
Renaming NAFLD to MAFLD: Could the LDE System Assist in This Transition?


Department of Internal Medicine, Azienda Ospedaliero-Universitaria di Modena, 4110 Modena, Italy
J. Clin. Med. 2021, 10(3), 492; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030492
Submission received: 16 December 2020
/
Revised: 25 January 2021
/
Accepted: 27 January 2021
/
Published: 31 January 2021
(This article belongs to the Special Issue Should Physicians Consider NAFLD a Primary or Secondary Disease?)
Abstract
:Our understanding of fatty liver syndromes and their relationship with the metabolic syndrome has improved over recent decades and, paralleling this, we are now at the dawn of the NAFLD (nonalcoholic fatty liver disease) to MAFLD (metabolic-associated fatty liver disease) transition. The pitfalls of NAFLD diagnosis, together with disappointing results in therapeutic trials, and the inconsistencies and risks inherent in a “negative” definition (such as “nonalcoholic”) as opposed to a “positive” one (i.e., “metabolic”) are predicted to facilitate the proposed renaming of NAFLD to MAFLD. However, a premature change of terminology would not necessarily address major unmet needs in this area, and may even become counterproductive. As an aid to selecting more homogeneous cohorts of patients, I propose the LDE (Liver, Determinants, Extra-hepatic) classification system which, in principle, may help to assess the natural course of disease as well as the efficacy of novel drugs in patients with NAFLD/MAFLD.
1. Background, Aim and Method
Steatosis, i.e., the pathological accumulation of intra-hepatic fat content, has been known since 1845 thanks to the work by Addison, who described liver histology changes induced by alcohol [1]. In 1938, Connor pinpointed the potential for fatty liver disease, owing to either alcohol or diabetes, to progress to liver cirrhosis [2] and, in 1964, Dianzani clearly addressed the pathogenesis of steatosis [3]. However, it was not until the 1980s that the terms “nonalcoholic steatohepatitis” (NASH) and “nonalcoholic fatty liver disease” (NAFLD) were coined by Ludwig et al. [4], and Shaffner and Thaler [5], respectively. Following decades of research, we are now fully aware that NAFLD and NASH are pathogenically diverse, are common in the general population on a worldwide basis, exact a heavy toll in terms of medical-related as well as indirect expenditures and remain orphans of an effective and safe drug treatment [6,7,8,9]. Of concern, many NASH trials fail [10], suggesting that we are far from dominating this non-transmissible though epidemic liver disease. Recently, based on previous suggestions reviewed in [11], it has been proposed that NAFLD should be renamed as MAFLD, i.e., metabolic-(associated) fatty liver disease [12,13]. With this background, the present review aims at illustrating the reasons underlying the debate on nomenclature of common fatty liver syndromes while highlighting unanswered research questions. Finally, I will illustrate a novel proposal of classification, the so called LDE (Liver, Determinants, Extra-hepatic) system, which may integrate both NAFLD and MAFLD for better pheno-genotyping of individual patients and cohorts. With the aim of analyzing published studies, the Pub Med data base was consulted using the following key-words: NAFLD, NASH, and MAFLD, without date limitations. Only references that were deemed to be relevant to the topic were retained.
2. NAFLD, Diagnosis, Pitfalls and Classification
NAFLD, comprising the whole gamut of alcohol-like liver lesions (i.e., steatosis, steatohepatitis with/without fibrosis, cirrhosis and hepatocellular carcinoma (HCC)) though observed in the nonalcoholic [14], was formerly believed to be “the hepatic manifestation of the Metabolic Syndrome”. However, this old notion is, at best, incomplete and accumulating data strongly indicate that the association of NAFLD with Metabolic Syndrome is indeed mutual and bi-directional [15,16,17].
The diagnosis of NAFLD is based on the non-invasive identification of fatty changes in the liver (through biomarkers and/or imaging studies) in the absence of competing causes of (steatogenic) liver disease [18]. Compared to biomarkers and other imaging techniques (such as Computed Tomography scanning and Magnetic Resonance) conventional ultrasonography retains a key role in as much as it is cheap, repeatable, widely available, allows the ruling out of focal liver disease and permits those semi-quantitative evaluations that mirror metabolic derangements and liver histology changes [19,20]. Liver biopsy is the diagnostic standard, given that it provides a definite characterization of the elementary histological lesions: steatosis, ballooning, inflammation and fibrosis, thereby permitting the differentiation of the more indolent uncomplicated steatosis from the more rapidly progressive NASH forms [21,22]. Pros and cons of the two chief histological methods of assessment including the American NASH Clinical Research Network (CRN) and the European Fatty Liver Inhibition of Progression (FLIP) have been discussed analytically elsewhere [23]. Importantly, neither the CRN nor the FLIP system evaluate portal chronic inflammation and the presence and location of Mallory-Denk bodies, which may raise the point of the differentiation of NAFLD from viral hepatitis, cholestatic disease and Wilson’s disease [24]. Moreover, the use of a numerical histological endpoint in the NASH clinical trials (typically the decrease of NAFLD activity score (NAS) by ≥2, without any worsening of fibrosis stage) will not necessarily guarantee the resolution of NASH [24]. The histological distinction of cases of NAFLD from those owing to competing liver diseases, such as drug-induced liver injury, congestive hepatopathy and lysosamial acid lipase deficiency, represent additional pitfalls [25]. Concurrent autoimmune hepatitis and NASH may be quite hard to distinguish histologically and steroid administration may improve the histological activity of autoimmune hepatitis while worsening NASH [26].
Per classification (Table 1), NAFLD is defined as “primary” when it is associated with (or deemed to herald an incidence of) Metabolic Syndrome [27,28,29]. “Secondary” NAFLD forms are myriad and include, among others, diseases occurring as a result of nutritional disorders, complications of abdominal surgery, use of several drugs, occupational exposure to organic solvents and (rare) metabolic disorders [27,30]. In addition, NAFLD may often occur secondarily to common viral infections (the so called “virus-associated fatty liver disease” or VAFLD) [31] and frequently occurring endocrine derangements [32]. These secondary NAFLD forms need to remain separated from primary NAFLD given that, for example, VAFLD owing to HIV infection follows a worse course than primary NAFLD [33] and that NAFLD associated with hypothyroidism has a specific pathogenesis which, in theory, is amenable to complete reversal following thyroid hormone replacement therapy [34].
NAFLD exacts a heavy toll on global medical expenditures. Younossi reported that the direct medical costs related to NAFLD per year were, in the United States, about $103 billion and, in four European countries alone (Germany, France, Italy, and United Kingdom), it totaled about €35 billion [35].
3. The Metabolic Syndrome
The development of Metabolic Syndrome, which defines the cluster of multiple cardio-metabolic derangements including visceral obesity, dyslipidemia, arterial hypertension, and type 2 diabetes mellitus, is deemed to be affected by those lifestyle habits which are typical of industrialized countries and also adopted by many developing countries [36]. Metabolic Syndrome is triggered by visceral obesity [37] which, in its turn, results from a positive energy balance owing to poor diets and a sedentary lifestyle [38], together with an as yet incompletely defined polygenic hereditary asset [39]. Insulin resistance is central in the pathogenesis of Metabolic Syndrome [40]. This is not to say that the ultimate mechanisms which are eventually conducive to the development of visceral adiposity and insulin resistance are limpidly clear and indeed it is possible that central dysregulation plays a key role [41]. Confirming this, a recent study found that that high brain insulin sensitivity anticipates weight loss during lifestyle intervention and is associated with a favorable body fat distribution; additionally, high brain insulin sensitivity is also associated with less regain of fat mass during a nine-year follow-up [42].
