Associations with the In-Hospital Survival Following Extracorporeal Membrane Oxygenation in Adult Acute Fulminant Myocarditis


Abstract
:1. Introduction
2. Experimental Section
2.1. Patients and Groups
2.2. Definitions
2.3. Intra-Aortic Balloon Pumping (IABP), ECMO, and Distal Perfusion Device Criteria
2.4. Study Endpoint
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Comparisons of Baseline Characteristics between the Survival Group and Non-Survival Group
3.3. Univariate and Multivariate Cox Regression Analyses for In-Hospital Mortality
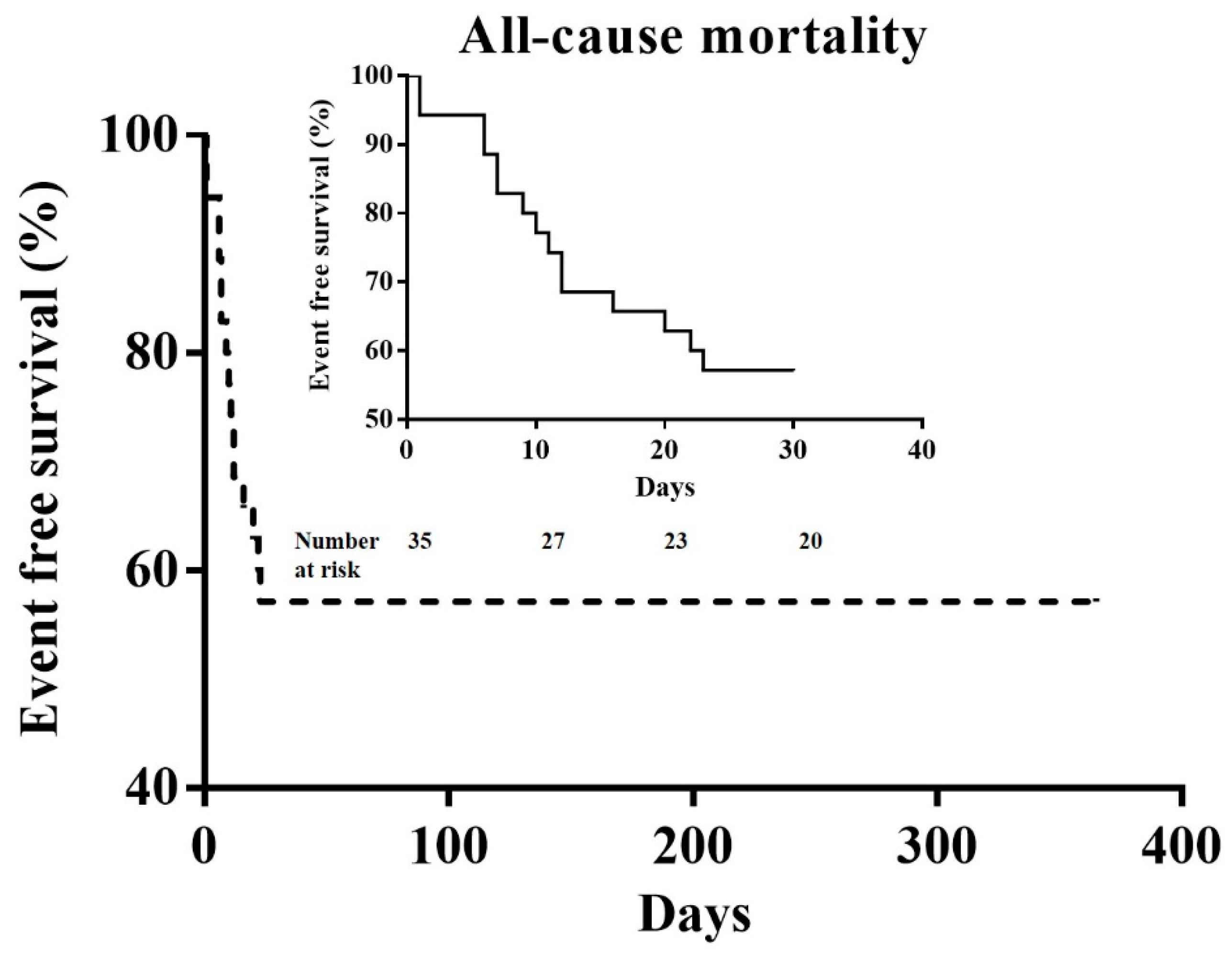
3.4. Kaplan–Meier Survival Curve of In-Hospital Mortality
3.5. The Reasons for All-Cause Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cooper, L.T., Jr. Myocarditis. N. Engl. J. Med. 2009, 360, 1526–1538. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr.; Keren, A.; Sliwa, K.; Matsumori, A.; Mensah, G.A. The global burden of myocarditis: Part 1: A systematic literature review for the Global Burden of Diseases, Injuries, and Risk Factors 2010 study. Glob. Heart 2014, 9, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Elamm, C.; Fairweather, D.; Cooper, L.T. Pathogenesis and diagnosis of myocarditis. Heart 2012, 98, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Fayssoil, A.; Nardi, O.; Orlikowski, D.; Combes, A.; Chastre, J.; Annane, D. Percutaneous extracorporeal membrane oxygenation for cardiogenic shock due to acute fulminant myocarditis. Ann. Thorac. Surg. 2010, 89, 614–616. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Cipriani, M.; Lilliu, M.; Sormani, P.; Varrenti, M.; Raineri, C.; Petrella, D.; Garascia, A.; Pedrotti, P.; Roghi, A.; et al. Survival and Left Ventricular Function Changes in Fulminant Versus Nonfulminant Acute Myocarditis. Circulation 2017, 136, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Pozzi, M.; Banfi, C.; Grinberg, D.; Koffel, C.; Bendjelid, K.; Robin, J.; Giraud, R.; Obadia, J.F. Veno-arterial extracorporeal membrane oxygenation for cardiogenic shock due to myocarditis in adult patients. J. Thorac. Dis. 2016, 8, E495–E502. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, N.; Izumi, T.; Hiramori, K.; Isobe, M.; Kawana, M.; Hiroe, M.; Hishida, H.; Kitaura, Y.; Imaizumi, T. Japanese Investigators of Fulminant Myocarditis. National survey of fulminant myocarditis in Japan: Therapeutic guidelines and long-term prognosis of using percutaneous cardiopulmonary support for fulminant myocarditis (special report from a scientific committee). Circ. J. 2002, 66, 133–144. [Google Scholar] [PubMed]
