
Investigation of the Effectiveness of Surgical Treatment on Maxillary Medication-Related Osteonecrosis of the Jaw: A Literature Review


Abstract
:1. Introduction
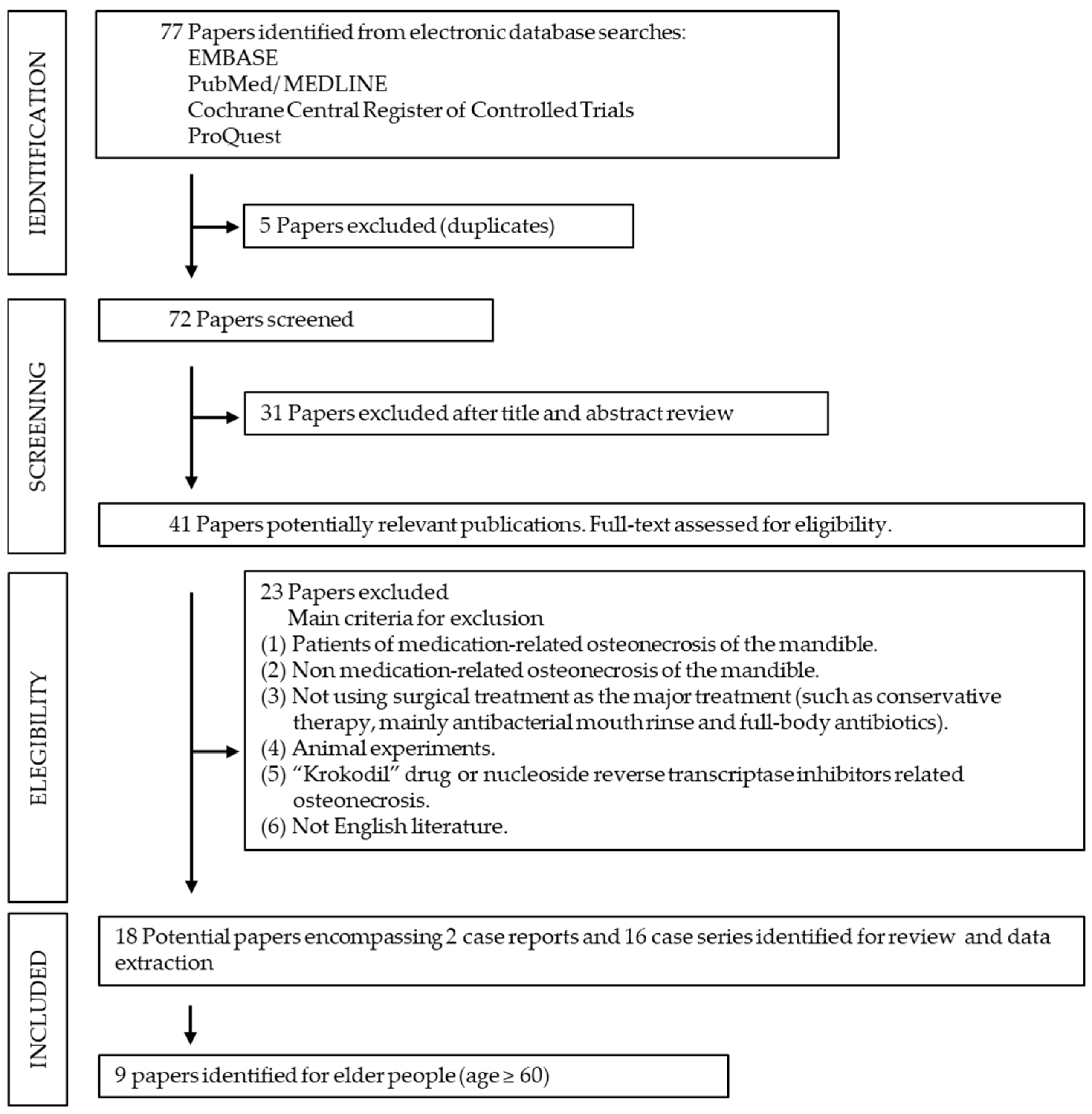
2. Materials and Methods
2.1. Study Methods
2.2. Literature Search Strategies (Full Electronic Text)
- (1)
- 2000–2021 English-language reference literature.