In many animals, including mammals, the regulation of reproductive, metabolic and behavioral activities follows a cyclical pattern of responses. Light exposure is believed to orchestrate such responses through the regulation of melatonin secretion [43]. For example, facilitated by an abundance of nutrients during longer summer days, hibernating mammals adopt those behavioral changes (such as decreased sleep length and maximized food intake) properly suited to storing energy that will rapidly result in a state of insulin resistance and altered secretion of adiponectin and leptin [43]. Conversely, during longer winter nights, increased melatonin secretion, which is regulated via the suprachiasmatic nucleus, will enhance insulin sensitivity and energy availability whilst the animal is dormant [43]. It is conceivable that human diseases possibly recapitulate animal behavior and, if this is the case, that the Metabolic Syndrome may mimic a “pre-hibernation” state reflecting dysregulation of neural pathways. This innovative pathogenic perspective paves the way for a line of research addressing deregulated serotonin pathways and psycho-depression among those with nonalcoholic fatty liver disease (NAFLD) [44,45,46]. For example, a subset of well characterized patients might be submitted to psychological counseling to disclose and address those offending life events and traumatic experiences that will eventually be conducive to depression in predisposed individuals. Other individuals with NAFLD might conceivably be administered antidepressants, though in the setting of randomized controlled trials (RCTs) on NASH, while keeping in mind that this class of drugs may often bear unfavorable metabolic effects.
Irrespective of its intimate patho-mechanisms, Metabolic Syndrome exacts a heavy toll on medical expenditures [47].
4. NAFLD and the Metabolic Syndrome: Chicken or Egg?
As alluded to above, a consistent body of evidence supports the notion that a bi-directional relationship links NAFLD with (features of) Metabolic Syndrome, with insulin resistance being the shared common pathophysiological denominator [48]. In the medical literature, the historical “chicken and egg” debate regarding the chronological association of NAFLD with Metabolic Syndrome, [41] eventually found its answer through novel data showing that NAFLD is both the cause and the effect of the Metabolic Syndrome (reviewed in [16,17]). However, it soon became clear that addressing the key pathogenic determinants of NASH would not necessarily improve disease outcomes. One of the first lines of evidence regarding this was provided by the finding that insulin sensitizers failed to invariably reverse NASH in all cases, did not reverse or even worsened mitochondrial abnormalities in NASH and, conversely, histological improvement, at least in some patients, was observed with pharmacological agents, such as vitamin E, acting through mechanisms other than insulin sensitization [49].
Why then, in overt conflict with studies on pathogenesis, is the correction of insulin resistance invariably not sufficient to successfully treat NASH in the majority of patients? This probably results from varying pathogenic mechanisms, concurring to determine liver damage to a variable extent in the individual patients. Based on this notion, treatment should be tailored to the individual subject [49]. However, how this can be accomplished is far from established.
A variety of pathogenic mechanisms interactively take part in the development of NAFLD/NASH and the identification of the role of each in the individual patient is an unmet research and clinical challenge. Just to provide a few examples, should individuals with NAFLD in the absence of Metabolic Syndrome [50] and those with lean NAFLD [51] be treated in a similar way to those with obesity? Should men and women be treated alike despite this not being evidence-based? [52].
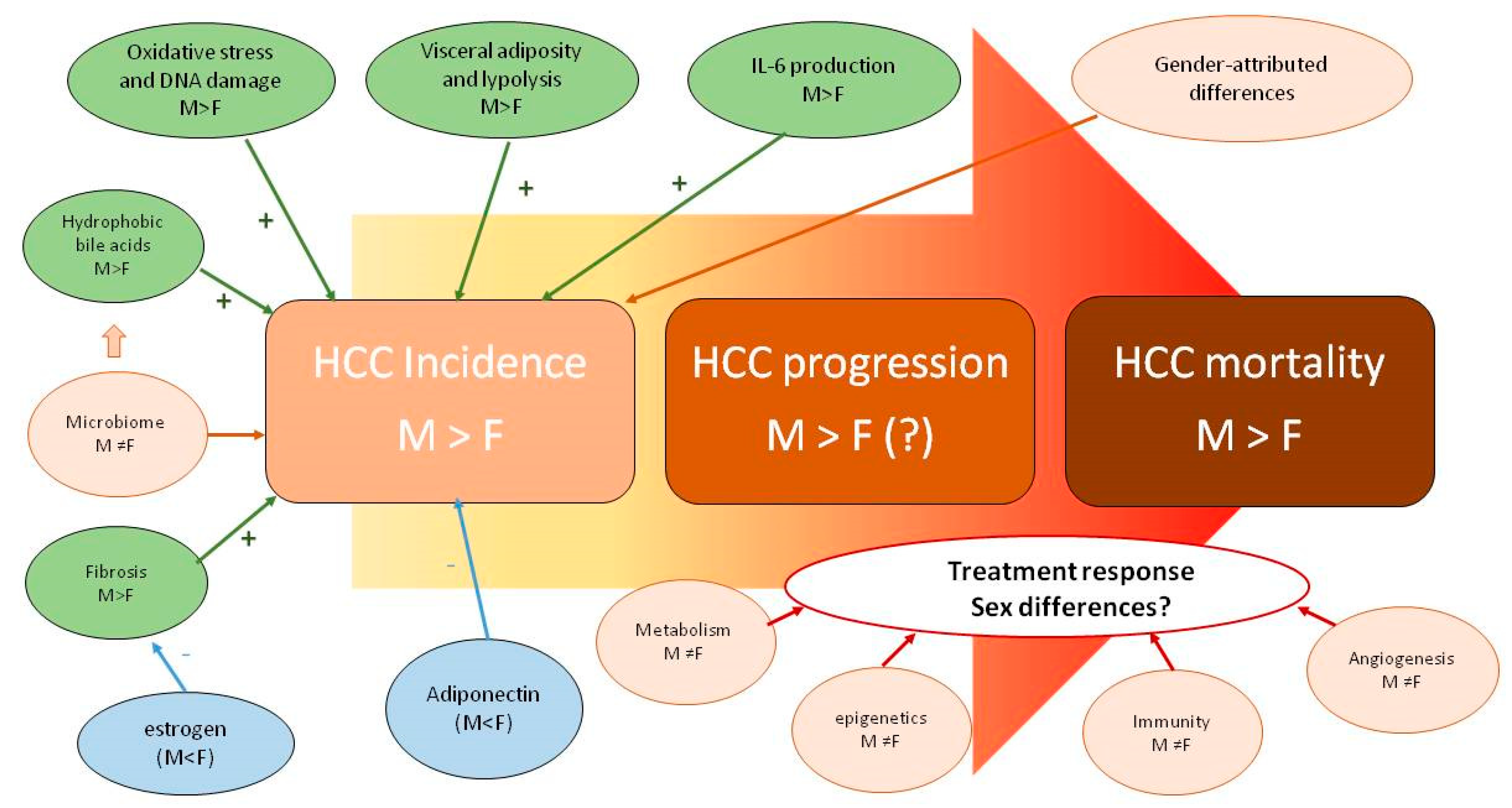
Irrespective of whether NAFLD is the cause or the effect of Metabolic Syndrome (and we now know it is both), it is worth highlighting that these two conditions are synergistic risk factors for the development of HCC [48]. HCC represents the most common primary liver cancer and is the fourth most common cause of mortality owing to cancer [53]. The reasons underlying differences in the male-to-female ratio of the incidence of HCC (which ranges between 2–3 in most countries) are intriguing and incompletely understood (Figure 1).
