
Applicability of the Leiden Convention and the Lipton Classification in Patients with a Single Coronary Artery in the Setting of Congenital Heart Disease

 , and
, and
Abstract: Background
1. Introduction
2. Materials and Methods
3. Results
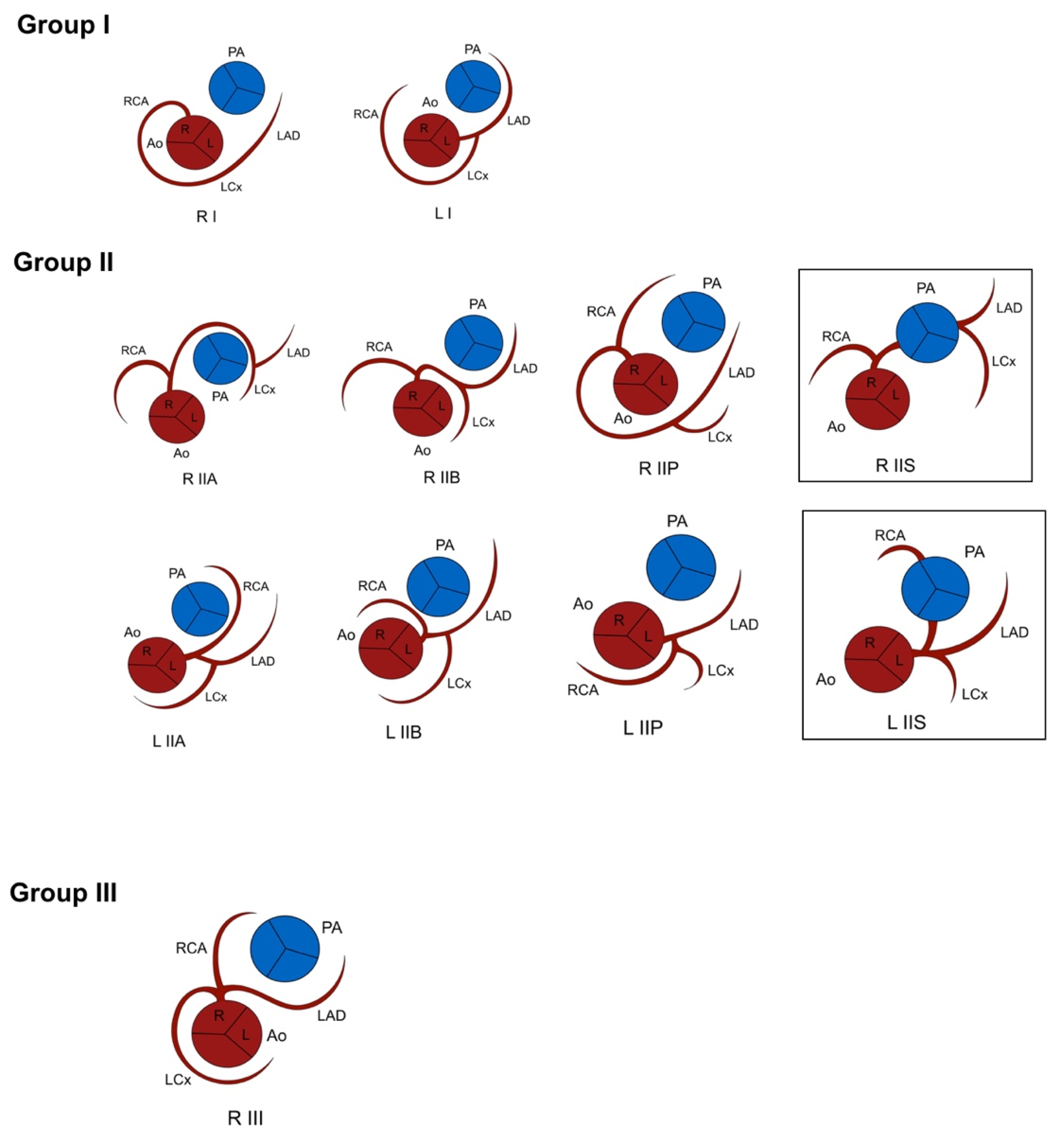
3.1. Lipton Classification
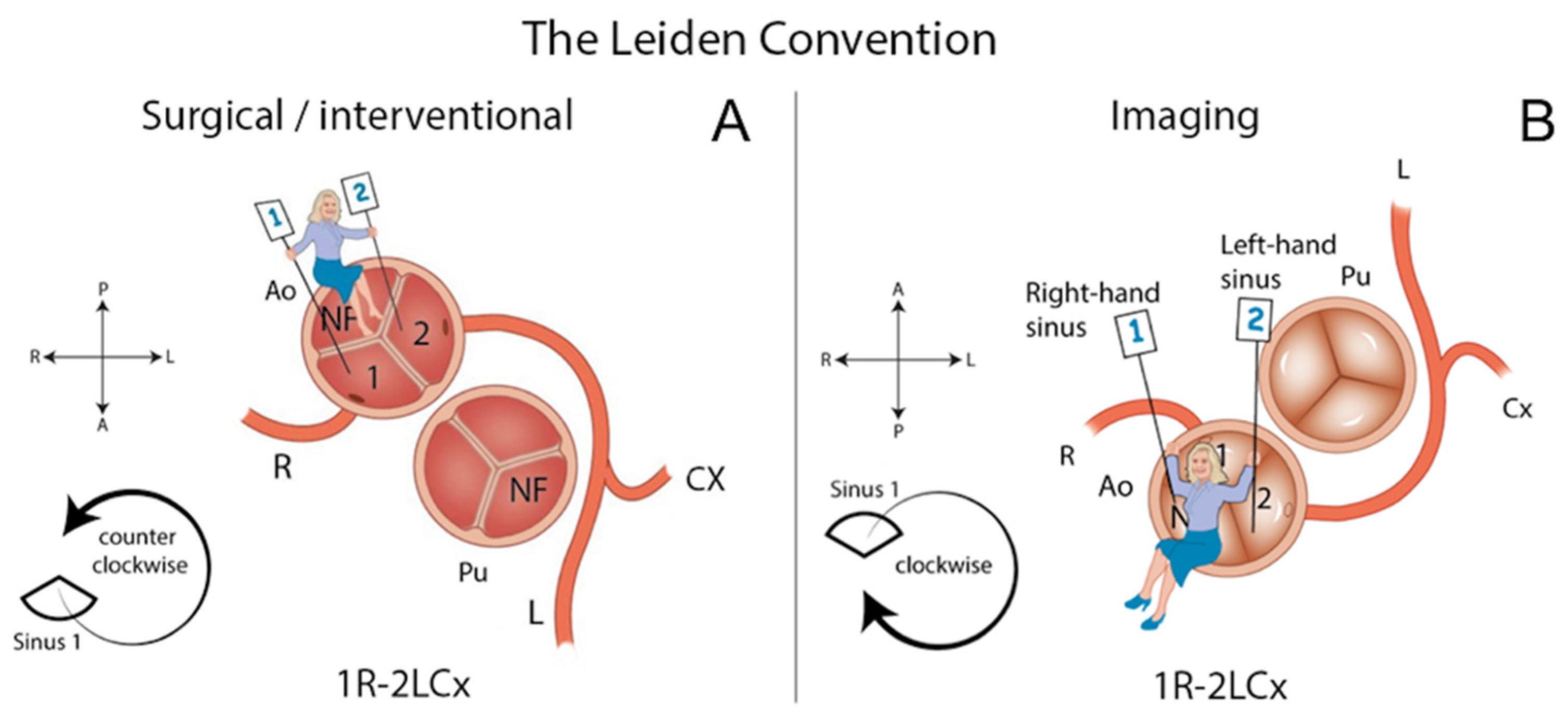
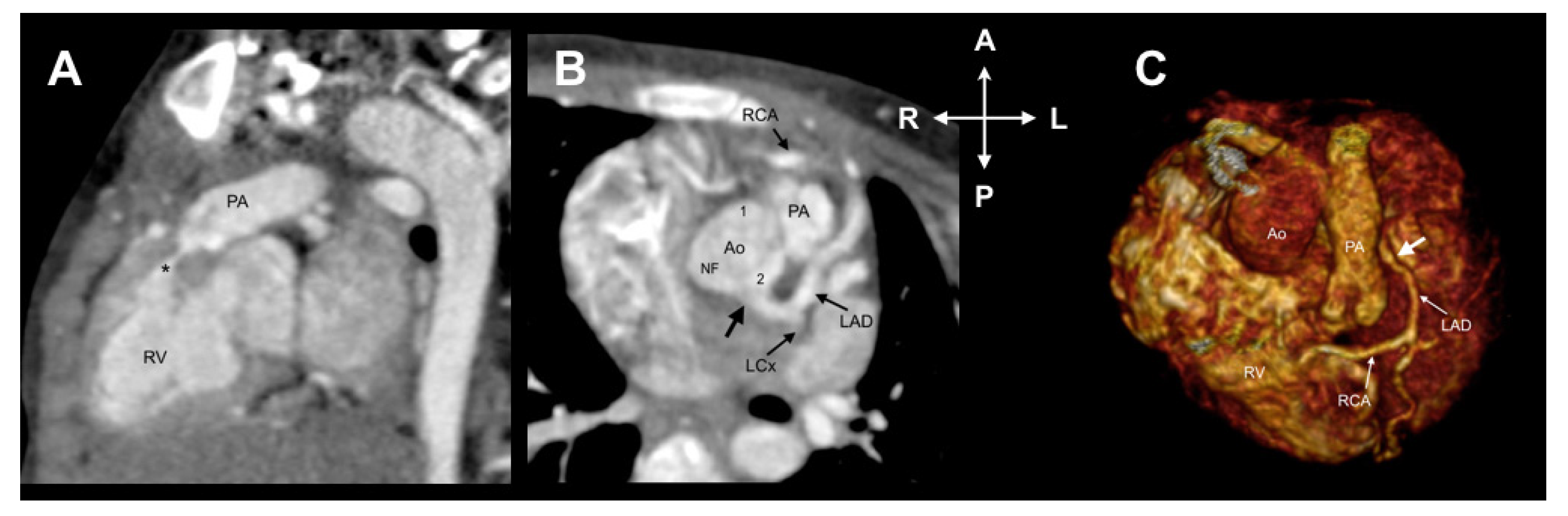
3.2. Leiden Convention Coronary Coding System
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aldana-Sepulveda, N.; Restrepo, C.S.; Kimura-Hayama, E. Single coronary artery: Spectrum of imaging findings with multidetector CT. J. Cardiovasc. Comput. Tomogr. 2013, 7, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Lipton, M.J.; Barry, W.H.; Obrez, I.; Silverman, J.F.; Wexler, L. Isolated single coronary artery: Diagnosis, angiographic classification, and clinical significance. Radiology 1979, 130, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, O.; Hobbs, R.E. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Catheter. Cardiovasc. Diagn. 1990, 21, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Gittenberger-de Groot, A.C.; Sauer, U.; Oppenheimer-Dekker, A.; Quaegebeur, J. Coronary arterial anatomy in transposition of the great arteries: A morphologic study. Pediatr. Cardiol. 1983, 4, 15–24. [Google Scholar]
- Gittenberger-de Groot, A.C.; Koenraadt, W.M.C.; Bartelings, M.M.; Bökenkamp, R.; DeRuiter, M.C.; Hazekamp, M.G.; Bogers, A.; Quaegebeur, J.M.; Schalij, M.J.; Vliegen, H.W.; et al. Coding of coronary arterial origin and branching in