Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in Newborn Screening System Quality Improvement

 ,
,
Abstract
:1. Introduction
2. Methodology
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CDC | Centers for Disease Control and Prevention (U.S.) |
| CH | Congenital hypothyroidism |
| CHD | Center for Health Development (regional health office) |
| DILG | Department of the Interior and Local Government |
| DOH | Department of Health (national health agency, Philippines) |
| ENBS | Expanded newborn screening |
| G6PD | Glucose-6-phosphate dehydrogenase |
| GAL | Galactosemia |
| LGU | Local Government Unit |
| MSUD | Maple syrup urine disease |
| NBS | Newborn bloodspot screening |
| NBSCC | Newborn screening continuity clinic (long-term follow-up) |
| NCNBSS | National Comprehensive Newborn Screening System |
| NIH | National Institutes of Health (Philippines) |
| NNSGRC | National Newborn Screening and Global Resource Center (U.S.) |
| NSC | Newborn Screening Center (screening laboratory) |
| NSF | Newborn Screening Facility (screening specimen collection site) |
| NSRC | Newborn Screening Reference Center (Philippines) |
| PEAS | Performance Evaluation and Assessment Scheme (U.S version) |
| PhilHealth | Philippine Health Insurance Corporation (national health insurance) |
| PIR | Program implementation review |
| PKU | Phenylketonuria |
| PPEAS | Philippine Performance Evaluation and Assessment Scheme |
| TPMF | Taiwan Preventive Medicine Foundation |
References
- Guthrie, R.; Susi, A. A simple phenylalanine method for detecting phenylketonuria in large populations of newborn infants. Pediatrics 1963, 32, 338–342. [Google Scholar] [PubMed]
- Levy, H.L. Historical perspective: Newborn metabolic screening. Neo Rev. 2005, 6, e57–e60. Available online: http://neoreviews.aappublications.org/cgi/content/full/neoreviews (accessed on 6 September 2020). [CrossRef]
- Therrell, B.L.; Padilla, C.D.; Loeber, J.G.; Khneisser, I.; Saadallah, A.; Borrajo, G.J.C.; Adams, J. Current status of newborn screening worldwide. Semin. Perinatol. 2015, 39, 171–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padilla, C.; Domingo, C.F. Implementation of newborn screening in the Philippines. Phil. J. Pediatr. 2002, 51, 2–10. [Google Scholar]
- Padilla, C. Newborn screening in the Philippines. Southeast Asia J. Trop. Med. Public Health 2003, 34 (Suppl. 3), 87–88. [Google Scholar]
- Padilla, C.D.; Therrell, B.L. Newborn screening in the Asia Pacific region. J. Inherit. Metab. Dis. 2007, 30, 490–506. [Google Scholar] [CrossRef] [PubMed]
- David-Padilla, C.; Basilio, J.A.; Oliveros, Y.E. Newborn Screening: Research to Policy. Acta Med. Philipp. 2009, 43, 6–14. [Google Scholar]
- PhilHealth Circular No. 34, s-2006. PhilHealth Newborn Care Package. Available online: https://www.philhealth.gov.ph/circulars/2006/circ34_2006.pdf (accessed on 10 September 2020).
- Department of Health Memorandum No. 2012-0154. Inclusion of MSUD in the Newborn Screening Panel of Disorders. Newborn Screening Reference Center. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/doh-2012-0154.pdf (accessed on 12 September 2020).
- Administrative Order 2014-0045. Guidelines on the Implementation of the Newborn Screening Program. Available online: https://dmas.doh.gov.ph:8083/Rest/GetFile?id=337007 (accessed on 14 September 2020).
- Expanded Newborn Screening Panel. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/enbs-panel.pdf (accessed on 23 November 2020).
- PhilHealth Circular No. 2018-0021. Enhancement of PhilHealth Newborn Care Package. Available online: https://www.philhealth.gov.ph/circulars/2018/circ2018-0021.pdf (accessed on 12 September 2020).
