
Impact of Liver Fibrosis on Survival of Patients with Intrahepatic Cholangiocarcinoma Receiving Gemcitabine-Based Chemotherapy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database and Study Population
2.2. Statistical Analysis
3. Results
3.1. Patients and Clinical Characteristics
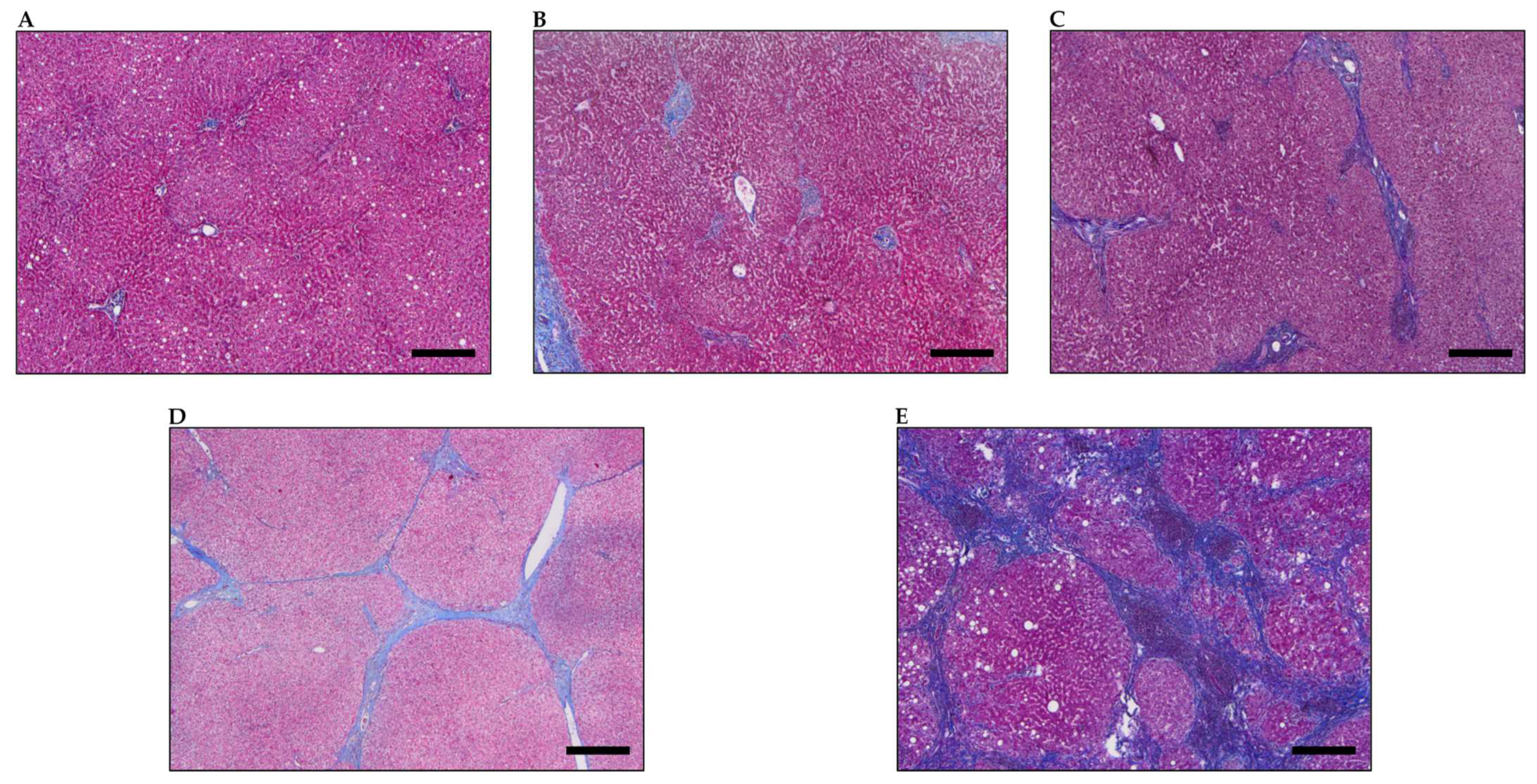
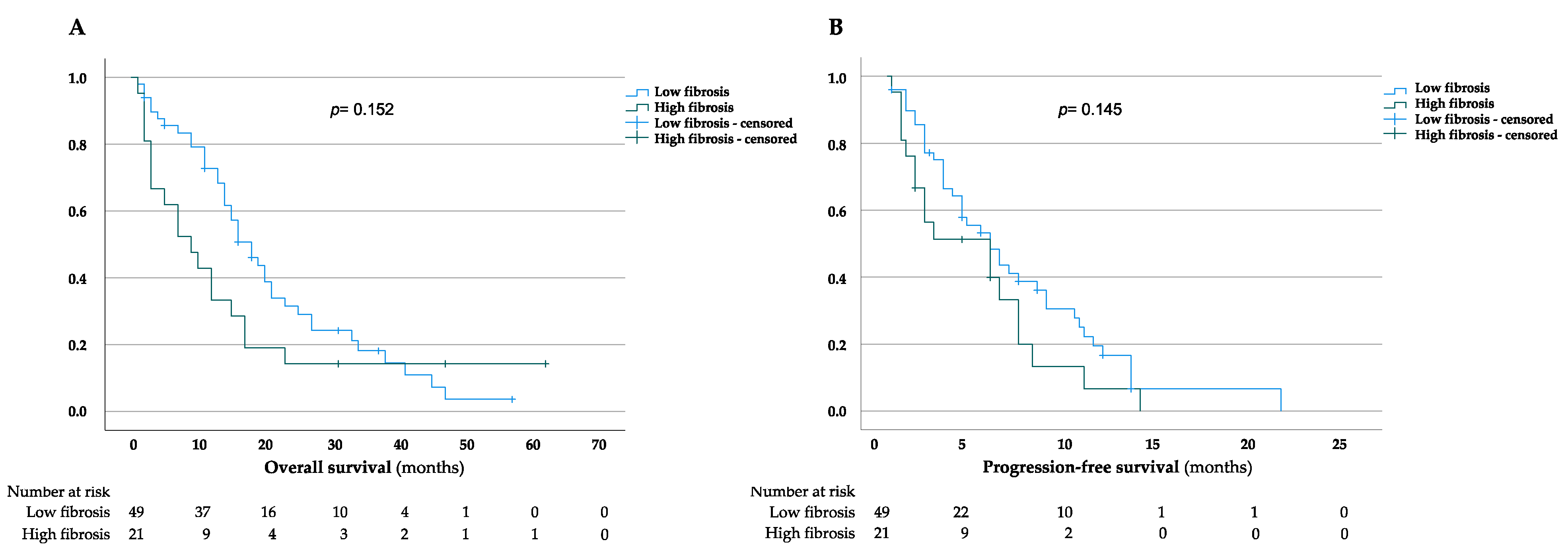
3.2. Impact of Liver Fibrosis
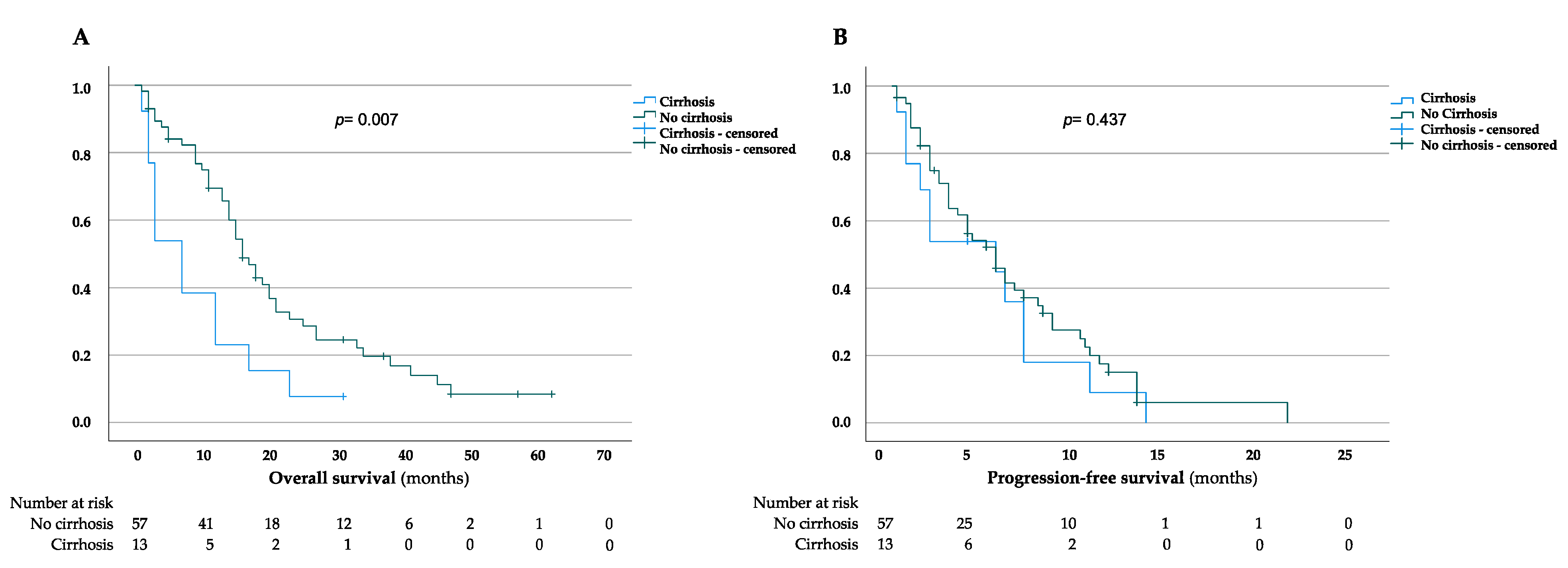
3.3. Impact of Liver Cirrhosis
3.4. Risk Factors Correlating with Overall Survival in iCCA Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bertuccio, P.; Bosetti, C.; Levi, F.; Decarli, A.; Negri, E.; la Vecchia, C. A comparison of trends in mortality from primary liver cancer and intrahepatic cholangiocarcinoma in Europe. Ann. Oncol. 2013, 24, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Shaib, Y.H.; Davila, J.A.; McGlynn, K.; El-Serag, H.B. Rising incidence of intrahepatic cholangiocarcinoma in the United States: A true increase? J. Hepatol. 2004, 40, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Walter, D.; Ferstl, P.; Waidmann, O.; Trojan, J.; Hartmann, S.; Schnitzbauer, A.A.; Zeuzem, S.; Kraywinkel, K. Cholangiocarcinoma in Germany: Epidemiologic trends and impact of misclassification. Liver Int. 2019, 39, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Macarulla, T.; Javle, M.M.; Kelley, R.K.; Lubner, S.J.; Adeva, J.; Cleary, J.M.; Catenacci, D.V.; Borad, M.J.; Bridgewater, J.; et al. Ivosidenib in Idh1-mutant, chemotherapy-refractory cholangiocarcinoma (claridhy): A multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2020, 21, 796–807. [Google Scholar] [CrossRef]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.-W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [Green Version]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Oh, D.-Y.; He, A.R.; Qin, S.; Chen, L.