congenital heart disease: The modified Leiden Convention. J. Thorac. Cardiovasc. Surg. 2018, 156, 2260–2269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koppel, C.J.; Vliegen, H.W.; Bökenkamp, R.; Ten Harkel, A.D.J.; Kiès, P.; Egorova, A.D.; Jukema, J.W.; Hazekamp, M.G.; Schalij, M.J.; Gittenberger-de Groot, A.C.; et al. The Leiden Convention coronary coding system: Translation from the surgical to the universal view. Eur. Heart J. Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Van Praagh, R.; Van Praagh, S. The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its embryologic implications. A study of 57 necropsy cases. Am. J. Cardiol. 1965, 16, 406–425. [Google Scholar] [CrossRef]
- De Agustín, J.A.; Marcos-Alberca, P.; Manzano Mdel, C.; Fernández-Golfín, C.; Pérez de Isla, L.; Hernández Antolín, R.; Macaya, C.; Zamorano, J. Percutaneous Intervention in a single coronary artery: Evaluation of multislice tomography and its feasibility. Rev. Esp. Cardiol. 2010, 63, 607–611. [Google Scholar] [CrossRef]
- Mandal, S.; Tadros, S.S.; Soni, S.; Madan, S. Single coronary artery anomaly: Classification and evaluation using multidetector computed tomography and magnetic resonance angiography. Pediatr. Cardiol. 2014, 35, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.; Sammut, E.; Nair, A.; Rajani, R.; Bonamini, R.; Chiribiri, A. Coronary artery anomalies overview: The normal and the abnormal. World J. Radiol. 2016, 8, 537–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Xu, L.; Zhang, N.; Wang, H.; Liu, W.; Sun, Z.; Fan, Z. CT coronary angiography findings in non-atherosclerotic coronary artery diseases. Clin. Radiol. 