
An Abnormal Inflammatory Pattern Associated with Long-Term Non-Progression of HIV Infection Impacts Negatively on Bone Quality

 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Post Hoc Power Calculation
3.3. Bone Strength Components
3.3.1. Bone Mineral Density, In Vivo Microindentation (Bone Quality)
3.3.2. Bone Turnover Markers
3.4. Inflammatory Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhavan, K.P.; Kampalath, V.N.; Overton, E.T. The aging of the HIV epidemic. Curr. HIV/AIDS Rep. 2008, 5, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Güerri-Fernandez, R.; Vestergaard, P.; Carbonell, C.; Knobel, H.; Avilés, F.F.; Castro, A.S.; Nogués, X.; Prieto-Alhambra, D.; Diez-Perez, A. HIV infection is strongly associated with hip fracture risk, independently of age, gender, and comorbidities: A population-based cohort study. J. Bone Miner. Res. 2013, 28, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Alhambra, D.; Güerri-Fernández, R.; De Vries, F.; Arief MSc, L.; Marloes, B.; Jakob, S.-L.; Adolfo, D.-P.; Cyrus, C.; Peter, V. HIV infection and its association with an excess risk of clinical fractures and: A nation-wide case-control study. J. Acquir. Immune Defic. Syndr. 2014, 66, 90–95. [Google Scholar] [CrossRef]
- Brown, T.T.; Qaqish, R.B. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: A meta-analytic review. AIDS 2006, 20, 2165–2174. [Google Scholar] [CrossRef]
- Stellbrink, H.-J.; Orkin, C.; Arribas, J.R.; Compston, J.; Gerstoft, J.; Wijngaerden, E.V.; Lazzarin, A.; Rizzardini, G.; Sprenger, H.G.; Lambert, J. Comparison of changes in bone density and turnover with abacavir-lamivudine versus tenofovir-emtricitabine in HIV-infected adults: 48-week results from the ASSERT study. Clin. Infect. Dis. 2010, 51, 963–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotter, A.G.; Sabin, C.; Simelane, S.; Macken, A.; Kavanagh, E.; Brady, J.J.; McCarthy, G.; Compston, J.; Mallon, P.W. Relative contribution of HIV infection, demographics and body mass index to bone mineral density. AIDS 2014, 28, 2051–2060. [Google Scholar] [CrossRef]
- Güerri-Fernández, R.; Villar-García, J.; Díez-Pérez, A.; Prieto-Alhambra, D. HIV infection, bone metabolism, and fractures | Infecção pelo HIV, o metabolismo ósseo e fraturas. Arq. Bras. Endocrinol. Metabol. 2014, 58, 478–483. [Google Scholar] [CrossRef] [Green Version]
