
Polysomnographic Assessment of Effects of Tobacco Smoking and Alcohol Consumption on Sleep Bruxism Intensity

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
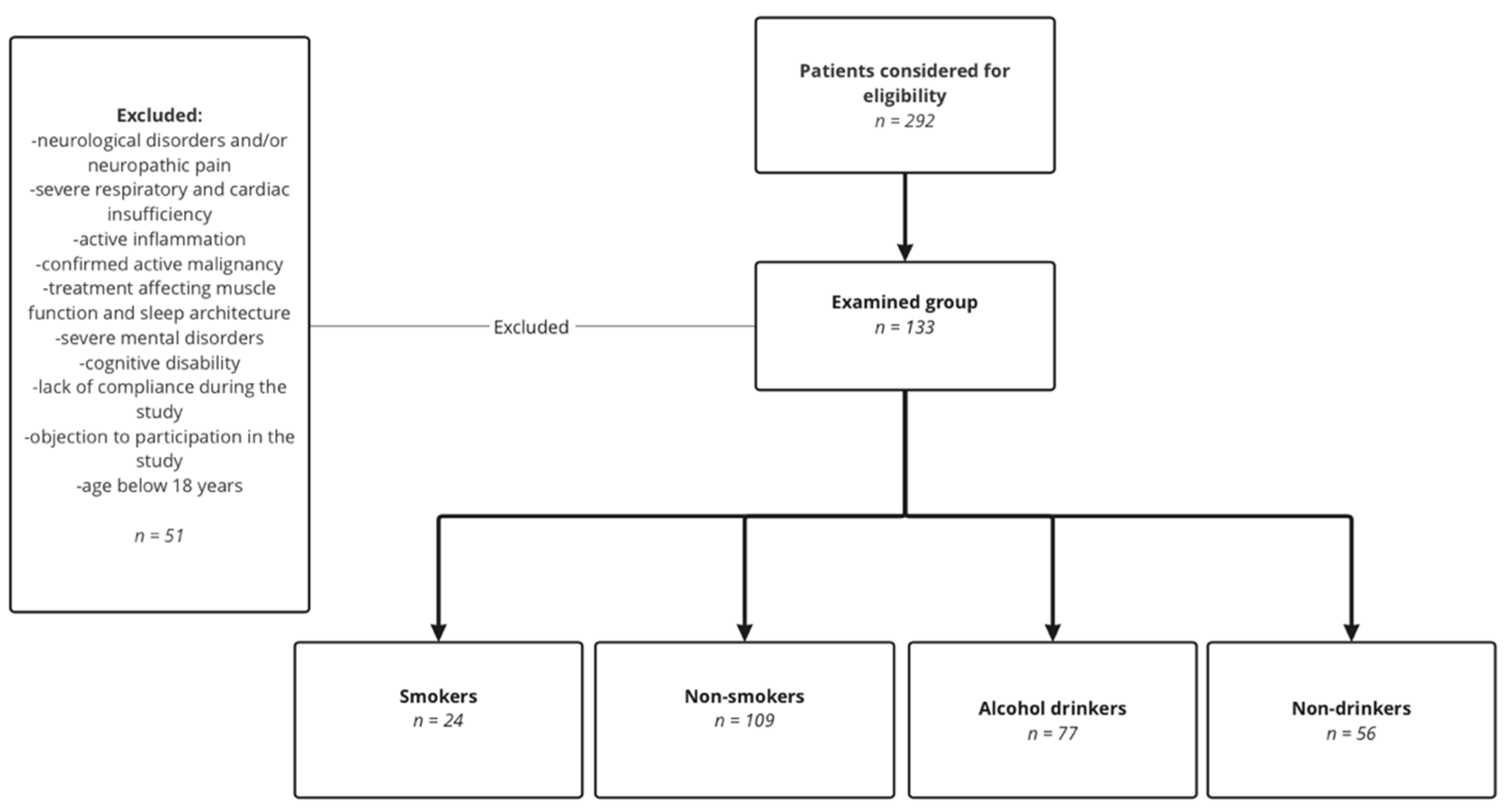
2.1. Inclusion and Exclusion Criteria
2.2. Study Methods and Design
2.3. Data Analysis
3. Results
4. Discussion
4.1. Effects of Smoking on SB
4.2. Effect of Alcohol Intake on SB
4.3. Study Strengths
4.4. Limitations
5. Conclusions
- Tobacco smokers have a higher bruxism intensity, especially the mixed phenotype, in N1 sleep and in the nonsupine position.