The biological grounds underlying sex disparity in the incidence, progression and mortality of HCC are incompletely understood and probably related to multiple factors pertaining to individual life habits and endocrine-metabolic factors, as well as to cancer biology per se.
Interestingly, similar to HCC, NAFLD and the Metabolic Syndrome have distinct features of sexual dimorphism which include the prevalence and significance of dysglycemia (impaired fasting glucose versus impaired glucose tolerance); sexual dimorphism in body fat distribution and patterns of android and gynoid obesity; pathobiology of adipocytes including cell size and function; and the influence of estrogen decline on clustering risk factors and the inherent dangers of liver fibrosis progression [52,54,55].
In their seminal article, voicing concerns from an established pipeline of previous studies, Bellentani and Tiribelli properly identified the limitations included in the “negative” definition of NAFLD and NASH as opposed to a positive one, i.e., “metabolic” [56]. In agreement, Fouad et al. also pinpointed that the allusion to alcohol contained in the term “nonalcoholic” incurred the risks of trivialization, stigmatization and non-consideration from health authorities [11]. Adding to the above limitations and risks, the impressive number of “therapeutic casualties” of innovative drugs in the NASH trials arena including simtuzumab, selnsertib, emricasan and MSDC-0602K, calls for careful consideration [57,58,59,60].
The reasons underlying this cemetery of failures are undoubtedly multiple and include the variability in endpoints adopted over time [61], as well as disease modifiers such as diet and exercise [62]. Ratziu and Friedman have recently argued that factors that may impact on the outcomes of NASH trials should be differentiated into NASH-cirrhosis as opposed to non-cirrhotic disease, and in pre-clinical vs. clinical studies; that some of these failures result from the overly simplistic interpretation of findings from small-sized pilot studies; and that the identification of primary versus secondary end-points may be confusing and the effects of alcohol and placebo uncertain [10]. It is also clear, in my opinion, that cohorts of NASH patients enrolled in RCTS are homogenous only with regard to liver biopsy findings rather than for determinants and extra-hepatic features of disease (such as those more extensively discussed below). This may be a strong limitation given that any given liver histology finding in the individual patient is the final result of often substantially differing spectra of pathogenic and systemic scenarios which may potentially affect, more than liver histology per se, response to treatments. In other words, liver histology compatible with NASH may underly a variable proportion of different contributions resulting from sex, genetics, endocrine modifiers, lifestyle habits, and concurrent extra-hepatic clinical phenotypes which, taken collectively, have the potential to alter the natural course of liver disease in the individual patient. All the considerations illustrated above, including the pitfalls in NASH diagnosis and the inconsistencies and the risks of a negative definition, together with the inability of the NAFLD terminology to provide homogeneous cohorts of NASH patients to submit to RCTs, strongly support the notion that a change in NAFLD terminology is an urgent and unmet research priority.
5. The NAFLD-MAFLD Debate
In trying to incorporate those proposals regarding the inaccuracy and possible negative consequences of using the term “NAFLD” that have accumulated over the past twenty years, a panel of experts from as many as 22 countries has recently proposed novel names and definitions for NAFLD in adults—namely, metabolic dysfunction-associated fatty liver disease (MAFLD) [12,13]. This proposal has rapidly gained consensus in Latin America, North Africa and the Middle East [62,63], indicating that the motivations to abandon the old nosography are universally believed to outnumber the reasons for maintaining it.
MAFLD is defined as the presence of hepatic steatosis (detected either histologically or by imaging techniques) in those individuals who have either type 2 diabetes or obesity. Interestingly, the presence of at least two, among the following criteria: abnormal abdominal adiposity (assessed with waist circumference above the sex-specific and ethnicity-specific threshold); arterial hypertension; hypertriglyceridemia; low HDL-cholesterol; pre-diabetes; insulin resistance (HOMA-IR); and subclinical systemic inflammatory state (high-sensitivity C-Reactive Protein), is deemed to be equivalent to either obesity or diabetes. It remains unproven whether NAFLD in the diabetic patient will follow the same course as in the metabolically healthy obese. Similarly, it remains to be seen whether individuals with borderline metabolic derangements will be prone to the same risk of developing those hepatic and extra-hepatic complications that we commonly find in association with overt diabesity. From the histological point of view, NAFLD and NASH were more rigorously defined [21] than MAFLD and defining liver histology remains a milestone in our capacity to predict clinical outcomes of disease [64,65]. However, clinicians and patients will undoubtedly appreciate the possibility of diagnosing MAFLD non-invasively given the many criticisms that can be attributed to liver biopsy [44]. Whether, and to what extent, steatosis/steatohepatitis/fibrosis seen in a dysmetabolic individual is MAFLD rather than “alcoholic-and-nonalcoholic liver disease” remains uncertain [66].
The panel of experts also issued a set of diagnostic criteria to establish the diagnosis of MAFLD- related cirrhosis, so avoiding the use of the term cryptogenic cirrhosis among dysmetabolic individuals [12,13]. Given that fatty changes may disappear over time [67], the panel suggested that patients with established cirrhosis, though in the absence of histological evidence of steatohepatitis, should be considered to have MAFLD-cirrhosis if they meet at least one of the following criteria: past or present evidence of dysmetabolic traits that satisfy the criteria to diagnose MAFLD (as reported above) with at least one of the following criteria in their medical history, namely previous biopsy-proven MAFLD, or previous evidence of hepatic steatosis via imaging techniques [12,13]. In this connection, it is worth remembering the seminal study in 1999 in which Caldwell, based on his personal series of 70 cases, was the first to suggest that “NASH plays an under-recognized role in many patients with cryptogenic cirrhosis, most of whom are older, type 2 diabetic and obese females” [68].
Although probably not the ultimate answer to all unmet clinical needs, the definition of MAFLD goes one step further in the attempt to better define NAFLD patients [66]. Indeed, the name “MAFLD” progresses from a “negative” (nonalcoholic) to a “positive” (metabolic-associated) qualification of fatty liver syndromes. Moreover, it is logical to differentiate NAFLD associated with (i.e., MAFLD) or dissociated from Metabolic Syndrome (i.e., genetic NAFLD), given that either may follow different outcomes, such as extensively discussed below. Moreover, the novel definition of MAFLD utilizes the lessons learnt regarding the ominous interaction of NAFLD with Metabolic Syndrome, an association which worsens liver histology, facilitates fibrosis progression, exposes to the risk of developing HCC and decreases life expectancy of patients with NAFLD [69,70,71,72]. However, the road ahead remains long given that, for example, we still know little, if anything, regarding the impact of other determinants of disease such as sex and gender [52], gut microbiota [73], the role of hyper-ferritinemia [74,75] and of genetic polymorphisms [76].
6. The LDE Classification System
On the background of the difficulties and complexities illustrated so far, it would appear logical to be as accurately descriptive as possible in defining the hepatic features of disease, its determinants and extra-hepatic involvement. The so called LDE system classification (Figure 2) [44] is an example of how this may be accomplished in the individual patient.
