A Pilot Study of Vaccine Therapy with Multiple Glioma Oncoantigen/Glioma Angiogenesis-Associated Antigen Peptides for Patients with Recurrent/Progressive High-Grade Glioma


Abstract
:1. Introduction
2. Materials and Methods
2.1. Vaccine Therapy Design
2.2. Patient Eligibility
2.3. Peptides
2.4. Vaccine Preparation and Treatment Protocol
2.5. Radiologic Response Monitoring and Other Clinical Endpoints
2.6. Toxicity Assessment
2.7. CTL Responses to Peptide Stimulation
2.8. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
3.2. Toxicity
3.3. CTL Response
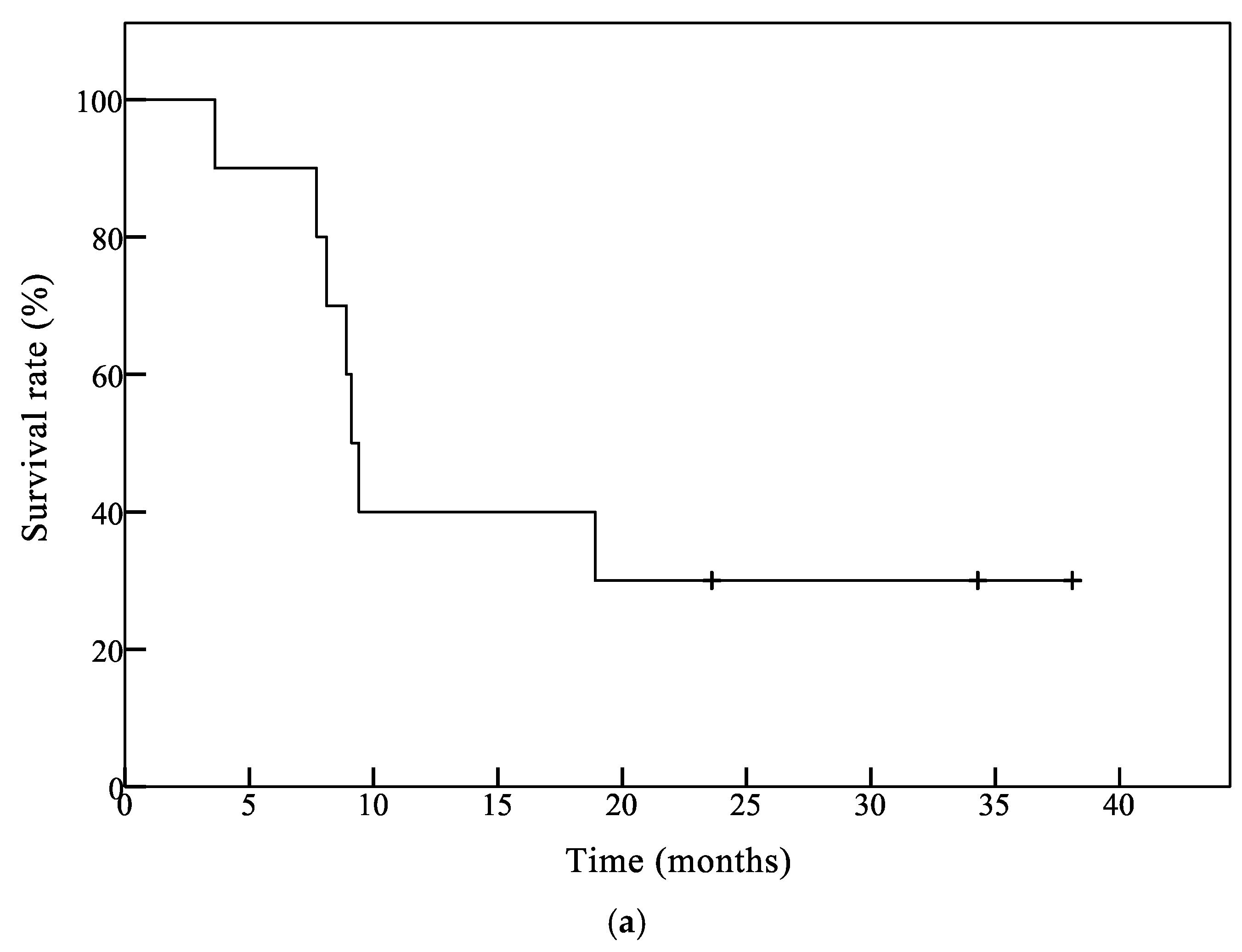
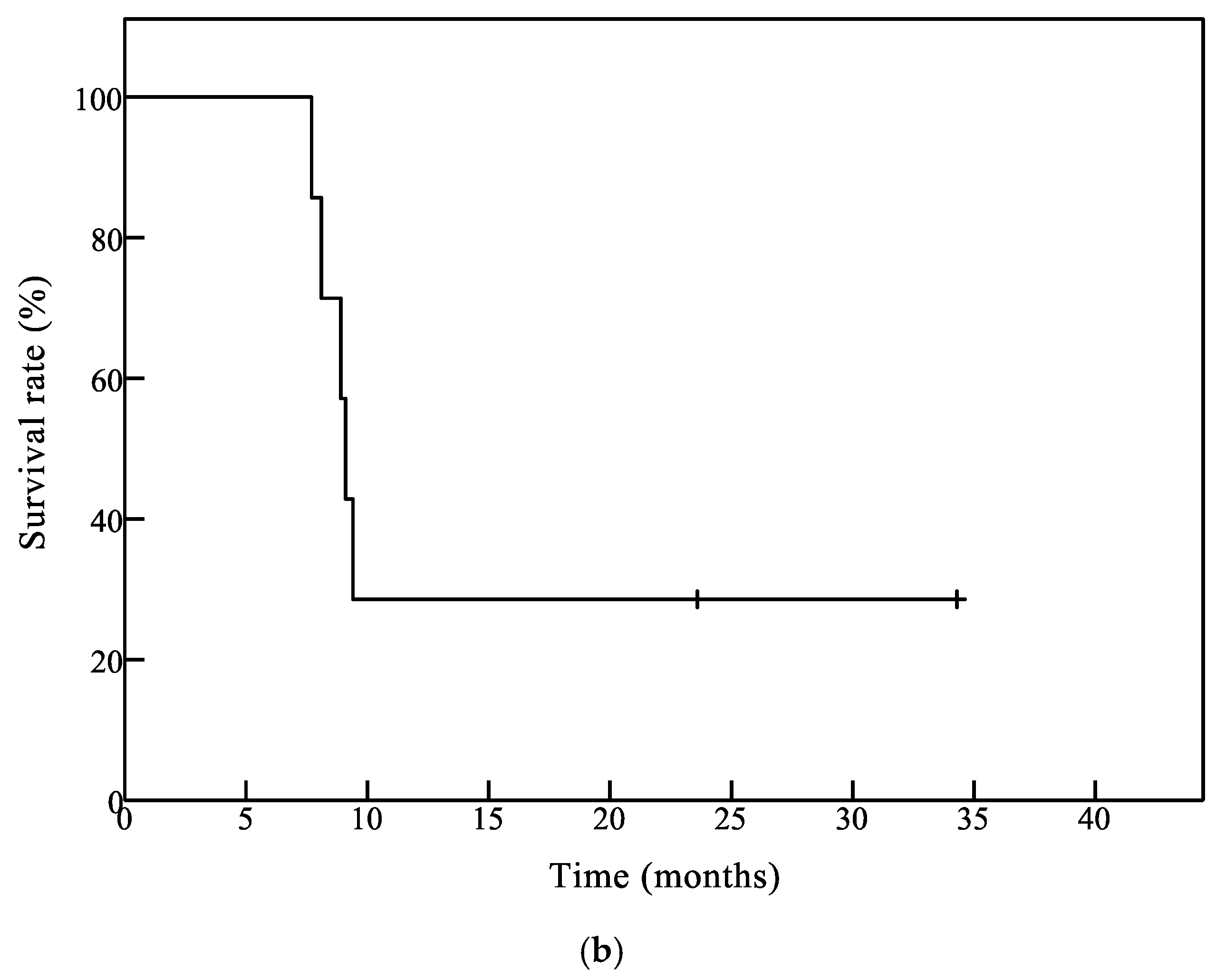
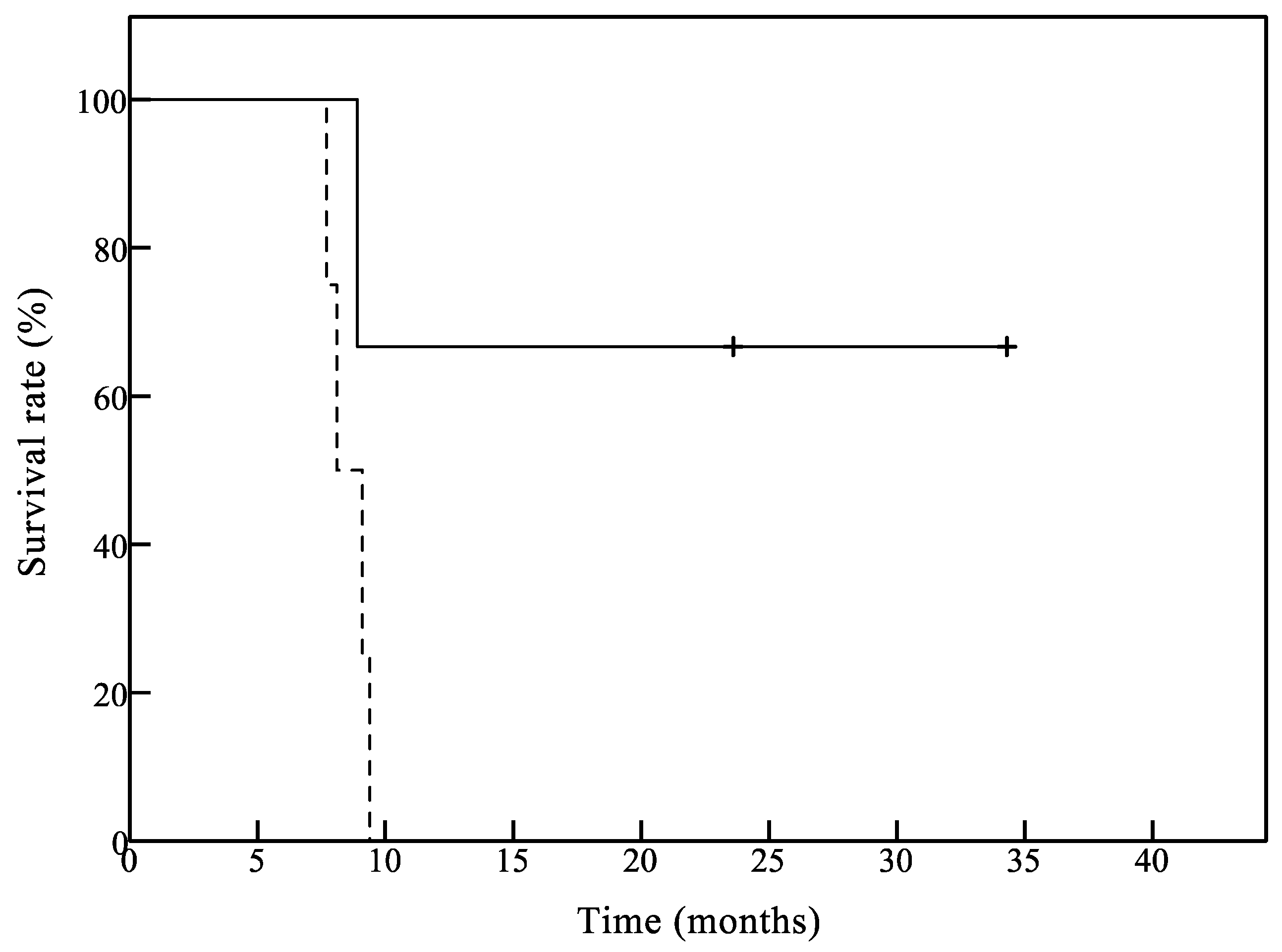
3.4. Clinical Outcomes
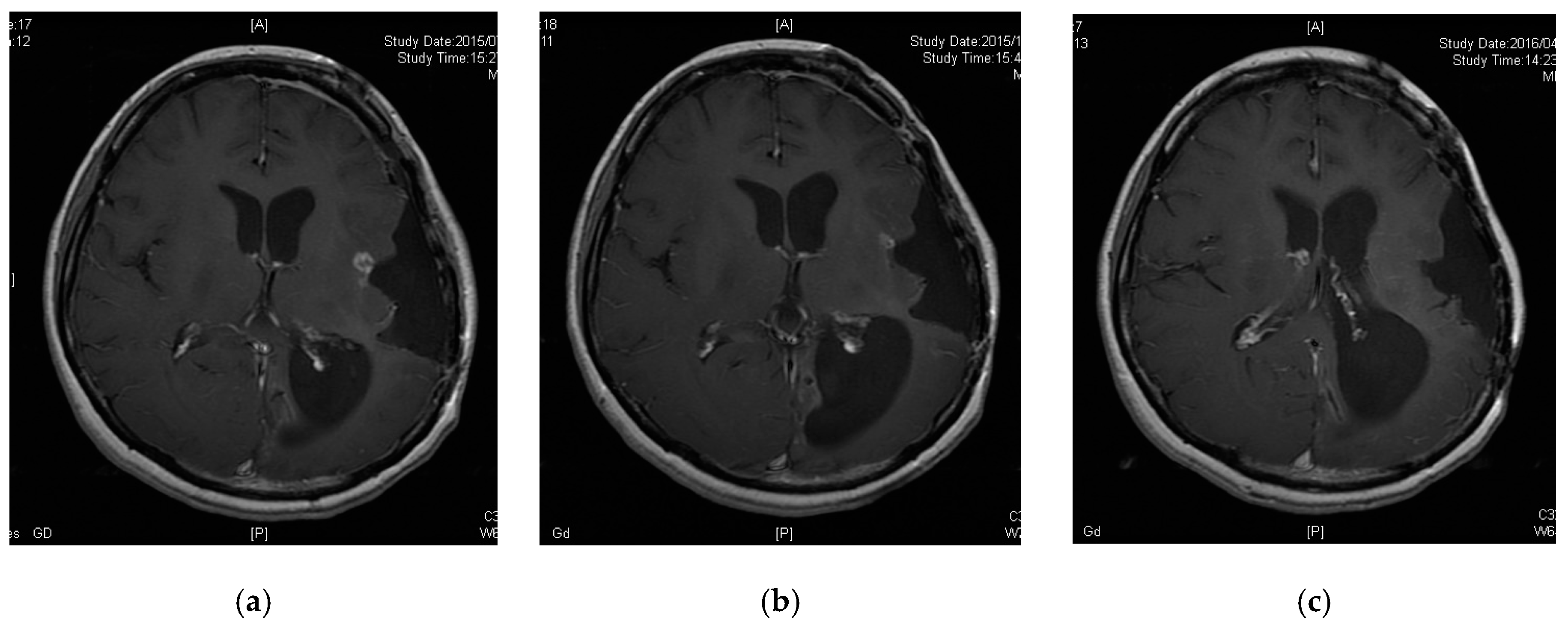
3.5. A Case of CR following Peptide Vaccination
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Chinot, O.L.; Wick, W.; Mason, W.; Henriksson, R.; Saran, F.; Nishikawa, R.; Carpentier, A.F.; Hoang-Xuan, K.; Kavan, P.; Cernea, D.; et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.R.; Dignam, J.J.; Armstrong, T.S.; Wefel, J.S.; Blumenthal, D.T.; Vogelbaum, M.A.; Colman, H.; Chakravarti, A.; Pugh, S.L.; Won, M.; et al. A randomized trial of bevacizumab for newly diagnosed glioblastoma. N. Engl. J. Med. 2014, 370, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbalý, V.; et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur. J. Cancer 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampson, J.H.; Heimberger, A.B.; Archer, G.E.; Aldape, K.D.; Friedman, A.H.; Friedman, H.S.; Gilbert, M.R.; Herndon, J.E.; McLendon, R.E.; Mitchell, D.A.; et al. Immunologic escape after prolonged progression-free survival with epidermal growth factor receptor variant III peptide vaccination in patients with newly diagnosed glioblastoma. J. Clin. Oncol. 2010, 28, 4722–4729. [Google Scholar] [CrossRef] [PubMed]
