Comparison of Short-Term Clinical and Pathological Outcomes after Transanal versus Laparoscopic Total Mesorectal Excision for Low Anterior Rectal Resection Due to Rectal Cancer: A Systematic Review with Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Methodology
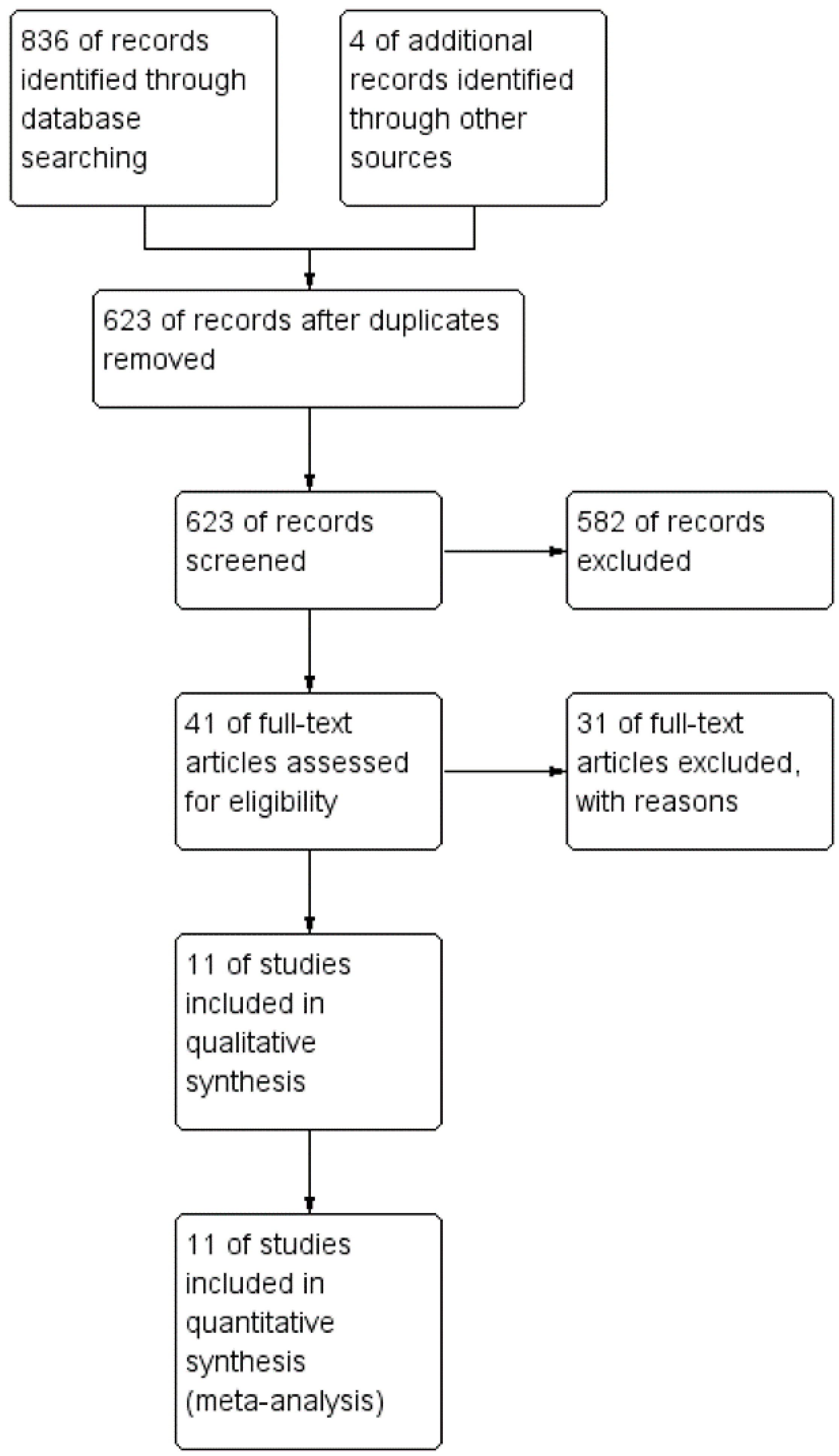
2.1. Search Strategy
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pędziwiatr, M.; Małczak, P.; Mizera, M.; Witowski, J.; Torbicz, G.; Major, P.; Pisarska, M.; Wysocki, M.; Budzyński, A. There is no difference in outcome between laparoscopic and open surgery for rectal cancer: A systematic review and meta-analysis on short- and long-term oncologic outcomes. Tech. Coloproctol. 2017, 21, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Heald, R.J.; Karanjia, N.D. Results of radical surgery for rectal cancer. World J. Surg. 1992, 16, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Heald, R.J.; Moran, B.J.; Ryall, R.D.; Sexton, R.; MacFarlane, J.K. Rectal cancer: The Basingstoke experience of total mesorectal excision, 1978–1997. Arch. Surg. 1998, 133, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Havenga, K.; Enker, W.E.; Norstein, J.; Moriya, Y.; Heald, R.J.; van Houwelingen, H.C.; van de Velde, C.J. Improved survival and local control after total mesorectal excision or D3 lymphadenectomy in the treatment of primary rectal cancer: An international analysis of 1411 patients. Eur. J. Surg. Oncol. 1999, 25, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Creavin, B.; Kelly, M.E.; Ryan, E.; Winter, D.C. Meta-analysis of the impact of surgical approach on the grade of mesorectal excision in rectal cancer. Br. J. Surg. 2017, 104, 1609–1619. [Google Scholar] [CrossRef] [PubMed]
- Rubinkiewicz, M.; Zarzycki, P.; Czerwińska, A.; Wysocki, M.; Gajewska, N.; Torbicz, G.; Budzyński, A.; Pędziwiatr, M. A quest for sphincter-saving surgery in ultralow rectal tumours-a single-centre cohort study. World J. Surg. Oncol. 2018, 16, 218. [Google Scholar] [CrossRef] [PubMed]
- Deijen, C.L.; Velthuis, S.; Tsai, A.; Mavroveli, S.; de Lange-de Klerk, E.S.; Sietses, C.; Tuynman, J.B.; Lacy, A.M.; Hanna, G.B.; Bonjer, H.J. COLOR III: A multicentre randomised clinical trial comparing transanal TME versus laparoscopic TME for mid and low rectal cancer. Surg. Endosc. 2016, 30, 3210–3215. [Google Scholar] [CrossRef] [PubMed]
- Lelong, B.; de Chaisemartin, C.; Meillat, H.; Cournier, S.; Boher, J.M.; Genre, D.; Karoui, M.; Tuech, J.J.; Delpero, J.R. A multicentre randomised controlled trial to evaluate the efficacy, morbidity and functional outcome of endoscopic transanal proctectomy versus laparoscopic proctectomy for low-lying rectal cancer (ETAP-GRECCAR 11 TRIAL): Rationale and design. BMC Cancer 2017, 17, 253. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, J.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 18 November 2018).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Hevia, M.; Delgado, S.; Castells, A.; Tasende, M.; Momblan, D.; Díaz, G.G.; De Lacy, B.; Balust, J.; Lacy, A.M. Transanal total mesorectal excision in rectal cancer: Short-term outcomes in comparison with laparoscopic surgery. Ann. Surg. 2015, 261, 221–227. [Google Scholar] [CrossRef] [PubMed]
