
Newborn Screening for X-Linked Adrenoleukodystrophy: Review of Data and Outcomes in Pennsylvania

Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Subjects Research
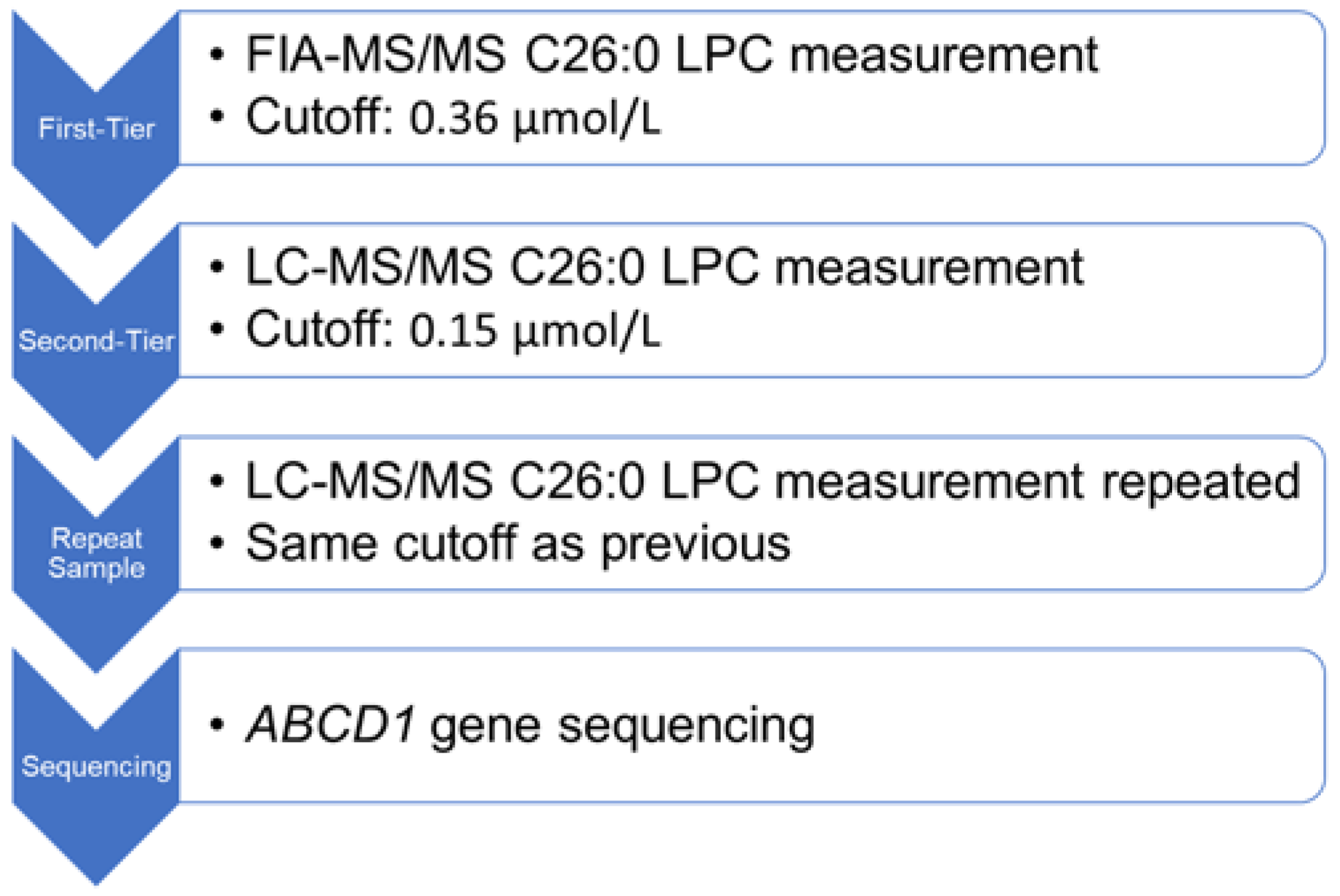
2.2. Pennsylvania X-ALD Newborn Screening Protocol
2.3. X-ALD Newborn Screening Follow-Up Care
3. Results
3.1. Pennsylvania X-ALD Newborn Screening Outcomes
3.2. Clinical Assessment and Outcomes
3.3. Population Genetics and Test Performance
3.4. Comparison of X-ALD NBS between States
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bezman, L.; Moser, A.B.; Raymond, G.V.; Rinaldo, P.; Watkins, P.A.; Smith, K.D.; Kass, N.E.; Moser, H.W. Adrenoleukodystrophy: Incidence, New Mutation Rate, and Results of Extended Family Screening. Ann. Neurol. 2001, 49, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Moser, A.B.; Jones, R.O.; Hubbard, W.C.; Tortorelli, S.; Orsini, J.J.; Caggana, M.; Vogel, B.H.; Raymond, G.V. Newborn Screening for X-Linked Adrenoleukodystrophy. Int. J. Neonatal Screen. 2016, 2, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosser, J.; Douar, A.M.; Sarde, C.O.; Kioschis, P.; Feil, R.; Moser, H.; Poustka, A.M.; Mandel, J.L.; Aubourg, P. Putative X-Linked Adrenoleukodystrophy Gene Shares Unexpected Homology with ABC Transporters. Nature 1993, 361, 726–730. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S.; Pujol, A.; Waterham, H.R.; van Geel, B.M.; Boehm, C.D.; Raymond, G.V.; Cutting, G.R.; Wanders, R.J.; Moser, H.W. ABCD1 Mutations and the X-Linked Adrenoleukodystrophy Mutation Database: Role in Diagnosis and Clinical Correlations. Hum. Mutat. 2001, 18, 499–515. [Google Scholar] [CrossRef]
- Moser, H.W.; Moser, A.B.; Powers, J.M.; Nitowsky, H.M.; Schaumburg, H.H.; Norum, R.A.; Migeon, B.R. The Prenatal Diagnosis of Adrenoleukodystrophy. Demonstration of Increased Hexacosanoic Acid Levels in Cultured Amniocytes and Fetal Adrenal Gland. Pediatr. Res. 1982, 16, 172–175. [Google Scholar] [CrossRef] [Green Version]
- Powers, J.M.; Moser, H.W.; Moser, A.B.; Schaumburg, H.H. Fetal Adrenoleukodystrophy: The Significance of Pathologic Lesions in Adrenal Gland and Testis. Hum. Pathol. 1982, 13, 1013–1019. [Google Scholar] [CrossRef]
- Igarashi, M.; Schaumburg, H.H.; Powers, J.; Kishmoto, Y.; Kolodny, E.; Suzuki, K. Fatty Acid Abnormality in Adrenoleukodystrophy. J. Neurochem. 1976, 26, 851–860. [Google Scholar] [CrossRef]
- Singh, I.; Pujol, A. Pathomechanisms Underlying X-Adrenoleukodystrophy: A Three-Hit Hypothesis. Brain Pathol. 2010, 20, 838–844. [Google Scholar] [CrossRef]
- Engelen, M.; Kemp, S.; de Visser, M.; van Geel, B.M.; Wanders, R.J.; Aubourg, P.; Poll-The, B.T. X-Linked Adrenoleukodystrophy (X-ALD): Clinical Presentation and Guidelines for Diagnosis, Follow-up and Management. Orphanet J. Rare Dis. 2012, 7, 51. [Google Scholar] [CrossRef]
