
Is There an Association between Sleep Disorders and Diabetic Foot? A Scoping Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search and Sources
2.2. Eligibility Criteria
2.3. Selection of Studies
2.4. Data Extraction and Synthesis of Results
3. Results
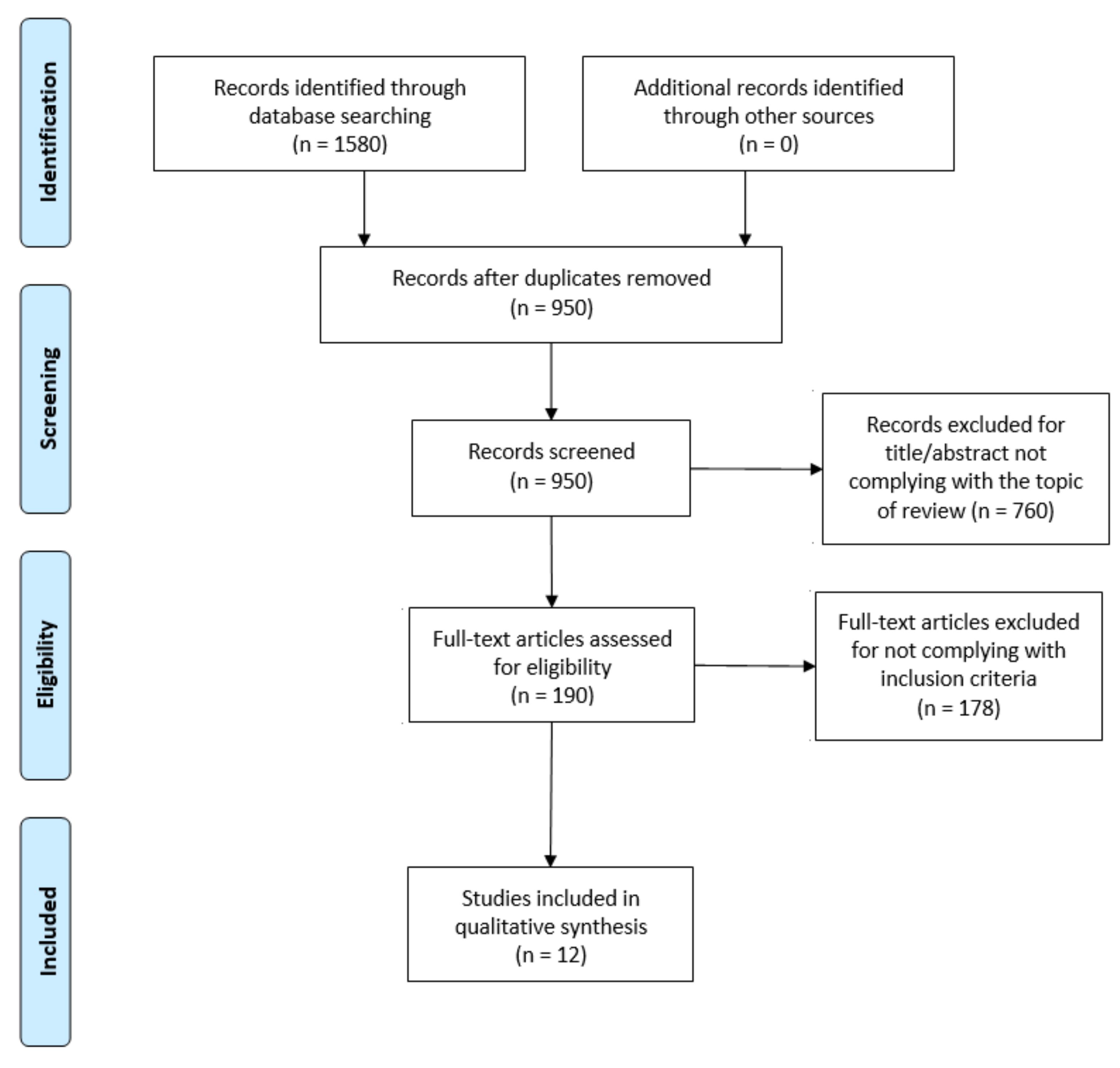
3.1. Selection of Studies
3.2. Data Extraction and Synthesis of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Harding, J.L.; Pavkov, M.E.; Magliano, D.J.; Shaw, J.E.; Gregg, E.W. Global trends in diabetes complications: A review of current evidence. Diabetologia 2019, 62, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Apelqvist, J. Diagnostics and treatment of the diabetic foot. Endocrine 2012, 41, 384–397. [Google Scholar] [CrossRef]
- Jia, L.; Parker, C.; Parker, T.J.; Kinnear, E.M.; Derhy, P.H.; Alvarado, A.M.; Huygens, F.; Lazzarini, P.A. Incidence and risk factors for developing infection in patients presenting with uninfected diabetic foot ulcers. PLoS ONE 2017, 12, e0177916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowry, D.; Saeed, M.; Narendran, P.; Tiwari, A. The Difference between the Healing and the Nonhealing Diabetic Foot Ulcer: A Review of the Role of the Microcirculation. J. Diabetes Sci. Technol. 2016, 11, 914–923. [Google Scholar] [CrossRef]
- Amin, N.; Doupis, J. Diabetic foot disease: From the evaluation of the “foot at risk” to the novel diabetic ulcer treatment mo-dalities. World J. Diabetes 2016, 7, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Jupiter, D.C.; Thorud, J.C.; Buckley, C.J.; Shibuya, N. The impact of foot ulceration and amputation on mortality in diabetic patients. I: From ulceration to death, a systematic review. Int. Wound J. 2016, 13, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Prompers, L.; Huijberts, M.; Schaper, N.; Apelqvist, J.; Bakker, K.; Edmonds, M.; Holstein, P.; Jude, E.; Jirkovska, A.; Mauricio, D.; et al. Resource utilisation and costs associated with the treatment of diabetic foot ulcers. Prospective data from the Eurodiale Study. Diabetologia 2008, 51, 1826–1834. [Google Scholar] [CrossRef]
- Vileikyte, L. Diabetic foot ulcers: A quality of life issue. Diabetes Metab. Res. Rev. 2001, 17, 246–249. [Google Scholar] [CrossRef]
- Udovichenko, O.V.; Maximova, N.V.; Amosova, M.V.; Yunilaynen, O.A.; Berseneva, E.A.; Starostina, E.G. Prevalence and Prognostic Value of Depression and Anxiety in Patients with Diabetic Foot Ulcers and Possibilities of their Treatment. Curr. Diabetes Rev. 2017, 13, 97–106. [Google Scholar] [CrossRef]
- Sibbald, R.G.; Armstrong, D.G.; Orsted, H.L. Pain in diabetic foot ulcers. Ostomy Wound Manag. 2003, 49, 24–29. [Google Scholar]
- Kaur, S.; Pandhi, P.; Dutta, P. Painful diabetic neuropathy: An update. Ann. Neurosci. 2011, 18, 168–175. [Google Scholar] [CrossRef]