2018, 73, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houyel, L.; Bajolle, F.; Capderou, A.; Laux, D.; Parisot, P.; Bonnet, D. The pattern of the coronary arterial orifices in hearts with congenital malformations of the outflow tracts: A marker of rotation of the outflow tract during cardiac development? J. Anat. 2013, 222, 349–357. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Gender | Age | Associated Anomalies | Anatomical Relationship of the Ao to the PA | Leiden Convention | Lipton Classification | Concomitant Coronary Anomaly |
|---|---|---|---|---|---|---|---|
| 1 | M | 1M | Double-outlet right ventricle | Right anterior | 2LCx | LI | Absent RCA |
| 2 | F | 2M | Truncus arteriosus Van Praagh type A4 | NA | NA | NI* | None |
| 3 | F | 6M | Pulmonary atresia. Single outlet right ventricle. Right aortic arch. | NA | NA | NI* | None |
| 4 | F | 6M | Pulmonary atresia. Single outlet right ventricle. | NA | NA | NI* | None |
| 5 | F | 8M | Transposition of the great arteries | Left anterior | 2CxRL | NI* | None |
| 6 | F | 3Y | Tetralogy of Fallot | Clockwise rotation of the aortic root | 2RLCx | LIIA | Anomalous origin of RCA from LAD |
| 7 | M | 3Y | Double-outlet right ventricle. Common atrioventricular canal type C of Rastelli. Right aortic arch | Left anterior | 1LCxR | NI* | None |
| 8 | F | 4Y | Stenosis left ventricular outflow tract by fibromuscular protrusion | Right posterior | 2LCx | LI | Absent RCA |
