
Cost-Effectiveness, Efficacy, and Safety Analysis of Tailored Therapy in Patients with Helicobacter pylori Infection


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. H. Pylori Diagnosis and DPO-Based Multiplex PCR
2.3. H. Pylori Eradication Therapy Regimen
2.4. Medical Cost
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Subjects
3.2. H. pylori Eradication Rate of Study Subjects
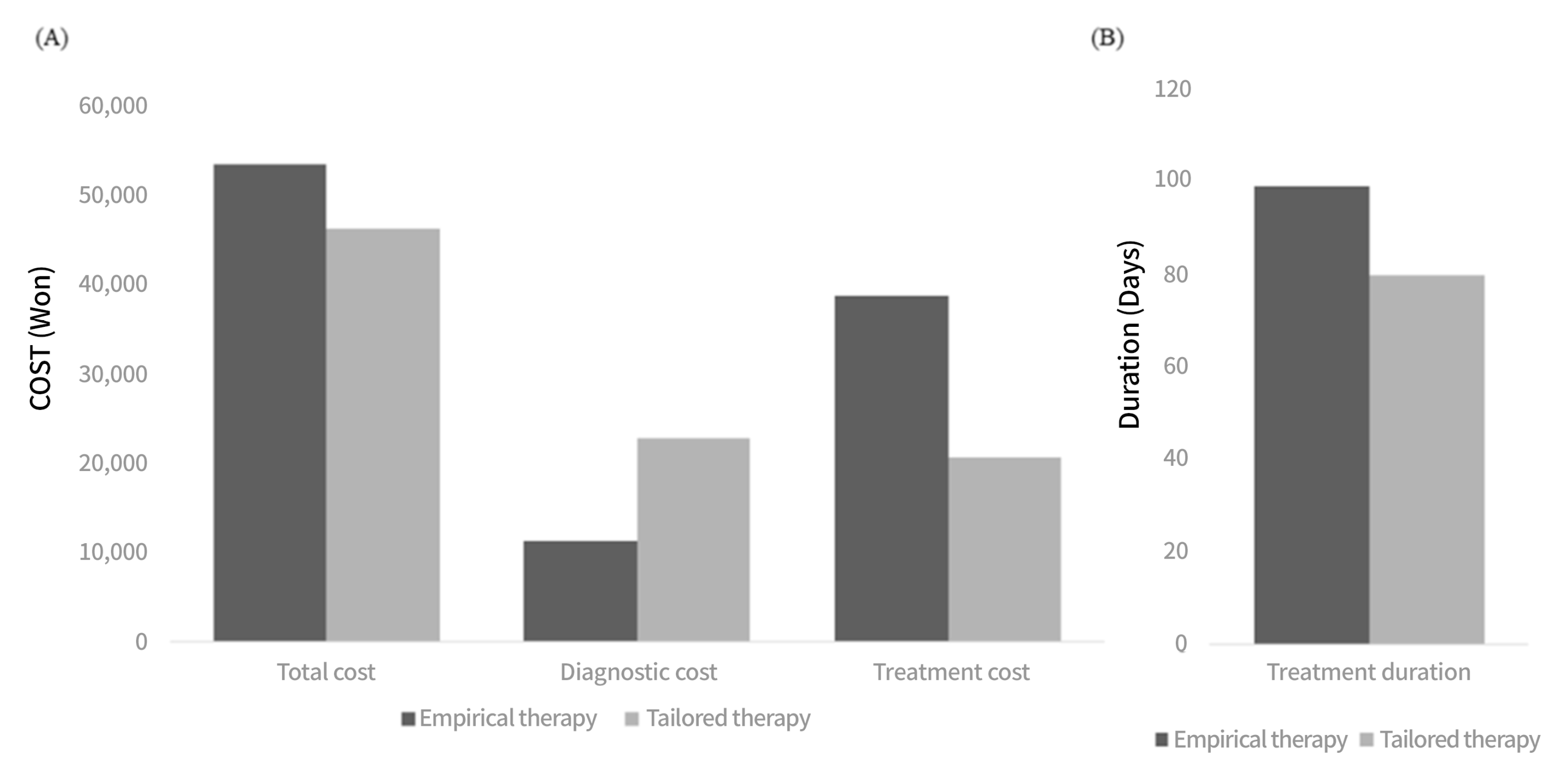
3.3. Medical Cost of Study Subjects
3.4. Adverse Effects Seen in Study Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farinha, P.; Gascoyne, R.D.J.G. Helicobacter pylori and MALT lymphoma. Gastroenterology 2005, 128, 1579–1605. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.-Q.; Sridhar, S.; Hunt, R.H.J.T.L. Role of Helicobacter pylori infection and non-steroidal anti-inflammatory drugs in peptic-ulcer disease: A meta-analysis. Lancet 2002, 359, 14–22. [Google Scholar] [CrossRef]
- Wroblewski, L.E.; Peek, R.M.; Wilson, K.T. Helicobacter pylori and gastric cancer: Factors that modulate disease risk. Clin. Microbiol. Rev. 2010, 23, 713–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, H.K.; Kang, S.J.; Lee, Y.C.; Yang, H.-J.; Park, S.-Y.; Shin, C.M.; Kim, S.E.; Lim, H.C.; Kim, J.-H.; Nam, S.Y.; et al. Evidence-based Guidelines for the Treatment of Helicobacter pylori Infection in Korea: 2020 Revised Edition. Korean J. Helicobacter Up. Gastrointest. Res. 2020, 20, 261–287. [Google Scholar] [CrossRef]
- Kim, J.M.; Kim, J.S.; Jung, H.C.; Kim, N.; Kim, Y.-J.; Song, I.S. Distribution of antibiotic MICs for Helicobacter pylori strains over a 16-year period in patients from Seoul, South Korea. Antimicrob. Agents Chemother. 2004, 48, 4843–4847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, T.J.; Kim, N.; Kim, H.B.; Lee, B.H.; Nam, R.H.; Park, J.H.; Lee, M.K.; Park, Y.S.; Lee, D.H.; Jung, H.C.; et al. Change in antibiotic resistance of Helicobacter pylori strains and the effect of A2143G point mutation of 23S rRNA on the eradication of H. pylori in a single center of Korea. J. Clin. Gastroenterol. 2010, 44, 536–543. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, V.; Giorgio, F.; Hassan, C.; Manes, G.; Vannella, L.; Panella, C.; Ierardi, E.; Zullo, A. Worldwide H. pylori antibiotic resistance: A systematic review. J. Gastrointest. Liver Dis. 2010, 19, 409–414. [Google Scholar]