- Clark, R.L.; Bowling, F.L.; Jepson, F.; Rajbhandari, S. Phantom limb pain after amputation in diabetic patients does not differ from that after amputation in nondiabetic patients. Pain 2013, 154, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leggett, A.; Assari, S.; Burgard, S.; Zivin, K. The effect of sleep disturbance on the association between chronic medical conditions and depressive symptoms over time. Longitud. Life Course Stud. 2017, 8, 138–151. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.R. Why Sleep Is Important for Health: A Psychoneuroimmunology Perspective. Annu. Rev. Psychol. 2015, 66, 143–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, B.-Q.; Li, X.-M.; Wang, D.; Yu, X.-F. Sleep quality and its impact on glycaemic control in patients with type 2 diabetes mellitus. Int. J. Nurs. Sci. 2014, 1, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, N.; Takatsuka, N.; Shimizu, H. Sleep disturbance and onset of type 2 diabetes. Diabetes Care 2004, 27, 282–283. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Vas, P.R.J.; Ahluwalia, R.; Manas, A.B.; Manu, C.; Kavarthapu, V.; Edmonds, M.E. Undiagnosed severe sleep apnoea and diabetic foot ulceration—A case series based hypothesis: A hitherto under emphasized factor in failure to heal. Diabet. Med. 2016, 33, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Adderley, N.J.; Tracy, A.; Taverner, T.; Hanif, W.; Toulis, K.A.; Thomas, G.N.; Tahrani, A.A.; Nirantharakumar, K. Risk of Incident Obstructive Sleep Apnea Among Patients with Type 2 Diabetes. Diabetes Care 2019, 42, 954–963. [Google Scholar] [CrossRef] [Green Version]
- Andruškienė, J.; Podlipskytė, A.; Martinkėnas, A.; Varoneckas, G. Depressive mood in association with sociodemographic, be-havioral, self-perceived health, and coronary artery disease risk factors and sleep complaints. Medicina 2013, 49, 372–378. [Google Scholar] [CrossRef]
- Nair, H.K. Microcurrent as an adjunct therapy to accelerate chronic wound healing and reduce patient pain. J. Wound Care 2018, 27, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Haveleia, A.; Gayatri, D. Sleep quality and the affecting factors in patients with diabetic ulcer. Enferm. Clín. 2019, 29, 70–75. [Google Scholar] [CrossRef]
- Altaf, Q.-A.A.; Ali, A.; Piya, M.K.; Raymond, N.T.; Tahrani, A.A. The relationship between obstructive sleep apnea and intra-epidermal nerve fiber density, PARP activation and foot ulceration in patients with type 2 diabetes. J. Diabetes Its Complicat. 2016, 30, 1315–1320. [Google Scholar] [CrossRef] [Green Version]
- Bener, A.; Al-Hamaq, A.O.; Abdulhadi, K.; Salahaldin, A.H.; Gansan, L. Interaction between diabetes mellitus and hypertension on risk of hearing loss in highly endogamous population. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S45–S51. [Google Scholar] [CrossRef] [PubMed]
- Puspita, A.D.; Gayatri, D.; Pujasari, H. Sleep quality in diabetic mellitus with diabetic foot ulcer. In AIP Conference Proceedings; AIP Publishing: Melville, NY, USA, 2019; Volume 2092, p. 040009. [Google Scholar]