Lonardo and Ballestri [44] have recently proposed the so called LDE system (Liver, Determinants and Extra-hepatic). The first section of the LDE syntax is the prefix “L” for “Liver” which identifies the key histological determinants of disease. While this section may be relatively straightforward to address based on liver histology findings, it can also be characterized noninvasively. For example, the extent of steatosis may accurately be gauged through controlled attenuation parameter (CAP) or, whenever available, Magnetic Resonance-based techniques [77,78,79]; and the stage of fibrosis with elasto-graphic techniques (based on either ultrasonography or Magnetic Resonance) or with biomarkers [80,81]. Liver inflammation may also be noninvasively evaluated with various either traditional or innovative biomarkers, the most widely available and best known being liver enzymes [80,81,82,83], although transaminases have a low sensitivity for the diagnosis of advanced NAFLD forms [84].
The central section of the LDE system is “D”, which stands for the “Determinants” of the fatty liver syndrome in the individual patient. These include, for example, sex and menopausal status; the presence of specific single nucleotide polymorphisms (SNPs) known to be associated with certain disease outcomes; and endocrine conditions deemed to facilitate the development of secondary forms of fatty liver syndromes. An exhaustive analysis of each of these determinants is beyond the scope of the present review. Moreover, recent studies have already covered the importance of sex and the endocrine system in the development and progression of NAFLD [32,85]. Here we will discuss selected studies supporting the notion that the presence of certain SNPs may affect either the natural course of NAFLD or its response to treatment.
One of the first studies suggesting that metabolic NAFLD (i.e., what we would now call MAFLD) could be different from “genetic NAFLD” was conducted by Lonardo et al. in 2006. By evaluating a small cohort of 22 individuals with NAFLD owing to familial heterozygous hypobetalipoproteinemia compared to 48 who had metabolic NAFLD and 42 healthy NAFLD-free controls, these authors found that individuals with metabolic NAFLD had higher levels of insulin resistance (as assessed with HOMA-IR) and gamma-glutamyl transferase than those in whom NAFLD was associated with familial heterozygous hypobetalipoproteinemia; this last cohort exhibited a level of insulin resistance in the same order of magnitude as found among healthy controls [86]. Bringing this further, Di Costanzo et al. accurately characterized a cohort of 83 blood donors with the mutant GG genotype (group G), 100 patients with features of the Metabolic Syndrome but the wild type CC genotype (group M), and 74 blood donors with the wild type CC genotype (controls) in the patatin-like phospholipase domain-containing 3 gene (PNPLA3). These authors found that, following adjustment for confounding factors, the median carotid intima-media thickness (a widely used marker of subclinical atherosclerosis) in group M was significantly greater than that in group G (0.84 (0.70–0.95) mm vs. 0.66 (0.55–0.74) mm; p < 0.001), and the latter was not different from that of controls (0.70 (0.64–0.81) mm) suggesting that hepatic steatosis was associated with an increased risk of subclinical carotid atherosclerosis burden only in patients with Metabolic Syndrome rather than in genetic NAFLD owing to PNPLA3 SNP [87]. Confirming this pioneer study, Käräjamäki et al. followed 249 patients with NAFLD (diagnosed based on liver ultrasonography) comprised in a large cohort of 958 middle-aged Finns for 21 years. Data have shown that Metabolic Syndrome, rather than the gene polymorphisms studied (PNPLA3 rs738409, TM6SF2 rs58542926 and MBOAT7 rs641738), predicted an increased mortality owing to either overall causes or cardiovascular diseases among NAFLD subjects [88]. As regards the risks of fibrosis progression and of developing HCC, Singal et al. have clearly shown in their meta-analytic review that PNPLA3 rs738409 confers an increased risk of advanced fibrosis in individuals in whom chronic liver disease occurs as a result of varying etiologies, notably including NAFLD. Moreover, these authors also found that PNPLA3 was associated with an increased risk of developing HCC in those with NASH [89]. Similarly, also the MBOAT7-TMC4 variant rs641738 has been found to increase the risk of HCC in NAFLD patients [90]. Pillai et al., by evaluating a large series of individuals with type 2 diabetes, of whom 1822 were treated with basal insulin peglispro and 1270 with insulin glargine, found that those with the PNPLA3 (148M/M) genotype treated with basal insulin peglispro were more prone to developing an increased intrahepatic fat content assessed with Magnetic Resonance Imaging [91]. More recently, Chen et al. have elegantly shown that PNPLA3 I148M might modify the anti-NAFLD response to exenatide based on in vitro and clinical evidence [92]. Collectively, all of the above studies support the importance of addressing the most common SNPs affecting the risk of development and progression of NAFLD [76,93].
Finally, the suffix “E” stands for “extra-hepatic” manifestations of fatty liver syndromes, the most common of which are metabolic, cardiovascular and cancer, extensively reviewed elsewhere by this group and others [94,95,96,97,98]. The extent and accuracy of the assessment which should be carried out in the individual patient to fully characterize the “E” section of the LDE system is best tailored based on careful evaluation of personal and family history.
The LDE classification system is intended to integrate and not replace the existing nomenclature in the attempt to better define the histological, pathogenic and systemic features of fatty liver syndromes, NAFLD and MAFLD, in the individual patient. This or similar accurate descriptive classification systems may facilitate the identification of more homogeneous cohorts of patients to better define the natural course of disease and responses to innovative treatment schedules.
7. Conclusions
While research on NAFLD continues to be conducted and published, we are witnessing the dawn of a new era. NAFLD, originally based on the exclusion of competing causes of liver disease (i.e., a disease defined by negation) is increasingly recognized as a truly metabolic disease (hence MAFLD, namely a positive diagnosis). This implicitly takes into account the disappearance of Hepatitis C thanks to the Direct Antiviral Agents and, therefore, the globally changing scenario of risk factors for the development of chronic liver disease [99]. However, MAFLD itself retains elements of ambiguity [66] and words of caution against the risks of prematurely abandoning the old NAFLD definition have been given by eminent experts based on uncertainties regarding definition of metabolic health and given our incomplete understanding of the molecular pathogenesis of disease [100]. This suggests that additional studies will have to ascertain whether MAFLD and NAFLD are equivalent, given that preliminary evidence suggests that NAFLD may specifically identify those individuals with more progressive disease [101] and, therefore, could be more equivalent to the notion of NASH rather than to NAFLD. Challenged by the disappointing findings of many NASH trials [10], what we need is a more accurate definition of NAFLD pathobiology in the individual patient. Proposals to better articulate the diagnosis of NAFLD/MAFLD have recently been formulated [44]. The so called LDE system addresses NAFLD features as seen from the Liver (L), the Determinants of Disease (D) and its extra-hepatic manifestations and complications (E). The LDE system is only one example of how we might better describe our patient population and it is assumed that this will help to improve the so far disappointing attempts to cure NASH. However, this prediction cannot be ascertained unless this or similar classification systems are utilized and assessed in the NAFLD/NASH research arena.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
I am grateful to Jacqueline Mole for careful editing of English.
Conflicts of Interest
The author declares no conflict of interest.
