
Impact of Daily Bedside Echocardiographic Assessment on Readmissions in Acute Heart Failure: A Randomized Clinical Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Oversight
2.2. Study Design
2.3. Outcomes
2.4. Statistical Analysis
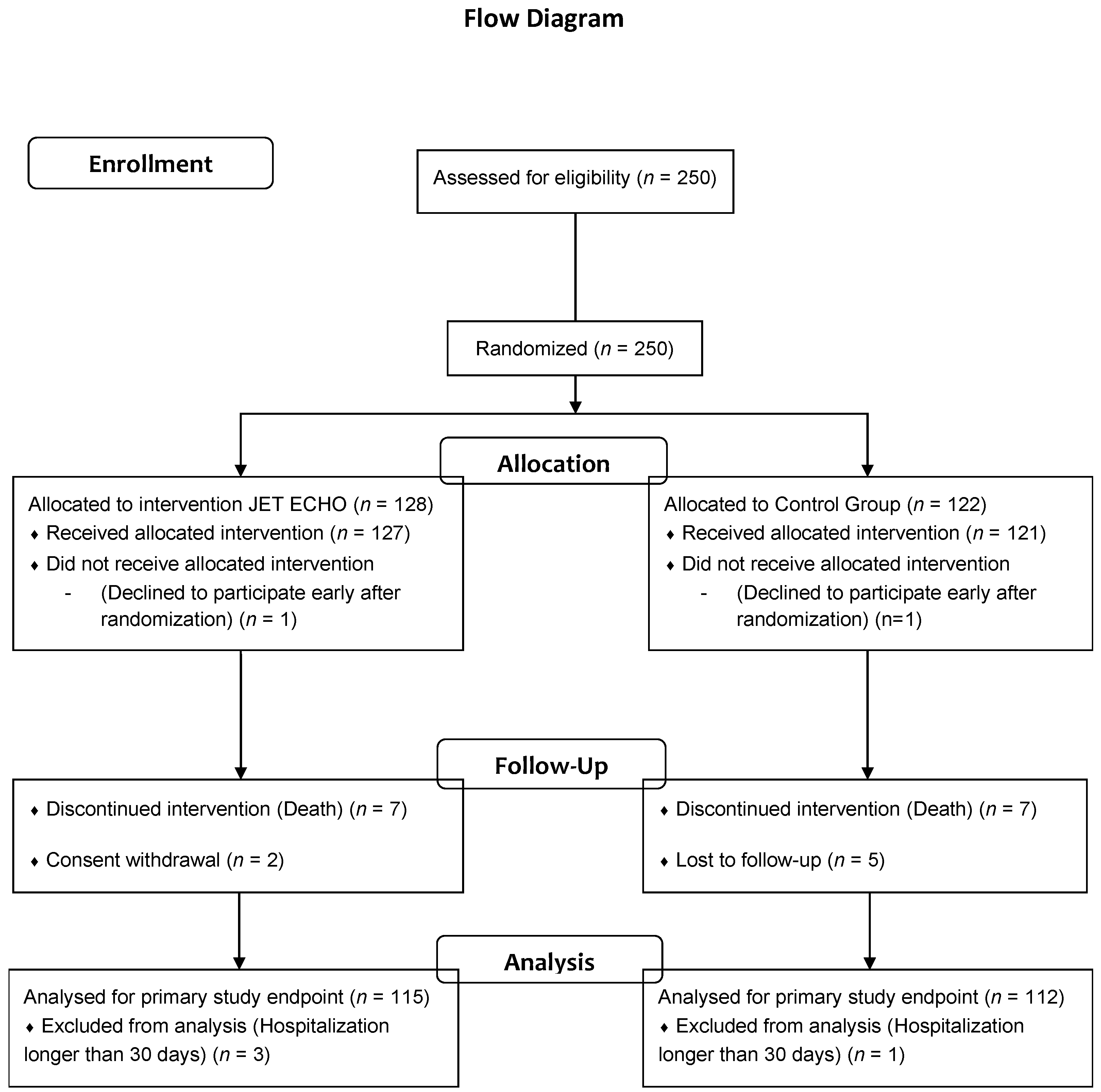
3. Results
3.1. Primary Endpoint: Readmission Rate for HF at Day 30
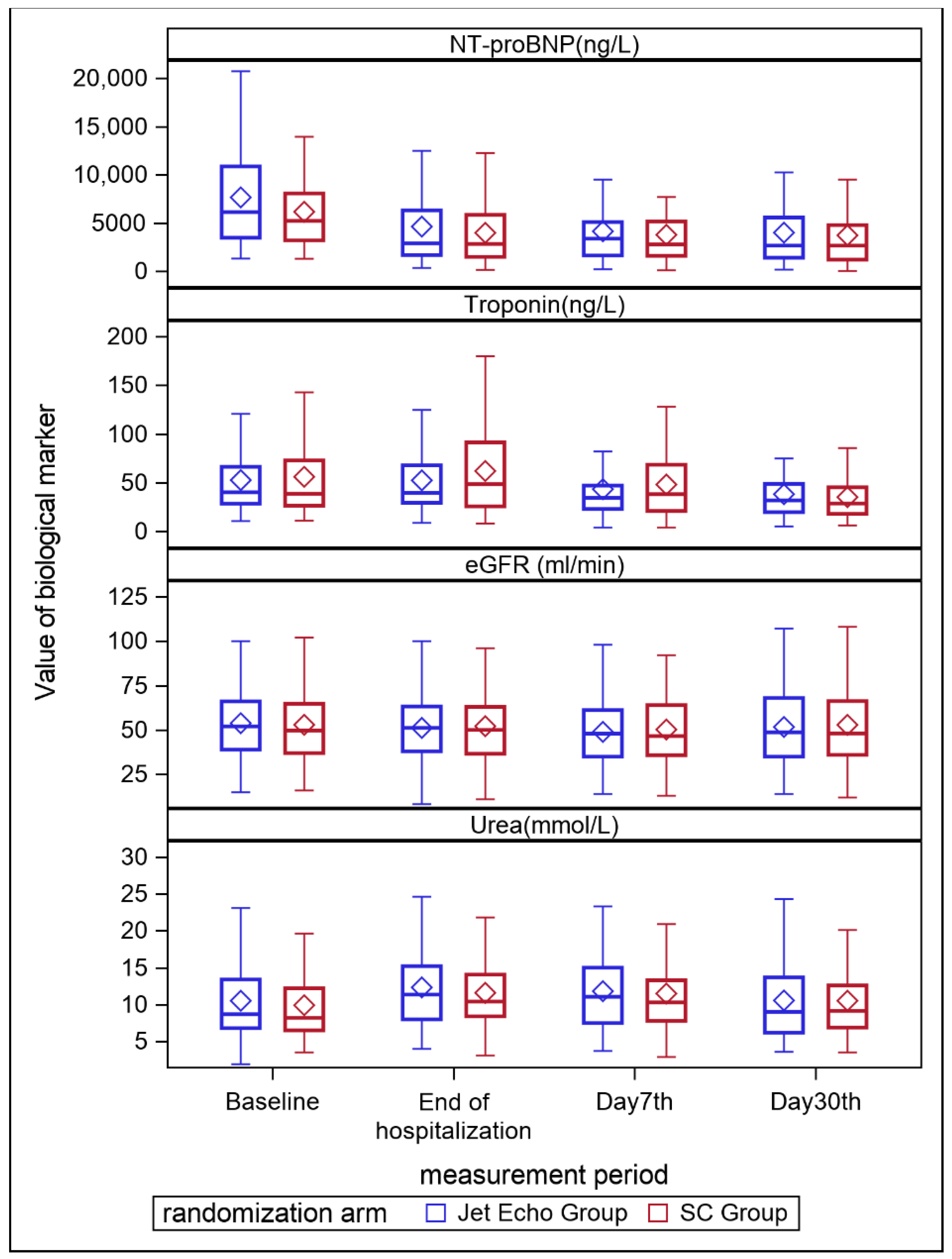
3.2. Secondary Outcomes
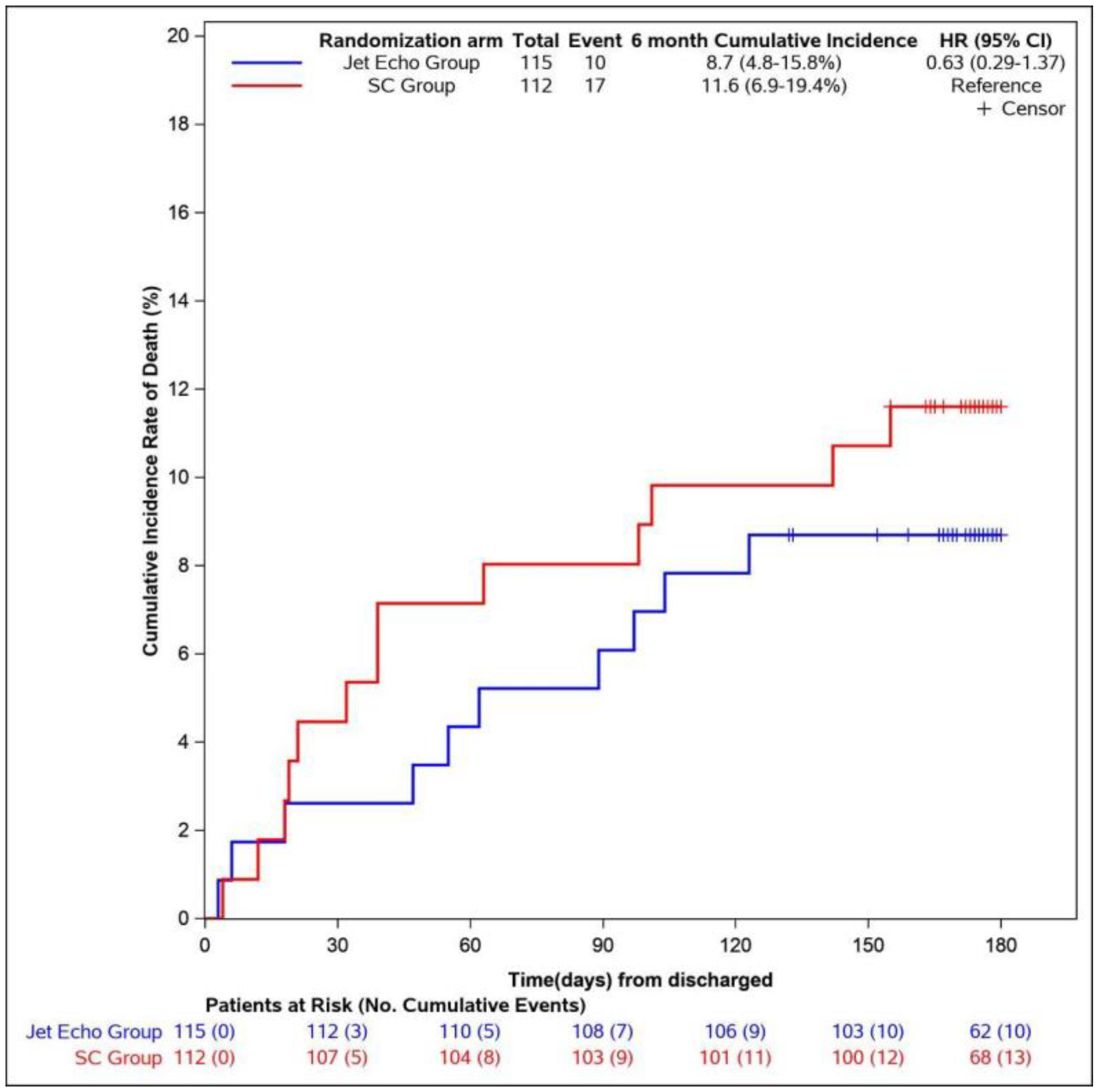
3.3. Six-Month Mortality
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| End of Hospitalization Treatment Target Dose% ± Se | Jet Echo N = 115 | Standard Care N = 112 | Mean Difference | p-Value |
|---|---|---|---|---|
| Beta-blockers | ||||
| Weighted Mean ± Se | 48.1 ± 7.5 | 41.5 ± 10.6 | 6.7 ± 7.6 | 0.4 |
| ACE-I/ARB/ARNI | ||||
| Weighted Mean ± Se | 50.2 ± 9.4 | 43.82± 6.0 | 6.39 ± 11.11 | 0.6 |
| MRA | ||||
| Weighted Mean ± Se | 52.4 ± 6.3 | 49.5 ± 3.0 | 2.9 ± 7.0 | 0.7 |
| Diuretics * | ||||
| Mean ± Se | 144.7 ± 15.1 | 116.7 ± 12.5 | 28.0 ± 19.6 | 0.3 |
References
- Van Riet, E.E.S.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.J.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Tuppin, P.; Cuerq, A.; de Peretti, C.; Fagot-Campagna, A.; Danchin, N.; Juillière, Y.; Alla, F.; Allemand, H.; Bauters, C.; Drici, M.D.; et al. Two-year outcome of patients after a first hospitalization for heart failure: A national observational study. Arch. Cardiovasc. Dis. 2014, 107, 158–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet Lond. Engl. 2018, 391, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Nohria, A.; Tsang, S.W.; Fang, J.C.; Lewis, E.F.; Jarcho, J.A.; Mudge, G.H.; Stevenson, L.W. Clinical assessment identifies hemodynamic profiles that predict outcomes in patients admitted with heart failure. J. Am. Coll. Cardiol. 2003, 41, 1797–1804. [Google Scholar] [CrossRef] [Green Version]
