Effects of Obstructive Sleep Apnea on Epilepsy, and Continuous Positive Airway Pressure as a Treatment Option


Abstract
:1. Introduction
2. Methods
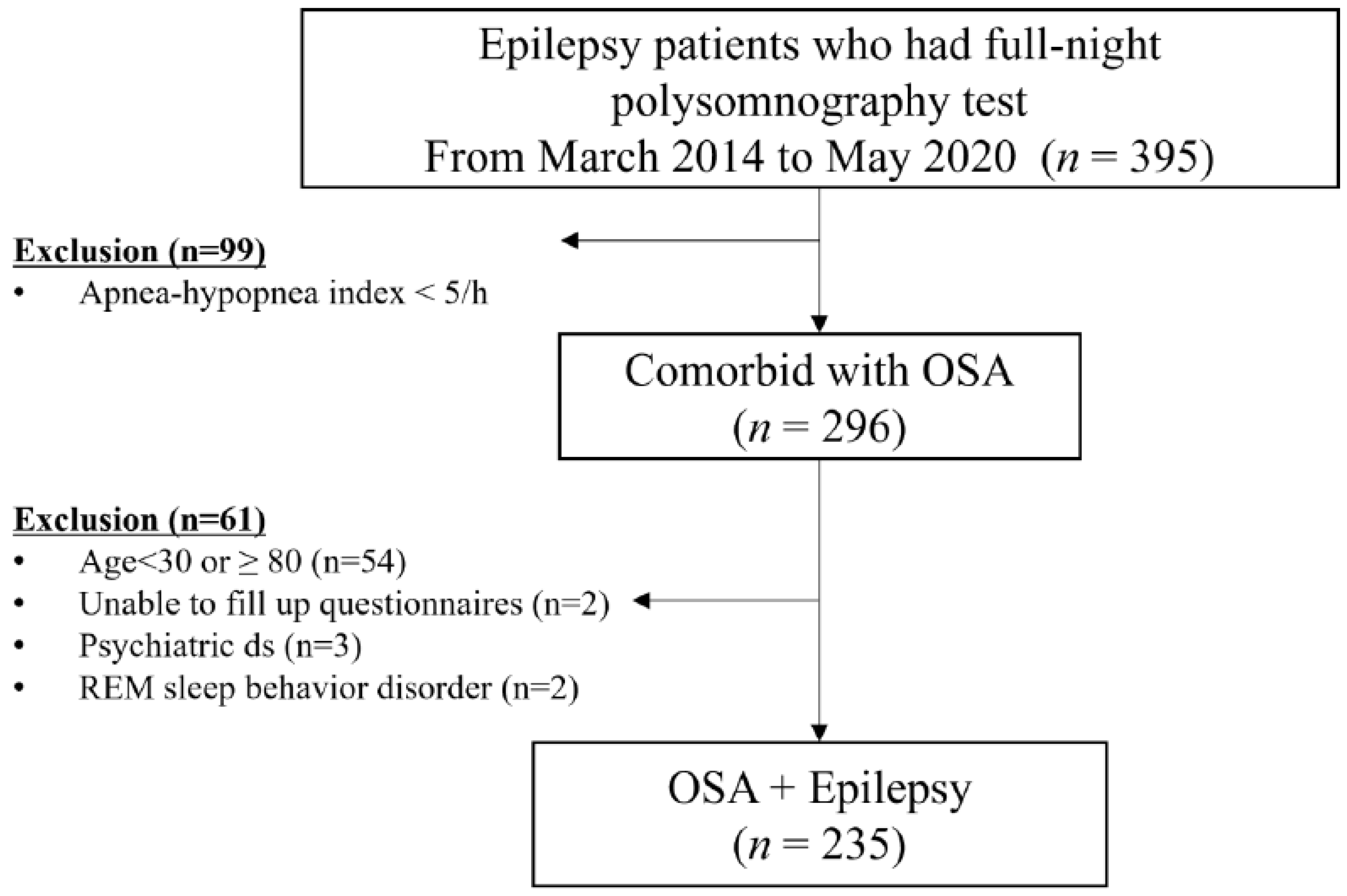
2.1. Subjects
2.2. Methods
2.2.1. PSG
2.2.2. Clinical Information
2.2.3. Self-Reported Questionnaires
2.3. Statistical Analysis
3. Results
3.1. Demographics and Subjective Sleep Questionnaires
3.2. Anthropometric and PSG Parameters
3.3. Analyses of Correlation between Epilepsy-Related Factors and Polysomnographic Parameters/Subject Questionnaires in OE
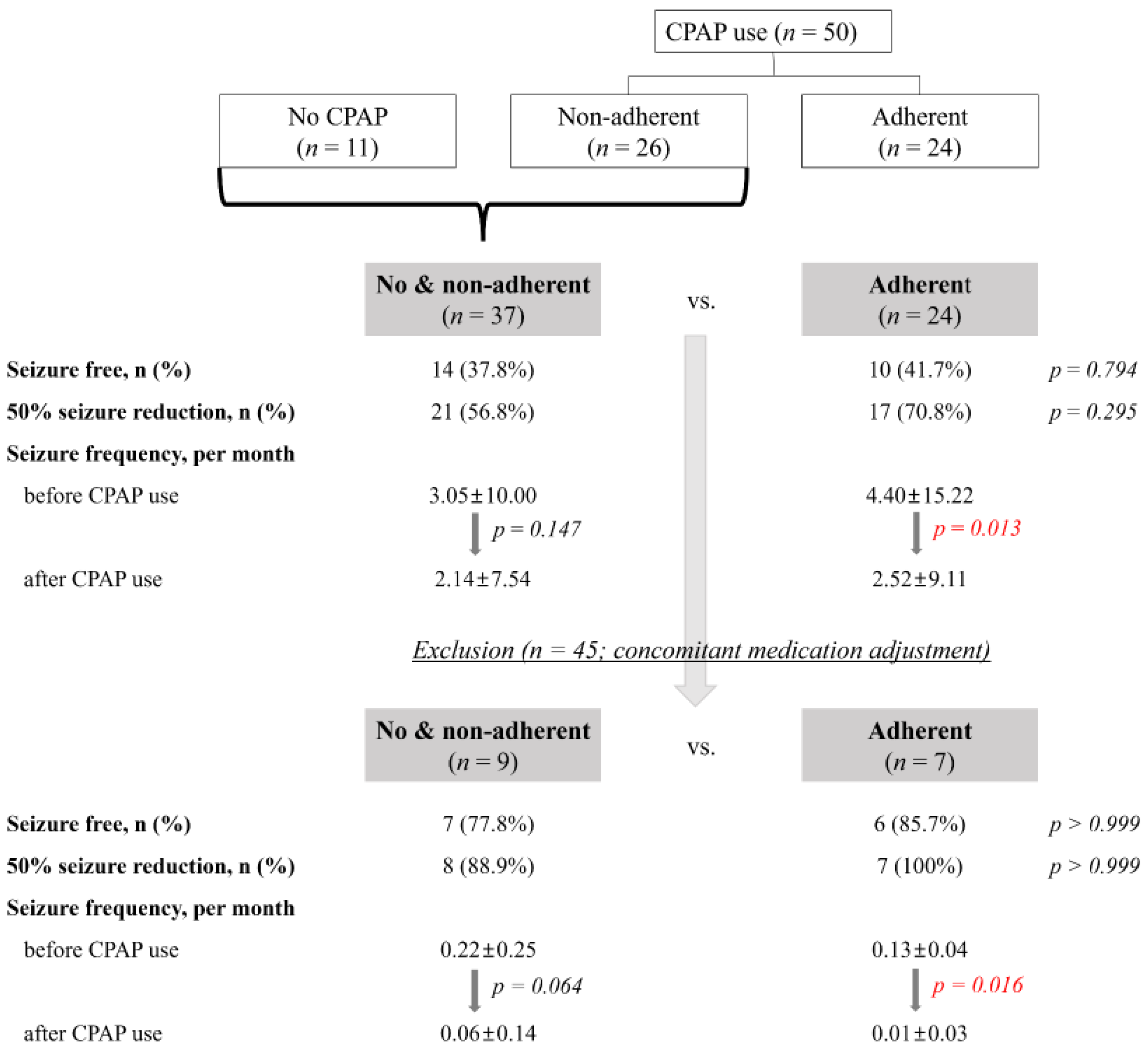
3.4. CPAP Adherence and Seizure Outcome
4. Discussion
4.1. Prevalence of OSA in PWE
4.2. Characteristics of OE Compared to OSA
4.3. CPAP as a Treatment Option for OE
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ngugi, A.K.; Kariuki, S.M.; Bottomley, C.; Kleinschmidt, I.; Sander, J.W.; Newton, C.R. Incidence of epilepsy: A systematic review and meta-analysis. Neurology 2011, 77, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Van Golde, E.G.A.; Gutter, T.; de Weerd, A.W. Sleep disturbances in people with epilepsy; prevalence, impact and treatment. Sleep Med. Rev. 2011, 15, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Heo, K. Sleep and epilepsy. J. Sleep Med. 2009, 6, 69–73. [Google Scholar] [CrossRef]
- Malow, B.A.; Levy, K.; Maturen, K.; Bowes, R. Obstructive sleep apnea is common in medically refractory epilepsy patients. Neurology 2000, 55, 1002–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Z.; Si, Q.; Xiaoyi, Z. Obstructive sleep apnoea in patients with epilepsy: A meta-analysis. Sleep Breath 2017, 21, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C. Clinical Features and Evaluation of Obstructive Sleep Apnea. In Principles and Practice of Sleep Medicine, 2nd ed.; WB Saunders: Philadelphia, PA, USA, 1994; pp. 667–677. [Google Scholar]
- Partinen, M.; Guilleminault, C. Daytime Sleepiness and Vascular Morbidity at Seven-Year Follow-up in Obstructive Sleep Apnea Patients. Chest 1990, 97, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Hung, J.; Whitford, E.G.; Hillman, D.R.; Parsons, R.W. Association of sleep apnoea with myocardial infarction in men. Lancet 1990, 336, 261–264. [Google Scholar] [CrossRef]