- Güerri-Fernández, R.; Lerma-Chippirraz, E.; Marron, A.F.; García-Giralt, N.; Villar-García, J.; Soldado-Folgado, J.; González-Mena, A.; Trenchs-Rodríguez, M.; Guelar, A.; Díez-Pérez, A.; et al. Bone density, microarchitecture, and tissue quality after 1 year of treatment with tenofovir disoproxil fumarate. AIDS 2018, 32, 913–920. [Google Scholar] [CrossRef]
- Güerri-Fernández, R.; Molina, D.; Villar-García, J.; Prieto-Alhambra, D.; Mellibovsky, L.; Nogues, X.; González-Mena, A.; Guelar, A.; Trenchs-Rodríguez, M.; Herrera, S.; et al. HIV infection is associated with worse bone material properties, independently of bone mineral density. J. Acquir. Immune Defic. Syndr. 2016, 72, 314–318. [Google Scholar] [CrossRef]
- Güerri-Fernández, R.; Molina-Morant, D.; Villar-García, J.; Herrera, S.; González-Mena, A.; Guelar, A.; Trenchs-Rodríguez, M.; Díez-Pérez, A.; Knobel, H. Bone Density, Microarchitecture, and Tissue Quality After Long-Term Treatment With Tenofovir/Emtricitabine or Abacavir/Lamivudine. J. Acquir. Immune Defic. Syndr. 2017, 75, 322–327. [Google Scholar] [CrossRef]
- Cummings, S.R.; Bates, D.; Black, D.M. Clinical use of bone densitometry: Scientific review. JAMA 2002, 288, 1889–1897. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/12377088 (accessed on 22 May 2018). [CrossRef] [PubMed] [Green Version]
- Bridges, D.; Randall, C.; Hansma, P.K. A new device for performing reference point indentation without a reference probe. Rev. Sci. Instrum. 2012, 83, 044301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
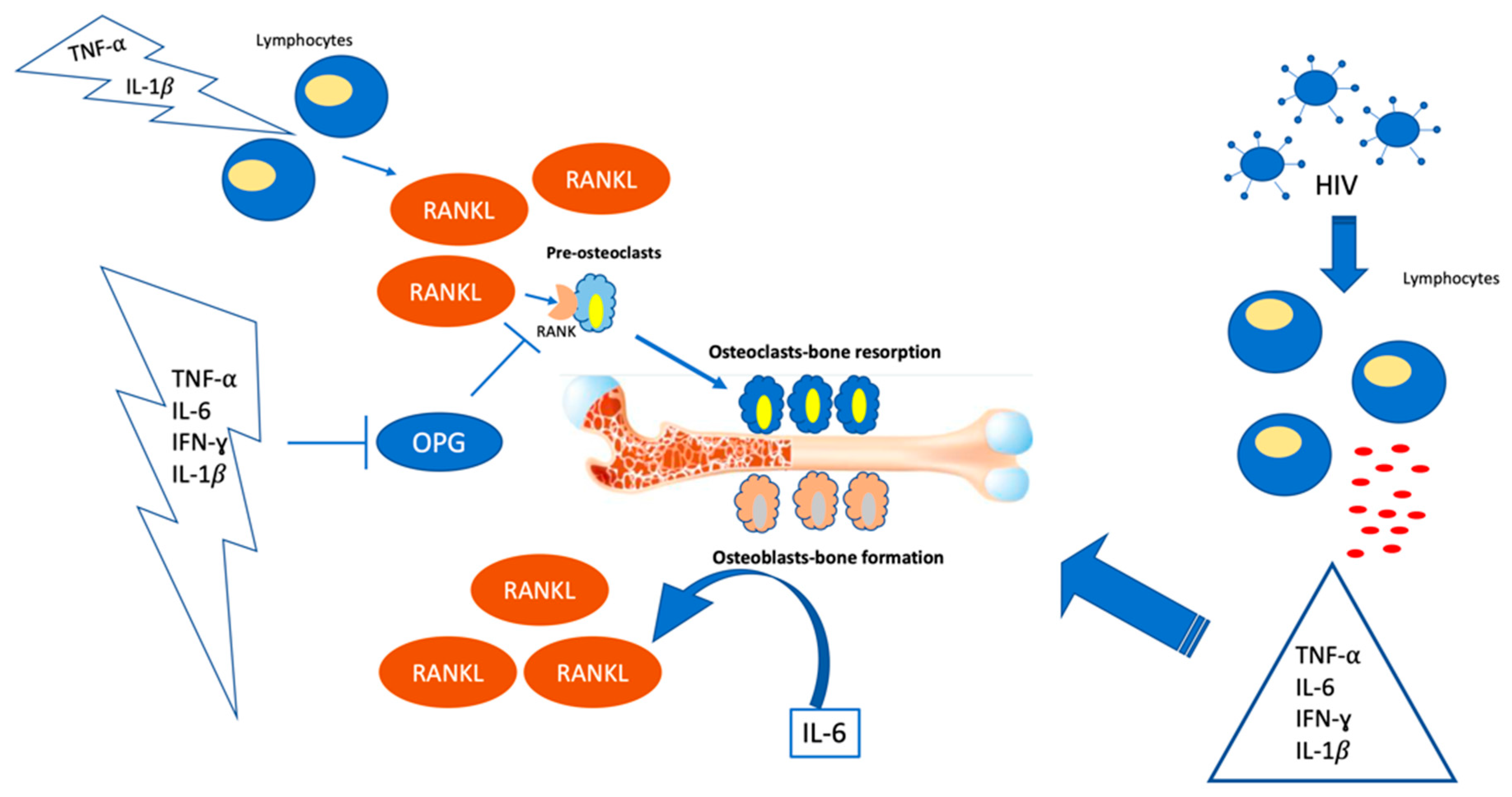
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Kotake, S.; Sato, K.; Kim, K.J.; Takahashi, N.; Udagawa, N.; Nakamura, I.; Yamaguchi, A.; Kishimoto, T.; Suda, T.; Kashiwazaki, S. Interleukin-6 and soluble interleukin-6 receptors in the synovial fluids from rheumatoid arthritis patients are responsible for osteoclast-like cell formation. J. Bone Mineral. Res. 2009, 11, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.K.; Quinn, J.M.; Sims, N.A.; van Nieuwenhuijze, A.; Campbell, I.K.; Wicks, I.P. Interleukin-6 modulates production of T lymphocyte-derived cytokines in antigen-induced arthritis and drives inflammation-induced osteoclastogenesis. Arthritis Rheum. 