
Surgical Assessment of Tissue Quality during Pelvic Organ Prolapse Repair in Postmenopausal Women Pre-Treated Either with Locally Applied Estrogen or Placebo: Results of a Double-Masked, Placebo-Controlled, Multicenter Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Intervention and Study Procedures
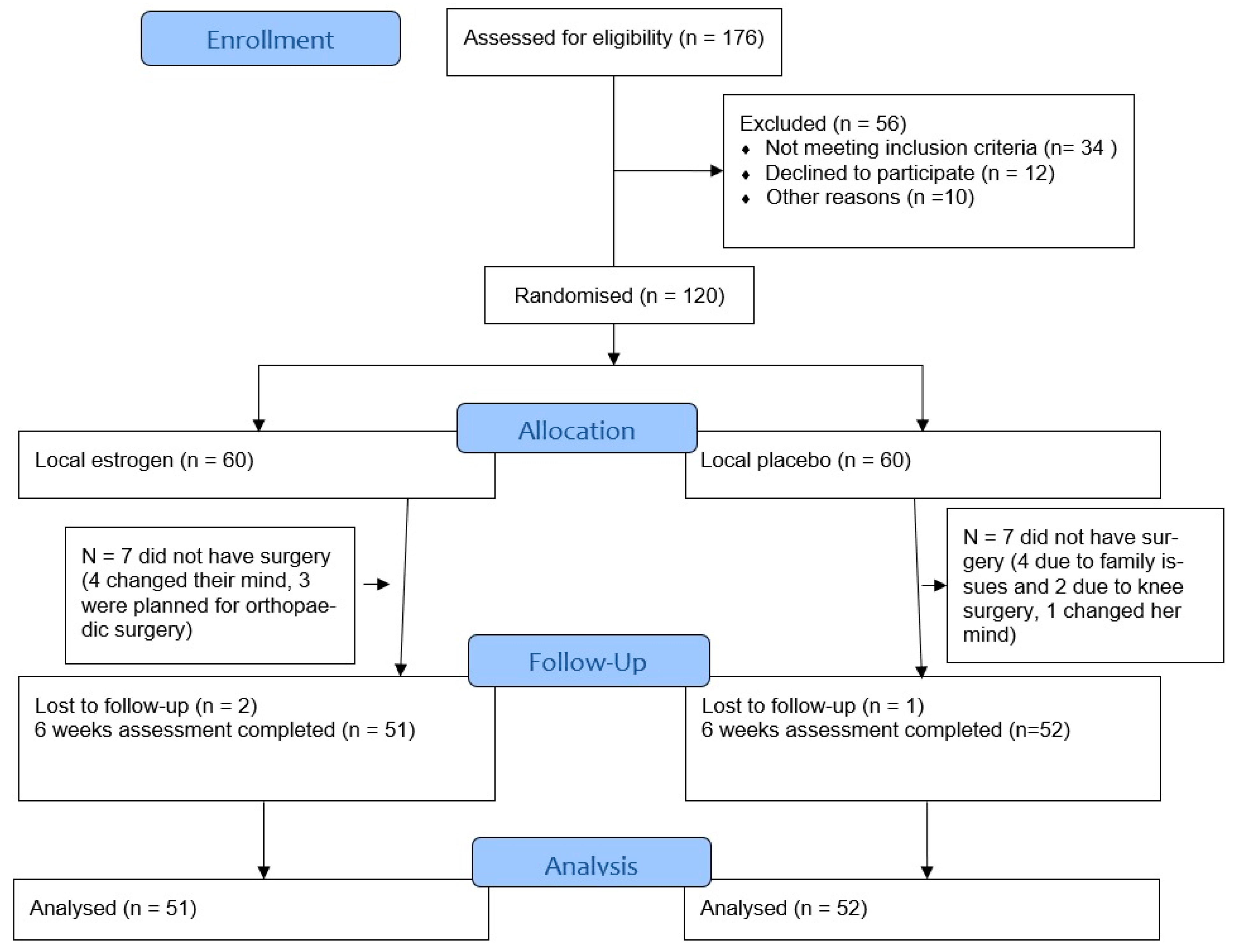
2.4. Randomization
2.5. Measurements
2.5.1. Intraoperative Surgical Assessment of Tissue Quality in Cases with or without Estrogen Pretreatment
- perfusion of the tissue within the operation area (four-point scoring system);
- atrophy with poor perfusion within the operation area (four-point scoring system);
- presence of a soft or firm tissue consistency (three-point scoring system);
- difficulty of dissection of delineating surgical planes (four-point scoring system);
- tissue handling (yes/no);
- regular pelvic anatomy (yes/no).