- Lucas, C.; Johnson, W.; Hamilton, M.A.; Fonarow, G.C.; Woo, M.A.; Flavell, C.M.; Creaser, J.A.; Stevenson, L.W. Freedom from congestion predicts good survival despite previous class IV symptoms of heart failure. Am. Heart J. 2000, 140, 840–847. [Google Scholar] [CrossRef]
- Smith, G.L.; Lichtman, J.H.; Bracken, M.B.; Shlipak, M.G.; Phillips, C.O.; DiCapua, P.; Krumholz, H.M. Renal impairment and outcomes in heart failure: Systematic review and meta-analysis. J. Am. Coll. Cardiol. 2006, 47, 1987–1996. [Google Scholar] [CrossRef] [Green Version]
- Mullens, W.; Damman, K.; Testani, J.M.; Martens, P.; Mueller, C.; Lassus, J.; Tang, W.W.; Skouri, H.; Verbrugge, F.H.; Orso, F.; et al. Evaluation of kidney function throughout the heart failure trajectory-a position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 584–603. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Stienen, S.; Salah, K.; Moons, A.H.; Bakx, A.L.; van Pol, P.; Kortz, R.A.M.; Ferreira, J.P.; Marques, I.; Schroeder-Tanka, J.M.; Keijer, J.T.; et al. NT-proBNP (N-Terminal pro-B-Type Natriuretic Peptide)-Guided Therapy in Acute Decompensated Heart Failure: PRIMA II Randomized Controlled Trial (Can NT-ProBNP-Guided Therapy During Hospital Admission for Acute Decompensated Heart Failure Reduce Mortality and Readmissions?). Circulation 2018, 137, 1671–1683. [Google Scholar]
- Lei, J.; Dhamoon, A.S.; Wang, J.; Iannuzzi, M.; Liu, K. Walking the tightrope: Using quantitative Doppler echocardiography to optimize ventricular filling pressures in patients hospitalized for acute heart failure. Eur. Heart J. Acute Cardiovasc. Care. 2016, 5, 130–140. [Google Scholar] [CrossRef]