- Therrell, B.L. US newborn screening policy dilemmas for the twenty-first century. Mol. Genet. Metab. 2001, 74, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Therrell, B.L.; Schwartz, M.; Southard, C.; Williams, D.; Hannon, H.; Mann, M.Y.; PEAS Organizing and Working Groups. Newborn Screening System Performance Evaluation Assessment Scheme (PEAS). Semin. Perinatol. 2010, 34, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Congress of the Philippines. Republic Act No. 9288 or Newborn Screening Act of 2004. Acta Med. Philipp. 2009, 43, 64–66. [Google Scholar]
- Administrative Order No. 2014-00035. Implementing Guidelines on the Setting-Up of Newborn Screening Continuity Clinics. Available online: https://dmas.doh.gov.ph:8083/Rest/GetFile?id=336996 (accessed on 10 September 2020).
- Rules and Regulations Implementing Republic Act No. 9288. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/IRR.pdf (accessed on 9 October 2020).
- Newborn Screening Reference Center. Manual of Operations for Newborn Screening Continuity Clinics. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/nbsccmanops.pdf (accessed on 9 October 2020).
- Department of Health—Department Order No. 29-Cs.2001. Creation of a National Technical Working Group on Newborn Screening Program under the National Center for Disease Prevention and Control. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/do29-c-2001.pdf (accessed on 9 October 2020).
- Department of Health—Department Personnel Order No. 2014-1438. Merging of the National Technical Working Group on Newborn Screening and the National Technical Working Group on the Expanded Newborn Screening Program under Family Health Office. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/dpo2014-1438.pdf (accessed on 9 October 2020).
- Department of Health—Department Personnel Order No. 2014-1438-A. Amendment to Department Personnel Order No. 2014-1438. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/dpo2014-1438-a.pdf (accessed on 9 October 2020).
- David-Padilla, C.; Basilio, J.A.; Therrell, B.L. A Performance Evaluation and Assessment Scheme (PEAS) for improving the Philippine newborn screening program. Acta Med. Philipp. 2009, 43, 58–63. [Google Scholar]