2.5.2. Intraoperative and Early Postoperative Surgical Course in Cases with or without Estrogen Pre-Treatment
2.6. Statistical Analysis
3. Results
3.1. Safety
3.2. Intraoperative Surgical Assessment of Tissue Quality
3.3. Intra- and Early Postoperative Course in Patients with or without Estrogen Pre-Treatment
3.4. Multivariate Analysis
4. Discussion
4.1. Main Results
4.2. Comparison with Literature
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robinson, D.; Cardozo, L.D. The role of estrogens in female lower urinary tract dysfunction. Urology 2003, 62, 45–51. [Google Scholar] [CrossRef]
- Soderberg, M.W.; Johansson, B.; Masironi, B.; Bystrom, B.; Falconer, C.; Sahlin, L.; Ordeberg, G.E. Pelvic floor sex steroid hormone receptors, distribution and expression in pre- and postmenopausal stress urinary incontinent women. Acta Obstet. Gynecol. Scand. 2007, 86, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Cooke, P.S.; Uchima, F.D.; Fujii, D.K.; Bern, H.A.; Cunha, G.R. Restoration of normal morphology and estrogen responsiveness in cultured vaginal and uterine epithelia transplanted with stroma. Proc. Natl. Acad. Sci. USA 1986, 83, 2109–2113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derzko, C.M.; Rohrich, S.; Panay, N. Does age at the start of treatment for vaginal atrophy predict response to vaginal estrogen therapy? Post hoc analysis of data from a randomized clinical trial involving 205 women treated with 10 mug estradiol vaginal tablets. Menopause 2020, 28, 113–118. [Google Scholar] [CrossRef]
- Rahn, D.D.; Good, M.M.; Roshanravan, S.M.; Shi, H.; Schaffer, J.I.; Singh, R.J.; Word, R.A. Effects of preoperative local estrogen in postmenopausal women with prolapse: A randomized trial. J. Clin. Endocrinol. Metab. 2014, 99, 3728–3736. [Google Scholar] [CrossRef] [Green Version]
- Bodner-Adler, B.; Alarab, M.; Ruiz-Zapata, A.M.; Latthe, P. Effectiveness of hormones in postmenopausal pelvic floor dysfunction-International Urogynecological Association research and development-committee opinion. Int. Urogynecol. J. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oppegaard, K.S.; Lieng, M.; Berg, A.; Istre, O.; Qvigstad, E.; Nesheim, B.I. A combination of misoprostol and estradiol for preoperative cervical ripening in postmenopausal women: A randomised controlled trial. BJOG 2010, 117, 53–61. [Google Scholar] [CrossRef]
- Olsen, A.L.; Smith, V.J.; Bergstrom, J.O.; Colling, J.C.; Clark, A.L. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet. Gynecol. 1997, 89, 501–506. [Google Scholar] [CrossRef]
- Barber, M.D. Pelvic organ prolapse. BMJ 2016, 354, i3853. [Google Scholar] [CrossRef]
- Tancer, M.L. Observations on prevention and management of vesicovaginal fistula after total hysterectomy. Surg. Gynecol. Obstet. 1992, 175, 501–506. [Google Scholar] [CrossRef]
- Williams, T.J. Urologic injuries. Obstet. Gynecol. Annu. 1975, 4, 347–368. [Google Scholar]
- Kato, K.; Hayashi, Y.; Adachi, M.; Ando, R.; Kawanishi, H.; Matsui, H.; Kato, T.; Hirabayashi, H.; Suzuki, S.; Hattori, R. Razor-type dermatomes enable quick and thin vaginal dissection with less bleeding in colpocleisis. Int. Urogynecol. J. 2020, 31, 1959–1964. [Google Scholar] [CrossRef] [Green Version]
- Tyagi, T.; Alarab, M.; Leong, Y.; Lye, S.; Shynlova, O. Local oestrogen therapy modulates extracellular matrix and immune response in the vaginal tissue of post-menopausal women with severe pelvic organ prolapse. J. Cell. Mol. Med. 2019, 23, 2907–2919. [Google Scholar] [CrossRef] [PubMed]