- Vitarelli, A.; Gheorghiade, M. Transthoracic and transesophageal echocardiography in the hemodynamic assessment of patients with congestive heart failure. Am. J. Cardiol. 2000, 86, 36–40. [Google Scholar] [CrossRef]
- Goonewardena, S.N.; Spencer, K.T. Handcarried echocardiography to assess hemodynamics in acute decompensated heart failure. Curr. Heart Fail. Rep. 2010, 7, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.T.Q.; Ho, J.E.; Ho, C.Y.; Givertz, M.M.; Stevenson, L.W. Handheld echocardiography offers rapid assessment of clinical volume status. Am. Heart J. 2008, 156, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef] [PubMed]
- Ricci, J.-E.; Kalmanovich, E.; Robert, C.; Chevallier, T.; Aguilhon, S.; Solecki, K.; Akodad, M.; Cornillet, L.; Cayla, G.; Lattuca, B.; et al. Management of acute heart failure: Contribution of daily bedside echocardiographic assessment on therapy adjustment with impact measure on the 30-day readmission rate (JECICA). Contemp. Clin. Trials. Commun. 2018, 12, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Rohde, L.E.; Palombini, D.V.; Polanczyk, C.A.; Goldraich, L.A.; Clausell, N. A hemodynamically oriented echocardiography-based strategy in the treatment of congestive heart failure. J. Card. Fail. 2007, 13, 618–625. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; Strickland, W.; Neelagaru, S.; Raval, N.; Krueger, S.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: A randomised controlled trial. Lancet Lond. Engl. 2011, 377, 658–666. [Google Scholar] [CrossRef]
- Binanay, C.; Califf, R.M.; Hasselblad, V.; O’Connor, C.M.; Shah, M.R.; Sopko, G.; Stevenson, L.W.; Francis, G.S.; Leier, C.V.; Miller, L.W. Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: The ESCAPE trial. JAMA 2005, 294, 1625–1633. [Google Scholar]