- (2)
- Case report or case series.
- (3)
- Patients with maxillary MRONJ or combined with mandibular MRONJ.
- (4)
- An intervention of surgical treatment.
- (5)
- Prognosis for the intervention outcome of wound healing, recurrence, or complication.
- (6)
- Elderly people (age ≥ 60).
- (1)
- Patients only with mandibular MRONJ.
- (2)
- Osteonecrosis of the mandible unrelated to medication.
- (3)
- Surgery not used as the major treatment but rather a conservative therapy, such as the use of antibacterial mouth rinse and full-body antibiotics.
- (4)
- Animal experimentation.
- (5)
- “Krokodil” drug or nucleoside reverse transcriptase inhibitor-related osteonecrosis.
- (6)
- Reporting language other than English.
2.3. Literature Quality Assessment and Risk of Bias
2.4. Data Extraction and Meta-Analysis
2.5. Eligibility Criteria
2.6. Statistical Analysis
2.7. Interpretation of Forest Plots
3. Results
3.1. Data Consolidation Analysis
3.2. Effectiveness of Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davies, E.A.; O’Mahony, M.S. Adverse drug reactions in special populations–the elderly. Br. J. Clin. Pharmaco. 2015, 80, 796–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavan, A.H.; Gallagher, P. Predicting risk of adverse drug reactions in older adults. Ther. Adv. Drug Saf. 2016, 7, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Sozen, T.; Ozisik, L.; Basaran, N.C. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Rachner, T.D.; Khosla, S.; Hofbauer, L.C. Osteoporosis: Now and the future. Lancet 2011, 377, 1276–1287. [Google Scholar] [CrossRef] [Green Version]
- Marx, R.E. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J. Oral Maxil. Surg. 2004, 62, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention, and treatment. J. Oral Maxil. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- King, R.; Tanna, N.; Patel, V. Medication-related osteonecrosis of the jaw unrelated to bisphosphonates and denosumab-a review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 289–299. [Google Scholar] [CrossRef]
- Estilo, C.L.; Fornier, M.; Farooki, A.; Carlson, D.; Bohle, G., 3rd; Huryn, J.M. Osteonecrosis of the jaw related to bevacizumab. J. Clin. Oncol. 2008, 26, 4037–4038. [Google Scholar] [CrossRef]
- van Cann, T.; Loyson, T.; Verbiest, A.; Clement, P.M.; Bechter, O.; Willems, L.; Spriet, I.; Coropciuc, R.; Politis, C.; Vandeweyer, R.O.; et al. Incidence of medication-related osteonecrosis of the jaw in patients treated with both bone resorption inhibitors and vascular endothelial growth factor receptor tyrosine kinase inhibitors. Support Care Cancer 2018, 26, 869–878. [Google Scholar] [CrossRef]
- Hernandez, M.; Phulpin, B.; Mansuy, L.; Droz, D. Use of new targeted cancer therapies in children: Effects on dental development and risk of jaw osteonecrosis: A review. J. Oral Pathol. Med. 2017, 46, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw-2014 Update. J. Oral Maxil. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Yuh, D.Y.; Chang, T.H.; Huang, R.Y.; Chien, W.C.; Lin, F.G.; Fu, E. The national-scale cohort study on bisphosphonate-related osteonecrosis of the jaw in Taiwan. J. Dent. 2014, 42, 1343–1352. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Rhee, Y.; Kwon, Y.D.; Kwon, T.G.; Lee, J.K.; Kim, D.Y. Medication Related Osteonecrosis of the Jaw: 2015 Position Statement of the Korean Society for Bone and Mineral Research and the Korean Association of Oral and Maxillofacial Surgeons. J. Bone Metab. 2015, 22, 151–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svejda, B.; Muschitz, C.; Gruber, R.; Brandtner, C.; Svejda, C.; Gasser, R.W.; Santler, G.; Dimai, H.P. Position paper on medication-related osteonecrosis of the jaw (MRONJ). Wien. Med. Wochenschr. 2016, 166, 68–74. [Google Scholar] [CrossRef]