-T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.A.; Kitano, M.; et al. A phase 3 randomized, double-blind, placebo-controlled study of durvalumab in combination with gemcitabine plus cisplatin (gemcis) in patients (Pts) with advanced biliary tract cancer (Btc): Topaz-1. J. Clin. Oncol. 2022, 40 (Suppl. 4), 378. [Google Scholar] [CrossRef]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-line folfox chemotherapy versus active symptom control for advanced biliary tract cancer (Abc-06): A phase 3, open-label, randomised, controlled trial. Lancet Oncol. 2022, 22, 690–701. [Google Scholar] [CrossRef]
- Tyson, G.L.; El-Serag, H.B. Risk factors for cholangiocarcinoma. Hepatology 2011, 54, 173–184. [Google Scholar] [CrossRef]
- Komuta, M.; Govaere, O.; Vandecaveye, V.; Akiba, J.; Van Steenbergen, W.; Verslype, C.; Laleman, W.; Pirenne, J.; Aerts, R.; Yano, H.; et al. Histological diversity in cholangiocellular carcinoma reflects the different cholangiocyte phenotypes. Hepatology 2012, 55, 1876–1888. [Google Scholar] [CrossRef] [PubMed]
- Carpino, G.; Cardinale, V.; Folseraas, T.; Overi, D.; Grzyb, K.; Costantini, D.; Berloco, P.B.; DI Matteo, S.; Karlsen, T.H.; Alvaro, D.; et al. Neoplastic transformation of the peribiliary stem cell niche in cholangiocarcinoma arisen in primary sclerosing cholangitis. Hepatology 2019, 69, 622–638. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Toledano, M.; Taylor-Robinson, S. Epidemiology, risk factors, and pathogenesis of cholangiocarcinoma. HPB 2008, 10, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, T.-H.; Chen, X.; Zhang, X.-H.; Zhang, E.-C.; Sun, C.-X. Clinicopathological characteristics and prognostic factors for intrahepatic cholangiocarcinoma: A population-based study. Sci. Rep. 2021, 11, 3990. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.X.; Li, P.; Chen, Z.; Lin, H.; Cai, Z.; Liao, W.; Pan, Z. Impact of liver fibrosis score on prognosis after common therapies for intrahepatic cholangiocarcinoma: A propensity score matching analysis. BMC Cancer 2020, 20, 556. [Google Scholar] [CrossRef] [PubMed]