- Öhman, J.; Harjola, V.-P.; Karjalainen, P.; Lassus, J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. 2018, 5, 120–128. [Google Scholar] [CrossRef]
- Metra, M.; Teerlink, J.R.; Cotter, G.; Davison, B.A.; Felker, G.M.; Filippatos, G.; Filippatos, G.; Greenberg, B.H.; Pang, P.S.; Ponikowski, P.; et al. Effects of Serelaxin in Patients with Acute Heart Failure. N. Engl. J. Med. 2019, 381, 716–726. [Google Scholar] [CrossRef]
- Packer, M.; O’Connor, C.; McMurray, J.J.V.; Wittes, J.; Abraham, W.T.; Anker, S.D.; Dickstein, K.; Filippatos, G.; Holcomb, R.; Krum, H.; et al. Effect of Ularitide on Cardiovascular Mortality in Acute Heart Failure. N. Engl. J. Med. 2017, 376, 1956–1964. [Google Scholar] [CrossRef] [PubMed]
- Jencks, S.F.; Williams, M.V.; Coleman, E.A. Rehospitalizations among patients in the Medicare fee-for-service program. N. Engl. J. Med. 2009, 360, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.J.; Fonarow, G.C.; Vaduganathan, M.; Khan, S.S.; Butler, J.; Gheorghiade, M. The vulnerable phase after hospitalization for heart failure. Nat. Rev. Cardiol. 2015, 12, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Bonow, R.O.; Gheorghiade, M. Thirty-day readmissions: The clock is ticking. JAMA. 2013, 309, 345–346. [Google Scholar] [CrossRef]
- Eapen, Z.J.; Reed, S.D.; Li, Y.; Kociol, R.D.; Armstrong, P.W.; Starling, R.C.; McMurray, J.J.; Massie, B.M.; Swedberg, K.; Ezekowitz, J.A.; et al. Do countries or hospitals with longer hospital stays for acute heart failure have lower readmission rates? Findings from ASCEND-HF. Circ. Heart Fail. 2013, 6, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, F.; Packer, M.; Coats, A.J.S.; Fowler, M.B.; Krum, H.; Mohacsi, P.; Rouleau, J.L.; Tendera, M.; Castaigne, A.; Anker, S.D.; et al. Prognostic impact of plasma N-terminal pro-brain natriuretic peptide in severe chronic congestive heart failure: A substudy of the Carvedilol Prospective Randomized Cumulative Survival (COPERNICUS) trial. Circulation 2004, 110, 1780–1786. [Google Scholar] [CrossRef] [Green Version]