- Japanese Allied Committee on Osteonecrosis of the Jaw; Yoneda, T.; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2017, 35, 6–19. [Google Scholar] [CrossRef]
- Muller, F.; Shimazaki, Y.; Kahabuka, F.; Schimmel, M. Oral health for an ageing population: The importance of a natural dentition in older adults. Int. Dent. J. 2017, 67, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, K.; Hayashida, S.; Rokutanda, S.; Kawakita, A.; Soutome, S.; Sawada, S.; Yanamoto, S.; Kojima, Y.; Umeda, M. Surgical strategy for medication-related osteonecrosis of the jaw (MRONJ) on maxilla: A multicenter retrospective study. J. Dent. Sci. 2021, 16, 885–890. [Google Scholar] [CrossRef]
- Park, J.H.; Alfafara, A.M.; Park, Y.L.; Bae, J.H.; Kim, S.J. Medication-related osteonecrosis of the maxilla: Prognosis of oral surgery combined with endoscopic sinus surgery. Oral Dis. 2020, 27, 962–969. [Google Scholar] [CrossRef]
- Ohta, K.; Yoshimura, H. Medication-Related Osteonecrosis of the Jaw. Am. J. Med. Sci. 2020, 360, 316–317. [Google Scholar] [CrossRef]
- Giovannacci, I.; Vescovi, P.; Magnoni, C.; Corradi, D.; Corcione, L.; Lucchina, A.G.; Mortellaro, C.; Nammour, S.; Meleti, M. Auto-Fluorescence and Histopathologic Evaluation of Medication-Related Osteonecrosis of the Jaws: Perspectives for Treatment. J. Craniofac. Surg. 2019, 30, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Aljohani, S.; Troeltzsch, M.; Hafner, S.; Kaeppler, G.; Mast, G.; Otto, S. Surgical treatment of medication-related osteonecrosis of the upper jaw: Case series. Oral Dis. 2019, 25, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Procacci, P.; Albanese, M.; Trevisiol, L.; Favero, V.; Bertossi, D.; Lonardi, F.; D’Agostino, A.; Manfrin, E.; Nocini, P.F. Medication-related osteonecrosis of the posterior maxilla: Surgical treatment using a combined transnasal endoscopic and intraoral approach, our experience with seven consecutive patients. Clin. Otolaryngol. 2018, 43, 685–691. [Google Scholar] [CrossRef]
- Voss, P.J.; Vargas Soto, G.; Schmelzeisen, R.; Izumi, K.; Stricker, A.; Bittermann, G.; Poxleitner, P. Sinusitis and oroantral fistula in patients with bisphosphonate-associated necrosis of the maxilla. Head Face Med. 2016, 12, 3. [Google Scholar] [CrossRef] [Green Version]
- Melville, J.C.; Tursun, R.; Shum, J.W.; Young, S.; Hanna, I.A.; Marx, R.E. A technique for the treatment of oral-antral fistulas resulting from medication-related osteonecrosis of the maxilla: The combined buccal fat pad flap and radical sinusotomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Yoshiga, D.; Sasaguri, M.; Matsuo, K.; Kokuryou, S.; Habu, M.; Oda, M.; Kodama, M.; Tsurushima, H.; Sakaguchi, O.; Sakurai, T.; et al. Intraoperative detection of viable bone with fluorescence imaging using Visually Enhanced Lesion Scope in patients with bisphosphonate-related osteonecrosis of the jaw: Clinical and pathological evaluation. Osteoporos. Int. 2015, 26, 1997–2006. [Google Scholar] [CrossRef]
- Sadiq, Z.; Sammut, S.; Lopes, V. Non-complex reconstructive techniques in the management of BRONJ: A case series of patient-related outcomes. Oral Maxillofac. Surg. 2014, 18, 223–227. [Google Scholar] [CrossRef]