- Pollack, I.F.; Jakacki, R.I.; Butterfield, L.H.; Hamilton, R.L.; Panigrahy, A.; Potter, D.M.; Connelly, A.K.; Dibridge, S.A.; Whiteside, T.L.; Okada, H. Antigen-specific immune responses and clinical outcome after vaccination with glioma-associated antigen peptides and polyinosinic-polycytidylic acid stabilized by lysine and carboxymethylcellulose in children with newly diagnosed malignant brainstem and nonbrainstem gliomas. J. Clin. Oncol. 2014, 32, 2050–2058. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Butterfield, L.H.; Hamilton, R.L.; Hoji, A.; Sakaki, M.; Ahn, B.J.; Kohanbash, G.; Drappatz, J.; Engh, J.; Amankulor, N.; et al. Induction of robust type-I CD8+ T-cell responses in WHO grade 2 low-grade glioma patients receiving peptide-based vaccines in combination with poly-ICLC. Clin. Cancer Res. 2015, 21, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Rampling, R.; Peoples, S.; Mulholland, P.J.; James, A.; Al-Salihi, O.; Twelves, C.J.; McBain, C.; Jefferies, S.; Jackson, A.; Stewart, W.; et al. A Cancer Research UK First Time in Human Phase I Trial of IMA950 (Novel Multipeptide Therapeutic Vaccine) in Patients with Newly Diagnosed Glioblastoma. Clin. Cancer Res. 2016, 22, 4776–4785. [Google Scholar] [CrossRef]
- Terasaki, M.; Shibui, S.; Narita, Y.; Fujimaki, T.; Aoki, T.; Kajiwara, K.; Sawamura, Y.; Kurisu, K.; Mineta, T.; Yamada, A.; et al. Phase I trial of a personalized peptide vaccine for patients positive for human leukocyte antigen--A24 with recurrent or progressive glioblastoma multiforme. J. Clin. Oncol. 2011, 29, 337–344. [Google Scholar] [CrossRef]
- Izumoto, S.; Tsuboi, A.; Oka, Y.; Suzuki, T.; Hashiba, T.; Kagawa, N.; Hashimoto, N.; Maruno, M.; Elisseeva, O.A.; Shirakata, T.; et al. Phase II clinical trial of Wilms tumor 1 peptide vaccination for patients with recurrent glioblastoma multiforme. J. Neurosurg. 2008, 108, 963–971. [Google Scholar] [CrossRef]
- Shibao, S.; Ueda, R.; Saito, K.; Kikuchi, R.; Nagashima, H.; Kojima, A.; Kagami, H.; Pareira, E.S.; Sasaki, H.; Noji, S.; et al. A pilot study of peptide vaccines for VEGF receptor 1 and 2 in patients with recurrent/progressive high grade glioma. Oncotarget 2018, 9, 21569–21579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenberg, S.A.; Yang, J.C.; Restifo, N.P. Cancer immunotherapy: moving beyond current vaccines. Nat. Med. 2004, 10, 