- Fonarow, G.C.; Peacock, W.F.; Phillips, C.O.; Givertz, M.M.; Lopatin, M.; ADHERE Scientific Advisory Committee and Investigators. Admission B-type natriuretic peptide levels and in-hospital mortality in acute decompensated heart failure. J. Am. Coll. Cardiol. 2007, 49, 1943–1950. [Google Scholar] [CrossRef] [Green Version]
- Iglesias-Garriz, I.; Olalla-Gómez, C.; Garrote, C.; López-Benito, M.; Martín, J.; Alonso, D.; Rodríguez, M.A. Contribution of right ventricular dysfunction to heart failure mortality: A meta-analysis. Rev. Cardiovasc. Med. 2012, 13, e62–e69. [Google Scholar] [CrossRef]
- Uthamalingam, S.; Kandala, J.; Selvaraj, V.; Martin, W.; Daley, M.; Patvardhan, E.; Capodilupo, R.; Moore, S.; Januzzi, J.L., Jr. Outcomes of patients with acute decompensated heart failure managed by cardiologists versus noncardiologists. Am. J. Cardiol. 2015, 115, 466–471. [Google Scholar] [CrossRef]
- Ziaeian, B.; Fonarow, G.C. The Prevention of Hospital Readmissions in Heart Failure. Prog. Cardiovasc. Dis. 2016, 58, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur. J. Heart Fail. 2015, 17, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Pellicori, P.; Platz, E.; Dauw, J.; Ter Maaten, J.M.; Martens, P.; Pivetta, E.; Cleland, J.G.; McMurray, J.J.; Mullens, W.; Solomon, S.D.; et al. Ultrasound imaging of congestion in heart failure: Examinations beyond the heart. Eur. J. Heart Fail. 2021, 23, 703–712. [Google Scholar] [CrossRef] [PubMed]



| N(%) or Median (q1;q3) | Jet Echo N = 127 | Standard Care N = 121 | p-Value * |