- Lee, J.J.; Cheng, S.J.; Wang, Y.P.; Jeng, J.H.; Chiang, C.P.; Kok, S.H. Osteonecrosis of the jaws associated with the use of yearly zoledronic acid: Report of 2 cases. Head Neck J. Sci Spec. 2013, 35, E6–E10. [Google Scholar] [CrossRef]
- Hewson, I.; Syme, D.; Bruscino-Raiola, F. Radical surgical treatment of bisphosphonate related osteonecrosis of the jaw. Aust. Dent. J. 2012, 57, 227–230. [Google Scholar] [CrossRef] [Green Version]
- Wilde, F.; Heufelder, M.; Winter, K.; Hendricks, J.; Frerich, B.; Schramm, A.; Hemprich, A. The role of surgical therapy in the management of intravenous bisphosphonates-related osteonecrosis of the jaw. Oral Surg. Oral Med. O 2011, 111, 153–163. [Google Scholar] [CrossRef]
- Maurer, P.; Sandulescu, T.; Kriwalsky, M.S.; Rashad, A.; Hollstein, S.; Stricker, I.; Holzle, F.; Kunkel, M. Bisphosphonate-related osteonecrosis of the maxilla and sinusitis maxillaris. Int. J. Oral Maxillofac. Surg. 2011, 40, 285–291. [Google Scholar] [CrossRef]
- Stubinger, S.; Dissmann, J.P.; Pinho, N.C.; Saldamli, B.; Seitz, O.; Sader, R. A Preliminary Report About Treatment of Bisphosphonate Related Osteonecrosis of the Jaw With Er:YAG Laser Ablation. Laser Surg. Med. 2009, 41, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Carlson, E.R.; Basile, J.D. The role of surgical resection in the management of bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2009, 67, 85–95. [Google Scholar] [CrossRef]
- Farrugia, M.C.; Summerlin, D.J.; Krowiak, E.; Huntley, T.; Freeman, S.; Borrowdale, R.; Tomich, C. Osteonecrosis of the mandible or maxilla associated with the use of new generation bisphosphonates. Laryngoscope 2006, 116, 115–120. [Google Scholar] [CrossRef]
- Wutzl, A.; Eisenmenger, G.; Hoffmann, M.; Czerny, C.; Moser, D.; Pietschmann, P.; Ewers, R.; Baumann, A. Osteonecrosis of the jaws and bisphosphonate treatment in cancer patients. Wien. Klin. Wochenschr. 2006, 118, 473–478. [Google Scholar] [CrossRef]
- Hellstein, J.W.; Adler, R.A.; Edwards, B.; Jacobsen, P.L.; Kalmar, J.R.; Koka, S.; Migliorati, C.A.; Ristic, H.; Affa, A.D.A.C.S. Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis Executive summary of recommendations from the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2011, 142, 1243–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottesen, C.; Schiodt, M.; Gotfredsen, K. Efficacy of a high-dose antiresorptive drug holiday to reduce the risk of medication-related osteonecrosis of the jaw (MRONJ): A systematic review. Heliyon 2020, 6, e03795. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Kawakita, A.; Ueda, N.; Funahara, R.; Tachibana, A.; Kobayashi, M.; Kondou, E.; Takeda, D.; Kojima, Y.; Sato, S.; et al. A multicenter retrospective study of the risk factors associated with medication-related osteonecrosis of the jaw after tooth extraction in patients receiving oral bisphosphonate therapy: Can primary wound closure and a drug holiday really prevent MRONJ? Osteoporos Int. 2017, 28, 2465–2473. [Google Scholar] [CrossRef]
- Jung, S.Y.; Suh, H.S.; Park, J.W.; Kwon, J.W. Drug holiday patterns and bisphosphonate-related osteonecrosis of the jaw. Oral Dis. 2019, 25, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Lee, H.K.; Song, S.I.; Lee, J.K. Drug holiday as a prognostic factor of medication-related osteonecrosis of the jaw. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 206–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, M.H.; Lee, D.K.; Kim, C.W.; Song, I.S.; Jun, S.H. Clinical characteristics and recurrence-related factors of medication-related osteonecrosis of the jaw. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Di Fede, O.; Panzarella, V.; Mauceri, R.; Fusco, V.; Bedogni, A.; Lo Muzio, L.; Sipmo Onj, B.; Campisi, G. The Dental Management of Patients at Risk of Medication-Related Osteonecrosis of the Jaw: New Paradigm of Primary Prevention. Biomed. Res. Int. 2018. [Google Scholar] [CrossRef]