- Kim, B.J.; Lee, H.; Lee, Y.C.; Jeon, S.W.; Kim, G.H.; Kim, H.-S.; Sung, J.K.; Lee, D.H.; Kim, H.U.; Park, M.I.; et al. Ten-Day Concomitant, 10-Day Sequential, and 7-Day Triple Therapy as First-Line Treatment for Helicobacter pylori Infection: A Nationwide Randomized Trial in Korea. Gut Liver 2019, 13, 531–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.S.; Kim, B.W.; Hong, S.J.; Kim, J.I.; Shim, K.-N.; Kim, J.-H.; Baik, G.H.; Kim, S.W.; Song, H.J.; Kim, J.H. Sequential Therapy versus Triple Therapy for the First Line Treatment of Helicobacter pylori in Korea: A Nationwide Randomized Trial. Gut Liver 2016, 10, 556–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, T.L.; Gao, J.G.; Wang, J.H.; Chen, D.; Lu, C.; Xu, C.-F. Current status of Helicobacter pylori eradication and risk factors for eradication failure. World J. Gastroenterol. 2020, 26, 4846–4856. [Google Scholar] [CrossRef]
- Tang, Y.; Tang, G.; Pan, L.; Zhu, H.; Zhou, S.; Wei, Z. Clinical factors associated with initial Helicobacter pylori eradication therapy: A retrospective study in China. Sci. Rep. 2020, 10, 1–5. [Google Scholar] [CrossRef]
- Liou, J.M.; Chen, P.Y.; Kuo, Y.T.; Wu, M.-S. The Taiwan Gastrointestinal Disease and Helicobacter Consortium. Toward population specific and personalized treatment of Helicobacter pylori infection. J. Biomed. Sci. 2018, 25, 70. [Google Scholar] [CrossRef]
- Kuo, C.J.; Lee, C.H.; Chang, M.L.; Lin, C.-Y.; Lin, W.-R.; Su, M.-Y.; Chiu, C.-H.; Tseng, C.-N.; Wu, Y.-S.; Chiu, C.-T.; et al. Multidrug resistance: The clinical dilemma of refractory Helicobacter pylori infection. J. Microbiol. Immunol. Infect. 2021. [Google Scholar] [CrossRef]
- De Francesco, V.; Pontone, S.; Bellesia, A.; Serviddio, G.; Panetta, C.; Palma, R.; Zullo, A. Quadruple, sequential, and concomitant first-line therapies for H. pylori eradication: A prospective, randomized study. Dig. Liver Dis. 2018, 50, 139–141. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Baj, J.; Forma, A.; Sitarz, M.; Portincasa, P.; Garruti, G.; Krasowska, D.; Maciejewski, R. Helicobacter pylori Virulence Factors-Mechanisms of Bacterial Pathogenicity in the Gastric Microenvironment. Cells 2020, 10, 27. [Google Scholar] [CrossRef]
- Imkamp, F.; Lauener, F.N.; Pohl, D.; Lehours, P.; Vale, F.F.; Jehanne, Q.; Zbinden, R.; Keller, P.M.; Wagner, K. Rapid Characterization of Virulence Determinants in Helicobacter pylori Isolated from Non-Atrophic Gastritis Patients by Next-Generation Sequencing. J. Clin. Med. 2019, 8, 1030. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Kim, N.; Nam, R.H.; Choi, S.I.; Lee, J.W.; Lee, D.H. Primary and secondary antibiotic resistance of Helicobacter pylori in Korea from 2003 to 2018. Helicobacter 2019, 24, e12660. [Google Scholar] [CrossRef]