- Miyake, C.Y.; Teele, S.A.; Chen, L.; Motonaga, K.S.; Dubin, A.M.; Balasubramanian, S.; Balise, R.R.; Rosenthal, D.N.; Alexander, M.E.; Walsh, E.P.; et al. In-hospital arrhythmia development and outcomes in pediatric patients with acute myocarditis. Am. J. Cardiol. 2014, 113, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Sankar, J.; Khalil, S.; Jeeva Sankar, M.; Kumar, D.; Dubey, N. Short-term outcomes of acute fulminant myocarditis in children. Pediatr. Cardiol. 2011, 32, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.P.; Lin, M.J.; Yang, W.C.; Wu, K.H.; Chen, C.Y. Predictors of Extracorporeal Membrane Oxygenation Support for Children with Acute Myocarditis. Biomed. Res. Int. 2017, 2017, 2510695. [Google Scholar] [CrossRef] [PubMed]
- Shauer, A.; Gotsman, I.; Keren, A.; Zwas, D.R.; Hellman, Y.; Durst, R.; Admon, D. Acute viral myocarditis: Current concepts in diagnosis and treatment. Isr. Med. Assoc. J. 2013, 15, 180–185. [Google Scholar] [PubMed]
- Kindermann, I.; Barth, C.; Mahfoud, F.; Ukena, C.; Lenski, M.; Yilmaz, A.; Klingel, K.; Kandolf, R.; Sechtem, U.; Cooper, L.T.; et al. Update on myocarditis. J. Am. Coll. Cardiol. 2012, 28, 779–792. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, F.; Kühl, U.; Pieske, B.; Garcia-Pavia, P.; Tschöpe, C. Update on Myocarditis and Inflammatory Cardiomyopathy: Reemergence of Endomyocardial Biopsy. Rev. Esp. Cardiol. 2016, 69, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef] [PubMed]
- Makdisi, G.; Wang, I.-W. Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. J. Thorac Dis. 2015, 7, E166–E176. [Google Scholar] [PubMed]
- Zhong, Z.P.; Wang, H.; Hou, X.T. Extracorporeal Membrane Oxygenation as a Bridge for Heart Failure and Cardiogenic Shock. Biomed. Res. Int. 2016, 2016, 7263187. [Google Scholar] [CrossRef] [PubMed]
- Asaumi, Y.; Yasuda, S.; Morii, I.; Kakuchi, H.; Otsuka, Y.; Kawamura, A.; Sasako, Y.; Nakatani, T.; Nonogi, H.; Miyazaki, S. Favourable clinical outcome in patients with cardiogenic shock due to fulminant myocarditis supported by percutaneous extracorporeal membrane oxygenation. Eur. Heart J. 2005, 26, 2185–2192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotani, Y.; Chetan, D.; Rodrigues, W.; Sivarajan, V.B.; Gruenwald, C.; Guerguerian, A.M.; Van Arsdell, G.S.; Honjo, O. Left atrial decompression during venoarterial extracorporeal membrane oxygenation for left ventricular failure in children: Current strategy and clinical outcomes. Artif. Organs 2013, 37, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.N.; Chen, Y.H.; Wang, H.J.; Hung, J.S.; Chang, K.C.; Lo, P.H. Atrial Septostomy for Left Atrial Decompression During Extracorporeal Membrane Oxygenation by Inoue Balloon Catheter. Circ. J. 2017, 25, 1419–1423. [Google Scholar] [CrossRef] [PubMed]