- Turk, B.R.; Theda, C.; Fatemi, A.; Moser, A.B. X-linked Adrenoleukodystrophy: Pathology, Pathophysiology, Diagnostic Testing, Newborn Screening and Therapies. Int. J. Dev. Neurosci. 2020, 80, 52–72. [Google Scholar] [CrossRef] [Green Version]
- Raymond, G.V.; Moser, A.B.; Fatemi, A. X-Linked Adrenoleukodystrophy. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J., Mirzaa, G., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- van Geel, B.M.; Assies, J.; Wanders, R.J.; Barth, P.G. X Linked Adrenoleukodystrophy: Clinical Presentation, Diagnosis, and Therapy. J. Neurol. Neurosurg. Psychiatry 1997, 63, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Van Geel, B.M.; Assies, J.; Weverling, G.J.; Barth, P.G. Predominance of the Adrenomyeloneuropathy Phenotype of X-Linked Adrenoleukodystrophy in The Netherlands: A Survey of 30 Kindreds. Neurology 1994, 44, 2343–2346. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.; Molzer, B.; Faé, I.; Bernheimer, H. X-Linked Adrenoleukodystrophy (ALD): A Novel Mutation of the ALD Gene in 6 Members of a Family Presenting with 5 Different Phenotypes. Biochem. Biophys. Res. Commun. 1994, 205, 1638–1643. [Google Scholar] [CrossRef]
- Mahmood, A.; Dubey, P.; Moser, H.W.; Moser, A. X-Linked Adrenoleukodystrophy: Therapeutic Approaches to Distinct Phenotypes. Pediatr Transplant. 2005, 9 (Suppl. S7), 55–62. [Google Scholar] [CrossRef] [PubMed]
- Huffnagel, I.C.; Laheji, F.K.; Aziz-Bose, R.; Tritos, N.A.; Marino, R.; Linthorst, G.E.; Kemp, S.; Engelen, M.; Eichler, F. The Natural History of Adrenal Insufficiency in X-Linked Adrenoleukodystrophy: An International Collaboration. J. Clin. Endocrinol. Metab. 2019, 104, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Engelen, M.; Barbier, M.; Dijkstra, I.M.E.; Schür, R.; de Bie, R.M.A.; Verhamme, C.; Dijkgraaf, M.G.W.; Aubourg, P.A.; Wanders, R.J.A.; van Geel, B.M.; et al. X-Linked Adrenoleukodystrophy in Women: A Cross-Sectional Cohort Study. Brain 2014, 137, 693–706. [Google Scholar] [CrossRef] [Green Version]
- Huffnagel, I.C.; Dijkgraaf, M.G.W.; Janssens, G.E.; van Weeghel, M.; van Geel, B.M.; Poll-The, B.T.; Kemp, S.; Engelen, M. Disease Progression in Women with X-Linked Adrenoleukodystrophy is Slow. Orphanet J. Rare Dis. 2019, 14, 30. [Google Scholar] [CrossRef] [Green Version]
- Habekost, C.T.; Schestatsky, P.; Torres, V.F.; de Coelho, D.M.; Vargas, C.R.; Torrez, V.; Oses, J.P.; Portela, L.V.; dos Santos Pereira, F.; Matte, U.; et al. Neurological Impairment Among Heterozygote Women for X-Linked Adrenoleukodystrophy: A Case Control Study on a Clinical, Neurophysiological and Biochemical Characteristics. Orphanet J. Rare Dis. 2014, 9, 6. [Google Scholar] [CrossRef] [Green Version]