References
- Addison, T. Observations on fatty degeneration of the liver. Guys Hosp. Rep. 1836, 1, 485. [Google Scholar]
- Connor, C.L. Fatty infiltration of the liver and the development of cirrhosis in diabetes and chronic alcoholism. Am. J. Pathol. 1938, 14, 347–364. [Google Scholar] [PubMed]
- Dianzani, M.U. Sulla patogenesi dell’accumulo del grasso nella steatosi epatica. Rass. Med. Sarda 1964, 66, 67–90. [Google Scholar] [PubMed]
- Ludwig, J.; Viggiano, T.R.; McGill, D.B.; Oh, B.J. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin. Proc. 1980, 55, 434–438. [Google Scholar]
- Schaffner, F.; Thaler, H. Nonalcoholic fatty liver disease. Prog. Liver Dis. 1986, 8, 283–298. [Google Scholar]
- Suzuki, A.; Diehl, A.M. Nonalcoholic steatohepatitis. Annu. Rev. Med. 2017, 68, 85–98. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Allen, A.M.; Van Houten, H.K.; Sangaralingham, L.R.; Talwalkar, J.A.; McCoy, R.G. Healthcare cost and utilization in nonalcoholic fatty liver disease: Real-World data from a large, U.S. claims database. Hepatology 2018, 68, 2230–2238. [Google Scholar] [CrossRef] [Green Version]
- Rinella, M.E.; Sanyal, A.J. Management of NAFLD: A stage-based approach. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 196–205. [Google Scholar] [CrossRef]
- Ratziu, V.; Friedman, S.L. Why do so many NASH trials fail? Gastroenterology 2020, 18, S0016-5085(20)30680-6. [Google Scholar] [CrossRef]
- Fouad, Y.; Waked, I.; Bollipo, S.; Gomaa, A.; Ajlouni, Y.; Attia, D. What’s in a name? Renaming ‘NAFLD’ to ‘MAFLD’. Liver Int. 2020, 40, 1254–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eslam, M.; Sanyal, A.J.; George, J. International consensus panel. MAFLD: A consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Diehl, A.M.; Goodman, Z.; Ishak, K.G. Alcohollike liver disease in nonalcoholics. A clinical and histologic comparison with alcohol-induced liver injury. Gastroenterology 1988, 95, 1056–1062. [Google Scholar] [CrossRef]
- Italian Association for the Study of the Liver (AISF). AISF position paper on nonalcoholic fatty liver disease (NAFLD): Updates and future directions. Dig. Liver Dis. 2017, 49, 471–483. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef]
- Lonardo, A.; Leoni, S.; Alswat, K.A.; Fouad, Y. History of nonalcoholic fatty liver disease. Int. J. Mol Sci. 2020, 21, 5888. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Targher, G.; Lonardo, A. Ultrasonographic fatty liver indicator detects mild steatosis and correlates with metabolic/histological parameters in various liver diseases. Metabolism 2017, 72, 57–65. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Lugari, S.; Lonardo, A.; Francica, G. A critical appraisal of the use of ultrasound in hepatic steatosis. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 667–681. [Google Scholar] [CrossRef]
- Nascimbeni, F.; Ballestri, S.; Machado, M.V.; Mantovani, A.; Cortez-Pinto, H.; Targher, G.; Lonardo, A. Clinical relevance of liver histopathology and different histological classifications of NASH in adults. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 351–367. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Allen, A.M.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Loomba, R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: A systematic review and meta-analysis of paired-biopsy studies. Clin. Gastroenterol. Hepatol. 2015, 13, 643–654.e1-9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunt, E.M. Nonalcoholic fatty liver disease: Pros and cons of histologic systems of evaluation. Int. J. Mol. Sci. 2016, 17, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunt, E.M. Nonalcoholic fatty liver disease and the ongoing role of liver biopsy evaluation. Hepatol. Commun. 2017, 1, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Koch, L.K.; Yeh, M.M. Nonalcoholic fatty liver disease (NAFLD): Diagnosis, pitfalls, and staging. Ann. Diagn. Pathol. 2018, 37, 83–90. [Google Scholar] [CrossRef]
- Aizawa, Y.; Hokari, A. Autoimmune hepatitis: Current challenges and future prospects. Clin. Exp. Gastroenterol. 2017, 10, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Paschos, P.; Paletas, K. Non alcoholic fatty liver disease and metabolic syndrome. Hippokratia 2009, 13, 9–19. [Google Scholar]
- Lonardo, A.; Ballestri, S.; Marchesini, G.; Angulo, P.; Loria, P. Nonalcoholic fatty liver disease: A precursor of the metabolic syndrome. Dig. Liver Dis. 2015, 47, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Ballestri, S.; Zona, S.; Targher, G.; Romagnoli, D.; Baldelli, E.; Nascimbeni, F.; Roverato, A.; Guaraldi, G.; Lonardo, A. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 936–944. [Google Scholar] [CrossRef]
- Angulo, P. Nonalcoholic fatty liver disease. N. Engl. J. Med. 2002, 346, 1221–1231. [Google Scholar] [CrossRef] [Green Version]
- Guaraldi, G.; Lonardo, A.; Ballestri, S.; Zona, S.; Stentarelli, C.; Orlando, G.; Carli, F.; Carulli, L.; Roverato, A.; Loria, P. Human immunodeficiency virus is the major determinant of steatosis and hepatitis C virus of insulin resistance in virus-associated fatty liver disease. Arch. Med. Res. 2011, 42, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. NAFLD in some common endocrine diseases: Prevalence, pathophysiology, and principles of diagnosis and management. Int. J. Mol. Sci. 2019, 20, 2841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vodkin, I.; Valasek, M.A.; Bettencourt, R.; Cachay, E.; Loomba, R. Clinical, biochemical and histological differences between HIV-associated NAFLD and primary NAFLD: A case-control study. Aliment. Pharmacol. Ther. 2015, 41, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Ballestri, S.; Mantovani, A.; Nascimbeni, F.; Lugari, S.; Targher, G. Pathogenesis of hypothyroidism-induced NAFLD: Evidence for a distinct disease entity? Dig. Liver Dis. 2019, 51, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Blissett, D.; Blissett, R.; Henry, L.; Stepanova, M.; Younossi, Y.; Racila, A.; Hunt, S.; Beckerman, R. The economic and clinical burden of nonalcoholic fatty liver disease in the United States and Europe. Hepatology 2016, 64, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [CrossRef]
- Matsuzawa, Y. Obesity and metabolic syndrome: The contribution of visceral fat and Adiponectin. Diabetes Manag. 2014, 4, 391–401. [Google Scholar] [CrossRef]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottière, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. IARC working group on energy balance and obesity. Energy balance and obesity: What are the main drivers? Cancer Causes Control 2017, 28, 247–258. [Google Scholar] [CrossRef] [Green Version]