- Hasegawa, T.; Ueda, N.; Yamada, S.I.; Kato, S.; Iwata, E.; Hayashida, S.; Kojima, Y.; Shinohara, M.; Tojo, I.; Nakahara, H.; et al. Denosumab-related osteonecrosis of the jaw after tooth extraction and the effects of a short drug holiday in cancer patients: A multicenter retrospective study. Osteoporos Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nicolatou-Galitis, O.; Schiodt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Niepel, D.; Van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ristow, O.; Otto, S.; Troeltzsch, M.; Hohlweg-Majert, B.; Pautke, C. Treatment perspectives for medication-related osteonecrosis of the jaw (MRONJ). J. Craniomaxillofac. Surg. 2015, 43, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Vescovi, P.; Giovannacci, I.; Merigo, E.; Meleti, M.; Manfredi, M.; Fornaini, C.; Nammour, S. Tooth extractions in high-risk patients under bisphosphonate therapy and previously affected with osteonecrosis of the jaws: Surgical protocol supported by low-level laser therapy. J. Craniofac. Surg. 2015, 26, 696–699. [Google Scholar] [CrossRef]
- Min, S.H.; Kang, N.E.; Song, S.I.; Lee, J.K. Regenerative effect of recombinant human bone morphogenetic protein-2/absorbable collagen sponge (rhBMP-2/ACS) after sequestrectomy of medication-related osteonecrosis of the jaw (MRONJ). J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 191–196. [Google Scholar] [CrossRef]
- de Souza Tolentino, E.; de Castro, T.F.; Michellon, F.C.; Passoni, A.C.C.; Ortega, L.J.A.; Iwaki, L.C.V.; da Silva, M.C. Adjuvant therapies in the management of medication-related osteonecrosis of the jaws: Systematic review. Head Neck 2019, 41, 4209–4228. [Google Scholar] [CrossRef]
- Kojima, Y.; Kawaoka, Y.; Sawada, S.; Hayashida, S.; Okuyama, K.; Yutori, H.; Kawakita, A.; Ishida, S.; Soutome, S.; Yanamoto, S.; et al. Clinical significance of periosteal reaction as a predictive factor for treatment outcome of medication-related osteonecrosis of the jaw. J. Bone Minar. Metab. 2019, 37, 913–919. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maxillary MRONJ (n = 314) | ||
|---|---|---|
| n | (%) a | |
| Gender | ||
| Males | 79 | (25.2%) |
| Females | 206 | (65.6%) |
| NA | 29 | (9.2%) |
| Age (years), mean ± SD | 70.6 ± 5.5 | |
| Osteonecrosis location | ||
| Maxilla | 313 | (99.7%) |
| Maxilla + mandible | 1 | (0.3%) |
| Stage b | ||
| 0 | 6 | (1.9%) |
| I | 19 | (6.1%) |
| II | 108 | (34.4%) |
| III | 137 | (43.6%) |
| NA | 44 | (14%) |
| Treatment | ||
| Surgery alone | 132 | (42.0%) |
| Surgery combined adjuvant therapy | 182 | (58.0%) |
| Disease history | ||
| Osteoporosis | 110 | (35.1%) |
| Breast cancer | 63 | (20.1%) |
| Multiple myeloma | 47 | (15.0%) |
| Prostate cancer | 16 | (5.1%) |
| Lung cancer | 2 | (0.6%) |
| Renal cancer | 2 | (0.6%) |
| Cervical cancer | 1 | (0.3%) |
| Thyroid cancer | 1 | (0.3%) |
| Rectal cancer | 1 | (0.3%) |
| Leukemia | 1 | (0.3%) |
| Other malignancies | 13 | (4.1%) |
| NA | 57 | (18.2%) |
| Drugs | ||
| Bisphosphonates | ||
| Zoledronate | 112 | (35.6%) |
| Alendronate | 32 | (10.2%) |
| Ibandronate | 19 | (6.1%) |