909–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryschich, E.; Nötzel, T.; Hinz, U.; Autschbach, F.; Ferguson, J.; Simon, I.; Weitz, J.; Fröhlich, B.; Klar, E.; Büchler, M.W.; et al. Control of T-cell-mediated immune response by HLA class I in human pancreatic carcinoma. Clin. Cancer Res. 2005, 11, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Khong, H.T.; Restifo, N.P. Natural selection of tumor variants in the generation of “tumor escape” phenotypes. Nat. Immunol. 2002, 3, 999–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, H.; Imano, M.; Shiraishi, O.; Yasuda, A. Phase I clinical trial of vaccination with LY6K-derived peptide in patients with advanced gastric cancer. Gastric Cancer 2013. [Google Scholar] [CrossRef] [PubMed]
- Obara, W.; Ohsawa, R.; Kanehira, M.; Takata, R.; Tsunoda, T.; Yoshida, K.; Takeda, K.; Katagiri, T.; Nakamura, Y.; Fujioka, T. Cancer peptide vaccine therapy developed from oncoantigens identified through genome-wide expression profile analysis for bladder cancer. Jpn. J. Clin. Oncol. 2012, 42, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, M.; Katsuda, M.; Nakamori, M.; Nakamura, M.; Naka, T.; Ojima, T.; Iida, T.; Yamaue, H. Vaccination with peptides derived from cancer-testis antigens in combination with CpG-7909 elicits strong specific CD8+ T cell response in patients with metastatic esophageal squamous cell carcinoma. Cancer Sci. 2010, 101, 2510–2517. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Fukuhara, M.; Yamaura, T.; Mutoh, S.; Okabe, N.; Yaginuma, H.; Hasegawa, T.; Yonechi, A.; Osugi, J.; Hoshino, M.; et al. Multiple therapeutic peptide vaccines consisting of combined novel cancer testis antigens and anti-angiogenic peptides for patients with non-small cell lung cancer. J. Transl. Med. 2013, 11, 97. [Google Scholar] [CrossRef] [Green Version]