- Jesper, D.; Heyn, S.G.; Schellhaas, G.; Pfeifer, L.; Goertz, R.S.; Zopf, S.; Neurath, M.F.; Strobel, D. Effects of liver cirrhosis and patient condition on clinical outcomes in intrahepatic cholangiocarcinoma: A retrospective analysis of 156 cases in a single center. Eur. J. Gastroenterol. Hepatol. 2018, 30, 552–556. [Google Scholar] [CrossRef]
- Levy, N.A.; Kern, G.; Shepshelovich, D.; Shibolet, O.; Hershkoviz, R.; Isakov, O. Effect of liver fibrosis on survival in patients with intrahepatic cholangiocarcinoma: A seer population-based study. Oncotarget 2020, 11, 4438–4447. [Google Scholar] [CrossRef]
- Li, Y.-Y.; Li, H.; Lv, P.; Liu, G.; Li, X.-R.; Tian, B.-N.; Chen, D.-J. Prognostic value of cirrhosis for intrahepatic cholangiocarcinoma after surgical treatment. J. Gastrointest. Surg. 2011, 15, 608–613. [Google Scholar] [CrossRef]
- Desmet, V.J.; Gerber, M.; Hoofnagle, J.H.; Manns, M.; Scheuer, P.J. Classification of chronic hepatitis: Diagnosis, grading and staging. Hepatology 1994, 19, 1513–1520. [Google Scholar] [CrossRef]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with Hiv/Hcv coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Gao, L.; Tong, Y.; Xia, L.; Xu, N.; Sha, M.; Zhang, J.; Kong, X.; Gu, J.; Xia, Q. Prognostic impact of cirrhosis in patients with intrahepatic cholangiocarcinoma following hepatic resection. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6543423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endo, I.; Gonen, M.; Yopp, A.C.; Dalal, K.M.; Zhou, Q.; Klimstra, D.; d’Angelica, M.; de Matteo, R.P.; Fong, Y.; Schwartz, L.; et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Ni, Q.; Shen, W.; Zhang, M.; Yang, C.; Cai, W.; Wu, M.; Yang, J. Prognostic analysis of radical resection