- Ziki, A.; Mani, A. Metabolic syndrome: Genetic insights into disease pathogenesis. Curr. Opin. Lipidol. 2016, 27, 162–171. [Google Scholar] [CrossRef]
- Roberts, C.K.; Hevener, A.L.; Barnard, R.J. Metabolic syndrome and insulin resistance: Underlying causes and modification by exercise training. Compr. Physiol. 2013, 3, 1–58. [Google Scholar]
- Lonardo, A.; Carani, C.; Carulli, N.; Loria, P. Chicken or egg turned into head or belly. J. Hepatol. 2006, 45, 454–456. [Google Scholar] [CrossRef]
- Kullmann, S.; Valenta, V.; Wagner, R.; Tschritter, O.; Machann, J.; Häring, H.U.; Preissl, H.; Fritsche, A.; Heni, M. Brain insulin sensitivity is linked to adiposity and body fat distribution. Nat. Commun. 2020, 11, 1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, E.M.; Grant, P.J. Neel revisited: The adipocyte, seasonality and type 2 diabetes. Diabetologia 2006, 49, 1462–1466. [Google Scholar] [CrossRef] [Green Version]
- Lonardo, A.; Ballestri, S. Perspectives of nonalcoholic fatty liver disease research: A personal point of view. Explor. Med. 2020, 1. [Google Scholar] [CrossRef]
- Binetti, J.; Bertran, L.; Riesco, D.; Aguilar, C.; Martínez, S.; Sabench, F.; Porras, J.A.; Camaron, J.; Del Castillo, D.; Richart, C.; et al. Deregulated serotonin pathway in women with morbid obesity and NAFLD. Life 2020, 10, 245. [Google Scholar] [CrossRef]
- Soto-Angona, O.; Anmella, G.; Valdés-Florido, M.J.; De Uribe-Viloria, N.; Carvalho, A.F.; Penninx, J.H.; Berk, M. Non-Alcoholic fatty liver disease (NAFLD) as a neglected metabolic companion of psychiatric disorders: Common pathways and future approaches. BMC Med. 2020, 18, 261. [Google Scholar] [CrossRef]
- Boudreau, D.M.; Malone, D.C.; Raebel, M.A.; Fishman, P.A.; Nichols, G.A.; Feldstein, A.C.; Boscoe, A.N.; Ben-Joseph, R.H.; Magid, D.J.; Okamoto, L.J. Health care utilization and costs by metabolic syndrome risk factors. Metab. Syndr. Relat. Disord. 2009, 7, 305–314. [Google Scholar] [CrossRef]
- Wainwright, P.; Byrne, C.D. Bidirectional relationships and disconnects between NAFLD and features of the metabolic syndrome. Int. J. Mol. Sci. 2016, 17, 367. [Google Scholar] [CrossRef] [Green Version]
- Lonardo, A.; Bellentani, S.; Ratziu, V.; Loria, P. Insulin resistance in nonalcoholic steatohepatitis: Necessary but not Sufficient—Death of a dogma from analysis of therapeutic studies? Expert Rev. Gastroenterol. Hepatol. 2011, 5, 279–289. [Google Scholar] [CrossRef]
- Yilmaz, Y. NAFLD in the absence of metabolic syndrome: Different epidemiology, pathogenetic mechanisms, risk factors for disease progression? Semin. Liver Dis. 2012, 32, 14–21. [Google Scholar] [CrossRef]
- Chen, F.; Esmaili, S.; Rogers, G.B.; Bugianesi, E.; Petta, S.; Marchesini, G.; Bayoumi, A.; Metwally, M.; Azardaryany, M.K.; Coulter, S.; et al. Lean NAFLD: A distinct entity shaped by differential metabolic adaptation. Hepatology 2020, 71, 1213–1227. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Suzuki, A. Sexual dimorphism of NAFLD in adults. focus on clinical aspects and implications for practice and translational research. J. Clin. Med. 2020, 9, 1278. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Ballestri, S.; Chow, P.K.H.; Suzuki, A. Sex disparity in hepatocellular carcinoma owing to NAFLD and non-NAFLD etiology. Epidemiological findings and patho-mechanisms. Hepatoma Res. 2020, 6, 83. [Google Scholar]
- Pradhan, A.D. Sex differences in the metabolic syndrome: Implications for cardiovascular health in women. Clin. Chem. 2014, 60, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Mauvais-Jarvis, F.; Merz, N.B.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Bellentani, S.; Tiribelli, C. Is it time to change NAFLD and NASH nomenclature? Lancet Gastroenterol. Hepatol. 2017, 2, 547–548. [Google Scholar] [CrossRef]
- Harrison, S.A.; Abdelmalek, M.F.; Caldwell, S.; Shiffman, M.L.; Diehl, A.M.; Ghalib, R.; Lawitz, E.J.; Rockey, D.C.; Schall, R.A.; Jia, C.; et al. GS-US-321-0105 and GS-US-321-0106 investigators. Simtuzumab is ineffective for patients with bridging fibrosis or compensated cirrhosis caused by nonalcoholic steatohepatitis. Gastroenterology 2018, 155, 1140–1153. [Google Scholar] [CrossRef]
- Harrison, S.A.; Wong, V.W.; Okanoue, T.; Bzowej, N.; Vuppalanchi, R.; Younes, Z.; Kohli, A.; Sarin, S.; Caldwell, S.H.; Alkhouri, N.; et al. Selonsertib for patients with bridging fibrosis or compensated cirrhosis due to NASH: Results from randomized phase III STELLAR trials. J. Hepatol. 2020, 73, 26–39. [Google Scholar] [CrossRef]
- Harrison, S.A.; Goodman, Z.; Jabbar, A.; Vemulapalli, R.; Younes, Z.H.; Freilich, B.; Sheikh, M.Y.; Schattenberg, J.M.; Kayali, Z.; Zivony, A.; et al. A randomized, placebo-controlled trial of emricasan in patients with NASH and F1-F3 fibrosis. J. Hepatol. 2020, 72, 816–827. [Google Scholar] [CrossRef]
- Harrison, S.A.; Alkhouri, N.; Davison, B.A.; Sanyal, A.; Edwards, C.; Colca, J.R.; Lee, B.H.; Loomba, R.; Cusi, K.; Kolterman, O.; et al. Insulin sensitizer MSDC-0602K in non-alcoholic steatohepatitis: A randomized, double-blind, placebo-controlled phase IIb study. J. Hepatol. 2020, 72, 613–626. [Google Scholar] [CrossRef]
- Rinella, M.E.; Tacke, F.; Sanyal, A.J.; Anstee, Q.M. Participants of the AASLD/EASL workshop. Report on the AASLD/EASL joint workshop on clinical trial endpoints in NAFLD. J. Hepatol. 2019, 71, 823–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez-Sanchez, N.; Arrese, M.; Gadano, A.; Oliveira, C.P.; Fassio, E.; Arab, J.P.; Chávez-Tapia, N.C.; Dirchwolf, M.; Torre, A.; Ridruejo, E.; et al. The Latin American association for the study of the liver (ALEH) position statement on the redefinition of fatty liver disease. Lancet Gastroenterol. Hepatol. 2021, 6, 65–72. [Google Scholar] [CrossRef]
- Shiha, G.; Alswat, K.; Al Khatry, M.; Sharara, A.I.; Örmeci, N.; Waked, I.; Benazzouz, M.; Al-Ali, F.; Hamed, A.E.; Hamoudi, W.; et al. Nomenclature and definition of metabolic-associated fatty liver disease: A consensus from the Middle East and north Africa. Lancet Gastroenterol. Hepatol. 2021, 6, 57–64. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Calzadilla-Bertot, L.; Wai-Sun Wong, V.; Castellanos, M.; Aller-de la Fuente, R.; Metwally, M.; Eslam, M.; Gonzalez-Fabian, L.; Alvarez-Quiñones Sanz, M.; Conde-Martin, A.F.; et al. Fibrosis Severity as a Determinant of Cause-Specific Mortality in Patients with Advanced Nonalcoholic Fatty Liver Disease: A Multi-National Cohort Study. Gastroenterology 2018, 155, 443–457. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Maurantonio, M.; Marrazzo, A.; Rinaldi, L.; Adinolfi, L.E. Nonalcoholic fatty liver disease: Evolving paradigms. World J. Gastroenterol. 2017, 23, 6571–6592. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kang, E.S.; Tsochatzis, E.A.; Kechagias, S.; Ekstedt, M.; Xanthakos, S.; Lonardo, A.; Mantovani, A.; Tilg, H.; Côté, I.; et al. Commentary: Nonalcoholic or metabolic dysfunction-associated fatty liver disease? The epidemic of the 21st century in search of the most appropriate name. Metabolism 2020, 113, 154413. [Google Scholar] [CrossRef]