| Risedronate | 10 | (3.2%) |
| Pamidronate | 9 | (2.9%) |
| Zoledronate combined other drugs | 9 | (2.9%) |
| NA | 57 | (18.2%) |
| Non bisphosphonates | ||
| Denosumab or denosumab combined with other drugs | 36 | (11.4%) |
| NA | 30 | (9.5%) |
| Duration of drug exposure (months), mean ± SD | 50.0 ± 20.1 | |
| Follow up time of post treatment (months), mean ± SD | 8.4 ± 6.6 | |
| Treatment effectiveness | ||
| Wound complete healing | 270 | (86%) |
| Impaired wound healing or recurrence | 44 | (14%) |
| Author [Ref]/Country (Year) | Study Design (n) | M (N)/F (N) Age (Years): Mean ± SD (Min.-Max.) | Therapy | Disease (n) | Drugs (n) | Treatment Outcome |
|---|---|---|---|---|---|---|
| Okuyama et al. [18]/Japan (2021) | Multiple center Case series (n = 54) | M (17)/F (37) Age: 73 (48–89) | Resection alone (n = 54) | Osteoporosis (n = 28) Cancer (n = 26) | Bisphosphonates (n = 34) Denosumab (n = 20) | No recurrence (n= 46) Residual necrotic bone (n = 8) |
| Park et al. [19]/Korea (2020) | Case series (n = 62) | M (10)/F (52) Age: 72.1 ± 11.3 (43–92) | Resection alone (n = 9) Resection + PRF (n = 19) Resection + PRF + BMP (n = 34) | Osteoporosis (n = 46) Breast cancer (n = 10) Multiple myeloma (n = 5) Cervical cancer (n = 1) | Alendronate (n = 27) Risedronate (n = 8) Pamidronate (n = 4) Ibandronate (n = 11) Zolendronate (n = 9) Others (n = 3) | Resection: Resolution (n = 5)/ No resolution (n = 4) Resection + PRF: Resolution (n = 14)/ No resolution (n = 5) Resection + PRF + BMP: Resolution (n = 30)/ No resolution (n = 4) |
| Ohta et al. [20]/Japan (2020) | Case report (n = 1) | M (1) Age: 79 | Resection alone (n = 1) | Bone metastatic prostate cancer | Zolendronate + denosumab | No recurrence/ No complications |
| Giovannacci et al. [21]/Italy (2019) | Case report (n = 1) | F (1) Age: 80 | Resection + auto-fluorescence + LLLT | Breast cancer | Denosumab | No recurrence No complications |
| Aljohani et al. [22]/Germany (2019) | Case series (n = 72) | M (26)/F (46) Age: 72 ± 9.6 | Resection (n = 32) Resection + BPF (n = 14) Resection + fluorescence guided (n = 5) | Breast cancer (n = 28) Multiple myeloma (n = 15) Prostate cancer (n = 10) Osteoporosis (n = 6) Others (n = 13) | Zoledronate (n = 45) Pamidronate (n = 1) Ibandronate (n = 3) Combination of bisphosphonates (n = 10) Denosumab (n = 4) Zoledronate and denosumab (n = 7) Denosumab and ibandronate (n = 1) Denosumab, zoledronate, pamidronate (n = 1) | No recurrence in 82.2% (65/79) of the lesions |
| Procacci et al. [23]/Italy (2018) | Case series (n = 7) | M (1)/F (6) Age: 66 ± 10.6 (51–79) | Resection + BPF (n = 7) | Breast cancer (n = 2) Osteoporosis + rheumatoid arthritis (n = 2) Leukaemia (n = 1) Severe osteoporosis (n = 2) | Zoledronate (n = 3) Risedronate (n = 2) Denosumab (n = 1) Risedronate (n = 1) | No recurrence No complications |
| Voss et al. [24]/Germany (2016) | Case series study (n = 12) | M (2)/F (10) Age: 67.0 (55–62) | Resection (n = 12) | Breast cancer (n = 5) Multiple myeloma (n = 5) Lung cancer (n = 1) Osteoporosis (n = 1) | Bisphosphonate: Zoledronate (n = 5) Pamidronate (n = 3) Ibandronate (n = 2) Alendronate (n = 1) Clodronate (n = 1) | No recurrence (n = 11) Recurrence (n = 1) |
| Melville et al. [25]/USA (2016) | Case series (n = 23) | M (3)/F(20) Age = 68.3 ± 12.3 | Resection + BFP (n = 5) Resection + BFP + PRP (n = 18) | Osteoporosis (n = 23) | Zoledronate (n = 19) Zoledronate and avastin (n = 1) Alendronate and ibandronate (n = 1) Alendronate (n = 1) Denosumab (n = 1) | No recurrence (n = 23) |