for intrahepatic cholangiocarcinoma: A retrospective cohort study. Oncotarget 2017, 8, 75627–75637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; Macsween, R.N.; et al. Histological grading and staging of chronic hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Chen, P.; Wang, Y.; Fang, X.; Wang, X.; Wang, G. Prognostic significance of peritumoral fibrosis after resection of pancreatic head cancer. Oncol. Lett. 2020, 19, 1235–1240. [Google Scholar] [CrossRef]
- Vaquero, J.; Aoudjehane, L.; Fouassier, L. Cancer-associated fibroblasts in cholangiocarcinoma. Curr. Opin. Gastroenterol. 2020, 36, 63–69. [Google Scholar] [CrossRef]
- Affo, S.; Nair, A.; Brundu, F.; Ravichandra, A.; Bhattacharjee, S.; Matsuda, M.; Chin, L.; Filliol, A.; Wen, W.; Song, X.; et al. Promotion of cholangiocarcinoma growth by diverse cancer-associated fibroblast subpopulations. Cancer Cell 2021, 39, 866–882.e11. [Google Scholar] [CrossRef]
- Lan, C.; Kitano, Y.; Yamashita, Y.I.; Yamao, T.; Kajiyama, K.; Yoshizumi, T.; Fukuzawa, K.; Sugimachi, K.; Ikeda, Y.; Takamori, H.; et al. Cancer-associated fibroblast senescence and its relation with tumour-infiltrating lymphocytes and Pd-L1 expressions in intrahepatic cholangiocarcinoma. Br. J. Cancer 2022, 126, 219–227. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients with Low Fibrosis Score (n = 49) No. (%) | Patients with High Fibrosis Score (n = 21) No. (%) | p-Value |
|---|---|---|---|
| Sex | 0.459 | ||
| Female | 16 (32.7) | 5 (23.8) | |
| Male | 33 (67.3) | 16 (76.2) | |
| Age at initial diagnosis | 0.4 | ||
| mean, years (range) | 60.7 (25–82) | 63.4 (37–79) | |
| First chemotherapy | 0.442 | ||
| Gem/Cis | 40 (81.6) | 18 (85.7) | |
| Gem mono | 3 (6.1) | 3 (14.3) | |
| Gem/Ox | 4 (8.2) | 0 (0) | |
| Gem/Sor | 1 (2) | 0 (0) | |
| Gem/Cis/Dur | 1 (2) | 0 (0) | |
| Child–Pugh score | 0.186 | ||
| A (5) | 40 (81.6) | 14 (66.7) | |