- Kono, K.; Iinuma, H.; Akutsu, Y.; Tanaka, H.; Hayashi, N.; Uchikado, Y.; Noguchi, T.; Fujii, H.; Okinaka, K.; Fukushima, R.; et al. Multicenter, phase II clinical trial of cancer vaccination for advanced esophageal cancer with three peptides derived from novel cancer-testis antigens. J. Transl. Med. 2012, 10, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, K.; Sugiura, F.; Kogita, A.; Yoshioka, Y.; Sukegawa, Y.; Hida, J.; Okuno, K. Clinical trial of a seven-peptide vaccine and tegafur-uracil/leucovorin as combination therapy for advanced colorectal cancer. Gan Kagaku Ryoho 2014, 41, 1276–1279. [Google Scholar]
- Yoshitake, Y.; Fukuma, D.; Yuno, A.; Hirayama, M.; Nakayama, H.; Tanaka, T.; Nagata, M.; Takamune, Y.; Kawahara, K.; Nakagawa, Y.; et al. Phase II clinical trial of multiple peptide vaccination for advanced head and neck cancer patients revealed induction of immune responses and improved OS. Clin. Cancer Res. 2015, 21, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Lollini, P.; Cavallo, F.; Nanni, P.; Forni, G. Vaccines for tumour prevention. Nat. Rev. Cancer 2006, 6, 204–216. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wei, P.; Gong, A.; Chiu, W.; Lee, H.; Colman, H.; Huang, H.; Xue, J.; Liu, M.; Wang, Y.; et al. FoxM1 promotes β-catenin nuclear localization and controls Wnt target-gene expression and glioma tumorigenesis. Cancer Cell 2011, 20, 427–442. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, R.; Sampetrean, O.; Saya, H.; Yoshida, K.; Toda, M. Functional analysis of the DEPDC1 oncoantigen in malignant glioma and brain tumor initiating cells. J. Neurooncol. 2017, 133, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Joshi, K.; Banasavadi-Siddegowda, Y.; Mo, X.; Kim, S.H.; Mao, P.; Kig, C.; Nardini, D.; Sobol, R.W.; Chow, L.M.L.; Kornblum, H.I.; et al. MELK-dependent FOXM1 phosphorylation is essential for proliferation of glioma stem cells. Stem Cells 2013, 31, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Ohta, S.; Kawakami, Y.; Yoshida, K.; Toda, M. Functional analysis of KIF20A, a potential immunotherapeutic target for glioma. J. Neurooncol. 2017, 132, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Plate, K.H.; Risau, W. Angiogenesis in malignant gliomas. Glia 1995, 15, 339–347. [Google Scholar] [CrossRef]