- el-Deiry, S.S.; Naidu, S.; Blevins, L.S.; Ladenson, P.W. Assessment of Adrenal Function in Women Heterozygous for Adrenoleukodystrophy. J. Clin. Endocrinol. Metab. 1997, 82, 856–860. [Google Scholar] [CrossRef]
- Jung, H.H.; Wimplinger, I.; Jung, S.; Landau, K.; Gal, A.; Heppner, F.L. Phenotypes of Female Adrenoleukodystrophy. Neurology 2007, 68, 960–961. [Google Scholar] [CrossRef]
- Moser, H.W.; Moser, A.B.; Frayer, K.K.; Chen, W.; Schulman, J.D.; O’Neill, B.P.; Kishimoto, Y. Adrenoleukodystrophy: Increased Plasma Content of Saturated Very Long Chain Fatty Acids. Neurology 1981, 31, 1241–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loes, D.J.; Hite, S.; Moser, H.; Stillman, A.E.; Shapiro, E.; Lockman, L.; Latchaw, R.E.; Krivit, W. Adrenoleukodystrophy: A Scoring Method for Brain MR Observations. Am. J. Neuroradiol. 1994, 15, 1761–1766. [Google Scholar] [PubMed]
- Loes, D.J.; Fatemi, A.; Melhem, E.R.; Gupte, N.; Bezman, L.; Moser, H.W.; Raymond, G.V. Analysis of MRI Patterns Aids Prediction of Progression in X-Linked Adrenoleukodystrophy. Neurology 2003, 61, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Mallack, E.J.; Turk, B.R.; Yan, H.; Price, C.; Demetres, M.; Moser, A.B.; Becker, C.; Hollandsworth, K.; Adang, L.; Vanderver, A.; et al. MRI Surveillance of Boys with X-Linked Adrenoleukodystrophy Identified by Newborn Screening: Meta-Analysis and Consensus Guidelines. J. Inherit. Metab. Dis. 2021, 44, 728–739. [Google Scholar] [CrossRef]
- Miller, W.P.; Rothman, S.M.; Nascene, D.; Kivisto, T.; DeFor, T.E.; Ziegler, R.S.; Eisengart, J.; Leiser, K.; Raymond, G.; Lund, T.C.; et al. Outcomes after Allogeneic Hematopoietic Cell Transplantation for Childhood Cerebral Adrenoleukodystrophy: The Largest Single-Institution Cohort Report. Blood 2011, 118, 1971–1978. [Google Scholar] [CrossRef]
- Mahmood, A.; Raymond, G.V.; Dubey, P.; Peters, C.; Moser, H.W. Survival Analysis of Haematopoietic Cell Transplantation for Childhood Cerebral X-Linked Adrenoleukodystrophy: A Comparison Study. Lancet Neurol. 2007, 6, 687–692. [Google Scholar] [CrossRef]
- Pierpont, E.I.; Eisengart, J.B.; Shanley, R.; Nascene, D.; Raymond, G.V.; Shapiro, E.G.; Ziegler, R.S.; Orchard, P.J.; Miller, W.P. Neurocognitive Trajectory of Boys Who Received a Hematopoietic Stem Cell Transplant at an Early Stage of Childhood Cerebral Adrenoleukodystrophy. JAMA Neurol. 2017, 74, 710–717. [Google Scholar] [CrossRef] [Green Version]
- Raymond, G.V.; Aubourg, P.; Paker, A.; Escolar, M.; Fischer, A.; Blanche, S.; Baruchel, A.; Dalle, J.-H.; Michel, G.; Prasad, V.; et al. Survival and Functional Outcomes in Boys with Cerebral Adrenoleukodystrophy with and without Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2019, 25, 538–548. [Google Scholar] [CrossRef] [Green Version]
- Moser, H.W. Therapy of X-Linked Adrenoleukodystrophy. NeuroRx 2006, 3, 246–253. [Google Scholar] [CrossRef]