| A (6) | 5 (10.2) | 3 (14.3) | |
| B (7) | 3 (6.1) | 3 (14.3) | |
| n.a. | 1 (2) | 1 (4.8) | |
| ECOG | 0.434 | ||
| 0 | 38 (77.6) | 18 (85.7) | |
| 1 | 11 (22.4) | 3 (14.3) | |
| 2 | 0 (0) | 0 (0) | |
| CA-19/9 (ng/mL) | 0.785 | ||
| <37 | 17 (34.7) | 8 (38.1) | |
| ≥37 | 32 (65.3) | 13 (61.9) | |
| Tumor size (cm) | 0.174 | ||
| ≤5 | 20 (40.8) | 5 (23.8) | |
| >5 | 29 (59.2) | 16 (76.2) | |
| Irresectable | 0.617 | ||
| Yes | 32 (65.3) | 15 (71.4) | |
| No | 17 (34.7) | 6 (28.6) | |
| Stage | 0.394 | ||
| Locally advanced | 18 (36.7) | 10 (47.6) | |
| Metastatic | 31 (63.3) | 11 (52.4) | |
| Lymph node metastasis | 0.424 | ||
| No | 20 (40.8) | 11 (52.4) | |
| Yes (regional) | 14 (28.6) | 3 (14.3) | |
| Yes (distant) | 15 (30.6) | 7 (33.3) | |
| 8th UICC stage | 0.218 | ||
| Ia | 2 (4.1) | 0 (0) | |
| Ib | 3 (6.1) | 1 (4.8) | |
| II | 6 (12.2) | 8 (38.1) | |
| IIIa | 3 (6.1) | 1 (4.8) | |
| IIIb | 6 (12.2) | 1 (4.8) | |
| IV | 29 (59.2) | 10 (47.6) | |
| FIB-4 score | <0.001 | ||
| mean (range) | 1.9 (0.6–7.4) | 4 (1.4–14.9) | |
| Hepatolithiasis | 0.097 | ||
| Yes | 6 (12.2) | 6 (28.6) | |
| No | 43 (87.8) | 15 (71.4) | |
| Viral hepatitis | 0.026 | ||
| Yes | 7 (14.3) | 8 (38.1) | |
| No | 42 (85.7) | 13 (61.9) | |
| Diabetes | 0.248 | ||
| Yes | 10 (20.4) | 7 (33.3) | |
| No | 39 (79.6) | 14 (66.7) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Characteristics | HR 95% CI p-Value | HR 95% CI p-Value | ||||
| Sex | ||||||
| Female | ref | |||||
| Male | 0.719 | 0.413–1.252 | 0.244 | |||
| ECOG | ||||||
| 0 | ref | |||||
| 1 | 1.416 | 0.755–2.654 | 0.278 | |||
| CA-19/9 (ng/mL) | ||||||
| <37 | ref | |||||
| ≥37 | 1.539 | 0.886–2.673 | 0.126 | |||
| Tumor size (cm) | ||||||
| ≤5 | ref | |||||
| >5 | 0.905 | 0.529–1.547 | 0.714 | |||
| Irresectable | ||||||
| No | ref | |||||
| Yes | 1.211 | 0.7–2.095 | 0.494 | |||
| Stage | ||||||
| Locally advanced | ref | |||||