- Tobacco smokers have a higher number of bruxism episodes with arousal than nonsmokers, which suggests increased sleep fragmentation.
- Smokers with comorbid sleep-related disorders tend to have electrolyte disturbances and lipid disorders.
- Alcohol consumption has no significant influence on bruxism parameters.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klasser, G.D.; Rei, N.; Lavigne, G.J. Sleep Bruxism Etiology: The Evolution of a Changing Paradigm. J. Can. Dent. Assoc. 2015, 81, 1–8. [Google Scholar]
- Wieckiewicz, M.; Bogunia-Kubik, K.; Mazur, G.; Danel, D.; Smardz, J.; Wojakowska, A.; Poreba, R.; Dratwa, M.; Chaszczewska-Markowska, M.; Winocur, E.; et al. Genetic Basis of Sleep Bruxism and Sleep Apnea—Response to a Medical Puzzle. Sci Rep. 2020, 10, 7497. [Google Scholar] [CrossRef] [PubMed]
- Topical Review: Sleep Bruxism and the Role of Peripheral Sensory Influences—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/14520766/ (accessed on 17 July 2022).
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of Bruxism in Adults: A Systematic Review of the Literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; de Laat, A.; de Leeuw, R.; et al. International Consensus on the Assessment of Bruxism: Report of a Work in Progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Darien, I.L. Sleep Related Bruxism. In International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Castroflorio, T.; Bargellini, A.; Rossini, G.; Cugliari, G.; Deregibus, A. Sleep Bruxism and Related Risk Factors in Adults: A Systematic Literature Review. Arch. Oral Biol. 2017, 83, 25–32. [Google Scholar] [CrossRef]
- Guo, H.; Wang, T.; Niu, X.; Wang, H.; Yang, W.; Qiu, J.; Yang, L. The Risk Factors Related to Bruxism in Children: A Systematic Review and Meta-Analysis. Arch. Oral Biol. 2018, 86, 18–34. [Google Scholar] [CrossRef]
- Cerón, L.; Pacheco, M.; Delgado Gaete, A.; Bravo Torres, W.; Astudillo Rubio, D. Therapies for Sleep Bruxism in Dentistry: A Critical Evaluation of Systematic Reviews. Dent. Med. Probl. 2022. [Google Scholar] [CrossRef]
- Lavigne, G.J.; Khoury, S.; Abe, S.; Yamaguchi, T.; Raphael, K. Bruxism Physiology and Pathology: An Overview for Clinicians. J. Oral Rehabil. 2008, 35, 476–494. [Google Scholar] [CrossRef]
- Manfredini, D.; Lobbezoo, F. Sleep Bruxism and Temporomandibular Disorders: A Scoping Review of the Literature. J. Dent. 2021, 111, 103711. [Google Scholar] [CrossRef]
- Smardz, J.; Martynowicz, H.; Michalek-Zrabkowska, M.; Wojakowska, A.; Mazur, G.; Winocur, E.; Wieckiewicz, M. Sleep Bruxism and Occurrence of Temporomandibular Disorders-Related Pain: A Polysomnographic Study. Front. Neurol. 2019, 10, 168. [Google Scholar] [CrossRef]
- Ohlmann, B.; Waldecker, M.; Leckel, M.; Bömicke, W.; Behnisch, R.; Rammelsberg, P.; Schmitter, M. Correlations between Sleep Bruxism and Temporomandibular Disorders. J. Clin. Med. 2020, 9, 611. [Google Scholar] [CrossRef] [PubMed]
- Michalek-Zrabkowska, M.; Wieckiewicz, M.; Macek, P.; Gac, P.; Smardz, J.; Wojakowska, A.; Poreba, R.; Mazur, G.; Martynowicz, H. The Relationship between Simple Snoring and Sleep Bruxism: A Polysomnographic Study. Int. J. Environ. Res. Public Health 2020, 17, 9860. [Google Scholar] [CrossRef] [PubMed]
- Ommerborn, M.A.; Walentek, N.; Bergmann, N.; Franken, M.; Gotter, A.; Schäfer, R. Validation of a New Diagnostic Method for Quantification of Sleep Bruxism Activity. Clin. Oral Investig. 2022, 26, 4351–4359. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.J.; Rompré, P.H.; Montplaisir, J.Y. Sleep Bruxism: Validity of Clinical Research Diagnostic Criteria in a Controlled Polysomnographic Study. J. Dent. Res. 1996, 75, 546–552. [Google Scholar] [CrossRef]
- Purani, H.; Friedrichsen, S.; Allen, A.M. Sleep Quality in Cigarette Smokers: Associations with Smoking-Related Outcomes and Exercise. Addict. Behav. 2019, 90, 71–76. [Google Scholar] [CrossRef]