2005, 54, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Pereyra, F.; Addo, M.; Kaufmann, D.E.; Liu, Y.; Miura, T.; Rathod, A.; Baker, B.; Trocha, A.; Rosenberg, R.; Mackey, E.; et al. Genetic and Immunologic Heterogeneity among Persons Who Control HIV Infection in the Absence of Therapy. J. Infect. Dis. 2008, 197, 563–571. [Google Scholar] [CrossRef]
- Lerma-Chippirraz, E.; Pineda-Moncusí, M.; González-Mena, A.; Soldado-Folgado, J.; Knobel, H.; Trenchs-Rodríguez, M.; Díez-Pérez, A.; Brown, T.T.; García-Giralt, N.; Güerri-Fernández, R. Inflammation status in HIV-positive individuals correlates with changes in bone tissue quality after initiation of ART. J. Antimicrob. Chemother. 2019, 74, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, M.E.; Mikhailova, A.; Brown, E.P.; Dowell, K.G.; Walker, B.D.; Bailey-Kellogg, C.; Suscovich, T.J.; Alter, G. Polyfunctional HIV-Specific Antibody Responses Are Associated with Spontaneous HIV Control. PLoS Pathog. 2016, 12, e1005315. [Google Scholar] [CrossRef]
- Brown, T.T. HIV: An underrecognized secondary cause of osteoporosis? J. Bone Miner. Res. 2013, 28, 1256–1258. [Google Scholar] [CrossRef]
- Thompson, J.B.; Kindt, J.H.; Drake, B.; Hansma, H.G.; Morse, D.E.; Hansma, P.K. Bone indentation recovery time correlates with bond reforming time. Nature 2001, 414, 773–776. [Google Scholar] [CrossRef]
- Zhu, S.; He, H.; Gao, C.; Luo, G.; Xie, Y.; Wang, H.; Tian, L.; Chen, X.; Yu, X.; He, C. Ovariectomy-induced bone loss in TNFα and IL6 gene knockout mice is regulated by different mechanisms. J. Mol. Endocrinol. 2018, 60, 185–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ke, D.; Fu, X.; Xue, Y.; Wu, H.; Zhang, Y.; Chen, X.; Hou, J.; Ke, D.; Fu, X.; Xue, Y.; et al. IL-17A regulates the autophagic activity of osteoclast precursors through RANKL-JNK1 signaling during osteoclastogenesis in vitro. Biochem. Biophys. Res. Commun. 2018, 497, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Ono, T.; Okamoto, K.; Nakashima, T.; Nitta, T.; Hori, S.; Iwakura, Y.; Takayanagi, H. IL-17-producing γδT cells enhance bone regeneration. Nat. Commun. 2016, 7, 10928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tejon, G.P.; Manríquez, V.; De Calisto, J.; Flores-Santibañez, F.; Hidalgo, Y.; Crisóstomo, N.; Fernandez, D.; Sauma, D.; Mora, J.R.; Bono, M.R.; et al. Vitamin A Impairs the Reprogramming of Tregs into IL-17-Producing Cells during Intestinal Inflammation. Biomed. Res. Int. 2015, 2015, 137893. [Google Scholar] [CrossRef] [PubMed]