| 9 | M | 4Y | Tetralogy of Fallot | Clockwise rotation of the aortic root | 2RLCx | LIIA | Anomalous origin of RCA from LAD |
| 10 | M | 4Y | Pulmonary atresia. Ambiguous atrioventricular connection. Right aortic arch | NA | NA | NI* | None |
| 11 | F | 5Y | Truncus arteriosus Van Praagh type A1. Right aortic arch | NA | NA | RIII | None |
| 12 | F | 5Y | Syndrome Noonan | Right posterior | 2RLCx | LIIA | None |
| 13 | F | 6Y | Double-outlet right ventricle | Right anterior | 2LCxR | NI* | None |
| 14 | F | 8Y | Isolated | Right posterior | 1RLCx | RIIS | None |
| 15 | F | 9Y | Double-outlet right ventricle. Pulmonary atresia | NA | NA | NI* | None |
| 16 | M | 10Y | Tetralogy of Fallot | Clockwise rotation of the aortic root | 1RLCx | RIIA | None |
| 17 | F | 10Y | Pulmonary agenesis. Common atrioventricular connection. Single outlet right ventricle | NA | NA | NI* | None |
| 18 | F | 11Y | Pulmonary atresia | NA | NA | NI* | None |
| 19 | M | 12Y | Pulmonary agenesis. Single outlet right ventricle. Right aortic arch | NA | NA | NI* | None |
| 20 | F | 13Y | Mitral valve prolapse | Right posterior | 1RL*Cx | RIII | None |
| 21 | M | 14Y | Transposition of the great arteries | Left anterior | 1LCxR | RIIP | None |
| 22 | M | 15Y | Supravalvular aortic stenosis | Right posterior | 2R*LCx | LIIB | None |
| 23 | M | 15Y | Tetralogy of Fallot | Clockwise rotation of the aortic root | 2RLCx | LIIA | Anomalous origin of RCA from LAD |
| 24 | M | 16Y | Transposition of the great arteries | Right anterior | 1RLCx | NI* | None |
| 25 | F | 18Y | Pulmonary atresia | NA | NA | NI* | None |