- Zierfuss, B.; Weinhofer, I.; Kühl, J.-S.; Köhler, W.; Bley, A.; Zauner, K.; Binder, J.; Martinović, K.; Seiser, C.; Hertzberg, C.; et al. Vorinostat in the Acute Neuroinflammatory Form of X-Linked Adrenoleukodystrophy. Ann. Clin. Transl. Neurol. 2020, 7, 639–652. [Google Scholar] [CrossRef]
- Eichler, F.; Duncan, C.; Musolino, P.L.; Orchard, P.J.; De Oliveira, S.; Thrasher, A.J.; Armant, M.; Dansereau, C.; Lund, T.C.; Miller, W.P.; et al. Hematopoietic Stem-Cell Gene Therapy for Cerebral Adrenoleukodystrophy. N. Engl. J. Med. 2017, 377, 1630–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, M.S.; Mann, M.Y.; Lloyd-Puryear, M.A.; Rinaldo, P.; Howell, R.R. Newborn Screening: Toward a Uniform Screening Panel and System. Genet. Med. 2006, 8, 1S–11S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recommended Uniform Screening Panel. Available online: https://www.hrsa.gov/advisory-committees/heritable-disorders/rusp/index.html (accessed on 2 March 2021).
- Natarajan, A.; Christopher, R.; Netravathi, M.; Bhat, M.D.; Chandra, S.R. Flow Injection Ionization-Tandem Mass Spectrometry-Based Estimation of a Panel of Lysophosphatidylcholines in Dried Blood Spots for Screening of X-Linked Adrenoleukodystrophy. Clin. Chim. Acta. 2019, 495, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, W.C.; Moser, A.B.; Liu, A.C.; Jones, R.O.; Steinberg, S.J.; Lorey, F.; Panny, S.R.; Vogt, R.F.; Macaya, D.; Turgeon, C.T.; et al. Newborn Screening for X-Linked Adrenoleukodystrophy (X-ALD): Validation of a Combined Liquid Chromatography-Tandem Mass Spectrometric (LC-MS/MS) Method. Mol. Genet. Metab. 2009, 97, 212–220. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef] [Green Version]
- Burtman, E.; Regelmann, M.O. Endocrine Dysfunction in X-Linked Adrenoleukodystrophy. Endocrinol. Metab. Clin. North Am. 2016, 45, 295–309. [Google Scholar] [CrossRef]
- Regelmann, M.O.; Kamboj, M.K.; Miller, B.S.; Nakamoto, J.M.; Sarafoglou, K.; Shah, S.; Stanley, T.L.; Marino, R. Pediatric Endocrine Society Drug and Therapeutics/Rare Diseases Committee Adrenoleukodystrophy: Guidance for Adrenal Surveillance in Males Identified by Newborn Screen. J. Clin. Endocrinol. Metab. 2018, 103, 4324–4331. [Google Scholar] [CrossRef] [Green Version]
- Wiens, K.; Berry, S.A.; Choi, H.; Gaviglio, A.; Gupta, A.; Hietala, A.; Kenney-Jung, D.; Lund, T.; Miller, W.; Pierpont, E.I.; et al. A Report on State-Wide Implementation of Newborn Screening for X-Linked Adrenoleukodystrophy. Am. J. Med. Genet. A 2019, 179, 1205–1213. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Clinard, K.; Young, S.P.; Rehder, C.W.; Fan, Z.; Calikoglu, A.S.; Bali, D.S.; Bailey, D.B.; Gehtland, L.M.; Millington, D.S.; et al. Evaluation of X-Linked Adrenoleukodystrophy Newborn Screening in North Carolina. JAMA Netw. Open 2020, 3, e1920356. [Google Scholar] [CrossRef]