- He, J.; Kryger, M.H.; Zorick, F.J.; Conway, W.; Roth, T. Mortality and Apnea Index in Obstructive Sleep Apnea: Experience in 385 Male Patients. Chest 1988, 94, 9–14. [Google Scholar] [CrossRef]
- Chihorek, A.M.; Abou-Khalil, B.; Malow, B.A. Obstructive sleep apnea is associated with seizure occurrence in older adults with epilepsy. Neurology 2007, 69, 1823–1827. [Google Scholar] [CrossRef]
- Foldvary-Schaefer, N.; Andrews, N.D.; Pornsriniyom, D.; Moul, D.E.; Sun, Z.; Bena, J. Sleep apnea and epilepsy: Who’s at risk? Epilepsy Behav. 2012, 25, 363–367. [Google Scholar] [CrossRef] [Green Version]
- Deng, X.; Gu, W.; Li, Y.; Liu, M.; Li, Y.; Gao, X. Age-group-specific associations between the severity of obstructive sleep apnea and relevant risk factors in male and female patients. PLoS ONE 2014, 9, e107380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.R.; Song, P.; Joo, E.Y. Sex Differences in Obstructive Sleep Apnea by Bioelectrical Impedance Analysis. J. Clin. Neurol. 2021, 17, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Rogawski, M.A.; Löscher, W.; Rho, J.M. Mechanisms of Action of Antiseizure Drugs and the Ketogenic Diet. Cold Spring Harb. Perspect. Med. 2016, 6, a022780. [Google Scholar] [CrossRef] [PubMed]
- Strollo, P.J., Jr.; Rogers, R.M. Obstructive sleep apnea. N. Engl. J. Med. 1996, 334, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.W.; Lee, J.H.; Son, H.K.; Lee, S.H.; Shin, C.; Johns, M.W. The reliability and validity of the Korean version of the Epworth sleepiness scale. Sleep Breath 2011, 15, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.W.; Song, M.L.; Morin, C.M. Validation of a Korean version of the insomnia severity index. J. Clin. Neurol. 2014, 10, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Sohn, S.I.; Kim, D.H.; Lee, M.Y.; Cho, Y.W. The reliability and validity of the Korean version of the Pittsburgh Sleep Quality Index. Sleep Breath 2012, 16, 803–812. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Sung, H.M.; Kim, J.B.; Park, Y.N.; Bai, D.S.; Lee, S.H.; Ahn, H.N. A study on the reliability and the validity of Korean version of the Beck Depression Inventory-II (BDI-II). J. Korean Soc. Biol. Ther. Psychiatry 2008, 14, 2001–2012. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the BDI-II; The Psychological Corporation: San Antoinio, TX, USA, 1996. [Google Scholar]