- PPEAS for the Centers for Health and Development (CHDs) Complete Checklist. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/roppeas.pdf (accessed on 12 October 2020).
- PPEAS for Newborn Screening Centers (NSCs) Complete Checklist. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/nscppeas.pdf (accessed on 12 October 2020).
- PPEAS for Newborn Screening Facilities (NSFs) Complete Checklist. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/nsfppeas.pdf (accessed on 12 October 2020).
- PPEAS for Newborn Screening Continuity Clinics (NBSCCs) Complete Checklist. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/nbsccppeas.pdf (accessed on 12 October 2020).

- 1
- 2
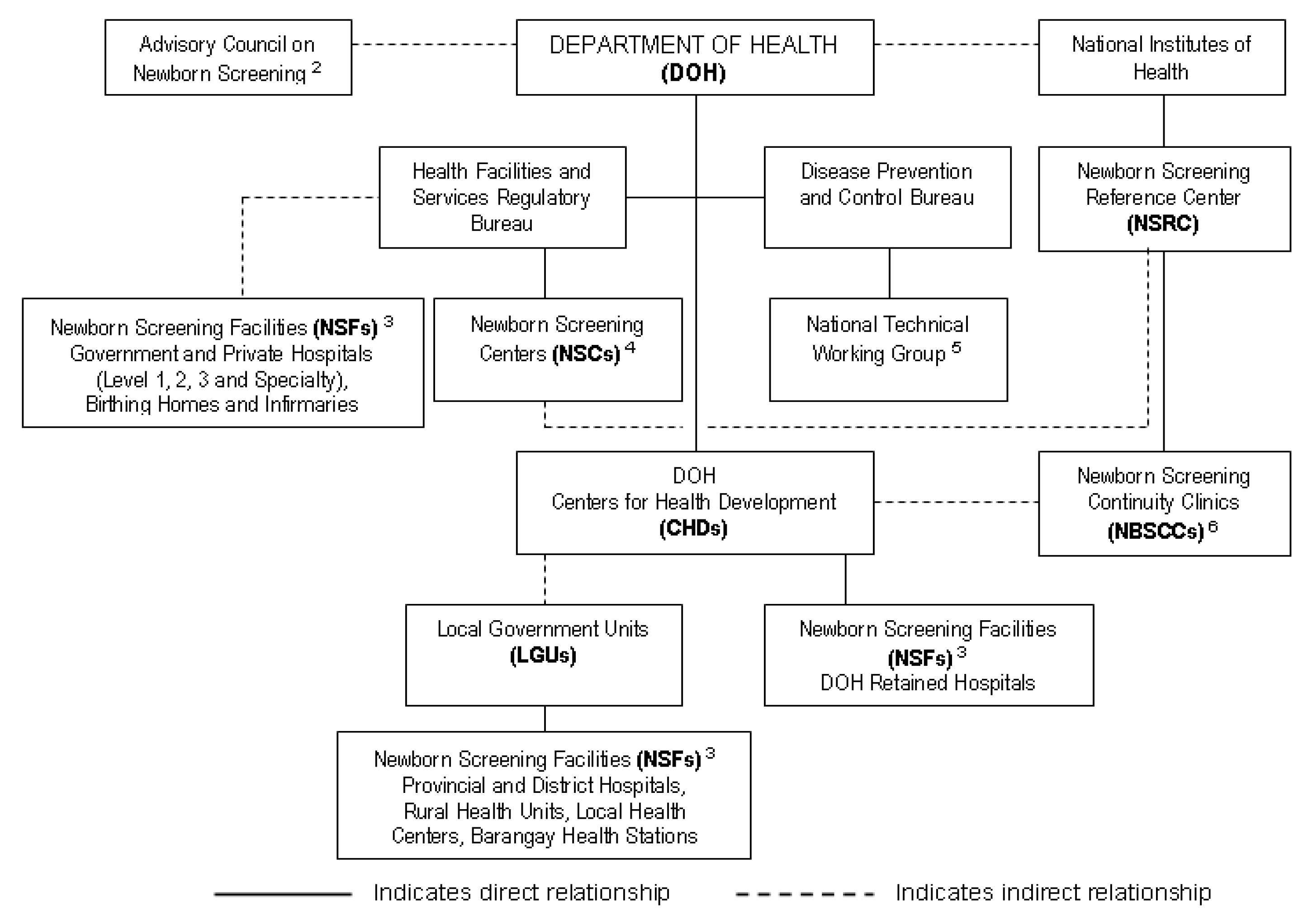
- According to the Newborn Screening Law, the Advisory Committee on Newborn Screening was, “… created and made an integral part of the Office of the Secretary of the Department of Health (national health agency, Philippines) (DOH) to ensure sustained inter-agency collaboration. The committee reviews annually and recommends conditions to be included in the newborn screening panel of disorders; reviews and recommends the newborn screening fee to be charged by Newborn Screening Centers; reviews the report of the Newborn Screening Reference Center on the quality assurance of the Newborn Screening Centers and recommends corrective measures as deemed necessary. The Committee shall be composed of eight (8), including the Secretary of Health, who shall act as the chairperson. The other members of the of the Committee shall be as follows: (1) the Executive Director of the National Institutes of Health (NIH) who shall act as a Vice Chairperson, (ii), an Undersecretary of the DILG (Department of the Interior and Local Government); (iii) the Executive Director of the Council for the Welfare of Children; (iv) the Director of the Newborn Screening Reference Center; (v) three (3) representatives appointed by the Secretary of Health who shall be a pediatrician, obstetrician, endocrinologist, family physician, nurse or midwife from either a public or private sector. The three (3) representatives shall be appointed for a term of three (3) years, subject to their being reappointed for additional three (3) year periods for each extension” [15].