- van der Poorten, D.; Samer, C.F.; Ramezani-Moghadam, M.; Coulter, S.; Kacevska, M.; Schrijnders, D.; Wu, L.E.; McLeod, D.; Bugianesi, E.; Komuta, M.; et al. Hepatic fat loss in advanced nonalcoholic steatohepatitis: Are alterations in serum adiponectin the cause? Hepatology 2013, 57, 2180–2188. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, S.H.; Oelsner, D.H.; Iezzoni, J.C.; Hespenheide, E.E.; Battle, E.H.; Driscoll, C.J. Cryptogenic cirrhosis: Clinical characterization and risk factors for underlying disease. Hepatology 1999, 29, 664–669. [Google Scholar] [CrossRef]
- Kang, H.; Greenson, J.K.; Omo, J.T.; Chao, C.; Peterman, D.; Anderson, L.; Foess-Wood, L.; Sherbondy, M.A.; Conjeevaram, H.S. Metabolic syndrome is associated with greater histologic severity, higher carbohydrate, and lower fat diet in patients with NAFLD. Am. J. Gastroenterol. 2006, 101, 2247–2253. [Google Scholar] [CrossRef] [Green Version]
- Francque, S.; De Maeght, S.; Adler, M.; Deltenre, P.; de Galocsy, C.; Orlent, H.; Van Steenbergen, W.; Bastens, B.; Wain, E.; Langlet, P.; et al. High prevalence of advanced fibrosis in association with the metabolic syndrome in a Belgian prospective cohort of NAFLD patients with elevated ALT. Results of the Belgian NAFLD registry. Acta Gastroenterol. Belg. 2011, 74, 9–16. [Google Scholar]
- Negro, F. Natural history of NASH and HCC. Liver Int. 2020, 40 (Suppl. 1), 72–76. [Google Scholar] [CrossRef] [Green Version]
- Golabi, P.; Otgonsuren, M.; de Avila, L.; Sayiner, M.; Rafiq, N.; Younossi, Z.M. Components of metabolic syndrome increase the risk of mortality in nonalcoholic fatty liver disease (NAFLD). Medicine (Baltimore) 2018, 97, e0214. [Google Scholar] [CrossRef] [PubMed]
- Aron-Wisnewsky, J.; Vigliotti, C.; Witjes, J.; Le, P.; Holleboom, A.G.; Verheij, J.; Nieuwdorp, M.; Clément, K. Gut microbiota and human NAFLD: Disentangling microbial signatures from metabolic disorders. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 279–297. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Halpern, Z.; Oren, R. NAFLD and hyperinsulinemia are major determinants of serum ferritin levels. J. Hepatol. 2007, 46, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Trombini, P.; Piperno, A. Ferritin, metabolic syndrome and NAFLD: Elective attractions and dangerous liaisons. J. Hepatol. 2007, 46, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; George, J. Genetic contributions to NAFLD: Leveraging shared genetics to uncover systems biology. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 40–52. [Google Scholar] [CrossRef]
- Pu, K.; Wang, Y.; Bai, S.; Wei, H.; Zhou, Y.; Fan, J.; Qiao, L. Diagnostic accuracy of controlled attenuation parameter (CAP) as a non-invasive test for steatosis in suspected non-alcoholic fatty liver disease: A systematic review and meta-analysis. BMC Gastroenterol. 2019, 19, 51. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.J.; Kim, S.U. Noninvasive monitoring of hepatic steatosis: Controlled attenuation parameter and magnetic resonance imaging-proton density fat fraction in patients with nonalcoholic fatty liver disease. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 523–530. [Google Scholar] [CrossRef]
- Han, M.A.; Saouaf, R.; Ayoub, W.; Todo, T.; Mena, E.; Noureddin, M. Magnetic resonance imaging and transient elastography in the management of nonalcoholic fatty liver disease (NAFLD). Expert Rev. Clin. Pharmacol. 2017, 10, 379–390. [Google Scholar] [CrossRef]
- Wong, V.W.; Adams, L.A.; de Lédinghen, V.; Wong, G.L.; Sookoian, S. Noninvasive biomarkers in NAFLD and NASH-current progress and future promise. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 461–478. [Google Scholar] [CrossRef]
- Ballestri, S.; Mantovani, A.; Baldelli, E.; Lugari, S.; Maurantonio, M.; Nascimbeni, F.; Marrazzo, A.; Romagnoli, D.; Targher, G.; Lonardo, A. Liver fibrosis biomarkers accurately exclude advanced fibrosis and are associated with higher cardiovascular risk scores in patients with NAFLD or viral chronic liver disease. Diagnostics 2021, 11, 98. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, M.; Assoumou, L.; De Wit, S.; Girard, P.M.; Valantin, M.A.; Katlama, C.; Necsoi, C.; Campa, P.; Huefner, A.D.; Wiesch, S.Z.J.; et al. Diagnostic accuracy of noninvasive markers of steatosis, NASH, and liver fibrosis in HIV-monoinfected individuals at risk of nonalcoholic fatty liver disease (NAFLD): Results from the ECHAM study. J. Acquir. Immune Defic. Syndr. 2019, 80, e86–e94. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.; Neuschwander-Tetri, B.A.; Kleiner, D.E.; Schabel, E.; Rinella, M.; Harrison, S.; Ratziu, V.; Sanyal, A.J.; Loomba, R.; Megnien, J.S.; et al. Liver forum case definitions working group. Defining improvement in nonalcoholic steatohepatitis for treatment trial endpoints: Recommendations from the liver forum. Hepatology 2019, 70, 1841–1855. [Google Scholar] [CrossRef] [PubMed]
- Mofrad, P.; Contos, M.J.; Haque, M.; Sargeant, C.; Fisher, R.A.; Luketic, V.A.; Sterling, R.K.; Shiffman, M.L.; Stravitz, R.T.; Sanyal, A.J. Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology 2003, 37, 1286–1292. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, M.; Patel, P.; Dunn-Valadez, S.; Dao, C.; Khan, V.; Ali, H.; El-Serag, L.; Hernaez, R.; Sisson, A.; Thrift, A.P.; et al. Women have a lower risk of nonalcoholic fatty liver disease but a higher risk of progression vs men: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 61–71.e15. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Lombardini, S.; Scaglioni, F.; Carulli, L.; Ricchi, M.; Ganazzi, D.; Adinolfi, L.E.; Ruggiero, G.; Carulli, N.; Loria, P. Hepatic steatosis and insulin resistance: Does etiology make a difference? J. Hepatol. 2006, 44, 90–96. [Google Scholar] [CrossRef]