- Meani, P.; Gelsomino, S.; Natour, E.; Johnson, D.M.; Rocca, H.B.; Pappalardo, F.; Bidar, E.; Makhoul, M.; Raffa, G.; Heuts, S.; et al. Modalities and Effects of Left Ventricle Unloading on Extracorporeal Life support: A Review of the Current Literature. Eur. J. Heart Fail. 2017, 19 (Suppl. 2), 84–91. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosyula, S.; O’Horo, J.C.; Antharam, P.; Ananthaneni, S.; Vallabhajosyula, S.; Stulak, J.M.; Eleid, M.F.; Dunlay, S.M.; Gersh, B.J.; Rihal, C.S.; et al. Concomitant Intra-Aortic Balloon Pump Use in Cardiogenic Shock Requiring Veno-Arterial Extracorporeal Membrane Oxygenation. Circ. Cardiovasc. Interv. 2018, 11, e006930. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Ishida, K.; Taniguchi, Y.; Nakagawa, T.; Seguchi, M.; Wada, H.; Sugawara, Y.; Funayama, H.; Mitsuhashi, T.; Momomura, S.-I. Prognosis of patients with fulminant myocarditis managed by peripheral venoarterial extracorporeal membranous oxygenation support: A retrospective single-center study. J. Intensive Care 2015, 3, 5. [Google Scholar] [CrossRef] [PubMed]
- Unosawa, S.; Hata, M.; Sezai, A.; Niino, T.; Yoshitake, I.; Shimura, K.; Takamori, T.; Minami, K. Successful management of fulminant myocarditis with left ventricular assist device: Report of a severe case. Ann. Thorac. Cardiovasc. Surg. 2010, 16, 48–51. [Google Scholar] [PubMed]
- Imamura, T.; Kinugawa, K.; Shiga, T.; Endo, M.; Kato, N.; Inaba, T.; Maki, H.; Hatano, M.; Yao, A.; Nishimura, T.; et al. Preoperative levels of bilirubin or creatinine adjusted by age can predict their reversibility after implantation of left ventricular assist device. Circ. J. 2013, 77, 96–104. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Survival Group (n = 20) | Non-Survival Group (n = 15) | p Value | |
|---|---|---|---|
| General demographics | |||
| Age (years) | 40.00 ± 14.73 | 41.53 ± 14.97 | 0.764 |
| Male sex (%) | 9 (45.0) | 9 (60.0) | 0.500 |
| Risk factors | |||
| Diabetes mellitus (%) | 1 (5.0) | 1 (6.7) | 0.833 |
| Hypertension (%) | 2 (10.0) | 1 (6.7) | 0.727 |
| Chronic kidney disease (%) | 2 (10.0) | 0 (0) | 0.496 |
| Thyroid dysfunction (%) | 3 (15.0) | 1 (6.7) | 0.619 |
| The severity of hemodynamic condition | |||
| Out-hospital cardiac arrest (OHCA) (%) | 2 (10.0) | 4 (26.7) | 0.367 |
| CPR (%) | 8 (40.0) | 7 (46.7) | 0.741 |
| SBP (mmHg) | 82.55 ± 34.23 | 67.33 ± 43.18 | 0.253 |