- Rintakoski, K.; Ahlberg, J.; Hublin, C.; Broms, U.; Madden, P.A.F.; Könönen, M.; Koskenvuo, M.; Lobbezoo, F.; Kaprio, J. Bruxism Is Associated with Nicotine Dependence: A Nationwide Finnish Twin Cohort Study. Nicotine Tob. Res. 2010, 12, 1254–1260. [Google Scholar] [CrossRef] [Green Version]
- Reitsma, M.B.; Kendrick, P.J.; Ababneh, E.; Abbafati, C.; Abbasi-Kangevari, M.; Abdoli, A.; Abedi, A.; Abhilash, E.S.; Abila, D.B.; Aboyans, V.; et al. Spatial, Temporal, and Demographic Patterns in Prevalence of Smoking Tobacco Use and Attributable Disease Burden in 204 Countries and Territories, 1990–2019: A Systematic Analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef]
- Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; Abegaz, K.H.; Abolhassani, H.; Aboyans, V.; et al. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Kuhn, M.; Türp, J.C. Risk Factors for Bruxism. Swiss Dent. J. 2018, 128, 118–124. [Google Scholar]
- Michalek-Zrabkowska, M.; Wieckiewicz, M.; Smardz, J.; Gac, P.; Poreba, R.; Wojakowska, A.; Mazur, G.; Martynowicz, H. Determination of Inflammatory Markers, Hormonal Disturbances, and Sleepiness Associated with Sleep Bruxism Among Adults. Nat. Sci. Sleep 2020, 12, 969. [Google Scholar] [CrossRef]
- Kondo, T.; Nakano, Y.; Adachi, S.; Murohara, T. Effects of Tobacco Smoking on Cardiovascular Disease. Circ. J. 2019, 83, 1980–1985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Qin, L.Q.; Arafa, A.; Eshak, E.S.; Hu, Y.; Dong, J.Y. Smoking Cessation, Weight Gain, Cardiovascular Risk, and All-Cause Mortality: A Meta-Analysis. Nicotine Tob. Res. 2021, 23, 1987–1994. [Google Scholar] [CrossRef]
- Messner, B.; Bernhard, D. Smoking and Cardiovascular Disease: Mechanisms of Endothelial Dysfunction and Early Atherogenesis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itani, O.; Kaneita, Y.; Ikeda, M.; Kondo, S.; Yamamoto, R.; Osaki, Y.; Kanda, H.; Suzuki, K.; Higuchi, S.; Ohida, T. Disorders of Arousal and Sleep-Related Bruxism among Japanese Adolescents: A Nationwide Representative Survey. Sleep Med. 2013, 14, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.J.; Kato, T.; Kolta, A.; Sessle, B.J. Neurobiologicalmechanisms Involved in Sleep Bruxism. Crit. Rev. Oral Biol. Med. 2003, 14, 30–46. [Google Scholar] [CrossRef] [Green Version]
- Wetselaar, P.; Vermaire, E.J.H.; Lobbezoo, F.; Schuller, A.A. The Prevalence of Awake Bruxism and Sleep Bruxism in the Dutch Adolescent Population. J. Oral Rehabil. 2021, 48, 143. [Google Scholar] [CrossRef]
- Chattrattrai, T.; Blanken, T.F.; Lobbezoo, F.; Su, N.; Aarab, G.; van Someren, E.J.W. A Network Analysis of Self-Reported Sleep Bruxism in the Netherlands Sleep Registry: Its Associations with Insomnia and Several Demographic, Psychological, and Life-Style Factors. Sleep Med. 2022, 93, 63–70. [Google Scholar] [CrossRef] [PubMed]
- van Selms, M.K.A.; Visscher, C.M.; Naeije, M.; Lobbezoo, F. Bruxism and Associated Factors among Dutch Adolescents. Commun. Dent. Oral Epidemiol. 2013, 41, 353–363. [Google Scholar] [CrossRef]
- Toyama, N.; Ekuni, D.; Taniguchi-Tabata, A.; Yoneda, T.; Kataoka, K.; Yokoi, A.; Uchida, Y.; Fukuhara, D.; Saho, H.; Monirul, I.M.; et al. Associations between Sleep Bruxism, Sleep Quality, and Exposure to Secondhand Smoke in Japanese Young Adults: A Cross-Sectional Study. Sleep Med. 2020, 68, 57–62. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Li, K.K.; Guilleminault, C. Risk Factors for Sleep Bruxism in the General Population. Chest 2001, 119, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Winocur, E.; Messer, T.; Eli, I.; Emodi-Perlman, A.; Kedem, R.; Reiter, S.; Friedman-Rubin, P. Awake and Sleep Bruxism Among Israeli Adolescents. Front. Neurol. 2019, 10, 443. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; de Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism Defined and Graded: An International Consensus. J. Oral Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Iber, C. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Walters, A.S.; Lavigne, G.; Hening, W.; Picchietti, D.L.; Allen, R.P.; Chokroverty, S.; Kushida, C.A.; Bliwise, D.L.; Mahowald, M.W.; Schenck, C.H.; et al. The Scoring of Movements in Sleep. J. Clin. Sleep Med. 2007, 3, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Serra-Negra, J.; Carboncini, F.; Lobbezoo, F. Current Concepts of Bruxism. Int. J. Prosthodont. 2017, 30, 437–438. [Google Scholar] [CrossRef] [Green Version]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to Interpret the Results of a Sleep Study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef] [Green Version]
- Khoury, S.; Carra, M.C.; Huynh, N.; Montplaisir, J.; Lavigne, G.J. Sleep Bruxism-Tooth Grinding Prevalence, Characteristics and Familial Aggregation: A Large Cross-Sectional Survey and Polysomnographic Validation. Sleep 2016, 39, 2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neu, D.; Baniasadi, N.; Newell, J.; Styczen, D.; Glineur, R.; Mairesse, O. Effect of Sleep Bruxism Duration on Perceived Sleep Quality in Middle-Aged Subjects. Eur. J. Oral Sci. 2018, 126, 411–416. [Google Scholar] [CrossRef]
- Saito, M.; Yamaguchi, T.; Mikami, S.; Watanabe, K.; Gotouda, A.; Okada, K.; Hishikawa, R.; Shibuya, E.; Shibuya, Y.; Lavigne, G. Weak Association between Sleep Bruxism and Obstructive Sleep Apnea. A Sleep Laboratory Study. Sleep Breath 2016, 20, 703–709. [Google Scholar] [CrossRef]
- Sjöholm, T.T.; Lowe, A.A.; Miyamoto, K.; Fleetham, J.A.; Ryan, C.F. Sleep Bruxism in Patients with Sleep-Disordered Breathing. Arch. Oral Biol. 2000, 45, 889–896. [Google Scholar] [CrossRef]
- Maluly, M.; Andersen, M.L.; Dal-Fabbro, C.; Garbuio, S.; Bittencourt, L.; de Siqueira, J.T.T.; Tufik, S. Polysomnographic Study of the Prevalence of Sleep Bruxism in a Population Sample. J. Dent. Res. 2013, 92, S97–S103. [Google Scholar] [CrossRef]
- Cigarette Smoking as a Risk Factor or an Exacerbating Factor for Restless Legs Syndrome and Sleep Bruxism—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/9231955/ (accessed on 2 September 2022).
- Kostrzewa-Janicka, J.; Jurkowski, P.; Zycinska, K.; Przybyłowska, D.; Mierzwitńska-Nastalska, E. Sleep-Related Breathing Disorders and Bruxism. Adv. Exp. Med. Biol. 2015, 873, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, G.M.; Guerra, P.; di Giovanni, G.; Boselli, M.; Parrino, L.; Terzano, M.G. Sleep Bruxism Is a Disorder Related to Periodic Arousals during Sleep. J. Dent. Res. 1998, 77, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Amiri, S.; Behnezhad, S. Smoking and Risk of Sleep-Related Issues: A Systematic Review and Meta-Analysis of Prospective Studies. Can. J. Public Health 2020, 111, 775. [Google Scholar] [CrossRef]
- Goldstein, G.; DeSantis, L.; Goodacre, C. Bruxism: Best Evidence Consensus Statement. J. Prosthodont. 2021, 30, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Melo, G.; Duarte, J.; Pauletto, P.; Porporatti, A.L.; Stuginski-Barbosa, J.; Winocur, E.; Flores-Mir, C.; de Luca Canto, G. Bruxism: An Umbrella Review of Systematic Reviews. J. Oral Rehabil. 2019, 46, 666–690. [Google Scholar] [CrossRef]
- Bertazzo-Silveira, E.; Kruger, C.M.; Porto De Toledo, I.; Porporatti, A.L.; Dick, B.; Flores-Mir, C.; de Luca Canto, G. Association between Sleep Bruxism and Alcohol, Caffeine, Tobacco, and Drug Abuse: A Systematic Review. J. Am. Dent. Assoc. 2016, 147, 859–866.e4. [Google Scholar] [CrossRef]
- Etiology of Sleep Bruxism: A Review of the Literature—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/18710065/ (accessed on 2 September 2022).