|---|---|---|---|
| Baseline characteristics | |||
| Age at inclusion (y) | 75 (66;82) | 76 (64;84) | 0.57 |
| Female | 38 (30%) | 36 (30%) | 0.98 |
| BMI (q1;q3) | 27.05 (24.2;30.7) | 27.35 (24.1;31.1) | 0.66 |
| Hypertension | 83 (65%) | 85 (70%) | 0.41 |
| Diabetes | 54 (43%) | 43 (36%) | 0.26 |
| Smoker | 17 (13%) | 23 (19%) | 0.23 |
| Atrial fibrillation | 45 (35%) | 53 (44%) | 0.32 |
| Ischemic Cardiomyopathy | 53 (42%) | 52 (43%) | 1.00 |
| Clinical parameters | |||
| NYHA functional class | 0.90 | ||
| stage (I, II) | 7 (5%) | 5(4%) | |
| stage III | 33 (26%) | 33 (28%) | |
| stage IV | 87 (69%) | 82 (68%) | |
| Sinus Rhythm | 85 (67%) | 61 (50%) | 0.01 |
| Heart rate (bpm) | 87 (72;106) | 82 (72;102) | 0.22 |
| SBP (mmHg) | 126 (112;141) | 125 (110;139) | 0.52 |
| DBP (mmHg) | 75 (67;89) | 76 (67;86) | 0.52 |
| LVEF (%) | 0.81 | ||
| <40% | 97(76%) | 94 (78%) | |
| 40–49% | 30 (24%) | 27 (22%) | |
| Types of HF | 0.53 | ||
| Global | 68 (54%) | 71 (59%) | |
| Right | 6 (5%) | 3 (2%) | |
| Left | 53 (42%) | 47 (39%) | |
| Laboratory | |||
| Nt-proBNP (ng/L) | 6460 (3551;12,336) | 6099 (3335.5;12,457) | 0.55 |
| Troponin (ng/L) | 51.7 (32;184.1) | 43.9 (27.7;101.8) | 0.22 |
| eGFR (ml/min) | 52 (39;66.1) | 50 (37;66) | 0.76 |
| BUN (mmol/L) | 9 (6.8;13.8) | 8.3 (6.5;13.2) | 0.55 |
| Natremia (mM) | 140 (137;143) | 141 (138;143) | 0.42 |
| Kaliemia (mM) | 4.2 (3.8;4.6) | 4.1 (3.8;4.5) | 0.35 |
| Haemoglobin (g/dL) | 12.6 (11.3;14.1) | 13 (11.5;14.7) | 0.16 |
| Treatment on admission | |||
| Diuretic | 23 (18%) | 23 (19%) | 0.86 |
| Beta-blocker | 70 (55%) | 63 (52%) | 0.63 |
| ACE inhibitor | 50 (39%) | 39 (32%) | 0.24 |
| ARB | 21 (17%) | 19 (16%) | 0.86 |
| MRA | 21 (17%) | 12 (10%) | 0.13 |
| ICD | 16 (13%) | 11 (9%) | 0.41 |
| CRT | 9 (7%) | 4 (3%) | 0.25 |