- Ismayilova, V.; Demir, A.U.; Tezer, F.I. Subjective sleep disturbance in epilepsy patients at an outpatient clinic: A questionnaire-based study on prevalence. Epilepsy Res. 2015, 115, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Zanzmera, P.; Shukla, G.; Gupta, A.; Goyal, V.; Srivastava, A.; Garg, A.; Bal, C.; Suri, A.; Behari, M. Effect of successful epilepsy surgery on subjective and objective sleep parameters--a prospective study. Sleep Med. 2013, 14, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Foldvary-Schaefer, N.; Stephenson, L.; Bingaman, W. Resolution of obstructive sleep apnea with epilepsy surgery? Expanding the relationship between sleep and epilepsy. Epilepsia 2008, 49, 1457–1459. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Molano, J.; Moseley, B.D. The STOP-BANG questionnaire improves the detection of epilepsy patients at risk for obstructive sleep apnea. Epilepsy Res. 2017, 129, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.E.; Morin, C.M. The effect of temazepam on respiration in elderly insomniacs with mild sleep apnea. Sleep 1995, 18, 644–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.B.; Kouchi, K.; Bower, J.; Prosise, G.; Light, R.W. Triazolam in patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 1995, 151, 450–454. [Google Scholar] [CrossRef]
- Hanly, P.; Powles, P. Hypnotics should never be used in patients with sleep apnea. J. Psychosom. Res. 1993, 37 (Suppl. 1), 59–65. [Google Scholar]
- Zhang, H.; Li, Y.; Li, X.; Liu, G.; Wang, B.; Li, C. Effect of sodium valproate on the sleep structures of epileptic patients. Exp. Ther. Med. 2014, 7, 1227–1232. [Google Scholar] [CrossRef] [Green Version]
- Myers, K.A.; Mrkobrada, M.; Simel, D.L. Does This Patient Have Obstructive Sleep Apnea?: The Rational Clinical Examination Systematic Review. JAMA 2013, 310, 731–741. [Google Scholar] [CrossRef]
- Krol, R.C.; Knuth, S.L.; Bartlett, D., Jr. Selective reduction of genioglossal muscle activity by alcohol in normal human subjects. Am. Rev. Respir. Dis. 1984, 129, 247–250. [Google Scholar] [PubMed]