- Sheahan, H.; Canning, K.; Refausse, N.; Kinnear, E.M.; Jorgensen, G.; Walsh, J.R.; Lazzarini, P. Differences in the daily activity of patients with diabetic foot ulcers compared to controls in their free-living environments. Int. Wound J. 2017, 14, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Maltese, G.; Fountoulakis, N.; Drakatos, P.; Shah, D.; Patel, K.; Sharma, A.; Thomas, S.; Pengo, M.; Karalliedde, J. Elevated obstructive sleep apnoea risk score is associated with poor healing of diabetic foot ulcers: A prospective cohort study. Diabet. Med. 2018, 35, 1494–1498. [Google Scholar] [CrossRef]
- Rutkove, S.B.; Veves, A.; Mitsa, T.; Nie, R.; Fogerson, P.M.; Garmirian, L.P.; Nardin, R.A. Impaired Distal Thermoregulation in Diabetes and Diabetic Polyneuropathy. Diabetes Care 2009, 32, 671–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salomé, G.M.; de Souza Pellegrino, D.M.; Blanes, L.; Ferreira, L.M. Sleep Quality in Patients with Diabetic Foot Ulcers. Wounds 2013, 25, 20–27. [Google Scholar]
- Mannarino, M.R.; Di, F.F.; Pirro, M. Obstructive sleep apnea syndrome. Eur. J. Intern. Med. 2012, 23, 586. [Google Scholar] [CrossRef] [PubMed]
- Drager, L.F.; Togeiro, S.M.; Polotsky, V.Y.; Lorenzi-Filho, G. Obstructive sleep apnea: A cardiometabolic risk in obesity and the metabolic syndrome. J. Am. Coll. Cardiol. 2013, 62, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Oyama, J.-I.; Yamamoto, H.; Maeda, T.; Ito, A.; Node, K.; Makino, N. Continuous Positive Airway Pressure Therapy Improves Vascular Dysfunction and Decreases Oxidative Stress in Patients with the Metabolic Syndrome and Obstructive Sleep Apnea Syndrome. Clin. Cardiol. 2012, 35, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Ferini-Strambi, L.; Baietto, C.; Di Gioia, M.; Castaldi, P.; Castronovo, C.; Zucconi, M.; Cappa, S. Cognitive dysfunction in patients with obstructive sleep apnea (OSA): Partial reversibility after continuous positive airway pressure (CPAP). Brain Res. Bull. 2003, 61, 87–92. [Google Scholar] [CrossRef]
- Reichmuth, K.J.; Austin, D.; Skatrud, J.B.; Young, T. Association of sleep apnea and type II diabetes: A population-based study. Am. J. Respir. Crit. Care Med. 2005, 172, 1590. [Google Scholar] [CrossRef] [Green Version]
- Garvey, J.F.; Taylor, C.T.; McNicholas, W.T. Cardiovascular disease in obstructive sleep apnoea syndrome: The role of intermittent hypoxia and inflammation. Eur. Respir. J. 2009, 33, 1195–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahrani, A.A.; Ali, A.; Raymond, N.T.; Begum, S.; Dubb, K.; Mughal, S.; Jose, B.; Piya, M.K.; Barnett, A.H.; Stevens, M.J. Obstructive sleep apnea and diabetic neuropathy: A novel association in patients with type 2 diabetes. Diabetes Care 2012, 186, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Paiva, T.; Attarian, H. Obstructive sleep apnea and other sleep-related syndromes. Handb. Clin. Neurol. 2014, 119, 251–271. [Google Scholar] [CrossRef]
- Nagappa, M.; Liao, P.; Wong, J.; Auckley, D.; Ramachandran, S.K.; Memtsoudis, S.G.; Mokhlesi, B.; Chung, F. Validation of the STOP-Bang Questionnaire as a Screening Tool for Obstructive Sleep Apnea among Different Populations: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0143697. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test–retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]