- Seo, S.I.; Do, B.J.; Kang, J.G.; Kim, H.S.; Jang, M.K.; Kim, H.Y.; Shin, W.G. Helicobacter pylori eradication according to sequencing-based 23S ribosomal RNA point mutation associated with clarithromycin resistance. J. Clin. Med. 2020, 9, 54. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.L.; Cho, S.-J.; Chung, S.J.; Lee, A.; Choi, J.; Chung, H.; Kim, S.G. Empiric Versus Clarithromycin Resistance-Guided Therapy for Helicobacter pylori Based on Polymerase Chain Reaction Results in Patients with Gastric Neoplasms or Gastric Mucosa-Associated Lymphoid Tissue Lymphoma: A Randomized Controlled Trial. Clin. Transl. Gastroenterol. 2020, 11, e00194. [Google Scholar] [CrossRef] [PubMed]
- Skrebinska, S.; Mégraud, F.; Bessède, E.J.H. Diagnosis of Helicobacter pylori infection. Helicobacter 2018, 23, e12515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, Y.S.; Park, C.H.; Park, J.H.; Nam, E.; Lee, H.L. Efficacy of Helicobacter pylori eradication therapies in Korea: A systematic review and network meta-analysis. Helicobacter 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.Z.; Xie, Y.; Lu, H.; Cheng, H.; Zeng, Z.R.; Zhou, L.Y.; Chen, Y.; Wang, J.B.; Du, Y.Q.; Lu, N.H.; et al. Fifth Chinese National Consensus Report on the management of Helicobacter pylori infection. Helicobacter 2018, 23, e12475. [Google Scholar] [CrossRef]
- Huang, Y.K.; Wu, M.C.; Wang, S.S.; Kuo, C.-H.; Lee, Y.-C.; Chang, L.-L.; Wang, T.-H.; Chen, Y.-H.; Wang, W.-M.; Wu, D.-C.; et al. Lansoprazole-based sequential and concomitant therapy for the first-line Helicobacter pylori eradication. J. Dig. Dis. 2012, 13, 232–238. [Google Scholar] [CrossRef]
- Liou, J.M.; Chen, P.Y.; Luo, J.C.; Lee, J.-Y.; Chen, C.-C.; Fang, Y.-J.; Yang, T.-H.; Chang, C.-Y.; Bair, M.-J.; Chen, M.-J.; et al. Efficacies of Genotypic Resistance-Guided vs Empirical Therapy for Refractory Helicobacter pylori Infection. Gastroenterology 2018, 155, 1109–1119. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.W.; Shin, G.Y.; Kim, J.W.; Moon, J.-C.; Chang, E.J.; Oh, C.H.; Jang, J.-Y. Cost-Effectiveness of Empirical Bismuth-Based Quadruple Therapy and Tailored Therapy After Clarithromycin Resistance Tests for Helicobacter pylori Eradication. Dig. Dis. Sci. 2021. [Google Scholar] [CrossRef]