- Robinson, R.W.; White, D.P.; Zwillich, C.W. Moderate alcohol ingestion increases upper airway resistance in normal subjects. Am. Rev. Respir. Dis. 1985, 132, 1238–1241. [Google Scholar] [PubMed]
- Kim, K.S.; Kim, J.H.; Park, S.Y.; Won, H.R.; Lee, H.J.; Yang, H.S.; Kim, H.J. Smoking induces oropharyngeal narrowing and increases the severity of obstructive sleep apnea syndrome. J. Clin. Sleep. Med. 2012, 8, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Manni, R.; Politini, L.; Ratti, M.T.; Marchioni, E.; Sartori, I.; Galimberti, C.A.; Tartara, A. Sleep hygiene in adult epilepsy patients: A questionnaire-based survey. Acta Neurol. Scand. 2000, 101, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Touchon, J.; Baldy-Moulinier, M.; Billiard, M.; Besset, A.; Valmier, J.; Cadilhac, J. Organization of sleep in recent temporal lobe epilepsy before and after treatment with carbamazepine. Rev. Neurol. 1987, 143, 462–467. [Google Scholar] [PubMed]
- Guilleminault, C. Benzodiazepines, breathing, and sleep. Am. J. Med. 1990, 88, S25–S28. [Google Scholar] [CrossRef]
- Mason, M.; Cates, C.J.; Smith, I. Effects of opioid, hypnotic and sedating medications on sleep-disordered breathing in adults with obstructive sleep apnoea. Cochrane Database Syst. Rev. 2015, CD011090. [Google Scholar] [CrossRef]
- Sivathamboo, S.; Perucca, P.; Velakoulis, D.; Jones, N.C.; Goldin, J.; Kwan, P.; O’Brien, T.J. Sleep-disordered breathing in epilepsy: Epidemiology, mechanisms, and treatment. Sleep 2018, 41, zsy015. [Google Scholar] [CrossRef] [Green Version]
- Devinsky, O.; Ehrenberg, B.; Barthlen, G.M.; Abramson, H.S.; Luciano, D. Epilepsy and sleep apnea syndrome. Neurology 1994, 44, 2060. [Google Scholar] [CrossRef]
- Malow, B.A.; Fromes, G.A.; Aldrich, M.S. Usefulness of polysomnography in epilepsy patients. Neurology 1997, 48, 1389–1394. [Google Scholar] [CrossRef]
- Vaughn, B.V.; D’Cruz, O.F.; Beach, R.; Messenheimer, J.A. Improvement of epileptic seizure control with treatment of obstructive sleep apnoea. Seizure 1996, 5, 73–78. [Google Scholar] [CrossRef] [Green Version]