- Yagihashi, S.; Mizukami, H.; Sugimoto, K. Mechanism of diabetic neuropathy: Where are we now and where to go? J. Diabetes Investig. 2010, 2, 18–32. [Google Scholar] [CrossRef] [Green Version]
- Sridhar, G.; Madhu, K. Prevalence of sleep disturbances in diabetes mellitus. Diabetes Res. Clin. Pract. 1994, 23, 183–186. [Google Scholar] [CrossRef]
- Murphy, M.J.; Peterson, M.J. Sleep Disturbances in Depression. Sleep Med. Clin. 2015, 10, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Nutt, D.; Wilson, S.; Paterson, L. Sleep disorders as core symptoms of depression. Dialogues Clin. Neurosci. 2008, 10, 329–336. [Google Scholar] [PubMed]
- Reutrakul, S.; Mokhlesi, B. Obstructive Sleep Apnea and Diabetes: A State of the Art Review. Chest 2017, 152, 1070–1086. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, A.; Jamil, D.I.; Karimi, E.B.; Baghi, V.; Gheshlagh, R.G. Prevalence of obstructive sleep apnea in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2463–2468. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.H.; Ng, K.Y.; Chin, W.K. The impact of sleep amount and sleep quality on glycemic control in type 2 diabetes: A systematic review and meta-analysis. Sleep Med. Rev. 2017, 31, 91–101. [Google Scholar] [CrossRef]
- Grandner, M.A.; Seixas, A.; Shetty, S.; Shenoy, S. Sleep Duration and Diabetes Risk: Population Trends and Potential Mechanisms. Curr. Diabetes Rep. 2016, 16, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chattu, V.K.; Chattu, S.K.; Burman, D.; Spence, D.W.; Pandi-Perumal, S.R. The Interlinked Rising Epidemic of Insufficient Sleep and Diabetes Mellitus. Health 2019, 7, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narisawa, H.; Komada, Y.; Miwa, T.; Shikuma, J.; Sakurai, M.; Odawara, M.; Inoue, Y. Prevalence, symptomatic features, and factors associated with sleep disturbance/insomnia in Japanese patients with type-2 diabetes. Neuropsychiatr. Dis. Treat. 2017, 13, 1873–1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nefs, G.; Bazelmans, E.; Donga, E.; Tack, C.J.; De Galan, B. Sweet dreams or bitter nightmare: A narrative review of 25 years of research on the role of sleep in diabetes and the contributions of behavioural science. Diabet. Med. 2019, 37, 418–426. [Google Scholar] [CrossRef] [Green Version]
- Vedhara, K.; Miles, J.N.V.; Wetherell, M.A.; Dawe, K.; Searle, A.; Tallon, D.; Cullum, N.; Day, A.; Dayan, C.; Drake, N.; et al. Coping style and depression influence the healing of diabetic foot ulcers: Observational and mechanistic evidence. Diabetology 2010, 53, 1590–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors (Year) | Type of Study | Sample Size | Diabetes Type | Gender | Age (Mean ±SD) |
|---|---|---|---|---|---|
| Altaf et al. (2016) [24] | Observational CSS | n = 234 | 2 | M= 48 F= 186 | Range: 59,6–62,6 |
| Andruskiene et al. (2013) [21] | Observational CSS | n = 1602 | - | M= 600 F= 1002 | Range: 25–64 |
| Bener et al. (2016) [25] | Observational CSS | n = 459 | 2 | M= 201 F= 258 | 48,2 ± 9,0 47,1 ± 8,3 |