- de Boer, T.A.; Slieker-Ten Hove, M.C.; Burger, C.W.; Kluivers, K.B.; Vierhout, M.E. The prevalence and factors associated with previous surgery for pelvic organ prolapse and/or urinary incontinence in a cross-sectional study in The Netherlands. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 158, 343–349. [Google Scholar] [CrossRef]
- Wei, J.T.; Nygaard, I.; Richter, H.E.; Nager, C.W.; Barber, M.D.; Kenton, K.; Amundsen, C.L.; Schaffer, J.; Meikle, S.F.; Spino, C.; et al. A midurethral sling to reduce incontinence after vaginal prolapse repair. N. Engl. J. Med. 2012, 366, 2358–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unger, C.A.; Walters, M.D.; Ridgeway, B.; Jelovsek, J.E.; Barber, M.D.; Paraiso, M.F. Incidence of adverse events after uterosacral colpopexy for uterovaginal and posthysterectomy vault prolapse. Am. J. Obstet. Gynecol. 2015, 212, 603.e1–603.e7. [Google Scholar] [CrossRef] [PubMed]
- Phillips, N.A.; Bachmann, G.A. The genitourinary syndrome of menopause. Menopause 2021, 28, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Buck, E.S.; Lukas, V.A.; Rubin, R.S. Effective Prevention of Recurrent UTIs With Vaginal Estrogen: Pearls for a Urological Approach to Genitourinary Syndrome of Menopause. Urology 2020, 151, 31–36. [Google Scholar] [CrossRef]
- Gandhi, J.; Chen, A.; Dagur, G.; Suh, Y.; Smith, N.; Cali, B.; Khan, S.A. Genitourinary syndrome of menopause: An overview of clinical manifestations, pathophysiology, etiology, evaluation, and management. Am. J. Obstet. Gynecol. 2016, 215, 704–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felding, C.; Mikkelsen, A.L.; Clausen, H.V.; Loft, A.; Larsen, L.G. Preoperative treatment with oestradiol in women scheduled for vaginal operation for genital prolapse. A randomised, double-blind trial. Maturitas 1992, 15, 241–249. [Google Scholar] [CrossRef]
- Rahn, D.D.; Ward, R.M.; Sanses, T.V.; Carberry, C.; Mamik, M.M.; Meriwether, K.V.; Olivera, C.K.; Abed, H.; Balk, E.M.; Murphy, M.; et al. Vaginal estrogen use in postmenopausal women with pelvic floor disorders: Systematic review and practice guidelines. Int. Urogynecol. J. 2015, 26, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Karp, D.R.; Jean-Michel, M.; Johnston, Y.; Suciu, G.; Aguilar, V.C.; Davila, G.W. A randomized clinical trial of the impact of local estrogen on postoperative tissue quality after vaginal reconstructive surgery. Female Pelvic Med. Reconstr. Surg. 2012, 18, 211–215. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Estrogen Group (n = 51) | Placebo Group (n = 52) | p-Value |
|---|---|---|---|
| Mean ± SD or n (%) | Mean ± SD or n (%) | ||
| Age (y) | 64.3 ± 9.7 | 61.2 ± 10.1 | n.s. |
| Age at menopause (y) | 48.9 ± 6.2 | 49.5 ± 5.9 | n.s. |
| Parity | 2.4 ± 2.1 | 2.3 ± 1.1 | n.s. |
| BMI (kg/m2) | 26.9 ± 4.0 | 27.3 ± 4.8 | n.s. |
| Diabetes | 4 (8) | 4 (8) | n.s. |
| COPD | 4 (8) | 3 (6) | n.s. |
| Smoking | 11 (22) | 8 (15) | n.s. |
| POP-Q stage baseline & after 6 weeks | 2.8 ± 0.4 | 2.7 ± 0.5 | n.s. |
| Stage II | 9 (17) | 13 (25) | |
| Stage III | 41 (80) | 38 (73) | |
| Stage IV | 1 (0) | 1 (0) | |
| Uterine Preservation | 0.043 | ||
| No | 26 (51) | 29 (56) | |
| Yes | 11 (22) | 18 (35) | |
| Previous hysterectomy | 14 (28) | 5 (10) | |
| Affected vaginal compartment | n.s. | ||
| Anterior (exclusive) | 3 (6) | 4 (8) | |
| Posterior (exclusive) | 1 (2) | 1 (2) | |
| all three (anterior, apical, posterior) | 47 (92) | 47 (90) | |