| 26 | F | 25Y | Pulmonary atresia. Double inlet left ventricle. Right aortic arch | NA | NA | NI* | None |
| 27 | F | 37Y | Atrial septal defect. Ventricular septal defect | Right posterior | 2R*LCx | LIIB | Anomalous origin of RCA from LAD |
| 28 | F | 51Y | Left ventricular non-compaction | Right posterior | 2RLCx | LIIA | Anomalous origin of RCA from LAD |
| 29 | M | 52Y | Isolated | Right posterior | 2LCx | LI | Absent RCA |
| 30 | M | 53Y | Dysplastic aortic valve | Right posterior | 2LCx | LI | Absent RCA |
| 31 | M | 58Y | Coronary artery disease. Rupture of right sinus of Valsalva aneurysm | Right posterior | 2LCxR | LIIP | None |
| 32 | F | 78Y | Isolated | Right posterior | 2RLCx | LIIA | Anomalous origin of RCA from LAD |
| Lipton Classification | Leiden Convention | |
|---|---|---|
| Patient Number | Associated Anomaly Preventing Use of Both Classification Systems | |
| 2 | Posterior sinus | Truncus arteriosus type A4 |
| 3 | Posterior sinus | Pulmonary atresia |
| 4 | Course not included | Pulmonary atresia |
| 10 | Course not included | Pulmonary atresia |
| 15 | Posterior sinus | Pulmonary atresia |
| 17 | Posterior sinus | Pulmonary atresia |
| 18 | Posterior sinus | Pulmonary atresia |
| 19 | Course not included | Pulmonary atresia |
| 5 | Course not included | Pulmonary atresia |
| 26 | Posterior sinus | Pulmonary atresia |
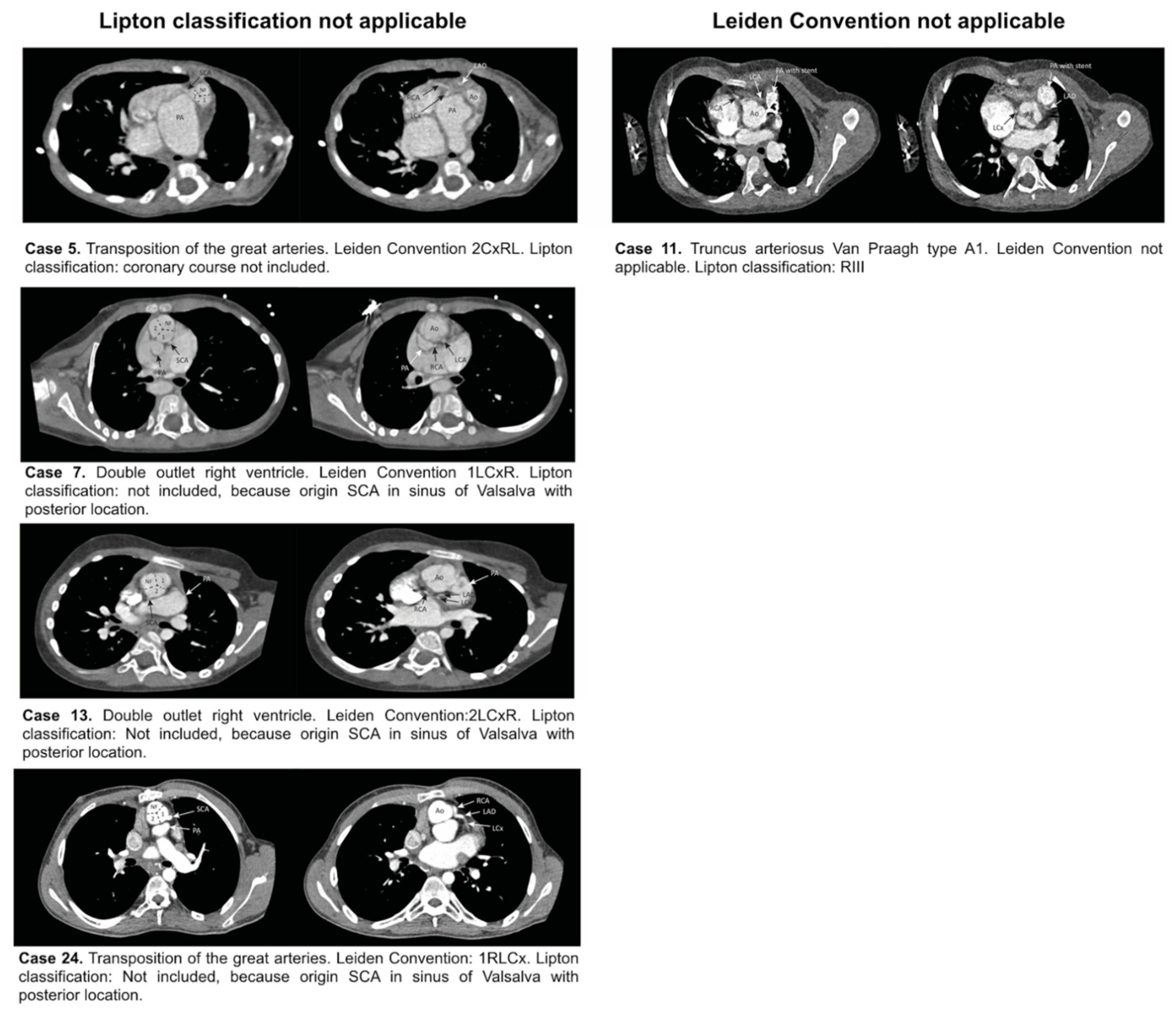
| Lipton classification applicable, Leiden Convention not applicable (Figure 5) | ||
| 11 | RIII | Truncus arteriosus type A1 |