| Metastatic | 1.205 | 0.704–2.061 | 0.496 | |||
| Lymph nodes metastasis | ||||||
| No | ref | |||||
| Yes (regional) | 1.1 | 0.561–2.156 | 0.781 | |||
| Yes (distant) | 1.24 | 0.685–2.245 | 0.477 | |||
| FIB-4 score | ||||||
| ≤3.25 | ref | |||||
| >3.25 | 1.18 | 0.649–2.168 | 0.579 | |||
| High fibrosis score | ||||||
| No | ref | |||||
| Yes | 0.67 | 0.382–1.176 | 0.163 | |||
| Liver cirrhosis | ||||||
| No | ref | ref | ||||
| Yes | 2.213 | 1.153–4.248 | 0.017 | 1.86 | 0.886–3.894 | 0.101 |
| Viral hepatitis | ||||||
| No | ref | |||||
| Yes | 1.065 | 0.561–2.021 | 0.847 | |||
| Hepatolithiasis | ||||||
| No | ref | ref | ||||
| Yes | 2.3 | 1.17–4.52 | 0.016 | 0.575 | 0.267–1.237 | 0.157 |
| Diabetes | ||||||
| No | ref | |||||
| Yes | 1.324 | 0.733–2.394 | 0.352 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinzler, M.N.; Klasen, C.; Schulze, F.; Herrmann, E.; Schnitzbauer, A.A.; Trojan, J.; Zeuzem, S.; Wild, P.J.; Walter, D. Impact of Liver Fibrosis on Survival of Patients with Intrahepatic Cholangiocarcinoma Receiving Gemcitabine-Based Chemotherapy. J. Clin. Med. 2022, 11, 2057. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072057
Kinzler MN, Klasen C, Schulze F, Herrmann E, Schnitzbauer AA, Trojan J, Zeuzem S, Wild PJ, Walter D. Impact of Liver Fibrosis on Survival of Patients with Intrahepatic Cholangiocarcinoma Receiving Gemcitabine-Based Chemotherapy. Journal of Clinical Medicine. 2022; 11(7):2057. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072057
Chicago/Turabian StyleKinzler, Maximilian N., Christina Klasen, Falko Schulze, Eva Herrmann, Andreas A. Schnitzbauer, Jörg Trojan, Stefan Zeuzem, Peter J. Wild, and Dirk Walter. 2022. "Impact of Liver Fibrosis on Survival of Patients with Intrahepatic Cholangiocarcinoma Receiving Gemcitabine-Based Chemotherapy" Journal of Clinical Medicine 11, no. 7: 2057. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072057