- Favre, D.; Lederer, S.; Kanwar, B.; Ma, Z.-M.; Proll, S.; Kasakow, Z.; Mold, J.; Swainson, L.; Barbour, J.D.; Baskin, C.R.; et al. loss of the balance between Th17 and T regulatory cell populations in pathogenic SIV infection. PLoS Pathog. 2009, 5, e1000295. [Google Scholar] [CrossRef]
- Kim, C.J.; McKinnon, L.R.; Kovacs, C.; Kandel, G.; Huibner, S.; Chege, D.; Shahabi, K.; Benko, E.; Loutfy, M.; Ostrowski, M.; et al. Mucosal Th17 Cell Function Is Altered during HIV Infection and Is an Independent Predictor of Systemic Immune Activation. J. Immunol. 2013, 191, 2164–2173. [Google Scholar] [CrossRef]
- Kared, H.; Tan, S.W.; Lau, M.C.; Chevrier, M.; Tan, C.; How, W.; Wong, G.; Strickland, M.; Malleret, B.; Amoah, A.; et al. Immunological history governs human stem cell memory CD4 heterogeneity via the Wnt signaling pathway. Nat. Commun. 2020, 11, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Ke, H.Z.; Richards, W.G.; Li, X.; Ominsky, M.S. Sclerostin and Dickkopf-1 as Therapeutic Targets in Bone Diseases. Endocr. Rev. 2012, 33, 747–783. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Kurimoto, P.; Zhang, J.; Niu, Q.; Stolina, M.; Dechow, P.; Feng, J.; Hesterman, J.; Silva, M.; Ominsky, M.; et al. Sclerostin and DKK1 Inhibition Preserves and Augments Alveolar Bone Volume and Architecture in Rats with Alveolar Bone Loss. J. Dent. Res. 2018, 97, 1031–1038. [Google Scholar] [CrossRef]
- Grey, A.; Mitnick, M.-A.; Masiukiewicz, U.; Sun, B.-H.; Rudikoff, S.; Jilka, R.L.; Manolagas, S.C.; Insogna, K. A role for interleukin-6 in parathyroid hormone-induced bone resorption in vivo. Endocrinology 1999, 140, 4683–4690. [Google Scholar] [CrossRef]
- Turk, G.; Seiger, B.K.; Lian, X.; Sun, W.; Parsons, B.E.M.; Gao, C.; Rassadkina, B.Y.; Polo, M.L.; Czernikier, M.A.; Ghiglione, Y.; et al. A Possible Sterilizing Cure of HIV-1 Infection Without Stem Cell Transplantation. Ann. Intern. Med. 2021, 175, 95–100. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control | HIV+ LTNP | HIV+ Progressors | p-Value | |