| Nair (2018) [22] | Observational CSe | n = 100 | - | M= 66 F= 34 | Range: 18–90 |
| Haveleia and Gayatri (2019) [23] | Observational CSS | n = 97 | - | M= 43 F= 54 | 54,84 ± 1,71 |
| Maltese et al. (2018) [28] | Observational CoS Prospective | n = 94 | 1 (n = 28) 2 (n= 66) | M= 69% F= 31% | 51,5 ± 16,2 62,7 ± 12,0 |
| Puspita et al. (2019) [26] | Observational CSS | n = 152 | 2 | M= 35.5% F= 64.5% | 57 ± 8,61 |
| Rutkove et al. (2009) [29] | Observational CoS Prospective | n = 82 | 1 2 | M= - F= - | Range: 18–80 |
| Salomé et al. (2013) [30] | Observational CSS | n = 60 | 1 (n = 27) 2 (n = 33) | M= 55% F= 45% | Range: 34–71 |
| Sheahan et al. (2017) [27] | Observational C-CS | n = 77 | 2 | M= 50 F= 27 | 61 ± 11 |
| Subramanian et al. (2019) [20] | Observational C-CS Retrospective | n= 1,656,739 | 2 | M= 902,868 F= 753,871 | 64.7 ± 13,3 |
| Vas et al. (2016) [19] | Observational CR | Three cases | 2 | M= 3 F= 0 | Range: 57, 61 - 63 |
| Authors (Year) | DF Variables | DF Measurement Tools | SC Variables | SC Measurement Tools |
|---|---|---|---|---|
| Altaf et al. (2016) [24] | - Diabetic neuropathy - Presence of DFU - Small fiber neuropathy | - Michigan Neuropathy Screening Instrument - PARP activation - Intraepidermalnervefiber density | - Presence of OSA | - Overnight cardio-respiratory device - Apnea/Hypopnea Index |
| Andruskiene et al. (2013) [21] | - Diabetic foot pain | Unknown | - Problems of falling asleep - Night-time awakenings - Self-rated sleep quality - Sleep latency period - Sleepiness in daytime - Taking naps - Using of sleeping pills | - Basic Nordic Sleep Questionnaire (BNSQ) |
| Bener et al. (2016) [25] | - Diabetic neuropathy - Presence of DFU | - Observation | - Sleep duration - Sleep loss - Sleep disturbances | - Hours |
| Nair (2018) [22] | - Inflammatory symptoms - Vasodilation - Gait | - Leg swelling, foot stiffness - Skin discoloration, sensation, leg heaviness, | - Sleep quality | Unknown |
| Haveleia and Gayatri (2019) [23] | - Presence of DFU - Duration of DFU | Observation | - Sleep quality | - PSQI |
| Maltese et al. (2018) [28] | - DFU severity - DFU persistence - DFU recurrence | - SINBAD scale - Non-healing in 12-month period - Re-ulceration in a healed site | - Risk of OSA | - STOP-BANG Questionnaire |
| Puspita et al. (2019) [26] | - Duration of DFU - DFU assessment | - </> 6 months - Wagner scale | - Sleep quality | - PSQI |
| Rutkove et al. (2009) [29] | - Foot temperature - Nerve conduction studies - Quantitative sensory testing - Diabetic Neuropathy | - iButton - TSA-II NeuroSensory Analyzer - MNSI - UENS | Same as besides, but measurements were done while asleep vs. awake | - iButton - TSA-IINeuroSensory Analyzer - MNSI - UENS |
| Salomé et al. (2013) [30] | - Presence of DFU | - Observation | - Sleep quality | - PSQI |
| Sheahan et al. (2017) [27] | - Foot deformity - DFU surface area - DFU infection - DFU depth - Amputation level | - Small muscle wastage, bony prominence, prominent metatarsal heads, hammer/claw toes, limited joint mobility or Charcot deformity - Longest edge and widest edge - University of Texas scale - IWGDF classification | - Daytime sleeping - Lying down duration - Sleep duration | - Epworth Sleepiness Scale - Minutes - Minutes |