| Operative time | 88.73 ± 30.3 | 78.46 ± 32.2 | n.s. |
| Total length of stay | 4.5 ± 1.2 | 4.6 ± 1.2 | n.s. |
| Significant blood loss (>500 mL) | 1 (2) | 1 (2) | n.s. |
| Use of analgesics | 51 (100) | 52 (100) | n.s. |
| Use of antibiotics | 3 (6) | 15 (29) | 0.003 |
| Readmission | 3 (6) | 2 (4) | n.s |
| Defined complication | 11(22) | 15(29) | 0.045 |
| POUR | 6/11 (55) | 4/15 (27) | |
| UTI | 3/11 (27) | 6 (40) | |
| Postoperative hemorrhage | 1/11(9) | 2 (13) | |
| surgical site infection | 1/11 (9) | 3 (20) |
| Estrogen Group (n = 51) Mean ± SD or n (%) | Placebo Group (n = 52) Mean ± SD or n (%) | p-Value | |
|---|---|---|---|
| Q1. The tissue within the operation area is well perfused. | 2.12 ±1.03 | 2.19 ± 0.99 | 0.219 |
| Q2. There is atrophy and poorly perfused tissue within the operation area. | 0.55 ± 0.95 | 0.54 ± 0.96 | 0.836 |
| Q3. The tissue consistency within the operation is (soft/firm) | 0.16 ± 0.42 | 0.15 ± 0.36 | 0.435 |
| Q4. The surgical planes are easily dissected of delineated. | 1.67 ± 1.16 | 1.88 ± 1.15 | 0.225 |
| Q5. Easy vesicovaginal dissection | 0.518 | ||
| 1: no | 8 (16) | 9 (17) | |
| 2: yes | 43 (84) | 43 (82) | |
| Q6. Easy rectovaginal dissection | 0.486 | ||
| 1: no | 9 (18) | 10 (19) | |
| 2: yes | 42 (82) | 41 (79) | |
| 3: Pouch of Douglas was not opened | 0 (0) | 1 (2) | |
| Q7. The pelvic anatomy is regular | 0.597 | ||
| 1: no | 7 (14) | 7 (14) | |
| 2: yes | 44 (86) | 45 (87) | |
| Q8. Do you think the patient received pretreatment with local estrogen cream? | 0.034 | ||
| 1: no | 12 (24) | 22 (42) | |
| 2: yes | 39 (77) | 30 (58) |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Age | 0.993 (0.945–1.043) | 0.780 |
| Estrogen treatment | 0.475 (0.177–1.274) | 0.139 |
| BMI | 0.984 (0.885–1.093) | 0.758 |
| Affected vaginal compartment | 1.338 (0.636–2.815) | 0.443 |
| Smoking | 1.223 (0.331–4.522) | 0.763 |
| COPD | 1.624 (0.143–18.485) | 0.696 |
| POP-Q at baseline | 0.454 (0.147–1.400) | 0.169 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marschalek, M.-L.; Bodner, K.; Kimberger, O.; Morgenbesser, R.; Dietrich, W.; Obruca, C.; Husslein, H.; Umek, W.; Kölbl, H.; Bodner-Adler, B. Surgical Assessment of Tissue Quality during Pelvic Organ Prolapse Repair in Postmenopausal Women Pre-Treated Either with Locally Applied Estrogen or Placebo: Results of a Double-Masked, Placebo-Controlled, Multicenter Trial. J. Clin. Med. 2021, 10, 2531. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112531
Marschalek M-L, Bodner K, Kimberger O, Morgenbesser R, Dietrich W, Obruca C, Husslein H, Umek W, Kölbl H, Bodner-Adler B. Surgical Assessment of Tissue Quality during Pelvic Organ Prolapse Repair in Postmenopausal Women Pre-Treated Either with Locally Applied Estrogen or Placebo: Results of a Double-Masked, Placebo-Controlled, Multicenter Trial. Journal of Clinical Medicine. 2021; 10(11):2531. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112531
Chicago/Turabian StyleMarschalek, Marie-Louise, Klaus Bodner, Oliver Kimberger, Raffaela Morgenbesser, Wolf Dietrich, Christian Obruca, Heinrich Husslein, Wolfgang Umek, Heinz Kölbl, and Barbara Bodner-Adler. 2021. "Surgical Assessment of Tissue Quality during Pelvic Organ Prolapse Repair in Postmenopausal Women Pre-Treated Either with Locally Applied Estrogen or Placebo: Results of a Double-Masked, Placebo-Controlled, Multicenter Trial" Journal of Clinical Medicine 10, no. 11: 2531. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10112531