| SBP < 80 mmHg (%) (except OHCA) | 4 (22.2) | 4 (36.4) | 0.433 |
| HR (beats/min) | 95.10 ± 44.89 | 86.40 ± 53.58 | 0.605 |
| HR > 120 beats/min (%) (except OHCA) | 5 (27.8) | 6 (50.0) | 0.266 |
| The number of inotropic agents use | 0.700 ± 0.656 | 1.133 ± 0.516 | 0.043 |
| Cardiac rhythm | |||
| AV block | 9 (45.0) | 7 (46.7) | 0.922 |
| VT/VF | 8 (50.0) | 7 (46.7) | 0.741 |
| Other supportive agents | |||
| IABP (%) | 17 (85.0) | 11 (73.3) | 0.430 |
| Ventilator (%) | 14 (70.0) | 14 (93.3) | 0.199 |
| Temporary pacemaker (%) | 9 (45.0) | 6 (40.0) | 0.767 |
| Laboratory examination | |||
| White blood cell count (×103) | 14.11 ± 7.96 | 12.56 ± 5.94 | 0.543 |
| Hemoglobin (g/dL) | 12.59 ± 2.57 | 12.41 ± 2.90 | 0.853 |
| Platelet (×103) | 205.18 ± 96.64 | 149.39 ± 84.60 | 0.095 |
| BUN (mg/dL) | 28.12 ± 17.56 | 29.93 ± 19.96 | 0.834 |
| Creatinine (mg/dL) | 1.80 ± 0.77 | 2.26 ± 0.47 | 0.437 |
| AST (U/L) | 1024.14 ± 794.24 | 1757.45 ± 722.92 | 0.517 |
| ALT (U/L) | 390.83 ± 156.49 | 829.46 ± 160.71 | 0.354 |
| Total bilirubin (mg/dL) | 1.15 ± 0.65 | 1.75 ± 1.05 | 0.089 |
| CRP (mg/dL) | 83.10 ± 47.01 | 82.84 ± 46.97 | 0.995 |
| Lactate acid (initial) (mg/dL) | 27.48 ± 11.53 | 67.59 ± 55.77 | 0.018 |
| Lactate acid (24 h) (mg/dL) | 16.93 ± 8.44 | 49.95 ± 33.38 | 0.001 |
| Peak Troponin-I (ng/mL) | 17.90 ± 6.03 | 62.87 ± 28.89 | 0.058 |
| Peak CK-MB (ng/mL) | 61.31 ± 29.78 | 233.40 ± 204.32 | 0.005 |
| pH value of arterial gas | 7.40 ± 0.11 | 7.20 ± 0.22 | 0.004 |
| Parameters of cardiac echo | |||
| LA dimension (mm) | 31.38 ± 5.69 | 28.75 ± 5.08 | 0.218 |
| LVESV (mL) | 75.13 ± 32.01 | 73.67 ± 27.67 | 0.901 |
| LVEDV (mL) | 114.06 ± 45.66 | 103.67 ± 39.24 | 0.533 |
| LVEF (%) | 30.06 ± 12.19 | 27.42 ± 12.94 | 0.575 |
| The incidence of acute kidney injury (%) | 12 (60.0) | 14 (93.3) | 0.048 |
| The need of hemodialysis (%) | 4 (20.0) | 11 (73.3) | 0.002 |
| The incidence of hypoxic encephalopathy (%) | 2 (10.0) | 5 (33.3) | 0.112 |
| The duration of shock to ECMO use (minutes) | 182.06 ± 128.09 | 173.53 ± 138.89 | 0.858 |
| The duration of ECMO use (days) | 6.56 ± 4.26 | 9.50 ± 6.37 | 0.111 |
| The need of LV venting (%) | 2 (10.0) | 2 (13.3) | 0.759 |
| The complication of ECMO (%) | 9 (45.0) | 11 (73.3) | 0.167 |
| Ischemic leg (%) | 4 (20.0) | 8 (53.3) | 0.071 |
| The need of distal perfusion device (%) | 4 (20.0) | 4 (26.7) | 0.700 |
| Bleeding (%) | 7 (35.0) | 7 (46.7) | 0.511 |
| ICH (%) | 1 (5.0) | 4 (26.7) | 0.141 |
| Univariate Analyses | Multivariate Analyses | |||||
|---|---|---|---|---|---|---|