- de’Angelis, N.; Portigliotti, L.; Azoulay, D.; Brunetti, F. Transanal total mesorectal excision for rectal cancer: A single center experience and systematic review of the literature. Langenbecks Arch. Surg. 2015, 400, 945–959. [Google Scholar] [CrossRef] [PubMed]
- Lelong, B.; Meillat, H.; Zemmour, C.; Poizat, F.; Ewald, J.; Mege, D.; Lelong, J.C.; Delpero, J.R.; de Chaisemartin, C. Short- and mid-term outcomes after endoscopic transanal or laparoscopic transabdominal total mesorectal excision for low rectal cancer: A single institutional case-control study. J. Am. Coll. Surg. 2017, 224, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-C.; Kiu, K.-T. Transanal total mesorectal excision in lower rectal cancer: Comparison of short-term outcomes with conventional laparoscopic total mesorectal excision. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-C.; Lai, Y.-L.; Jiang, J.-K.; Chu, C.-H.; Huang, I.-P.; Chen, W.-S.; Cheng, A.-Y.; Yang, S.-H. Transanal total mesorectal excision versus laparoscopic surgery for rectal cancer receiving neoadjuvant chemoradiation: A matched case-control study. Ann. Surg. Oncol. 2016, 23, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Rasulov, A.O.; Mamedli, Z.Z.; Gordeyev, S.S.; Kozlov, N.A.; Dzhumabaev, H.E. Short-term outcomes after transanal and laparoscopic total mesorectal excision for rectal cancer. Tech. Coloproctol. 2016, 20, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Chouillard, E.; Regnier, A.; Vitte, R.L.; Bonnet, B.V.; Greco, V.; Chahine, E.; Daher, R.; Biaqini, J. Transanal NOTES total mesorectal excision (TME) in patients with rectal cancer: Is anatomy better preserved? Tech. Coloproctol. 2016, 20, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Mege, D.; Hain, E.; Lakkis, Z.; Maggiori, L.; Prost À la Denise, J.; Panis, Y. Is trans-anal total mesorectal excision really safe and better than laparoscopic total mesorectal excision with a perineal approach first in patients with low rectal cancer? A learning curve with case-matched study in 68 patients. Colorectal Dis. 2018, 20, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Persiani, R.; Biondi, A.; Pennestrì, F.; Fico, V.; De Simone, V.; Tirelli, F.; Santullo, F.; D’Ugo, D. Transanal total mesorectal excision vs laparoscopic total mesorectal excision in the treatment of low and middle rectal cancer: A propensity score matching analysis. Dis. Colon Rectum 2018, 61, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Veltcamp Helbach, M.; Koedam, T.W.A.; Knol, J.J.; Velthuis, S.; Bonjer, H.J.; Tuynman, J.B.; Sietses, C. Quality of life after rectal cancer surgery: Differences between laparoscopic and transanal total mesorectal excision. Surg. Endosc. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rubinkiewicz, M.; Nowakowski, M.; Wierdak, M.; Mizera, M.; Dembiński, M.; Pisarska, M.; Major, P.; Małczak, P.; Budzyński, A.; Pędziwiatr, M. Transanal Total Mesorectal Excision for Low Rectal Cancer: A Case-Matched Study Comparing TaTME versus Standard Laparoscopic TME. Cancer Manag. Res. 2018, 10, 5239–5245. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Fleshman, J.; Branda, M.; Sargent, D.J.; Boller, A.M.; George, V.; Abbas, M.; Peters, W.R., Jr.; Maun, D.; Chang, G.; Herline, A.; et al. Effect of laparoscopic-assisted resection vs open resection of stage II or III rectal cancer on pathologic outcomes: The ACOSOG Z6051 randomized clinical trial. JAMA 2015, 314, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, A.R.; Solomon, M.J.; Lumley, J.W.; Hewett, P.; Clouston, A.D.; Gebski, V.J.; Davies, L.; Wilson, K.; Haque, W.; Simes, J. Effect of laparoscopic-assisted resection vs open resection on pathological outcomes in rectal cancer: The ALaCaRT randomized clinical trial. JAMA 2015, 314, 1356–1363. [Google Scholar] [CrossRef] [PubMed]
- Piątkowski, J.; Jackowski, M.; Szeliga, J. Laparoscopic surgery of esophageal hiatus hernia—Single center experience. Videosurg. Other Miniinvasive Tech. 2014, 9, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Jin, P.; Hu, L.; Liu, W.; Zhang, W.; Guo, T.; Yang, X. The application of transanal total mesorectal excision for patients with middle and low rectal cancer. Medicine 2018, 97, e11410. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.P.; Li, Y.S.; Wang, B.; Wang, C.; Liu, F.; Shen, Z.L.; Ye, Y.J.; Wang, S. Pathological outcomes of transanal versus laparoscopic total mesorectal excision for rectal cancer: A systematic review with meta-analysis. Surg. Endosc. 2018, 32, 2632–2642. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.; Gao, P.; Song, Y.; Zhang, C.; Zhang, C.; Wang, L.; Liu, H.; Wang, Z. Transanal total mesorectal excision (taTME) for rectal cancer: A systematic review and meta-analysis of oncological and perioperative outcomes compared with laparoscopic total mesorectal excision. BMC Cancer 2016, 16, 380. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Gao, Y.; Dai, X.; Zhang, H.; Shang, Z.; Cai, X.; Shen, T.; Cheng, X.; Yu, K.; Li, Y. Short- and long-term outcomes of transanal versus laparoscopic total mesorectal excision for mid-to-low rectal cancer: A meta-analysis. Surg. Endosc. 2018. [Google Scholar] [CrossRef] [PubMed]