- Cosme, A.; Montes, M.; Martos, M.; Gil, I.; Mendarte, U.; Salicio, Y.; Piñeiro, L.; Recasens, M.T.; Ibarra, B.; Sarasqueta, C.; et al. Usefulness of antimicrobial susceptibility in the eradication of Helicobacter pylori. Clin. Microbiol. Infect. 2013, 19, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Gweon, T.G.; Kim, J.S.; Kim, B.W. An Economic Modeling Study of Helicobacter pylori Eradication: Comparison of Dual Priming Oligonucleotide-Based Multiplex Polymerase Chain Reaction and Empirical Treatment. Gut Liver 2018, 12, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Gisbert, J.P. Empirical or susceptibility-guided treatment for Helicobacter pylori infection? A comprehensive review. Ther. Adv. Gastroenterol. 2020, 13, 1756284820968736. [Google Scholar] [CrossRef] [PubMed]
- Pero, R.; Brancaccio, M.; Laneri, S.; De Biasi, M.G.; Lombardo, B.; Scudiero, O. A Novel View of Human Helicobacter pylori Infections: Interplay between Microbiota and Beta-Defensins. Biomolecules 2019, 9, 237. [Google Scholar] [CrossRef] [Green Version]
- Pero, R.; Coretti, L.; Nigro, E.; Lembo, F.; Laneri, S.; Lombardo, B.; Daniele, A.; Scudiero, O. β-Defensins in the Fight against Helicobacter pylori. Molecules 2017, 22, 424. [Google Scholar] [CrossRef] [PubMed]
- Angrisano, T.; Pero, R.; Brancaccio, M.; Coretti, L.; Florio, E.; Pezone, A.; Calabrò, V.; Falco, G.; Keller, S.; Lembo, F.; et al. Cyclical DNA Methylation and Histone Changes Are Induced by LPS to Activate COX-2 in Human Intestinal Epithelial Cells. PLoS ONE 2016, 11, e0156671. [Google Scholar] [CrossRef]
- Woo, H.D.; Fernandez-Jimenez, N.; Ghantous, A.; Degli Esposti, D.; Cuenin, C.; Cahais, V.; Choi, I.J.; Kim, Y.-I.; Kim, J.; Herceg, Z. Genome-wide profiling of normal gastric mucosa identifies Helicobacter pylori- and cancer-associated DNA methylome changes. Int. J. Cancer 2018, 143, 597–609. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Zhang, J.; Song, Z.; He, L.; Li, Y.; Qian, J.; Bai, P.; Xue, Y.; Wang, Y.; Lin, S. Tailored versus Triple plus Bismuth or Concomitant Therapy as Initial Helicobacter pylori Treatment: A Randomized Trial. Helicobacter 2016, 21, 91–99. [Google Scholar] [CrossRef]
- Choi, Y.I.; Chung, J.W.; Park, D.K.; Kim, K.O.; Kwon, K.A.; Kim, Y.J.; Seo, J.Y. Tailored eradication vs empirical bismuth-containing quadruple therapy for first-line Helicobacter pylori eradication: A comparative, open trial. World J. Gastroenterol. 2019, 25, 6743–6751. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 364) | Empirical Therapy (n = 155) | Tailored Therapy (n = 209) | p Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 56.0 ± 12.5 | 54.8 ± 11.7 | 56.9 ± 13.0 | 0.117 |
| Sex, n (%) | ||||
| Male | 197 (54.1) | 79 (51.0) | 118 (56.5) | 0.298 |
| Female | 167 (45.9) | 76 (49.0) | 91 (43.5) | |
| Smoking, n (%) | 108 (29.7) | 37 (23.9) | 71 (34.0) | 0.037 |