| Yoshiga et al. [26]/Japan 2015 | Case series (n = 4) | F (4) Age: 69.8 ± 11.2 (58–85) | Resection (n = 4) | Osteoporosis (n = 1); Breast cancer (n = 3) | Bisphosphonate (oral) (n = 1)/120 Bisphosphonate (IV) (n = 3)/ | No recurrence (n = 4) |
| Sadiq et al. [27]/UK (2014) | Case series (n = 1) | F (1) Age = 83 | Resection (n = 1) | Osteoporosis | Alendronate Bendroflumethiazide Enalapril | No recurrence (n = 1) |
| Lee et al. [28]/Taiwan (2013) | Case series (n = 1) | F (1) Age = 76 | Resection (n = 1) | Osteoporosis | Zoledronate | No recurrence (n = 1) |
| Hewson et al. [29]/Australia (2012) | Case series (n = 1) | F (1) Age = 64 | Resection (n = 1) | Multiple myeloma | Pamidronate + zoledronate | No recurrence (n = 1) |
| Wilde et al. [30]/Germany (2011) | Case series (n = 12) | M (4)/F (8) Age = (48–93) | Resection +BFP | Multiple myeloma (n = 3)Breast cancer (n = 5) Prostate cancer (n = 3); Thyroid cancer (n = 1) | Zolendronate (n = 6) Zolendronate + bondronate (n = 2) Zolendronate + pamindronate (n = 2) Zolendronate + pamindronate + bondronate (n = 2) | No recurrence (n = 10) Recurrence (n = 2) |
| Maurer et al. [31]/Germany (2011) | Case series (n = 21) | M (5)/F (16) Age: 69.0 ± 10.2 (48–91) | Resection | Breast cancer (n = 6) Multiple myeloma (n = 8) Osteoporosis (n = 3) Lung cancer (n = 1) Prostate cancer (n = 1) Rectal cancer (n = 1) Renal cancer (n = 1) | Alendronate (n = 3)/ibandronate (n = 3)/zoledronate (n = 15)/ | No recurrence (n = 15) Recurrence (n = 6) |
| Stubinger et al. [32]/Slovenia (2009) | Case series (n = 4) | M (3)/F (1) Age: 70.0 ± 9.6 (56–77) | Resection + Er:YAG laser ablation | Prostate cancer (n = 1) Myeloma (n = 2) Renal cell carcinoma (n = 1) | Zoledronate (n = 4) | No recurrence (n = 4) |
| Carlson and Basile [33]/USA (2009) | Case series (n = 29) | NA | Resection (n = 29) | Breast cancer Multiple myeloma Prostate cancer Osteoporosis Other malignancies | Alendronate Risedronate Zoledronate Pamidronate | No recurrence (n = 29) |
| Farrugia et al. [34]/USA (2006) | Case series (n = 10) | NA | Resection | Breast cancer (n = 3) Multiple myeloma (n = 5) Paget’s disease (n = 1) Osteoporosis (n = 1) | Pamidronate + zoledronate | No recurrence (n = 1) |
| Wutzl et al. [35]/Austria (2006) | Case series (n = 8) | M (5)/F (3) Age: 66 ± 9 (51–76) | Resection (n = 7) Refused surgery (n = 1) | Breast cancer (n = 3) Multiple myeloma (n = 5) | Zoledronate (n = 5) Pamidronate (n = 1) Pamidronate/zoledronate (n = 2) | No recurrence (n = 7) Recurrence (n = 1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, K.-J.; Hsiao, S.-Y.; Chen, P.-H.; Chen, H.-S.; Chen, C.-M. Investigation of the Effectiveness of Surgical Treatment on Maxillary Medication-Related Osteonecrosis of the Jaw: A Literature Review. J. Clin. Med. 2021, 10, 4480. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194480
Hsu K-J, Hsiao S-Y, Chen P-H, Chen H-S, Chen C-M. Investigation of the Effectiveness of Surgical Treatment on Maxillary Medication-Related Osteonecrosis of the Jaw: A Literature Review. Journal of Clinical Medicine. 2021; 10(19):4480. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194480
Chicago/Turabian StyleHsu, Kun-Jung, Szu-Yu Hsiao, Ping-Ho Chen, Han-Sheng Chen, and Chun-Ming Chen. 2021. "Investigation of the Effectiveness of Surgical Treatment on Maxillary Medication-Related Osteonecrosis of the Jaw: A Literature Review" Journal of Clinical Medicine 10, no. 19: 4480. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10194480