| Variables | Hazard Ratio | 95% CI | p Value | Hazard Ratio | 95% CI | p Value |
| Age > 60-year-old | 2.060 | 0.271–15.675 | 0.485 | |||
| Male gender | 1.730 | 0.614–4.874 | 0.299 | |||
| Shock to ECMO time (mins) | 1.000 | 0.996–1.004 | 0.928 | |||
| OHCA | 1.989 | 0.629–6.289 | 0.242 | |||
| CPR | 1.154 | 0.418–3.185 | 0.783 | |||
| SBP < 80 mmHg | 2.139 | 0.675–6.782 | 0.196 | |||
| HR > 120 beats/min | 2.120 | 0.682–6.587 | 0.194 | |||
| Cardiac rhythm as VT/VF | 1.154 | 0.418–3.185 | 0.783 | |||
| Platelet (×103) | 0.996 | 0.990–1.002 | 0.160 | |||
| Total bilirubin (mg/dL) | 1.498 | 0.965–2.325 | 0.072 | |||
| Lactate acid (initial) (mg/dL) | 1.020 | 1.006–1.033 | 0.003 | |||
| Lactate acid (24 h) (mg/dL) | 1.057 | 1.029–1.086 | <0.001 | 1.064 | 1.029–1.099 | <0.001 |
| Peak Troponin-I (ng/mL) | 1.009 | 1.001–1.016 | 0.032 | 1.014 | 1.004–1.024 | 0.008 |
| Peak CK-MB (ng/mL) | 1.005 | 1.002–1.008 | <0.001 | |||
| pH value of arterial gas | 0.064 | 0.008–0.527 | 0.011 | |||
| LVEF (%) | 0.988 | 0.944–1.033 | 0.592 | |||
| Acute kidney injury (%) | 6.485 | 0.851–49.417 | 0.071 | |||
| The need of hemodialysis (%) | 5.744 | 1.807–18.254 | 0.003 | |||
| Hypoxic encephalopathy (%) | 3.623 | 1.220–10.763 | 0.020 | |||
| Ischemic leg (%) | 2.389 | 0.864–6.607 | 0.093 | |||
| ICH (%) | 2.853 | 0.110–1.119 | 0.077 | |||
| Prior IABP setting (%) | 0.676 | 0.215–2.127 | 0.503 | |||
| The need of LV venting (%) | 1.107 | 0.249–4.915 | 0.893 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chong, S.-Z.; Fang, C.-Y.; Fang, H.-Y.; Chen, H.-C.; Chen, C.-J.; Yang, C.-H.; Hang, C.-L.; Yip, H.-K.; Wu, C.-J.; Lee, W.-C. Associations with the In-Hospital Survival Following Extracorporeal Membrane Oxygenation in Adult Acute Fulminant Myocarditis. J. Clin. Med. 2018, 7, 452. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110452
Chong S-Z, Fang C-Y, Fang H-Y, Chen H-C, Chen C-J, Yang C-H, Hang C-L, Yip H-K, Wu C-J, Lee W-C. Associations with the In-Hospital Survival Following Extracorporeal Membrane Oxygenation in Adult Acute Fulminant Myocarditis. Journal of Clinical Medicine. 2018; 7(11):452. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110452
Chicago/Turabian StyleChong, Shaur-Zheng, Chih-Yuan Fang, Hsiu-Yu Fang, Huang-Chung Chen, Chien-Jen Chen, Cheng-Hsu Yang, Chi-Ling Hang, Hon-Kan Yip, Chiung-Jen Wu, and Wei-Chieh Lee. 2018. "Associations with the In-Hospital Survival Following Extracorporeal Membrane Oxygenation in Adult Acute Fulminant Myocarditis" Journal of Clinical Medicine 7, no. 11: 452. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm7110452