- Koedam, T.W.A.; Veltcamp Helbach, M.; Penna, M.; Wijsmuller, A.; Doornebosch, P.; van Westreenen, H.L.; Hompes, R.; Bonjer, H.J.; Sietses, C.; de Graaf, E.; et al. Short-term outcomes of transanal completion total mesorectal excision (cTaTME) for rectal cancer: A case-matched analysis. Surg. Endosc. 2018. [Google Scholar] [CrossRef] [PubMed]
- Velthuis, S.; Nieuwenhuis, D.H.; Ruijter, T.E.; Cuesta, M.A.; Bonjer, H.J.; Sietses, C. Transanal versus traditional laparoscopic total mesorectal excision for rectal carcinoma. Surg. Endosc. 2014, 28, 3494–3499. [Google Scholar] [CrossRef] [PubMed]
- Marks, J.H.; Montenegro, G.A.; Salem, J.F.; Shields, M.V.; Marks, G.J. Transanal TATA/TME: A case-matched study of taTME versus laparoscopic TME surgery for rectal cancer. Tech. Coloproctol. 2016, 20, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Perdawood, S.K.; Thinggaard, B.S.; Bjoern, M.X. Effect of transanal total mesorectal excision for rectal cancer: Comparison of short-term outcomes with laparoscopic and open surgeries. Surg Endosc. 2017, 32, 2312–2321. [Google Scholar] [CrossRef] [PubMed]
- Denost, Q.; Adam, J.P.; Rullier, A.; Buscail, E.; Laurent, C.; Rullier, E. Perineal transanal approach: A new standard for laparoscopic sphincter-saving resection in low rectal cancer, a randomized trial. Ann. Surg. 2014, 260, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Adamina, M.; Buchs, N.C.; Penna, M.; Hompes, R. St. Gallen consensus on safe implementation of transanal total mesorectal excision. Surg Endosc. 2018, 32, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Sylla, P.; Rattner, D.W.; Delgado, S.; Lacy, A.M. NOTES transanal rectal cancer resection using transanal endoscopic microsurgery and laparoscopic assistance. Surg Endosc. 2010, 24, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Kanso, F.; Maggiori, L.; Debove, C.; Chau, A.; Ferron, M.; Panis, Y. Perineal or abdominal approach first during intersphincteric resection for low rectal cancer: Which is the best strategy? Dis. Colon Rectum 2015, 58, 637–644. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, G.; Paganini, A.M.; Balla, A.; Quaresima, S.; Ursi, P.; Bruzzone, P.; Picchetto, A.; Mattei, F.I.; Lezoche, E. Quality of life in non-early rectal cancer treated by neoadjuvant radio-chemotherapy and endoluminal loco-regional resection (ELRR) by transanal endoscopic microsurgery (TEM) versus laparoscopic total mesorectal excision. Surg. Endosc. 2016, 30, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Martin-Perez, B.; Otero-Piñeiro, A.; Lacy, A.M. Purse-string rupture: Pitfalls of transanal total mesorectal excision (Cecil approach). Tech. Coloproctol. 2018, 22, 393–394. [Google Scholar] [CrossRef] [PubMed]