- Di Costanzo, A.; D’Erasmo, L.; Polimeni, L.; Baratta, F.; Coletta, P.; Di Martino, M.; Loffredo, L.; Perri, L.; Ceci, F.; Montali, A.; et al. Non-Alcoholic fatty liver disease and subclinical atherosclerosis: A comparison of metabolically-versus genetically-driven excess fat hepatic storage. Atherosclerosis 2017, 257, 232–239. [Google Scholar] [CrossRef]
- Käräjämäki, A.J.; Hukkanen, J.; Kauma, H.; Kesäniemi, Y.A.; Ukkola, O. Metabolic syndrome but not genetic polymorphisms known to induce NAFLD predicts increased total mortality in subjects with NAFLD (OPERA study). Scand. J. Clin. Lab. Investig. 2020, 80, 106–113. [Google Scholar] [CrossRef]
- Singal, A.G.; Manjunath, H.; Yopp, A.C.; Beg, M.S.; Marrero, J.A.; Gopal, P.; Waljee, A.K. The effect of PNPLA3 on fibrosis progression and development of hepatocellular carcinoma: A meta-analysis. Am. J. Gastroenterol. 2014, 109, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Donati, B.; Dongiovanni, P.; Romeo, S.; Meroni, M.; McCain, M.; Miele, L.; Petta, S.; Maier, S.; Rosso, C.; De Luca, L.; et al. MBOAT7 rs641738 variant and hepatocellular carcinoma in non-cirrhotic individuals. Sci. Rep. 2017, 7, 4492. [Google Scholar] [CrossRef] [Green Version]
- Pillai, S.; Duvvuru, S.; Bhatnagar, P.; Foster, W.; Farmen, M.; Shankar, S.; Harris, C.; Bastyr, E., 3rd; Hoogwerf, B.; Haupt, A. The PNPLA3 I148M variant is associated with transaminase elevations in type 2 diabetes patients treated with basal insulin peglispro. Pharmacogenom. J. 2018, 18, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yan, X.; Xu, X.; Yuan, S.; Xu, F.; Liang, H. PNPLA3 I148M is involved in the variability in anti-NAFLD response to exenatide. Endocrine 2020, 70, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Trépo, E.; Valenti, L. Update on NAFLD genetics: From new variants to the clinic. J. Hepatol. 2020, 72, 1196–1209. [Google Scholar] [CrossRef] [PubMed]
- Ballestri, S.; Mantovani, A.; Nascimbeni, F.; Lugari, S.; Lonardo, A. Extra-Hepatic manifestations and complications of nonalcoholic fatty liver disease. Future Med. Chem. 2019, 11, 2171–2192. [Google Scholar] [CrossRef]
- Rosato, V.; Masarone, M.; Dallio, M.; Federico, A.; Aglitti, A.; Persico, M. NAFLD and extra-hepatic comorbidities: Current evidence on a multi-organ metabolic syndrome. Int. J. Environ. Res. Public Health 2019, 16, 3415. [Google Scholar] [CrossRef] [Green Version]
- Velasco, V.-R.J.A.; García-Jiménez, E.S.; García-Zermeño, K.R.; Morel-Cerda, E.C.; Aldana-Ledesma, J.M.; Castro-Narro, G.E.; Cerpa-Cruz, S.; Tapia-Calderón, D.K.; Mercado-Jauregui, L.A.; Contreras-Omaña, R. Extrahepatic complications of non-alcoholic fatty liver disease: Its impact beyond the liver. Rev. Gastroenterol. Mex. 2019, 84, 472–481. [Google Scholar]
- Chacko, K.R.; Reinus, J. Extrahepatic complications of nonalcoholic fatty liver disease. Clin. Liver Dis. 2016, 20, 387–401. [Google Scholar] [CrossRef]
- Vanni, E.; Marengo, A.; Mezzabotta, L.; Bugianesi, E. Systemic complications of nonalcoholic fatty liver disease: When the liver is not an innocent bystander. Semin. Liver Dis. 2015, 35, 236–249. [Google Scholar] [CrossRef]
- Terrault, N.A.; Pageaux, G.P. A changing landscape of liver transplantation: King HCV is dethroned, ALD and NAFLD take over! J. Hepatol. 2018, 69, 767–768. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Rinella, M.E.; Sanyal, A.; Harrison, S.A.; Brunt, E.; Goodman, Z.; Cohen, D.E.; Loomba, R. From NAFLD to MAFLD: Implications of a premature change in terminology. Hepatology 2020. [Google Scholar] [CrossRef]
- Lin, S.; Huang, J.; Wang, M.; Kumar, R.; Liu, Y.; Liu, S.; Wu, Y.; Wang, X.; Zhu, Y. Comparison of MAFLD and NAFLD diagnostic criteria in real world. Liver Int. 2020, 40, 2082–2089. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sex disparity in pathobiology, epidemiology and clinical features of HCC (reprinted from [53]).
Figure 1.
Sex disparity in pathobiology, epidemiology and clinical features of HCC (reprinted from [53]).

Figure 2.
Articulating the taxonomy of nonalcoholic fatty liver disease (NAFLD)/metabolic-associated fatty liver disease (MAFLD) with the LDE system. This schematic figure illustrates the proposed high standard of accuracy in defining NAFLD/MAFLD cases to be recruited for trials of innovative treatment, as well as for a better prediction of the natural course of disease in the individual patient. In its essence, the system requires clarification of nine criteria that should be recorded to better characterize cohorts of patients recruited in randomized controlled trials.
Figure 2.
Articulating the taxonomy of nonalcoholic fatty liver disease (NAFLD)/metabolic-associated fatty liver disease (MAFLD) with the LDE system. This schematic figure illustrates the proposed high standard of accuracy in defining NAFLD/MAFLD cases to be recruited for trials of innovative treatment, as well as for a better prediction of the natural course of disease in the individual patient. In its essence, the system requires clarification of nine criteria that should be recorded to better characterize cohorts of patients recruited in randomized controlled trials.


{kind=link}
{kind=link}
| PRIMARY NAFLD | ||
| Associated with/predisposing to incident Metabolic Syndrome | ||
| SECONDARY NAFLD | ||
| Nutritional Disorders | ||
| total parenteral nutrition, acute starvation | ||
| Abdominal Surgery | ||
| extensive small bowel resection bilio-pancreatic diversionjejunal bypass | ||
| Drug-Induced | ||
| diltiazem, aspirin, methotrexate, highly active antiretroviral therapy (stavudine and zidovudine) | ||
| Occupational exposure to organic solvents | ||
| (Rare) Metabolic Disorders | Hypobetalipoproteinemia, Lipodystrophy, Weber-Christian syndrome, Acute fatty liver of pregnancy, Reyes syndrome and Mauriac syndrome | |
| VAFLD | ||
| HIV, HCV | ||
| Common Endocrine Disorders | ||
| Hypothyroidism, hypogonadism in either sex, GH deficiency, PCOS | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lonardo, A. Renaming NAFLD to MAFLD: Could the LDE System Assist in This Transition? J. Clin. Med. 2021, 10, 492. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030492
AMA Style
Lonardo A. Renaming NAFLD to MAFLD: Could the LDE System Assist in This Transition? Journal of Clinical Medicine. 2021; 10(3):492. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030492
Chicago/Turabian StyleLonardo, Amedeo. 2021. "Renaming NAFLD to MAFLD: Could the LDE System Assist in This Transition?" Journal of Clinical Medicine 10, no. 3: 492. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10030492
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.