- Plate, K.H.; Breier, G.; Weich, H.A.; Mennel, H.D.; Risau, W. Vascular endothelial growth factor and glioma angiogenesis: coordinate induction of VEGF receptors, distribution of VEGF protein and possible in vivo regulatory mechanisms. Int. J. Cancer 1994, 59, 520–529. [Google Scholar] [CrossRef]
- Ishizaki, H.; Tsunoda, T.; Wada, S.; Yamauchi, M.; Shibuya, M.; Tahara, H. Inhibition of tumor growth with antiangiogenic cancer vaccine using epitope peptides derived from human vascular endothelial growth factor receptor 1. Clin. Cancer Res. 2006, 12, 5841–5849. [Google Scholar] [CrossRef]
- Wada, S.; Tsunoda, T.; Baba, T.; Primus, F.J.; Kuwano, H.; Shibuya, M.; Tahara, H. Rationale for antiangiogenic cancer therapy with vaccination using epitope peptides derived from human vascular endothelial growth factor receptor 2. Cancer Res. 2005, 65, 4939–4946. [Google Scholar] [CrossRef]
- Suda, T.; Tsunoda, T.; Daigo, Y.; Nakamura, Y.; Tahara, H. Identification of human leukocyte antigen-A24-restricted epitope peptides derived from gene products upregulated in lung and esophageal cancers as novel targets for immunotherapy. Cancer Sci. 2007, 98, 1803–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osawa, R.; Tsunoda, T.; Yoshimura, S.; Watanabe, T.; Miyazawa, M.; Tani, M.; Takeda, K.; Nakagawa, H.; Nakamura, Y.; Yamaue, H. Identification of HLA-A24-restricted novel T cell epitope peptides derived from P-cadherin and kinesin family member 20A. J. Biomed. Biotechnol. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Yokomine, K.; Senju, S.; Nakatsura, T.; Irie, A.; Hayashida, Y.; Ikuta, Y.; Harao, M.; Imai, K.; Baba, H.; Iwase, H.; et al. The forkhead box M1 transcription factor as a candidate of target for anti-cancer immunotherapy. Int. J. Cancer 2010, 126, 2153–2163. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Okada, H.; Weller, M.; Huang, R.; Finocchiaro, G.; Gilbert, M.R.; Wick, W.; Ellingson, B.M.; Hashimoto, N.; Pollack, I.F.; Brandes, A.A.; et al. Immunotherapy response assessment in neuro-oncology: A report of the RANO working group. Lancet Oncol. 2015, 16, e534–e542. [Google Scholar] [CrossRef]