- Penna, M.; Hompes, R.; Arnold, S.; Wynn, G.; Austin, R.; Warusavitarne, J.; Moran, B.; Hanna, G.B.; Mortensen, N.J.; Tekkis, P.P. Transanal Total Mesorectal Excision: International Registry Results of the First 720 Cases. Ann. Surg. 2017, 266, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Arroyave, M.C.; DeLacy, F.B.; Lacy, A.M. Transanal total mesorectal excision (TaTME) for rectal cancer: Step by step description of the surgical technique for a two-teams approach. Eur. J. Surg. Oncol. 2017, 43, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Lacy, A.M.; Tasende, M.M.; Delgado, S.; Fernandez-Hevia, M.; Jimenez, M.; De Lacy, B.; Castells, A.; Bravo, R.; Wexner, S.D.; Heald, R.J. Transanal total mesorectal excision for rectal cancer: Outcomes after 140 patients. J. Am. Coll. Surg. 2015, 221, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Kitz, J.; Fokas, E.; Beissbarth, T.; Ströbel, P.; Wittekind, C.; Hartmann, A.; Rüschoff, J.; Papadopoulos, T.; Rösler, E.; Ortloff-Kittredge, P.; et al. Association of plane of total mesorectal excision with prognosis of rectal cancer: Secondary analysis of the CAO/ARO/AIO-04 Phase 3 RANDOMIZED CLINICAL TRIAL. JAMA Surg. 2018, 153, e181607. [Google Scholar] [CrossRef] [PubMed]
- Koedam, T.W.A.; Veltcamp Helbach, M.; van de Ven, P.M.; Kruyt, P.M.; van Heek, N.T.; Bonjer, H.J.; Tuynman, J.B.; Sietses, C. Transanal total mesorectal excision for rectal cancer: Evaluation of the learning curve. Tech. Coloproctol. 2018, 22, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, T.L.; Brinkley, J.; Zervos, E.E. Pushing the envelope beyond a centimeter in rectal cancer: Oncologic implications of close, but negative margins. J. Am. Coll. Surg. 2011, 213, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Glimelius, B.; Tiret, E.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 28, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.J.; Chi, P.; Zhang, Y.Y.; Lin, H.M.; Lu, X.R.; Huang, Y.; Xu, Z.B.; Ghareeb, W.M.; Huang, S.H.; Sun, Y.W.; et al. Survival outcome of adjuvant radiotherapy after local excision for T2 early rectal cancer: An analysis based on the surveillance, epidemiology, and end result registry database. Eur. J. Surg. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Leijtens, J.W.A.; Koedam, T.W.A.; Borstlap, W.A.A.; Maas, M.; Doornebosch, P.G.; Karsten, T.M.; Derksen, E.J.; Stassen, L.P.S.; Rosman, C.; de Graaf, E.J.R.; et al. Transanal endoscopic microsurgery with or without completion total mesorectal excision for T2 and T3 rectal carcinoma. Dig. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.G.; Malcomson, L.; Emsley, R.; Gollins, S.; Maw, A.; Myint, A.S.; Rooney, P.S.; Susnerwala, S.; Blower, A.; Saunders, M.P.; et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): A propensity-score matched cohort analysis. Lancet Oncol. 2016, 17, 174–183. [Google Scholar] [CrossRef]