- Hall, P.L.; Li, H.; Hagar, A.F.; Jerris, S.C.; Wittenauer, A.; Wilcox, W. Newborn Screening for X-Linked Adrenoleukodystrophy in Georgia: Experiences from a Pilot Study Screening of 51,081 Newborns. Int. J. Neonatal Screen. 2020, 6, 81. [Google Scholar] [CrossRef]
- Matteson, J.; Sciortino, S.; Feuchtbaum, L.; Bishop, T.; Olney, R.S.; Tang, H. Adrenoleukodystrophy Newborn Screening in California Since 2016: Programmatic Outcomes and Follow-Up. Int. J. Neonatal Screen. 2021, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Burton, B.K.; Hickey, R.; Hitchins, L.; Shively, V.; Ehrhardt, J.; Ashbaugh, L.; Peng, Y.; Basheeruddin, K. Newborn Screening for X-Linked Adrenoleukodystrophy: The Initial Illinois Experience. Int. J. Neonatal Screen. 2022, 8, 6. [Google Scholar] [CrossRef]
- van Geel, B.M.; Assies, J.; Haverkort, E.B.; Barth, P.G.; Wanders, R.J.; Schutgens, R.B.; Keyser, A.; Zwetsloot, C.P. Delay in Diagnosis of X-Linked Adrenoleukodystrophy. Clin. Neurol. Neurosurg. 1993, 95, 115–120. [Google Scholar] [CrossRef]
- Schaller, J.; Moser, H.; Begleiter, M.L.; Edwards, J. Attitudes of Families Affected by Adrenoleukodystrophy toward Prenatal Diagnosis, Presymptomatic and Carrier Testing, and Newborn Screening. Genet. Test. 2007, 11, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Schwan, K.; Youngblom, J.; Weisiger, K.; Kianmahd, J.; Waggoner, R.; Fanos, J. Family Perspectives on Newborn Screening for X-Linked Adrenoleukodystrophy in California. Int. J. Neonatal Screen. 2019, 5, 42. [Google Scholar] [CrossRef] [Green Version]
- Farrell, M.H.; Sims, A.M.; Kirschner, A.L.P.; Farrell, P.M.; Tarini, B.A. Vulnerable Child Syndrome and Newborn Screening Carrier Results for Cystic Fibrosis or Sickle Cell. J. Pediatr. 2020, 224, 44–50.e1. [Google Scholar] [CrossRef]
- Waisbren, S.E.; Albers, S.; Amato, S.; Ampola, M.; Brewster, T.G.; Demmer, L.; Eaton, R.B.; Greenstein, R.; Korson, M.; Larson, C.; et al. Effect of Expanded Newborn Screening for Biochemical Genetic Disorders on Child Outcomes and Parental Stress. JAMA 2003, 290, 2564–2572. [Google Scholar] [CrossRef] [Green Version]
- Gurian, E.A.; Kinnamon, D.D.; Henry, J.J.; Waisbren, S.E. Expanded Newborn Screening for Biochemical Disorders: The Effect of a False-Positive Result. Pediatrics 2006, 117, 1915–1921. [Google Scholar] [CrossRef]
- Takashima, S.; Saitsu, H.; Shimozawa, N. Expanding the Concept of Peroxisomal Diseases and Efficient Diagnostic System in Japan. J. Hum. Genet. 2019, 64, 145–152. [Google Scholar] [CrossRef]
- Shimozawa, N.; Takashima, S.; Kawai, H.; Kubota, K.; Sasai, H.; Orii, K.; Ogawa, M.; Ohnishi, H. Advanced Diagnostic System and Introduction of Newborn Screening of Adrenoleukodystrophy and Peroxisomal Disorders in Japan. Int. J. Neonatal Screen. 2021, 7, 58. [Google Scholar] [CrossRef]