- Ahlberg, J.; Savolainen, A.; Rantala, M.; Lindholm, H.; Könönen, M. Reported Bruxism and Biopsychosocial Symptoms: A Longitudinal Study. Commun. Dent. Oral Epidemiol. 2004, 32, 307–311. [Google Scholar] [CrossRef]
- Rintakoski, K.; Kaprio, J. Legal Psychoactive Substances as Risk Factors for Sleep-Related Bruxism: A Nationwide Finnish Twin Cohort Study. Alcohol Alcohol. 2013, 48, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Martynowicz, H.; Dymczyk, P.; Dominiak, M.; Kazubowska, K.; Skomro, R.; Poreba, R.; Gac, P.; Wojakowska, A.; Mazur, G.; Wieckiewicz, M. Evaluation of Intensity of Sleep Bruxism in Arterial Hypertension. J. Clin. Med. 2018, 7, 327. [Google Scholar] [CrossRef] [Green Version]
- Rom, O.; Avezov, K.; Aizenbud, D.; Reznick, A.Z. Cigarette Smoking and Inflammation Revisited. Respir. Physiol. Neurobiol. 2013, 187, 5–10. [Google Scholar] [CrossRef]
- Tibuakuu, M.; Kamimura, D.; Kianoush, S.; DeFilippis, A.P.; al Rifai, M.; Reynolds, L.M.; White, W.B.; Butler, K.R.; Mosley, T.H.; Turner, S.T.; et al. The Association between Cigarette Smoking and Inflammation: The Genetic Epidemiology Network of Arteriopathy (GENOA) Study. PLoS ONE 2017, 12, e0184914. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Jiang, C.Q.; Xu, L.; Zhang, W.S.; Zhu, F.; Jin, Y.L.; Thomas, G.N.; Cheng, K.K.; Lam, T.H.; Tarantino, G. The Mediating Role of Inflammation in the Association between Cigarette Smoking and Intima-Media Thickness: The Guangzhou Biobank Cohort Study. Medicine 2020, 99, 19207. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, M.; Semprini, M.; Filho, J.E.; de Luca Canto, G.; Regalo, I.H.; Bataglion, C.; Rodrigues, L.A.M.; Siéssere, S.; Regalo, S.C.H. Nocturnal Sleep Architecture Is Altered by Sleep Bruxism. Arch. Oral Biol. 2017, 81, 56–60. [Google Scholar] [CrossRef] [PubMed]
- de Holanda, T.A.; Castagno, C.D.; Barbon, F.J.; Costa, Y.M.; Goettems, M.L.; Boscato, N. Sleep Architecture and Factors Associated with Sleep Bruxism Diagnosis Scored by Polysomnography Recordings: A Case-Control Study. Arch. Oral Biol. 2020, 112, 104685. [Google Scholar] [CrossRef] [PubMed]
- Smardz, J.; Wieckiewicz, M.; Wojakowska, A.; Michalek-Zrabkowska, M.; Poreba, R.; Gac, P.; Mazur, G.; Martynowicz, H. Incidence of Sleep Bruxism in Different Phenotypes of Obstructive Sleep Apnea. J. Clin. Med. 2022, 11, 4091. [Google Scholar] [CrossRef]
- Zhang, W.Z.; Butler, J.J.; Cloonan, S.M. Smoking-Induced Iron Dysregulation in the Lung. Free Radic. Biol. Med. 2019, 133, 238. [Google Scholar] [CrossRef]
- Nakhaee, S.; Amirabadizadeh, A.; Ataei, M.; Ataei, H.; Zardast, M.; Shariatmadari, M.R.; Mousavi-Mirzaei, S.M.; Mehrpour, O. Comparison of Serum Concentrations of Essential and Toxic Elements between Cigarette Smokers and Non-Smokers. Environ. Sci. Pollut. Res. Int. 2021, 28, 37672–37678. [Google Scholar] [CrossRef]