| Lipton classification not applicable, Leiden Convention applicable (Figure 5) | ||
| 5 | Course not included | 2CxRL |
| 7 | Posterior sinus | 1LCxR |
| 13 | Posterior sinus | 2LCxR |
| 24 | Posterior sinus | 1RLCx |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katekaru-Tokeshi, D.I.; Jiménez-Santos, M.; Koppel, C.J.; Vliegen, H.W.; Díaz-Zamudio, M.; Castillo-Castellón, F.; Jongbloed, M.R.M.; Kimura-Hayama, E. Applicability of the Leiden Convention and the Lipton Classification in Patients with a Single Coronary Artery in the Setting of Congenital Heart Disease. J. Cardiovasc. Dev. Dis. 2021, 8, 93. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080093
Katekaru-Tokeshi DI, Jiménez-Santos M, Koppel CJ, Vliegen HW, Díaz-Zamudio M, Castillo-Castellón F, Jongbloed MRM, Kimura-Hayama E. Applicability of the Leiden Convention and the Lipton Classification in Patients with a Single Coronary Artery in the Setting of Congenital Heart Disease. Journal of Cardiovascular Development and Disease. 2021; 8(8):93. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080093
Chicago/Turabian StyleKatekaru-Tokeshi, Diana Isabel, Moisés Jiménez-Santos, Claire J. Koppel, Hubert W. Vliegen, Mariana Díaz-Zamudio, Francisco Castillo-Castellón, Monique R. M. Jongbloed, and Eric Kimura-Hayama. 2021. "Applicability of the Leiden Convention and the Lipton Classification in Patients with a Single Coronary Artery in the Setting of Congenital Heart Disease" Journal of Cardiovascular Development and Disease 8, no. 8: 93. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080093