| Alcohol drinking, n (%) | 110 (30.2) | 56 (36.1) | 54 (25.8) | 0.034 |
| Disease for H. pylori eradication, n (%) | <0.001 | |||
| Peptic ulcer | 109 (29.9) | 39 (25.2) | 70 (33.5) | |
| Post-ESD for EGC | 24 (6.6) | 5 (3.2) | 19 (9.1) | |
| Post-ER for adenoma | 35 (9.6) | 11 (7.1) | 24 (11.5) | |
| MALT Lymphoma | 4 (1.1) | 2 (1.3) | 2 (1.0) | |
| H. pylori gastritis | 175 (48.1) | 93 (60.0) | 82 (39.2) | |
| Lymphoid follicular gastritis | 13 (3.6) | 4 (2.6) | 9 (4.3) | |
| Family history of gastric cancer | 4 (1.1) | 1 (0.6) | 3 (1.5) |
| Empirical Therapy (n = 155) | Tailored Therapy (n = 209) | p Value | ||
|---|---|---|---|---|
| 1st line eradication regimen, n (%) | Triple | 27 (17.4) | 139 (66.5) | - |
| Quadruple | 17 (11.0) | 60 (28.7) | - | |
| Sequential | 111 (71.6) | 10 (4.8) | - | |
| 1st line eradication rate according to regimen, n (%) | Triple | 22/27 (81.5) | 124/139 (89.2) | 0.328 |
| Quadruple | 15/17 (88.2) | 55/60 (91.7) | 0.646 | |
| Sequential | 91/111 (82.0) | 8/10 (80.0) | 1.000 | |
| Outcome of H. pylori 1st line eradication, % (n/N) | ||||
| Eradication rate in analysis | 82.6 (128/155) | 91.7 (187/204) | 0.023 | |
| Empirical Therapy | Tailored Therapy | p Value | |
|---|---|---|---|
| Adverse event for eradication treatment, n (%) | 23 (14.8) | 27 (12.9) | 0.028 |
| Abdominal pain | 5 (21.8) | 2 (7.4) | |
| Nausea/Vomiting | 6 (26.1) | 8 (29.7) | |
| Headache | 4 (17.4) | 2 (7.4) | |
| Diarrhea | 5 (21.7) | 4 (14.8) | |
| Dyspepsia | 0 (0.0) | 7 (25.9) | |
| Metallic taste | 3 (13.0) | 4 (14.8) | |
| No further treatment after eradication fail, n (%) | 6 (3.9) | 0 (0.0) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choe, A.R.; Shim, K.-N.; Park, Y.; Song, E.-M.; Tae, C.H.; Jung, S.-A. Cost-Effectiveness, Efficacy, and Safety Analysis of Tailored Therapy in Patients with Helicobacter pylori Infection. J. Clin. Med. 2021, 10, 2619. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122619
Choe AR, Shim K-N, Park Y, Song E-M, Tae CH, Jung S-A. Cost-Effectiveness, Efficacy, and Safety Analysis of Tailored Therapy in Patients with Helicobacter pylori Infection. Journal of Clinical Medicine. 2021; 10(12):2619. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122619
Chicago/Turabian StyleChoe, A Reum, Ki-Nam Shim, Yehyun Park, Eun-Mi Song, Chung Hyun Tae, and Sung-Ae Jung. 2021. "Cost-Effectiveness, Efficacy, and Safety Analysis of Tailored Therapy in Patients with Helicobacter pylori Infection" Journal of Clinical Medicine 10, no. 12: 2619. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10122619