- Vivek, A.; Kaushik, R.M.; Kaushik, R. Tobacco Smoking-Related Risk for Iron Deficiency Anemia: A Case-Control Study. J. Addict. Dis. 2022, 14, 607. [Google Scholar] [CrossRef]
- Salvi, S. Tobacco Smoking and Environmental Risk Factors for Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2014, 35, 17–27. [Google Scholar] [CrossRef]
- Jain, R.B.; Ducatman, A. Associations between Smoking and Lipid/Lipoprotein Concentrations among US Adults Aged ≥20 Years. J. Circ. Biomark. 2018, 7, 1849454418779310. [Google Scholar] [CrossRef] [Green Version]
- Nickol, A.H.; Frise, M.C.; Cheng, H.Y.; McGahey, A.; McFadyen, B.M.; Harris-Wright, T.; Bart, N.K.; Curtis, M.K.; Khandwala, S.; O’Neill, D.P.; et al. A Cross-Sectional Study of the Prevalence and Associations of Iron Deficiency in a Cohort of Patients with Chronic Obstructive Pulmonary Disease. BMJ Open 2015, 5, e007911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, W.; Gao, C.; Zhao, X.; Li, C.; Fan, B.; Lv, J.; Wei, M.; He, L.; Su, C.; Zhang, T. Four-Way Decomposition of Effect of Cigarette Smoking and Body Mass Index on Serum Lipid Profiles. PLoS ONE 2022, 17, e0270486. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Yamamoto, Y.; Imaoka, W.; Kuroshima, T.; Toragai, R.; Ito, Y.; Kanda, E.; Schaefer, E.J.; Ai, M. Relationships between Smoking Status, Cardiovascular Risk Factors, and Lipoproteins in a Large Japanese Population. J. Atheroscler. Thromb. 2021, 28, 942. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W. Association between Dual Smoking and Dyslipidemia in South Korean Adults. PLoS ONE 2022, 17, e0270577. [Google Scholar] [CrossRef] [PubMed]
- Ata, M.A.; Shaikh, S.S.; Iqbal, T.; Hina; Jamil, D.; Khan, R.; Qazi, M.B.; Riwan, T. Inverse Correlation between Serum C-Reactive Protein and Magnesium Levels in Smokers and Nonsmokers. N. Am. J. Med. Sci. 2015, 7, 271. [Google Scholar] [CrossRef] [Green Version]
- Kotlinska-Hasiec, E.; Makara-Studzinska, M.; Czajkowski, M.; Rzecki, Z.; Olszewski, K.; Stadnik, A.; Pilat, J.; Rybojad, B.; Dabrowski, W. Plasma Magnesium Concentration in Patients Undergoing Coronary Artery Bypass Grafting. Ann. Agric. Environ. Med. 2017, 24, 181–184. [Google Scholar] [CrossRef]
- Ortega Anta, R.M.; Jiménez Ortega, A.I.; Martínez García, R.M.; Lorenzo Mora, A.M.; Lozano Estevan, M.D.C. Nutritional Problems in Smokers and Passive Smokers. Nutr. Hosp. 2021, 38, 31–34. [Google Scholar] [CrossRef]
- Simou, E.; Britton, J.; Leonardi-Bee, J. Alcohol and the Risk of Sleep Apnoea: A Systematic Review and Meta-Analysis. Sleep Med. 2018, 42, 38. [Google Scholar] [CrossRef]
- He, S.; Hasler, B.P.; Chakravorty, S. Alcohol and Sleep-Related Problems. Curr. Opin. Psychol. 2019, 30, 117–122. [Google Scholar] [CrossRef]