- Barendsen, R.W.; Dijkstra, I.M.E.; Visser, W.F.; Alders, M.; Bliek, J.; Boelen, A.; Bouva, M.J.; van der Crabben, S.N.; Elsinghorst, E.; van Gorp, A.G.M.; et al. Adrenoleukodystrophy Newborn Screening in the Netherlands (SCAN Study): The X-Factor. Front. Cell Dev. Biol. 2020, 8, 499. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| # | Sex | NBS C26:0-LPC Initial/Repeat | VLCFA C26:0 | ABCD1 Variant | Classification | Previously Reported? | Inheritance | Family History | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | 0.32 | 0.52 | 3.40 | c.887A>C | p.Tyr296Ser | Likely pathogenic | Yes | Maternal | No |
| 2 | Female | 0.38 | 0.3 | 2.12 | c.1166G>A | p.Arg389His | Pathogenic | Yes | Paternal | No |
| 3 | Female | 0.31 | 0.23 | 1.03 | c.1415_1416delAG | p.Gln472Profs*84 | Pathogenic | Yes | Maternal | Yes |
| 4 | Female | 0.62 | 0.32 | - | c.1447dupA | - | Pathogenic | No | - | - |
| 5 | Female | 0.29 | 0.34 | 1.97 | c.1516dupA | - | Pathogenic | No | De novo | No |
| 6 | Female | 0.43 | 0.26 | - | c.1628del | p.Pro543Argfs*15 | Pathogenic | Yes | - | No |
| 7 | Female | 0.31 | 0.28 | 2.34 | c.1690delG | - | Pathogenic | No | De novo | No |
| 8 | Female | 0.73 | 0.47 | 2.67 | c.1978C>T | p.Arg660Trp | Pathogenic | Yes | Maternal | No ^ |
| 9 | Female | 0.54 | 0.4 | 1.84 | c.2135G>A | p.Arg712His | Pathogenic | Yes | Paternal or De novo | No |
| 10 | Female | 0.81 | 0.39 | - | c.264C>A | p.Cys88* | Pathogenic | Yes | De novo | No |
| 11 | Female | 0.58 | 0.37 | 0.93 | c.346G>A | p.Gly116Arg | Pathogenic | Yes | Maternal | Yes |
| 12 | Female | 0.39 | 0.35 | 2.52 | c.390dupT | - | Pathogenic | No | Paternal or De novo | No |
| 13 | Female | 0.51 | 0.29 | 2.50 | c.521A>G | p.Tyr174Cys | Pathogenic | Yes | - | No |
| 14 | Female | 0.4 | 0.29 | 2.22 | c.838C>T | p.Arg280Cys | Pathogenic | Yes | - | No |
| 15 | Female | 0.63 | 0.36 | - | c.978G>A | p.Trp326* | Pathogenic | No | - | - |
| 16 | Female | 0.48 | 0.37 | 3.48 | Deletion of exons 3 and 4 | - | Pathogenic | No | - | No |
| 17 | Female | 0.49 | 0.26 | 2.99 | c.1533C>G | p.Cys511Trp | VUS | Yes | Maternal | No ^ |
| 18 | Female | 0.55 | 0.22 | 1.39 | c.262T>C | p.Cys88Arg | VUS | No | Maternal | No |
| 19 | Female | 0.33 | 0.34 | 1.79 | c.467G>A | p.Gly156Asp | VUS | No | Maternal | No |
| 20 | Female | 0.28 | 0.28 | 1.46 | c.700C>T | p.Arg234Cys | VUS | Yes | Maternal | No ^ |
| 21 | Female | 0.24 | 0.17 | - | c.739G>A | p.Ala247Thr | VUS | Yes | Maternal | No * |
| 22 | Female | 0.24 | 0.21 | 2.14 | c.880G>A | p.Ala294Thr | VUS | Yes | Maternal | No |
| 23 | Female | 0.23 | 0.19 | 0.76 | c.970C>T | p.Arg324Cys | VUS | Yes | Maternal | No ^ |
| 24 | Male | 0.7 | 0.2 | 2.32 | c.565C>T | p.Arg189Trp | Likely pathogenic | Yes | Maternal | Yes |