- Vendrame, M.; Auerbach, S.; Loddenkemper, T.; Kothare, S.; Montouris, G. Effect of continuous positive airway pressure treatment on seizure control in patients with obstructive sleep apnea and epilepsy. Epilepsia 2011, 52, e168–e171. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Category | OSA Only (n = 268) | OSA with Epilepsy (n = 235) | p-Value |
|---|---|---|---|---|
| Age, years | 51.3 ± 11.0 | 49.8 ± 11.9 | 0.146 | |
| Gender | Male | 216 (80.6) | 183 (77.9) | 0.508 † |
| Marital status | Single | 28 (10.4) | 48 (20.4) | 0.002 † |
| Married | 219 (81.7) | 153 (65.1) | ||
| Divorced or widowed | 19 (7.1) | 17 (7.2) | ||
| Education, n (%) | ≤12 years | 65 (24.3) | 80 (34.0) | <0.002 * |
| ≥13 years | 198 (73.9) | 135 (57.4) | ||
| Occupation † | Yes | 224 (83.6) | 151 (64.3) | <0.001 * |
| Students | 3 (1.1) | 1 (0.4) | ||
| No | 32 (11.9) | 64 (27.2) | ||
| Alcohol, n (%) | 175 (65.3) | 89 (37.9) | <0.001 * | |
| Smoking, n (%) | None | 140 (52.2) | 140 (59.6) | 0.001 * |
| Ex-smoker | 81 (30.2) | 35 (14.9) | ||
| Current | 46 (17.2) | 44 (18.7) | ||
| Comorbidities | Hypertension | 71 (26.5) | 23 (9.8) | 0.075 |
| Diabetes mellitus | 24 (9.0) | 11 (4.7) | 0.541 | |
| Cardiovascular disease | 19 (7.1) | 9 (3.8) | 0.518 | |
| Hyperlipidemia † | 11 (4.1) | 4 (1.7) | 0.482 | |
| Use of hypnotics, n (%) | 23 (8.6) | 4 (1.7) | 0.056 | |
| Insomnia severity index | 11.2 ± 6.3 | 8.8 ± 5.4 | <0.001 * | |
| PSQI | 7.8 ± 3.4 | 6.0 ± 3.1 | <0.001 * | |
| 5a. cannot get to sleep within 30 min | 1.07 ± 1.15 | 0.93 ± 1.07 | 0.192 | |
| 5b. wake up in the middle of the night or early morning | 2.10 ± 1.03 | 1.59 ± 1.15 | <0.001 * | |
| 5d. cannot breathe comfortably | 1.18 ± 1.23 | 0.57 ± 0.97 | <0.001 * | |
| 5e. cough or snore loudly | 2.20 ± 1.10 | 1.55 ± 1.25 | <0.001 * | |
| 5h. have bad dreams | 0.69 ± 0.92 | 0.64 ± 0.87 | 0.576 | |
| ESS | 10.7 ± 4.8 | 8.0 ± 4.4 | <0.001 * | |
| EDS (ESS > 10) | 136 (50.7) | 58 (24.7) | <0.001 * | |
| K-BDI-II | 12.3 ± 7.2 | 14.5 ± 10.0 | 0.011 | |
| Variables | Category | Mean ± SD/n (%) |
|---|---|---|
| Age at seizure onset, year | 31.0 ± 17.5 | |
| Epilepsy classification, n (%) | Generalized epilepsy | 36 (15.3) |
| Focal epilepsy | 195 (83.0) | |
| lesional/nonlesional | 127 (65.1)/68 (34.9) | |
| Temporal/Frontal | 78 (40.0)/37 (19.0) | |