|---|---|---|---|---|
| N | 10 | 10 | 10 | |
| Age (years) | 42 (35–55) | 47 (45–54) | 44 (41–45) | 0.413 |
| Male (n, %) | 5 (50%) | 6 (60%) | 7 (70%) | 0.384 |
| BMI (kg/m2) | 24 (23–26) | 25 (23–26) | 24 (22–24) | 0.125 |
| Smoking (n, %) | 5 (50%) | 6 (60%) | 6 (60%) | 0.548 |
| Alcohol (>10 g/d) (n, %) | 0 | 1 (10%) | 0 | 0.833 |
| Ex-IDU (n, %) | 0 | 1 (10%) | 0 | 0.833 |
| Recreational drugs (n, %) | 2 (20%) | 2 (20%) | 3 (30%) | 0.428 |
| Previous fracture (n, %) | 0 | 0 | 0 | |
| Family history of fracture (n, %) | 0 | 1 (10%) | 1 (10%) | 0.441 |
| Prevalent spine fractures (n, %) | 0 | 0 | 0 | |
| eGFR < 60 mL/min | 0 | 0 | 0 | |
| eGFR (CKD-EPI (mL/minl) | 82 (78–87) | 85 (77–89) | 85 (78–91) | 0.188 |
| Years since HIV diagnosis | 0 | 6 (3–13) | 3 (2–4) a | 0.032 |
| Nadir CD4 count (per mL) | 438 (305–678) | 417 (341–548) | 0.939 | |
| Current CD4 count (per mL) | 444 (393–730) | 510 (341–579) | 0.791 | |
| Current viral load (per mL) | 66 (39–145) | 13,180 (4396–160,977) a | 0.021 | |
| Ever met AIDS criteria (n, %) | 0 | 1 (10%) |
| Control | HIV+ LTNP | HIV+ Progressors | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Bone Strength | |||||||
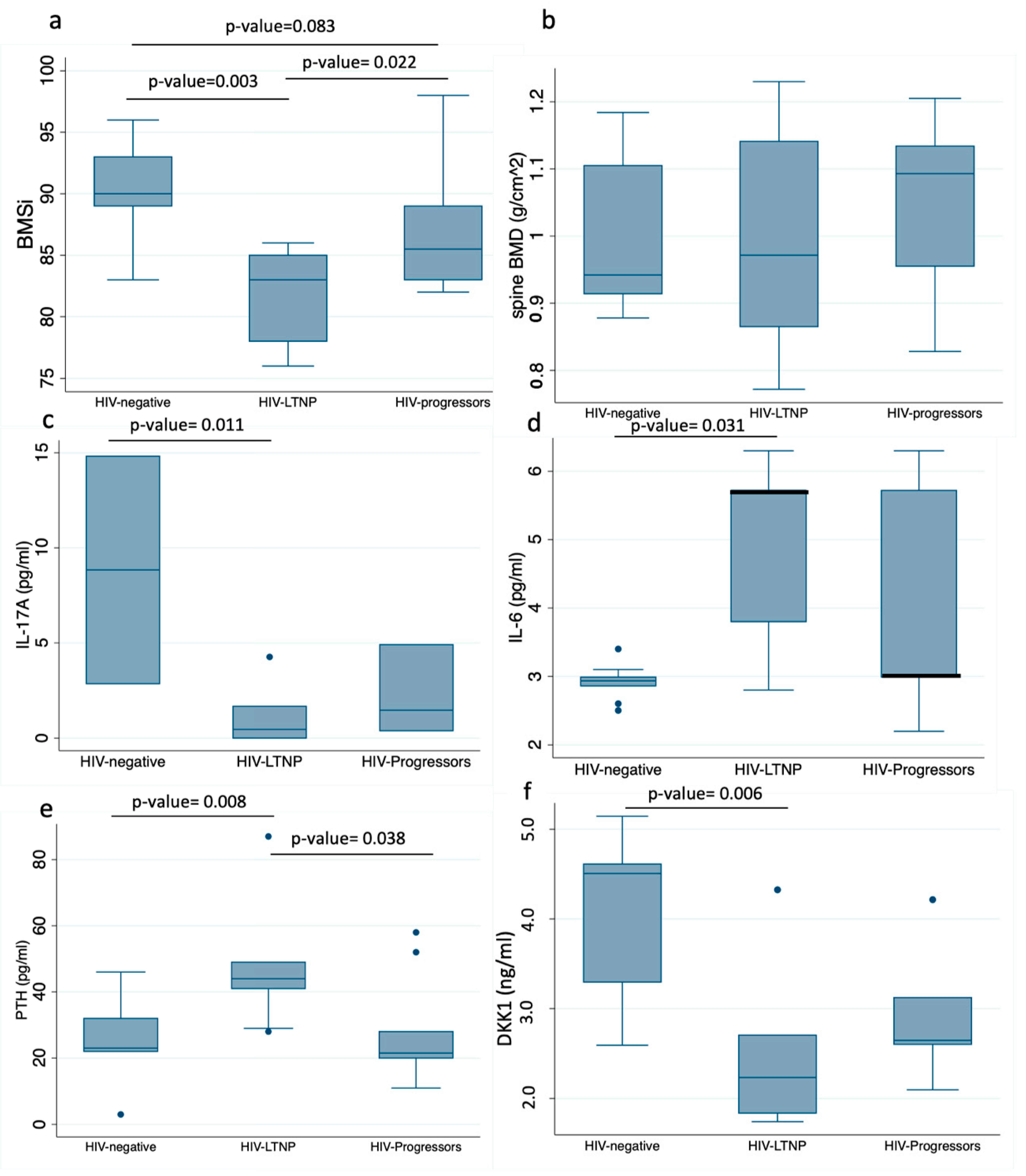
| BMSi | 90 | (89–93) | 83 | (78–85) 1,2 | 86 | (83–89) * | 0.001 |
| Lumbar spine BMD (g/cm2) | 0.936 | (0.91–0.988) | 0.933 | (0.86–1.14) | 1.05 | (0.95–1.13) | 0.558 |
| Femoral neck BMD (g/cm2) | 0.774 | (0.73–0.82) | 0.821 | (0.787–0.98) | 0.848 | (0.79–0.87) | 0.104 |
| Inflammation | |||||||
| hs-CRP (mg/dl) | 0.14 | (0.002–0.47) | 0.15 | (0.09–0.32) | 0.39 | (0.15–0.78) | 0.182 |
| D-Dimer (IU/mL) | 190 | (143–191) | 240 | (147–290) | 180 | (131–202) | 0.389 |
| IFN-γ (pg/mL) | 11.7 | (10.4–11.9) | 9.85 | (0.46–24.31) | 8.35 | (6.5–12.7) | 0.613 |
| IL-10 (pg/mL) | 3.41 | (3.24–3.57) | 2.85 | (0.22–2.85) 1,2 | 3.5 | (3.24–3.57) | 0.023 |
| IL-17A (pg/mL) | 8.83 | (2.85–14.82) | 0.46 | (0.46–1.67) 1,** | 1.46 | (0.39–4.91) | 0.014 |
| IL-2 (pg/mL) | 2.41 | (0.58–3.14) | 1.46 | (0.5–1.46) | 2.41 | (1.46–2.41) | 0.554 |
| IL-6 (pg/mL) | 2.92 | (2.86–2.99) | 5.72 | (3.8–5.72) 1,** | 2.99 | (2.99–5.72) | 0.231 |
| IL-8 (pg/mL) | 48.2 | (35.6–51.2) | 1.89 | (0.97–5.85) 1,2 | 14.4 | (8.27–37.2) | 0.004 |