- 3
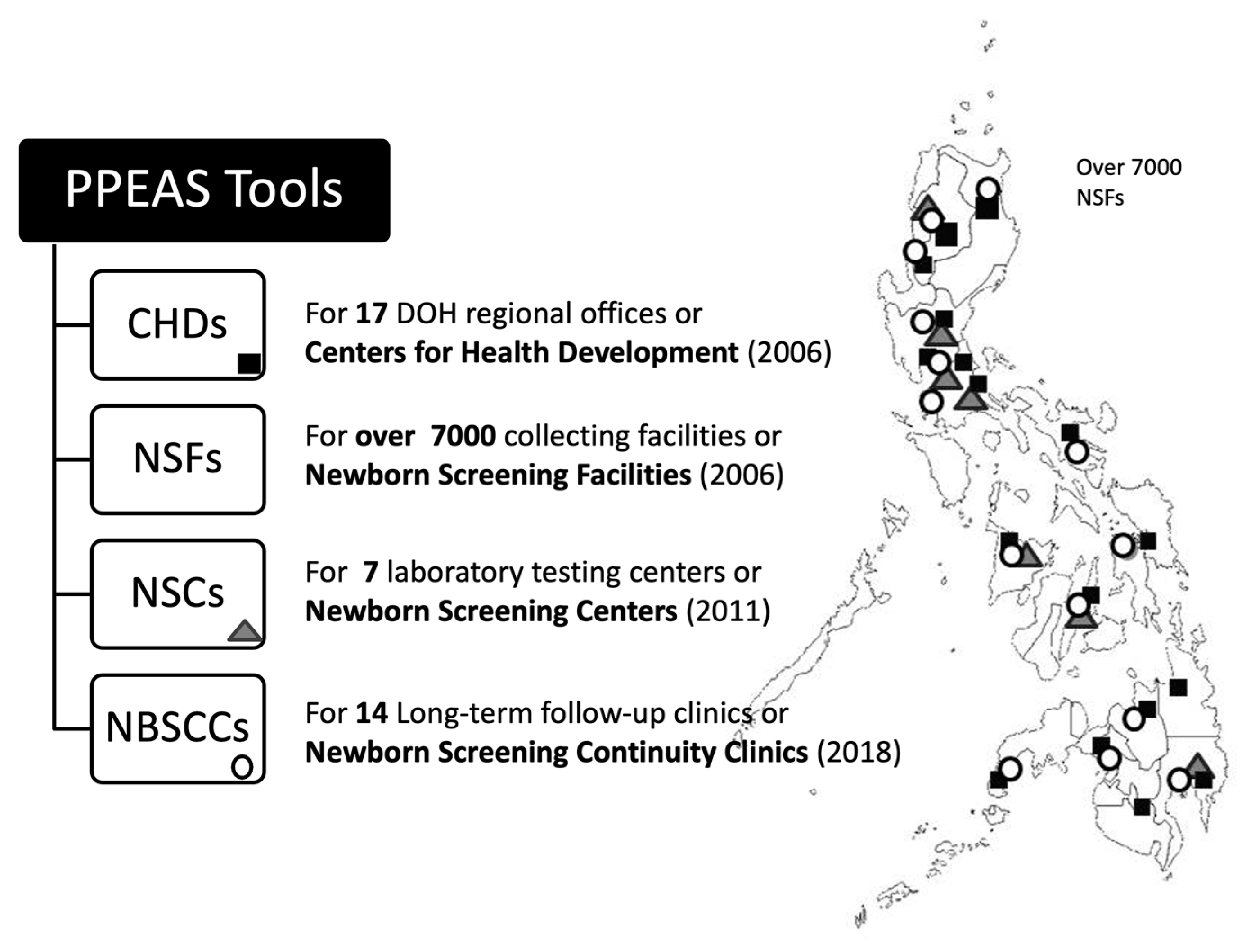
- A Newborn Screening Facility (NSF) is a health facility that educates parents about NBS during prenatal visits, collects blood specimens for NBS, sends specimens to the Newborn Screening Center (NSC), and recalls patients found positive for NBS and assists in managing patients.
- 4
- A Newborn Screening Center (NSC) is a facility equipped with a NBS laboratory that complies with standards established by NIH and DOH and provides required laboratory tests and recall/follow-up for newborns with conditions identified by NBS [17].
- 5
- The National Technical Working Group on Newborn Screening has the goal of the long- and medium-term target setting and planning of the National Comprehensive NBS System. It ensures that all policies and standards of the program adhere to overall internationally accepted standards and ethical considerations [19,20,21].