| 25 | Male | 0.52 | 0.56 | - | c.1390C>T | p.Arg464* | Pathogenic | Yes | Maternal | Yes |
| 26 | Male | 0.84 | 0.9 | - | c.1415_1416delAG | p.Gln472Profs*84 | Pathogenic | Yes | Maternal | No |
| 27 | Male | 1.08 | 0.52 | 2.90 | c.1661G>A | p.Arg554His | Pathogenic | Yes | Maternal | Yes |
| 28 | Male | 0.62 | 0.36 | - | c.1772G>A | p.Arg591Gln | Pathogenic | Yes | Maternal | No * |
| 29 | Male | 0.62 | 0.33 | - | c.1772G>A | p.Arg591Gln | Pathogenic | Yes | Maternal | No * |
| 30 | Male | 0.76 | 0.61 | 4.06 | c.796G>A | p.Gly266Arg | Pathogenic | Yes | Maternal | No |
| 31 | Male | 0.28 | 0.2 | 1.51 | c.1184C>T | p.Ala395Val | VUS | No | Maternal | No * |
| 32 | Male | 0.35 | 0.29 | 2.50 | c.1253G>A | p.Arg418Gln | VUS | Yes | Maternal | No ^ |
| 33 | Male | 0.55 | 0.3 | 3.13 | c.1448C>T | p.Thr483Met | VUS | No | Maternal | No ^ |
| 34 | Male | 0.64 | 0.75 | - | c.1832A>G | p.Gln611Arg | VUS | Yes | - | - |
| 35 | Male | 0.48 | 0.2 | - | c.229_237delTGGCTCCTG | p.Trp77_Leu79del | VUS | Yes | - | - |
| 36 | Male | 0.37 | 0.25 | 3.35 | c.229_237delTGGCTCCTG | p.Trp77_Leu79del | VUS | Yes | Maternal | No ^ |
| 37 | Male | 0.3 | 0.27 | 2.60 | c.452T>C | p.Ile151Thr | VUS | No | Maternal | Yes |
| 38 | Male | 0.67 | 0.33 | - | c.487C>T | p.Arg163Cys | VUS | No | - | - |
| 39 | Male | 0.82 | 0.39 | 2.67 | c.700C>T | p.Arg234Cys | VUS | Yes | Maternal | No * |
| 40 | Male | 0.69 | 0.3 | 3.18 | c.700C>T | p.Arg234Cys | VUS | Yes | Maternal | Yes |
| 41 | Male | 0.29 | 0.27 | - | c.739G>A | p.Ala247Thr | VUS | Yes | - | - |
| 42 | Male | 0.86 | 0.97 | 3.05 | c.824G>C | p.Arg275Pro | VUS | Yes | Maternal | No ^ |
| 43 | Male | 0.41 | 0.33 | 1.34 | c.851C>T | p.Ser284Leu | VUS | No | Maternal | No |
| 44 | Male | 0.31 | 0.27 | - | c.851C>T | p.Ser284Leu | VUS | Yes | Maternal | No * |
| # | Sex | NBS C26:0-LPC Initial/Repeat | VLCFA C26:0 | ABCD1 Variant | Screen Outcome | |
|---|---|---|---|---|---|---|
| 1 | Female | 0.64 | 0.4 | 2.57 | none | Parent refusal |
| 2 | Female | 0.36 | 0.29 | 0.76 | none | False positive |
| 3 | Male | 0.33 | 0.19 | 0.90 | none | False positive |
| 4 | Female | 0.69 | 0.48 | 2.47 | none | Peroxisomal biogenesis defect |
| 5 | Male | 1.32 | 1.36 | 8.75 | none | Peroxisomal biogenesis defect |
| 6 | Male | 1.19 | 1.82 | 21.48 | none | Peroxisomal biogenesis defect |
| 7 | Unknown | 2.18 | 2.22 | - | none | Peroxisomal biogenesis defect |
| State | Tier 1: Method/Target/Cutoff | Tier 2: Method/Target/Cutoff | ABCD1 Sequencing | ||
|---|---|---|---|---|---|
| California [43] | FIA-MS/MS | C26 ≥ 0.42 µmol/L | LC-MS/MS | C26 ≥ 0.22 µmol/L a | Integrated with NBS |
| Georgia [42] | FIA-MS/MS | CLIR analysis of C20, C22, C24, and C26 LPC | LC-MS/MS | C26:0-LPC > 0.30 nmol/mL | Following referral |