- Wick, A.; Felsberg, J.; Steinbach, J.P.; Herrlinger, U.; Platten, M.; Blaschke, B.; Meyermann, R.; Reifenberger, G.; Weller, M.; Wick, W. Efficacy and tolerability of temozolomide in an alternating weekly regimen in patients with recurrent glioma. J. Clin. Oncol. 2007, 25, 3357–3361. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.R.; Bélanger, K.; Mason, W.P.; Fulton, D.; Kavan, P.; Easaw, J.; Shields, C.; Kirby, S.; Macdonald, D.R.; Eisenstat, D.D.; et al. Phase II trial of continuous dose-intense temozolomide in recurrent malignant glioma: RESCUE study. J. Clin. Oncol. 2010, 28, 2051–2057. [Google Scholar] [CrossRef]
- Franceschi, E.; Cavallo, G.; Scopece, L.; Paioli, A.; Pession, A.; Magrini, E.; Conforti, R.; Palmerini, E.; Bartolini, S.; Rimondini, S.; et al. Phase II trial of carboplatin and etoposide for patients with recurrent high-grade glioma. Br. J. Cancer 2004, 91, 1038–1044. [Google Scholar] [CrossRef] [Green Version]
- Nagane, M.; Nishikawa, R.; Narita, Y.; Kobayashi, H.; Takano, S.; Shinoura, N.; Aoki, T.; Sugiyama, K.; Kuratsu, J.; Muragaki, Y.; et al. Phase II study of single-agent bevacizumab in Japanese patients with recurrent malignant glioma. Jpn. J. Clin. Oncol. 2012, 42, 887–895. [Google Scholar] [CrossRef]
- Terme, M.; Pernot, S.; Marcheteau, E.; Sandoval, F.; Benhamouda, N.; Colussi, O.; Dubreuil, O.; Carpentier, A.F.; Tartour, E.; Taieb, J. VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res. 2013, 73, 539–549. [Google Scholar] [CrossRef]
- Adotevi, O.; Pere, H.; Ravel, P.; Haicheur, N.; Badoual, C.; Merillon, N.; Medioni, J.; Peyrard, S.; Roncelin, S.; Verkarre, V.; et al. A decrease of regulatory T cells correlates with overall survival after sunitinib-based antiangiogenic therapy in metastatic renal cancer patients. J. Immunother. 2010, 33, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Du Four, S.; Maenhout, S.K.; Benteyn, D.; De Keersmaecker, B.; Duerinck, J.; Thielemans, K.; Neyns, B.; Aerts, J.L. Disease progression in recurrent glioblastoma patients treated with the VEGFR inhibitor axitinib is associated with increased regulatory T cell numbers and T cell exhaustion. Cancer Immunol. Immunother. 2016, 65, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Sturm, D.; Pfister, S.M.; Jones, D.T.W. Pediatric Gliomas: Current Concepts on Diagnosis, Biology, and Clinical Management. J. Clin. Oncol. 2017, 35, 2370–2377. [Google Scholar] [CrossRef] [PubMed]