- 6
- Newborn Screening Continuity Clinics (long-term follow-up) (NBSCCs) are administratively under the NBS Reference Center (NSRC) with referrals from the NSCs. DOH offices (CHDs) assist the NBSCCs in monitoring patients. NBSCCs are located in government hospitals administratively under the CHDs [18].
- 1
- 2
- According to the Newborn Screening Law, the Advisory Committee on Newborn Screening was, “… created and made an integral part of the Office of the Secretary of the Department of Health (national health agency, Philippines) (DOH) to ensure sustained inter-agency collaboration. The committee reviews annually and recommends conditions to be included in the newborn screening panel of disorders; reviews and recommends the newborn screening fee to be charged by Newborn Screening Centers; reviews the report of the Newborn Screening Reference Center on the quality assurance of the Newborn Screening Centers and recommends corrective measures as deemed necessary. The Committee shall be composed of eight (8), including the Secretary of Health, who shall act as the chairperson. The other members of the of the Committee shall be as follows: (1) the Executive Director of the National Institutes of Health (NIH) who shall act as a Vice Chairperson, (ii), an Undersecretary of the DILG (Department of the Interior and Local Government); (iii) the Executive Director of the Council for the Welfare of Children; (iv) the Director of the Newborn Screening Reference Center; (v) three (3) representatives appointed by the Secretary of Health who shall be a pediatrician, obstetrician, endocrinologist, family physician, nurse or midwife from either a public or private sector. The three (3) representatives shall be appointed for a term of three (3) years, subject to their being reappointed for additional three (3) year periods for each extension” [15].
- 3
- A Newborn Screening Facility (NSF) is a health facility that educates parents about NBS during prenatal visits, collects blood specimens for NBS, sends specimens to the Newborn Screening Center (NSC), and recalls patients found positive for NBS and assists in managing patients.
- 4
- A Newborn Screening Center (NSC) is a facility equipped with a NBS laboratory that complies with standards established by NIH and DOH and provides required laboratory tests and recall/follow-up for newborns with conditions identified by NBS [17].
- 5
- The National Technical Working Group on Newborn Screening has the goal of the long- and medium-term target setting and planning of the National Comprehensive NBS System. It ensures that all policies and standards of the program adhere to overall internationally accepted standards and ethical considerations [19,20,21].
- 6
- Newborn Screening Continuity Clinics (long-term follow-up) (NBSCCs) are administratively under the NBS Reference Center (NSRC) with referrals from the NSCs. DOH offices (CHDs) assist the NBSCCs in monitoring patients. NBSCCs are located in government hospitals administratively under the CHDs [18].



{kind=link}
{kind=link}
{kind=link}