| Illinois [44] | LC-MS/MS | Borderline: C26:0-LPC ≥ 0.18 µmol/L Positive: C26:0-LPC ≥ 0.28 µmol/L | LC-MS/MS | Borderline: C26:0-LPC ≥ 0.18 µmol/L Positive: C26:0-LPC ≥ 0.28 µmol/L | Following referral |
| New York [2] | MS/MS | C26:0-LPC | HPLC-MS/MS | C26:0-LPC | Integrated with NBS |
| North Carolina [41] | HPLC-MS/MS | C24:0-LPC ≥ 0.175 µmol/L and C26:0-LPC ≥ 0.08 µmol/L | Duplicate HPLC-MS/MS | Median C26:0-LPC ≥ 0.15 µmol/L OR Median C26:0-LPC 0.08–0.15 µmol/L and C24:0-LPC ≥ 0.175 µmol/L | Integrated with NBS |
| Minnesota [40] | LC-MS/MS | Borderline: C26:0-LPC ≥ 0.16 µmol/L Positive: C26:0-LPC ≥ 0.30 µmol/L | Repeat LC-MS/MS | C26:0-LPC ≥ 0.16 µmol/L | Following referral |
| Pennsylvania | FIA-MS/MS | C26:0-LPC > 0.36 µmol/L | LC-MS/MS | C26:0-LPC > 0.15 µmol/L | Integrated with NBS |
| State | Publication | Study Length | Total # Screened | Positive Screens | Male X-ALD | Female Heterozygote | Peroxisome Biogenesis Disorder | Other Genetic Syndrome |
|---|---|---|---|---|---|---|---|---|
| California | Matteson et al., 2021 [43] | 4 years | 1,854,631 | 355 | 95 | 110 | 23 | 12 |
| Georgia | Hall et al., 2020 [42] | 7 months | 51,081 | 11 | 1 | 0 | 2 | 0 |
| Illinois | Burton et al., 2022 [44] | 1 year 11 months | 276,000 | 34 a | 7 | 10 b | 3 | 0 |
| New York | Moser et al., 2016 [2] | 2 years 8 months | 630,000 | 53 | 20 c | 22 | - d | - d |
| North Carolina | Lee et al., 2020 [41] | 6 months | 52,301 | 12 | 3 | 3 | 1 | 1 |
| Minnesota | Wiens et al., 2019 [40] | 1 year | 67,836 | 14 | 9 | 5 | 0 | 0 |
| Pennsylvania | Present Study | 4 years 2 months | 542,554 | 51 | 21 | 23 | 4 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priestley, J.R.C.; Adang, L.A.; Drewes Williams, S.; Lichter-Konecki, U.; Menello, C.; Engelhardt, N.M.; DiPerna, J.C.; DiBoscio, B.; Ahrens-Nicklas, R.C.; Edmondson, A.C.; et al. Newborn Screening for X-Linked Adrenoleukodystrophy: Review of Data and Outcomes in Pennsylvania. Int. J. Neonatal Screen. 2022, 8, 24. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8020024
Priestley JRC, Adang LA, Drewes Williams S, Lichter-Konecki U, Menello C, Engelhardt NM, DiPerna JC, DiBoscio B, Ahrens-Nicklas RC, Edmondson AC, et al. Newborn Screening for X-Linked Adrenoleukodystrophy: Review of Data and Outcomes in Pennsylvania. International Journal of Neonatal Screening. 2022; 8(2):24. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8020024
Chicago/Turabian StylePriestley, Jessica R. C., Laura A. Adang, Sarah Drewes Williams, Uta Lichter-Konecki, Caitlin Menello, Nicole M. Engelhardt, James C. DiPerna, Brenda DiBoscio, Rebecca C. Ahrens-Nicklas, Andrew C. Edmondson, and et al. 2022. "Newborn Screening for X-Linked Adrenoleukodystrophy: Review of Data and Outcomes in Pennsylvania" International Journal of Neonatal Screening 8, no. 2: 24. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8020024