- Thakkar, M.M.; Sharma, R.; Sahota, P. Alcohol Disrupts Sleep Homeostasis. Alcohol 2015, 49, 299. [Google Scholar] [CrossRef] [Green Version]
- Ebrahim, I.O.; Shapiro, C.M.; Williams, A.J.; Fenwick, P.B. Alcohol and Sleep I: Effects on Normal Sleep. Alcohol Clin. Exp. Res. 2013, 37, 539–549. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Total (n = 133, %) | Smokers (n = 24, %) | Nonsmokers (n = 109, %) | Alcohol Drinkers (n = 77, %) | Nondrinkers (n = 56, %) |
|---|---|---|---|---|---|
| Myocardial infarction | 7, 5% | 5, 20.8% | 2, 1.83% | 5, 6.5% | 2, 3.5% |
| Stroke | 6, 4.5% | 4, 16.6% | 2, 1.83% | 4, 5.2% | 2, 3.5% |
| Hypertension | 52, 39% | 13, 54.2% | 39, 35.7% | 32, 41.5% | 20, 35.7% |
| Diabetes | 24, 18% | 7, 29.2% | 17, 15.6% | 16, 20.7% | 8, 14.3% |
| Ischemic heart disease | 10, 7.5% | 4, 16.6% | 6, 5.5% | 6, 7.8% | 4, 7.1% |
| Parameter | Smokers | Nonsmokers | p | Alcohol Drinkers | Nondrinkers | p |
|---|---|---|---|---|---|---|
| Bruxism episode index (BEI) (n/h) | 5.50 ± 4.71 | 3.83 ± 3.26 | 0.045 | 4.07 ± 3.38 | 4.26 ± 3.96 | 0.750 |
| Phasic episodes (n/h) | 2.88 ± 3.02 | 1.89 ± 2.27 | 0.051 | 2.13 ± 2.23 | 2.01 ± 2.69 | 0.370 |
| Tonic episodes (n/h) | 1.70 ± 1.31 | 1.34 ± 1.27 | 0.130 | 1.32 ± 1.09 | 1.53 ± 1.51 | 0.779 |
| Mixed episodes (n/h) | 0.93 ± 1.00 | 0.59 ± 0.59 | 0.039 | 0.62 ± 0.69 | 0.71 ± 0.72 | 0.538 |
| BEI supine (n/h) | 8.02 ± 8.62 | 6.74 ± 11.25 | 0.291 | 5.70 ± 5.83 | 8.75 ± 15.05 | 0.999 |
| BEI nonsupine (n/h) | 4.93 ± 5.56 | 2.50 ± 2.31 | 0.002 | 3.20 ± 3.71 | 2.58 ± 2.50 | 0.488 |
| BEI N1 (n/h) | 22.85 ± 20.46 | 15.67 ± 13.61 | 0.042 | 17.72 ± 15.38 | 16.10 ± 15.31 | 0.414 |
| BEI N2 (n/h) | 5.34 ± 5.45 | 3.91 ± 4.20 | 0.250 | 3.97 ± 3.87 | 4.46 ± 5.22 | 0.912 |
| BEI N3 (n/h) | 2.05 ± 2.29 | 1.58 ± 1.94 | 0.0540 | 1.73 ± 2.23 | 1.59 ± 1.70 | 0.660 |
| BEI REM (n/h) | 3.54 ± 2.50 | 3.12 ± 2.67 | 0.340 | 3.00 ± 2.43 | 3.48 ± 2.89 | 0.470 |
| Bruxism with arousal (n/h) | 2.91 ± 2.84 | 1.61 ± 1.49 | 0.000006 | 1.84 ± 1.96 | 1.86 ± 1.73 | 0.833 |
| Parameter | Smokers | Nonsmokers | p | Alcohol Drinkers | Nondrinkers | p |
|---|---|---|---|---|---|---|
| AHI (n/h) | 21.23 ± 26.79 | 19.52 ± 22.74 | 0.811 | 17.28 ± 21.14 | 23.28 ± 26.00 | 0.270 |
| ODI (n/h) | 21.11 ± 26.23 | 17.56 ± 20.10 | 0.861 | 16.68 ± 19.90 | 20.28 ± 23.00 | 0.580 |
| Snore (%) | 26.84 ± 24.30 | 19.49 ± 20.23 | 0.246 | 23.01 ± 23.00 | 17.85 ± 18.10 | 0.501 |
| PLMS index (n/h) | 8.33 ± 13.30 | 7.96 ± 18.05 | 0.552 | 10.10 ± 21.40 | 5.21 ± 8.50 | 0.084 |
| SL (min) | 18.81 ± 29.75 | 17.99 ± 18.90 | 0.460 | 15.32 ± 13.52 | 21.96 ± 28.10 | 0.210 |
| REM latency (min) | 97.80 ± 68.10 | 101.70 ± 80.00 | 0.899 | 89.51 ± 56.60 | 116.42 ± 98.00 | 0.218 |