| PPEAS Requirements for CHDs (DOH Regional Offices) | PPEAS Requirements for NSFs (Specimen Collection Facilities) | PPEAS Requirements for NSCs (Laboratory Testing Facilities) | PPEAS Requirements for NSBCCs (Long-Term Follow-up Clinics) |
|---|---|---|---|
| 1. Evidence of a usable and appropriate operational structure 2. Enactment of an appropriate plan of action (including financing) 3. Availability of defined systems to support Newborn Bloodspot Screening (NBS) 4. Utilization of a quality health promotion plan for NBS 5. Creation/use of innovative strategies leading to best practices | 1. Definition and use of an effective NBS team 2. Creation/use of an organized NBS program within the health facility 3. Specific administrative support for NBS implementation/ continuation 4. Ongoing monitoring and evaluation program for NBS 5. Utilization of a failsafe reporting system to patients and a summary reporting system to NBS Reference Center (NSRC) | 1. Adequate and timely service delivery (laboratory and short-term follow-up) 2. A defined education and regulation program 3. Appropriately educated and trained personnel including ongoing education 4. Compliance and proficiency with technical standards 5. Efficient program administration and financing 6. Appropriate and efficient specimen management system 7. Defined useful program linkages 8. Supportive and efficient facility management system | 1. A defined multi-disciplinary operational structure 2. Adequate facility support (housing, finances, etc.) 3. Efficient data management system 4. A defined clinical management and referral network 5. NBS program advocacy activities 6. Long-term follow-up data monitoring and evaluation 7. A supportive and efficient administrative system 8. Creation of innovative strategies leading to best practices |
| Major Issues and Concerns | Recommendations/Agreements |
|---|---|
| Training |
|
| Regional NBS teamwork |
|
| NBS coverage |
|
| Unsatisfactory specimens |
|
| Quality of result transmittal |
|
| Advocacy |
|
| ENBS Awareness |
|
| Confirmatory testing |
|
| Follow-up |
|
| Monitoring |
|
| Others/service delivery |
|
| NBS System Challenges Identified Using PPEAS | Corrective Actions Taken and Impact |
|---|---|
| Variability in level of support across CHDs | Clarified financial policies resulting in greater operational uniformity and expanded support leading to improved program quality → Better specimens and fewer patients lost to follow-up, better turnaround time from collection, send out to the laboratory and recall of patient |
| Low newborn population coverage in general | Initiated goal setting and standardized training for program personnel with incentives (awards) for meeting or exceeding goals → Participating NSFs and number of newborns served increasing (currently over 7000 NSFs and greater than 90% coverage (most with ENBS) |
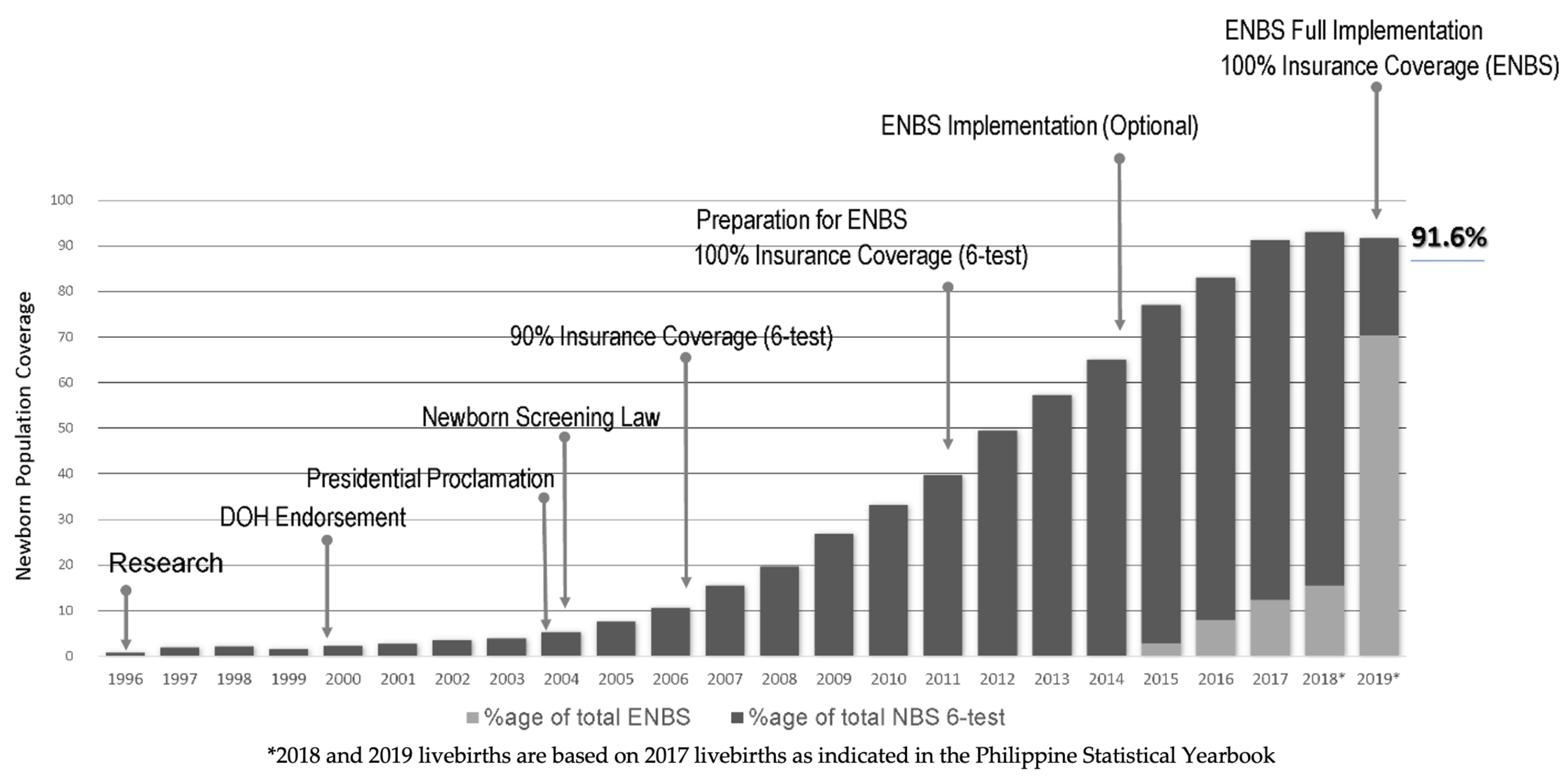
| Low newborn population coverage for expanded ENBS (29 conditions) following its implementation | Identified patient finances identified as inadequate → Able to convince national health insurance to shift coverage from 6-test panel to ENBS 29-test panel (note increase in Figure 1) |
| Inadequate information on which NSFs are active and their location | Developed and created the NSF online database of information on all facilities offering newborn screening |