- Dossa, F.; Chesney, T.R.; Acuna, S.A.; Baxter, N.N. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 501–513. [Google Scholar] [CrossRef]
- Quirke, P.; Morris, E. Reporting colorectal cancer. Histopathology 2007, 50, 103–112. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Country | Study Design | N TaTME/Lap | % Male TaTME/Lap | Age TaTME/Lap | Distance to Anal Verge TaTME/Lap [mm] | T0–T2/T3–T4 TaTME | T0–T2/T3–T4 Lap | NOS |
|---|---|---|---|---|---|---|---|---|---|---|
| Fernandez-Hevia [13] | 2015 | Spain | C | 37/37 | 65/59 | 64.5/69.5 | ND | 8/28 | 10/24 | 9 |
| de’Angelis [14] | 2015 | France | CM | 32/32 | 66/66 | 64.91/67.16 | 4/3.7 | 13/19 | 16/16 | 8 |
| Lelong [15] | 2016 | France | C | 34/48 | 68/58 | ND | ND | 19/15 | 27/11 | 9 |
| Chang [16] | 2017 | China | C | 23/23 | 57/57 | 62.4/62.9 | 4.3/5.9 | ND | ND | 8 |
| Chen [17] | 2016 | China | C | 50/100 | 76/76 | 57.3/58.3 | 5.8/6.7 | ND | ND | 9 |
| Rasulov [18] | 2016 | Russia | C | 22/23 | 50/61 | 56/60 | ND | 5/17 | 7/16 | 9 |
| Chouilard [19] | 2016 | France | C | 18/15 | 33/47 | 55.4/57.8 | <70/<70 | 10/8 | 8/7 | 9 |
| Mege [20] | 2018 | France | CM | 34/34 | 68/68 | 58/59 | 13/22 | 10/24 | 17/12 | 9 |
| Persiani [21] | 2018 | Italy | CM | 46/46 | 65/67 | 69/66.5 | 55/60 | ND | ND | 8 |
| Veltcamp [22] | 2018 | Netherlands | C | 27/27 | 67/74 | 68/67.2 | ND | 16/11 | 15/12 | 8 |
| Rubinkiewicz [23] | 2018 | Poland | CM | 35/35 | 35/35 | 64.3/60.3 | 29/31.9 | 21/14 | 24/11 | 9 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubinkiewicz, M.; Czerwińska, A.; Zarzycki, P.; Małczak, P.; Nowakowski, M.; Major, P.; Budzyński, A.; Pędziwiatr, M. Comparison of Short-Term Clinical and Pathological Outcomes after Transanal versus Laparoscopic Total Mesorectal Excision for Low Anterior Rectal Resection Due to Rectal Cancer: A Systematic Review with Meta-Analysis. J. Clin. Med. 2018, 7, 448. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110448
Rubinkiewicz M, Czerwińska A, Zarzycki P, Małczak P, Nowakowski M, Major P, Budzyński A, Pędziwiatr M. Comparison of Short-Term Clinical and Pathological Outcomes after Transanal versus Laparoscopic Total Mesorectal Excision for Low Anterior Rectal Resection Due to Rectal Cancer: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2018; 7(11):448. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110448
Chicago/Turabian StyleRubinkiewicz, Mateusz, Agata Czerwińska, Piotr Zarzycki, Piotr Małczak, Michał Nowakowski, Piotr Major, Andrzej Budzyński, and Michał Pędziwiatr. 2018. "Comparison of Short-Term Clinical and Pathological Outcomes after Transanal versus Laparoscopic Total Mesorectal Excision for Low Anterior Rectal Resection Due to Rectal Cancer: A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 7, no. 11: 448. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110448