| WASO (min) | 60.03 ± 47.11 | 67.12 ± 64.25 | 0.804 | 56.71 ± 60.23 | 78.20 ± 61.32 | 0.007 |
| SE (%) | 79.73 ± 16.81 | 81.85 ± 13.74 | 0.581 | 83.13 ± 15.00 | 79.21 ± 13.16 | 0.013 |
| N1 (% of TST) | 7.23 ± 5.70 | 6.71 ± 6.50 | 0.647 | 6.53 ± 5.80 | 7.17 ± 7.00 | 0.795 |
| N2 (% of TST) | 46.19 ± 12.72 | 50.43 ± 23.60 | 0.264 | 47.27 ± 10.51 | 52.90 ± 31.43 | 0.498 |
| N3 (% of TST) | 24.00 ± 10.10 | 26.67 ± 27.03 | 0.701 | 23.32 ± 8.20 | 30.10 ± 36.71 | 0.181 |
| REM (% of TST) | 22.60 ± 8.93 | 22.58 ± 9.93 | 0.650 | 22.90 ± 7.50 | 22.18 ± 12.21 | 0.345 |
| AI (n/h) | 9.55 ± 7.76 | 6.75 ± 6.34 | 0.063 | 7.23 ± 7.05 | 7.30 ± 6.19 | 0.732 |
| Parameter | Smokers | Nonsmokers | p | Alcohol Drinkers | Nondrinkers | p |
|---|---|---|---|---|---|---|
| Mg [mmol/L] | 1.85 ± 0.22 | 1.96 ± 0.21 | 0.042 | 1.95 ± 0.21 | 1.93 ± 0.23 | 0.417 |
| Fe [µg/dL] | 96.68 ± 43.58 | 123.83 ± 52.36 | 0.041 | 121.55 ± 48.87 | 113.46 ± 55.15 | 0.408 |
| Na [mmol/L] | 139.92 ± 1.72 | 139.90 ± 2.35 | 0.688 | 139.90 ± 2.35 | 139.92 ± 1.71 | 0.703 |
| K [mmol/L] | 4.31 ± 0.26 | 4.29 ± 0.31 | 0.685 | 4.29 ± 0.28 | 4.30 ± 0.33 | 0.913 |
| Ca [mmol/L | 9.32 ± 0.31 | 9.33 ± 0.31 | 0.752 | 9.31 ± 0.28 | 3.36 ± 0.34 | 0.216 |
| Total cholesterol [mg/dL] | 212.73 ± 56.63 | 196.80 ± 46.31 | 0.154 | 204.52 ± 49.00 | 193.16 ± 47.55 | 0.148 |
| LDL [mg/dL] | 124.86 ± 47.20 | 112.60 ± 39.16 | 0.317 | 119.38 ± 40.66 | 108.33 ± 40.48 | 0.154 |
| HDL [mg/dL] | 54.59 ± 16.42 | 57.43 ± 15.64 | 0.459 | 56.84 ± 15.94 | 56.98 ± 15.64 | 0.804 |
| TG [mg/dL] | 177.68 ± 106.96 | 129.18 ± 65.61 | 0.016 | 143.69 ± 76.02 | 130.81 ± 78.39 | 0.066 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frosztega, W.; Wieckiewicz, M.; Nowacki, D.; Michalek-Zrabkowska, M.; Poreba, R.; Wojakowska, A.; Kanclerska, J.; Mazur, G.; Martynowicz, H. Polysomnographic Assessment of Effects of Tobacco Smoking and Alcohol Consumption on Sleep Bruxism Intensity. J. Clin. Med. 2022, 11, 7453. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247453
Frosztega W, Wieckiewicz M, Nowacki D, Michalek-Zrabkowska M, Poreba R, Wojakowska A, Kanclerska J, Mazur G, Martynowicz H. Polysomnographic Assessment of Effects of Tobacco Smoking and Alcohol Consumption on Sleep Bruxism Intensity. Journal of Clinical Medicine. 2022; 11(24):7453. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247453
Chicago/Turabian StyleFrosztega, Weronika, Mieszko Wieckiewicz, Dorian Nowacki, Monika Michalek-Zrabkowska, Rafal Poreba, Anna Wojakowska, Justyna Kanclerska, Grzegorz Mazur, and Helena Martynowicz. 2022. "Polysomnographic Assessment of Effects of Tobacco Smoking and Alcohol Consumption on Sleep Bruxism Intensity" Journal of Clinical Medicine 11, no. 24: 7453. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm11247453