| Subramanian et al. (2019) [20] | - Diabetes-related foot disease | - Signs of amputation, gangrene, presence of DFU, Charcot foot, peripheral vascular disease and peripheral neuropathy | - Presence of OSA | - Previous medical diagnosis |
| Vas et al. (2016) [19] | - Presence of DFU - Osteomyelitis - DFU healing | - Observation - MRI - Observation | - Presence of OSA | - Previous medical diagnosis |
| Sleep Variable | Diabetic Foot Variable | Findings |
|---|---|---|
| OSA | IENFD | - Negative correlation (p < 0.001) between IENFD and OSA that implies small fiber neuropathy [24] |
| MNSI | - Mild OSA was associated with past history of DFU(p = 0.016) [24] | |
| History of DFU | - Positive correlation with OSA presence (p = 0.022) [24] | |
| PARP | - Positive correlation (p = 0.025)between PARP and OSA that involves endothelial dysfunction [24] | |
| DF presence | - DF was significantly predictive of OSA [20] | |
| DFU healing | - CPAP therapy for OSA led to DFU healing in patients under treatment [19] - High risk of OSA led to poor DFU healing [28] | |
| Sleep quality | DFU healing | - Microcurrent therapy for DFU led to a significantly better sleep quality [22] |
| DFU presence | - Subjective sleep quality showed significant disparity with comprehensive sleep quality (PQSI) [23] - Poor sleep quality was significantly related to pain level (p = 0.013) [26] - No significant difference in sleep quality of people with diabetes with and without DFU [26] - Pain (p: 0.048) and stress (p: 0.001) were significantly related to poor sleep quality [23] - Patients with DFU had poor sleep quality (Salomé et al., 2013) | |
| Sleep duration | Minor amputation presence | - Patients with minor amputation had lower Epworth Sleepiness Scale score (lower score = normal) than those without amputation [27] |
| DFU presence | - DFU group showed no differences from DM and/or DN groups in lying down duration and sleep duration [27] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Torres, R.; Ruiz-Muñoz, M.; Pérez-Belloso, A.J.; García-Romero, J.; Gónzalez-Sánchez, M. Is There an Association between Sleep Disorders and Diabetic Foot? A Scoping Review. J. Clin. Med. 2021, 10, 2530. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112530
Fernández-Torres R, Ruiz-Muñoz M, Pérez-Belloso AJ, García-Romero J, Gónzalez-Sánchez M. Is There an Association between Sleep Disorders and Diabetic Foot? A Scoping Review. Journal of Clinical Medicine. 2021; 10(11):2530. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112530
Chicago/Turabian StyleFernández-Torres, Raúl, María Ruiz-Muñoz, Ana J. Pérez-Belloso, Jerónimo García-Romero, and Manuel Gónzalez-Sánchez. 2021. "Is There an Association between Sleep Disorders and Diabetic Foot? A Scoping Review" Journal of Clinical Medicine 10, no. 11: 2530. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112530