| NSCs lack of uniformity in laboratory testing protocols | Initiated a laboratory standardization effort for laboratory, follow-up, and quality manuals at all NSCs and required development of training plans for the various NSC positions |
| NSFs lack of uniformity in providing NBS information and services | Created a “Facilitator’s Guidebook” (periodically updated) to aid in standardizing education and service provision among NSFs |
| Poor specimen quality recognized across many NSFs | Implemented reporting templates for standardizing reports of specimen quality from NSCs and an alert system from NSC to CHD for action in poorer performing NSFs |
| Uneven work performance across NSCs | Developed a Standard Competency Tool per position/staff to be used in all NSCs |
| Low recall rate of patients under long-term care | Established Newborn screening continuity clinics (long-term follow-up) NBSCCs in 14 regions in the country resulting in significant improvement in recall rate (from ~30% to >70% recall rate) |
| Improved collaboration with pediatric endocrinologists in the referral and management of endocrine patients, and in securing the anthropometric data of their private patients | |
| Solidified collaboration with the metabolic geneticists for the acute care management of diagnosed metabolic cases | |
| Low treatment compliance among indigent patients | Revised guidelines for the use of CHD fee funds to include other laboratory tests, long-term management, and other support for indigent patients, resulting in marked improvement in adherence to treatment and management among indigent patients seen at NBSCCs |
| Inadequate disease tracking | Created NBSCC Online Registry for long-term patient tracking |
| Variable, unstable, or no contingency plans available in many facilities | Developed advisories, guidelines and protocols in times of emergency operations |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padilla, C.D.; Therrell, B.L.; Panol, K.A.R.; Suarez, R.C.N.; Reyes, M.E.L.; Jomento, C.M.; Maceda, E.B.G.; Lising, J.A.C.; Beltran, F.D.E.; Orbillo, L.L. Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in Newborn Screening System Quality Improvement. Int. J. Neonatal Screen. 2020, 6, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns6040095
Padilla CD, Therrell BL, Panol KAR, Suarez RCN, Reyes MEL, Jomento CM, Maceda EBG, Lising JAC, Beltran FDE, Orbillo LL. Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in Newborn Screening System Quality Improvement. International Journal of Neonatal Screening. 2020; 6(4):95. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns6040095
Chicago/Turabian StylePadilla, Carmencita D., Bradford L. Therrell, Karen Asuncion R. Panol, Riza Concordia N. Suarez, Ma. Elouisa L. Reyes, Charity M. Jomento, Ebner Bon G. Maceda, Jovy Ann C. Lising, Frederick David E. Beltran, and Lita L. Orbillo. 2020. "Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in Newborn Screening System Quality Improvement" International Journal of Neonatal Screening 6, no. 4: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns6040095