.R.; Landgraf, R.; Kleinebreil, L. Resistance to insulin therapy among patients and providers: Results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care 2005. [Google Scholar] [CrossRef] [Green Version]
- Kunt, T.; Snoek, F.J. Barriers to insulin initiation and intensification and how to overcome them. Int. J. Clin. Pract. 2009. [Google Scholar] [CrossRef]
- Nakar, S.; Yitzhaki, G.; Rosenberg, R.; Vinker, S. Transition to insulin in Type 2 diabetes: Family physicians′ misconception of patients’ fears contributes to existing barriers. J. Diabetes Complicat. 2007. [Google Scholar] [CrossRef]
- Riddle, M.C.; Gerstein, H.C.; Holman, R.R.; Inzucchi, S.E.; Zinman, B.; Zoungas, S.; Cefalu, W.T. A1C targets should be personalized to maximize benefits while limiting risks. Diabetes Care 2018. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, E.; Weeda, E.R.; Sobieraj, D.M.; Bookhart, B.K.; Piech, C.T.; Coleman, C.I. Impact of non-medical switching on clinical and economic outcomes, resource utilization and medication-taking behavior: A systematic literature review. Curr. Med. Res. Opin. 2016. [Google Scholar] [CrossRef]
- Blonde, L.; Burudpakdee, C.; Divino, V.; Bookhart, B.; Cai, J.; Pfeifer, M.; Coleman, C.I. The impact of non-medical switch on type 2 diabetes patients treated with canagliflozin in the commercially insured US population. Curr. Med. Res. Opin. 2018. [Google Scholar] [CrossRef]
- Ross, S.A. Breaking down patient and physician barriers to optimize glycemic control in type 2 diabetes. Am. J. Med. 2013. [Google Scholar] [CrossRef]
- Brunton, S. Therapeutic Inertia is a Problem for All of Us. Clin. Diabetes 2019. [Google Scholar] [CrossRef]
- Guignard, B.; Bonnabry, P.; Perrier, A.; Dayer, P.; Desmeules, J.; Samer, C.F. Drug-related problems identification in general internal medicine: The impact and role of the clinical pharmacist and pharmacologist. Eur. J. Intern. Med. 2015. [Google Scholar] [CrossRef]
- Peters, K.R. Continuing educational inertia? Clin. Diabetes 2014. [Google Scholar] [CrossRef] [Green Version]
- Khunti, K.; Gomes, M.B.; Pocock, S.; Shestakova, M.V.; Pintat, S.; Fenici, P.; Hammar, N.; Medina, J. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: A systematic review. Diabetes Obes. Metab. 2018. [Google Scholar] [CrossRef] [Green Version]
- Wrzal, P.K.; Bunko, A.; Myageri, V.; Kukaswadia, A.; Neish, C.S.; Ivers, N.M. Strategies to Overcome Therapeutic Inertia in Type 2 Diabetes Mellitus: A Scoping Review. Can. J. Diabetes 2021, 45, 273.e13–281.e13. [Google Scholar] [CrossRef] [PubMed]
- Reach, G.; Pechtner, V.; Gentilella, R.; Corcos, A.; Ceriello, A. Clinical inertia and its impact on treatment intensification in people with type 2 diabetes mellitus. Diabetes Metab. 2017, 43, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Gabbay, R.A.; Kendall, D.; Beebe, C.; Cuddeback, J.; Hobbs, T.; Khan, N.D.; Leal, S.; Miller, E.; Novak, L.M.; Rajpathak, S.N.; et al. Addressing Therapeutic Inertia in 2020 and Beyond: A 3-Year Initiative of the American Diabetes Association. Clin. Diabetes 2020, 38, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.M.; Lai, T.S.; Chen, P.Y.; Lai, C.F.; Yang, S.Y.; Wu, V.; Chiang, C.K.; Kao, T.W.; Huang, J.W.; Chiang, W.C.; et al. Multidisciplinary care program for advanced chronic kidney disease: Reduces renal replacement and medical costs. Am. J. Med. 2015, 128, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Helou, N.; Talhouedec, D.; Zumstein-Shaha, M.; Zanchi, A. A Multidisciplinary Approach for Improving Quality of Life and Self-Management in Diabetic Kidney Disease: A Crossover Study. J. Clin. Med. 2020, 9, 2160. [Google Scholar] [CrossRef]