- Paugh, B.S.; Qu, C.; Jones, C.; Liu, Z.; Adamowicz-Brice, M.; Zhang, J.; Bax, D.A.; Coyle, B.; Barrow, J.; Hargrave, D.; et al. Integrated molecular genetic profiling of pediatric high-grade gliomas reveals key differences with the adult disease. J. Clin. Oncol. 2010, 18, 3061–3068. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Age (Years) | Sex | Diagnosis | Tumor Size (mm) | Operation | Radiotherapy | Chemotherapy | IDH1 Mutation | 1p/19q Codeletion | MGMT Methylation |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 17 | M | GB | 32.5 × 29.5 × 32.5 | 2 | 60 Gy | TMZ, ICE | WT | (−) | (−) |
| 2 | 38 | M | HGG | 20.6 × 11.7 × 16.6 | 0 | 60 Gy + SRT30 Gy | TMZ | NT | NT | NT |
| 3 | 38 | M | GB with oligo | No enhanced lesion * | 2 | 60 Gy | TMZ | WT | NT | (−) |
| 4 | 66 | F | GB | 18.0 × 11.5 × 20.0 | 1 | 60 Gy | TMZ, BEV | NT | NT | NT |
| 5 | 46 | F | sGB | 48.0 × 25.0 × 48.8 | 5 | GK, 60 Gy | TMZ, IFNb, BEV | NT | NT | NT |
| 6 | 33 | F | AOA | 12.0 × 8.5 × 18.0 | 4 | 60 Gy | TMZ | R132H | (−) | (−) |
| 7 | 72 | M | OA rec | 33.0 × 20.5 × 23.7 | 1 | 60 Gy | TMZ, BEV | WT | (−) | (±) |
| 8 | 36 | F | sGB | 16.0 × 13.0 × 18.6 | 2 | 60 Gy | TMZ, BEV | R132H | (−) | (−) |
| 9 | 27 | F | sGB | 30.2 × 24.1 × 28.6 | 1 | SRT | TMZ, BEV | R132H | (−) | (+) |
| 10 | 67 | F | GB | 23.3 × 12.1 × 17.5 | 2 | 60 Gy | TMZ | WT | (−) | (±) |
| Case No. | Vaccination | LY6K | FOXM1 | DEPDC1 | KIF20A | VEGFR1 | VEGFR2 | Positive Control |
|---|---|---|---|---|---|---|---|---|
| 1 | before | − | + | + | + | + | − | +++ |
| 2 weeks after | +++ | +++ | +++ | + | + | − | +++ | |
| 2 | before | − | − | + | + | − | − | +++ |
| 2 weeks after | +++ | +++ | +++ | + | − | − | +++ | |
| 3 | before | − | − | NT | NT | − | NT | +++ |
| 2 weeks after | + | +++ | + | − | + | NT | +++ | |
| 4 | before | − | + | + | − | − | + | +++ |