| Frequency of seizure, /m | 1.5 ± 8.3 | |
| Presence of nocturnal seizure, n (%) | 112 (47.7) | |
| Number of ASMs | 2.3 ± 1.7 | |
| 0 | 29 (12.3) | |
| 1 | 52 (22.1) | |
| ≥2 | 150 (63.8) | |
| Mechanisms of action of ASMs | Voltage-gated ion channels | 172 (73.2) |
| GABA inhibition | 91 (38.7) | |
| Synaptic release machinery | 94 (40.0) | |
| Ionotropic glutamate receptors | 126 (53.6) |
| Variables | OSA Only (n = 268) | OSA with Epilepsy (n = 235) | p-Value | OSA with Epilepsy | ||
|---|---|---|---|---|---|---|
| ASM 0 or 1 (n = 81) | ASMs ≥ 2 (n = 150) | p-Value | ||||
| BMI, kg/m2 | 25.9 ± 3.4 | 27.0 ± 3.6 | <0.001 * | |||
| ≥25 kg/m2 | 162 (60.4) | 158 (67.2) | 0.069 † | |||
| Neck circumference-lying, cm | 39.4 ± 3.4 | 39.2 ± 3.6 | 0.626 | |||
| Waist circumference, cm | 92.7 ± 9.5 | 90.0 ± 19.1 | 0.065 | |||
| Hip circumference, cm | 97.4 ± 6.3 | 97.8 ± 7.0 | 0.570 | |||
| Waist-hip ratio | 0.95 ± 0.06 | 0.97 ± 0.57 | 0.008 * | |||
| Total sleep time, min | 371.1 ± 63.2 | 372.7 ± 59.0 | 0.773 | 377.0 ± 53.6 | 371.0 ± 61.7 | 0.458 |
| Sleep latency, min | 9.6 ± 14.3 | 10.1 ± 16.2 | 0.722 | 11.6 ± 22.1 | 8.9 ± 11.8 | 0.310 |
| WASO, % | 14.0 ± 9.4 | 14.3 ± 10.1 | 0.714 | 14.1 ± 8.8 | 14.4 ± 10.8 | 0.859 |
| Sleep efficiency, % | 84.3 ± 10.3 | 83.8 ± 10.8 | 0.501 | 84.0 ± 10.2 | 83.8 ± 11.2 | 0.916 |
| Sleep stages | ||||||
| N1 sleep, % | 24.4 ± 14.1 | 20.5 ± 11.6 | 0.001 * | 22.7 ± 12.7 | 19.3 ± 10.8 | 0.033 |
| N2 sleep, % | 52.2 ± 12.6 | 57.7 ± 11.7 | <0.001 * | 53.7 ± 12.3 | 60.0 ± 10.6 | <0.001 * |
| N3 sleep, % | 2.8 ± 5.2 | 4.5 ± 6.4 | 0.001 | 5.4 ± 5.8 | 4.0 ± 6.7 | 0.124 |
| REM sleep, % | 20.7 ± 6.9 | 17.3 ± 6.6 | <0.001 * | 18.3 ± 6.7 | 16.8 ± 6.5 | 0.097 |
| AHI, /h | 33.4 ± 21.3 | 24.9 ± 17.6 | <0.001 * | 28.5 ± 18.4 | 22.7 ± 16.5 | 0.015 |
| OSA severity | <0.001 * | 0.076 | ||||
| Mild (5 ≤ AHI < 15/h) | 50 (18.7) | 80 (34.0) | 22 (27.2) | 57 (38.0) | ||
| Moderate (15 ≤ AHI < 30/h) | 95 (35.4) | 85 (36.2) | 28 (34.6) | 56 (37.3) | ||
| Severe (AHI ≥ 30/h) | 121 (45.1) | 70 (29.8) | 31 (38.3) | 37 (24.7) | ||
| Oxygen desaturation index | 28.8 ± 21.4 | 19.6 ± 17.2 | <0.001 * | 22.3 ± 18.4 | 18.0 ± 16.0 | 0.083 |