- Diamantidis, C.J.; Bosworth, H.B.; Oakes, M.M.; Davenport, C.A.; Pendergast, J.F.; Patel, S.; Moaddeb, J.; Barnhart, H.X.; Merrill, P.D.; Baloch, K.; et al. Simultaneous Risk Factor Control Using Telehealth to slow Progression of Diabetic Kidney Disease (STOP-DKD) study: Protocol and baseline characteristics of a randomized controlled trial. Contemp. Clin. Trials 2018, 69, 28–39. [Google Scholar] [CrossRef]
- Zullig, L.L.; Oakes, M.M.; McCant, F.; Bosworth, H.B. Lessons learned from two randomized controlled trials: CITIES and STOP-DKD. Contemp. Clin. Trials Commun. 2020, 19, 100612. [Google Scholar] [CrossRef]


{kind=link}
| Drug Class | Medications | Recommendation |
|---|---|---|
| Biguanides | Metformin | Contraindicated if GFR <30 mL/min/1.73 m2 Not started in GFR 30–45 mL/min/1.73 m2 |
| SGLT2 inhibitors | Empagliflozin | Avoid use or discontinue if GFR <45 mL/min/1.73 m2 |
| Canagliflozin | Avoid use if GFR <30 mL/min/1.73 m2 Dose adjustment in GFR 30–59 mL/min/1.73 m2 | |
| Dapagliflozin | Contraindicated if GFR <30 mL/min/1.73 m2 Not started in GFR 30–45 mL/min/1.73 m2 | |
| First-generation sulfonylureas | Acetohexamide, tolazamide, tolbutamide, chlorpropamide | Avoid use |
| Second-generation sulfonylureas | Glyburide | Avoid use |
| Glimepiride | Start cautiously in GFR <15 mL/min/1.73 m2 | |
| Glipizide | No dose adjustment | |
| Glicazide | No dose adjustment | |
| Alpha-glucosidase inhibitors | Acarbose | Contraindicated if GFR <30 mL/min/1.73 m2 |
| GPL-1 receptor agonists | Exenatide | Contraindicated if GFR <30 mL/min/1.73 m2 |
| Lixisenatide | Contraindicated if GFR <15 mL/min/1.73 m2 | |
| Liraglutide | No dose adjustment | |
| Albiglutide | No dose adjustment | |
| Dulaglutide | No dose adjustment | |
| Thiazolidinediones | Pioglitazone | No dose adjustment |
| Rosiglitazone | No dose adjustment | |
| Meglitinides | Repaglinide | Start cautiously in GFR <15 mL/min/1.73 m2 |
| DPP-4 inhibitors | Sitagliptin | Lower dosage |
| Vildagliptin | Lower dosage | |
| Saxagliptin | Lower dosage | |
| Alogliptin | Lower dosage | |
| Linagliptin | No dose adjustment | |
| Insulins | Dose adjustment based on patient response | |
| Statins | Normal to Mildly Decreased (GFR: ≥90 to 60–89 mL/min/1.73 m2) | Mildly/Moderate Decreased to Kidney Failure (GFR: 45–59 to <15 mL/min/1.73 m2) |
|---|---|---|
| Lovastatin | No dose adjustment | NA |
| Fluvastatin | No dose adjustment | 80 mg/day |
| Atorvastatin | No dose adjustment | 20 mg/day |
| Rosuvastatin | No dose adjustment | 10 mg/day |
| Simvastatin/Ezetmibe | No dose adjustment | 20 mg/day |
| Pravastatin | No dose adjustment | 40 mg/day |
| Simvastatin | No dose adjustment | 40 mg/day |
| Pitavastatin | No dose adjustment | 2 mg/day |
| Strategies to avoid therapeutic inertia |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gembillo, G.; Ingrasciotta, Y.; Crisafulli, S.; Luxi, N.; Siligato, R.; Santoro, D.; Trifirò, G. Kidney Disease in Diabetic Patients: From Pathophysiology to Pharmacological Aspects with a Focus on Therapeutic Inertia. Int. J. Mol. Sci. 2021, 22, 4824. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094824
Gembillo G, Ingrasciotta Y, Crisafulli S, Luxi N, Siligato R, Santoro D, Trifirò G. Kidney Disease in Diabetic Patients: From Pathophysiology to Pharmacological Aspects with a Focus on Therapeutic Inertia. International Journal of Molecular Sciences. 2021; 22(9):4824. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094824
Chicago/Turabian StyleGembillo, Guido, Ylenia Ingrasciotta, Salvatore Crisafulli, Nicoletta Luxi, Rossella Siligato, Domenico Santoro, and Gianluca Trifirò. 2021. "Kidney Disease in Diabetic Patients: From Pathophysiology to Pharmacological Aspects with a Focus on Therapeutic Inertia" International Journal of Molecular Sciences 22, no. 9: 4824. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22094824