| 2 weeks after | +++ | +++ | +++ | + | − | + | +++ | |
| 5 | before | − | + | − | − | − | − | +++ |
| 2 weeks after | +++ | +++ | +++ | + | + | +++ | +++ | |
| 6 | before | − | + | − | − | − | − | +++ |
| 2 weeks after | +++ | +++ | +++ | + | + | +++ | +++ |
| Case No. | Frequency of Vaccination | Period of Vaccination (mo) | Evaluation after 3 Months | Evaluation after 6 Months | PFS (mo) | OS (mo) |
|---|---|---|---|---|---|---|
| 1 | 18 | 6.2 | PD | PD | 6.3 | 8.9 |
| 2 | 11 | 6.7 | PD | PD | 6.8 | 18.9 |
| 3 | 26 | 21.0 | SD | SD | 18.2 | 34.3 |
| 4 | 12 | 4.8 | PD | PD | 4.9 | 9.1 |
| 5 | 8 | 1.6 | PD | PD | 1.7 | 8.1 |
| 6 | 20 | 37.5 | PR | PR * | 38.1 | 38.1 |
| 7 | 8 | 1.6 | PD | Dead | 1.9 | 3.6 |
| 8 | 11 | 4.6 | SD | PD | 4.7 | 7.7 |
| 9 | 10 | 2.1 | PD | PD | 2.9 | 9.4 |
| 10 | 18 | 10.8 | SD | SD | 11.0 | 23.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kikuchi, R.; Ueda, R.; Saito, K.; Shibao, S.; Nagashima, H.; Tamura, R.; Morimoto, Y.; Sasaki, H.; Noji, S.; Kawakami, Y.; et al. A Pilot Study of Vaccine Therapy with Multiple Glioma Oncoantigen/Glioma Angiogenesis-Associated Antigen Peptides for Patients with Recurrent/Progressive High-Grade Glioma. J. Clin. Med. 2019, 8, 263. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020263
Kikuchi R, Ueda R, Saito K, Shibao S, Nagashima H, Tamura R, Morimoto Y, Sasaki H, Noji S, Kawakami Y, et al. A Pilot Study of Vaccine Therapy with Multiple Glioma Oncoantigen/Glioma Angiogenesis-Associated Antigen Peptides for Patients with Recurrent/Progressive High-Grade Glioma. Journal of Clinical Medicine. 2019; 8(2):263. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020263
Chicago/Turabian StyleKikuchi, Ryogo, Ryo Ueda, Katsuya Saito, Shunsuke Shibao, Hideaki Nagashima, Ryota Tamura, Yukina Morimoto, Hikaru Sasaki, Shinobu Noji, Yutaka Kawakami, and et al. 2019. "A Pilot Study of Vaccine Therapy with Multiple Glioma Oncoantigen/Glioma Angiogenesis-Associated Antigen Peptides for Patients with Recurrent/Progressive High-Grade Glioma" Journal of Clinical Medicine 8, no. 2: 263. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020263