| Arousal Index, /h | 30.8 ± 21.9 | 23.3 ± 12.1 | <0.001 * | 26.9 ± 13.2 | 21.4 ± 11.1 | 0.001 |
| Respiratory AI, /h | 22.8 ± 18.0 | 15.0 ± 12.7 | <0.001 * | 18.8 ± 15.0 | 12.9 ± 10.8 | 0.002 |
| Spontaneous AI, /h | 3.9 ± 4.0 | 4.1 ± 3.6 | 0.616 | 4.3 ± 3.7 | 4.0 ± 3.6 | 0.664 |
| AHI | ODI | AI | ESS | ISI | PSQI | BDI-II | |
|---|---|---|---|---|---|---|---|
| Age at seizure onset | 0.083 | 0.048 | 0.081 | −0.148 * | −0.068 | −0.026 | 0.014 |
| Epilepsy classification | |||||||
| Focal/Generalized | −0.106 | −0.104 | −0.041 | 0.023 | 0.072 | 0.023 | 0.028 |
| lesional/nonlesional | 0.055 | 0.064 | 0.057 | −0.088 | 0.125 | 0.161 | 0.131 |
| Temporal/Frontal | 0.089 | 0.099 | 0.006 | 0.014 | −0.097 | 0.073 | 0.109 |
| Frequency of seizure (/month) | −0.054 | −0.054 | −0.014 | −0.084 | 0.052 | −0.034 | 0.184 * |
| Presence of nocturnal seizure | −0.004 | −0.030 | −0.015 | −0.010 | 0.009 | −0.066 | −0.030 |
| Number of ASMs | −0.109 | −0.061 | −0.220 * | 0.129 | 0.144 | 0.036 | 0.228 * |
| Mechanism of action of ASMs | |||||||
| Voltage-gated ion channels | −0.077 | −0.040 | −0.109 | 0.069 | −0.013 | −0.093 | −0.063 |
| GABA inhibition | −0.166 * | −0.109 | −0.221 * | 0.149 * | 0.157 * | −0.038 | 0.219 * |
| Synaptic release machinery | −0.077 | −0.074 | −0.110 | −0.023 | 0.069 | −0.035 | 0.121 |
| Ionotropic glutamate receptors | 0.010 | 0.015 | −0.100 | 0.190 * | 0.092 | 0.013 | 0.137 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, H.; Choi, S.; Kim, D.; Joo, E. Effects of Obstructive Sleep Apnea on Epilepsy, and Continuous Positive Airway Pressure as a Treatment Option. J. Clin. Med. 2022, 11, 2063. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072063
Jo H, Choi S, Kim D, Joo E. Effects of Obstructive Sleep Apnea on Epilepsy, and Continuous Positive Airway Pressure as a Treatment Option. Journal of Clinical Medicine. 2022; 11(7):2063. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072063
Chicago/Turabian StyleJo, Hyunjin, Sujung Choi, Dongyeop Kim, and Eunyeon Joo. 2022. "Effects of Obstructive Sleep Apnea on Epilepsy, and Continuous Positive Airway Pressure as a Treatment Option" Journal of Clinical Medicine 11, no. 7: 2063. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11072063