| Outcomes | Jet Echo N = 115 | Standard Care N = 112 | Relative Risk or Hazard Ratio or Difference (95% CI) | p-Value |
|---|---|---|---|---|
| Primary outcome | ||||
| 30-day readmission rate for HF | 22 (19%) | 17 (15%) | 1.26 (0.70–2.24) | 0.4 |
| Secondary outcomes | ||||
| Cumulative incidence of death from any causes at 6 months | 8.7% | 11,6% | 0.63 (0.3–1.4) | 0.3 |
| Worsening HF | 17 (14%) | 24 (20%) | 0.7 (0.4–1.2) | 0.2 |
| Length of stay (days) * | 6 (4;10) | 6 (4;10) | 0 (−1–1) | 0.8 |
| Weight difference from inclusion to discharge (kg) ** | −3.22 (±5.1) | −2.83 (±4.26) | −0.40 (−1.6–0.82) | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricci, J.-E.; Aguilhon, S.; Occean, B.-V.; Soullier, C.; Solecki, K.; Robert, C.; Huet, F.; Cornillet, L.; Schmutz, L.; Chevallier, T.; et al. Impact of Daily Bedside Echocardiographic Assessment on Readmissions in Acute Heart Failure: A Randomized Clinical Trial. J. Clin. Med. 2022, 11, 2047. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072047
Ricci J-E, Aguilhon S, Occean B-V, Soullier C, Solecki K, Robert C, Huet F, Cornillet L, Schmutz L, Chevallier T, et al. Impact of Daily Bedside Echocardiographic Assessment on Readmissions in Acute Heart Failure: A Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(7):2047. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072047
Chicago/Turabian StyleRicci, Jean-Etienne, Sylvain Aguilhon, Bob-Valéry Occean, Camille Soullier, Kamila Solecki, Christelle Robert, Fabien Huet, Luc Cornillet, Laurent Schmutz, Thierry Chevallier, and et al. 2022. "Impact of Daily Bedside Echocardiographic Assessment on Readmissions in Acute Heart Failure: A Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 7: 2047. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072047