| Soluble CD40 Ligand (ng/mL) | 7.26 | (5.1–7.5) | 9.3 | (6.2–17.7) | 5.5 | (4–10.2) | 0.341 |
| TNF-α (pg/mL) | 16.9 | (11.3–24.51) | 3.7 | (2.07–4.69) 1,2 | 18.3 | (16.7–22.02) | 0.004 |
| IL-6 Soluble Receptor (ng/mL) | 28.6 | (22.9–37.2) | 32.6 | (22.7–33.6) | 29.7 | (25.9–33.1) | 0.915 |
| Bone Metabolism Markers | |||||||
| DKK1 (ng/mL) | 4.5 | (3.2–4.6) | 2.2 | (1.8–2.7) 1 | 2.6 | (2.6–3.1) | 0.043 |
| OPG (ng/mL) | 0.5 | (0.4–0.6) | 0.53 | (0.46–0.61) | 0.5 | (0.44–0.52) | 0.678 |
| SOST (ng/mL) | 1.6 | (1.3–1.6) | 1.2 | (0.3–1.5) | 1.4 | (1.1–1.5) | 0.417 |
| P1NP (ng/mL) | 30.1 | (22.3–36) | 31.4 | (28.8–48.9) | 43.5 | (34.4–52.2) | 0.231 |
| Ctx (ng/mL) | 0.21 | (0.11–0.47) | 0.31 | (0.19–0.44) | 0.25 | (0.24–0.35) | 0.678 |
| Bone Alkaline Phosphatase (µg/mL) | 12.5 | (7.5–17.8) | 10.8 | (8.8–14.7) | 13.3 | (11.7–19.1) | 0.791 |
| 25OH Vitamin D (ng/mL) | 27 | (22.8–41.2) | 26.6 | (23–43) | 25.1 | (13.4–29.1) | 0.544 |
| PTH (pg/mL) | 23 | (22–32) | 44 | (41–49) 1,2 | 21 | (20–28) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soldado-Folgado, J.; Chillarón, J.J.; Cañas-Ruano, E.; Arrieta-Aldea, I.; González-Mena, A.; Blasco-Hernando, F.; Knobel, H.; Garcia-Giralt, N.; Güerri-Fernández, R. An Abnormal Inflammatory Pattern Associated with Long-Term Non-Progression of HIV Infection Impacts Negatively on Bone Quality. J. Clin. Med. 2022, 11, 2927. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102927
Soldado-Folgado J, Chillarón JJ, Cañas-Ruano E, Arrieta-Aldea I, González-Mena A, Blasco-Hernando F, Knobel H, Garcia-Giralt N, Güerri-Fernández R. An Abnormal Inflammatory Pattern Associated with Long-Term Non-Progression of HIV Infection Impacts Negatively on Bone Quality. Journal of Clinical Medicine. 2022; 11(10):2927. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102927
Chicago/Turabian StyleSoldado-Folgado, Jade, Juan José Chillarón, Esperanza Cañas-Ruano, Itziar Arrieta-Aldea, Alicia González-Mena, Fabiola Blasco-Hernando, Hernando Knobel, Natalia Garcia-Giralt, and Robert Güerri-Fernández. 2022. "An Abnormal Inflammatory Pattern Associated with Long-Term Non-Progression of HIV Infection Impacts Negatively on Bone Quality" Journal of Clinical Medicine 11, no. 10: 2927. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11102927