Hormonal Contraceptives, Female Sexual Dysfunction, and Managing Strategies: A Review


Abstract
:1. Introduction
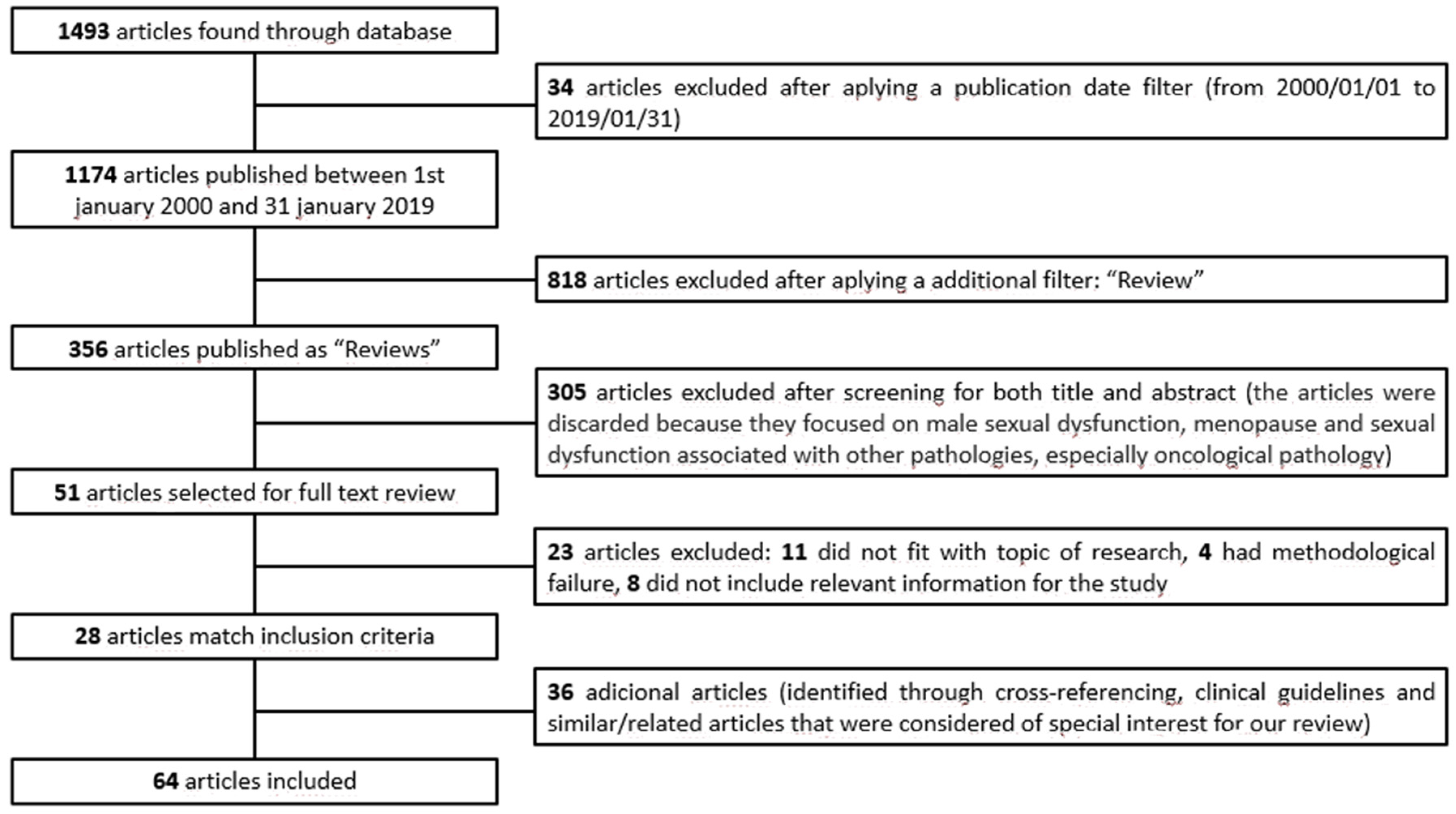
2. Materials and Methods
3. Results
3.1. Hormonal Contraceptives
3.1.1. Types
3.1.2. Hormones
3.1.3. Mechanism of Action of Hormonal Contraceptives
3.1.4. Hormonal Alterations of Hormonal Contraceptives and Their Influence on Female Sexual Function
3.2. Sexual Dysfunction
3.3. The Effects of Hormonal Contraceptives on Sexuality
3.3.1. Hormonal Contraceptives Do Not Have Sexual Effects
3.3.2. Hormonal Contraceptives Have Sexual Effects
Positive Effects
Negative Effects
3.3.3. Effects on Sexual Function According to the Type of Hormonal Contraceptive
Contraceptive Patch
Contraceptive Ring
Depot Medroxyprogesterone Acetate (DMPA)
Etonogestrel Implant
Levonorgestrel-Releasing Intrauterine Systems (LNG-IUS)
3.3.4. Other Non-Hormonal Methods of Contraception and Their Effect on Sexual Function
Copper Intrauterine Devices (Cu-IUDs)
Vasectomy/Tubal Ligation
Nonuse of Contraception
3.3.5. The Sexual Side Effects of Hormonal Contraceptives are not Well Studied
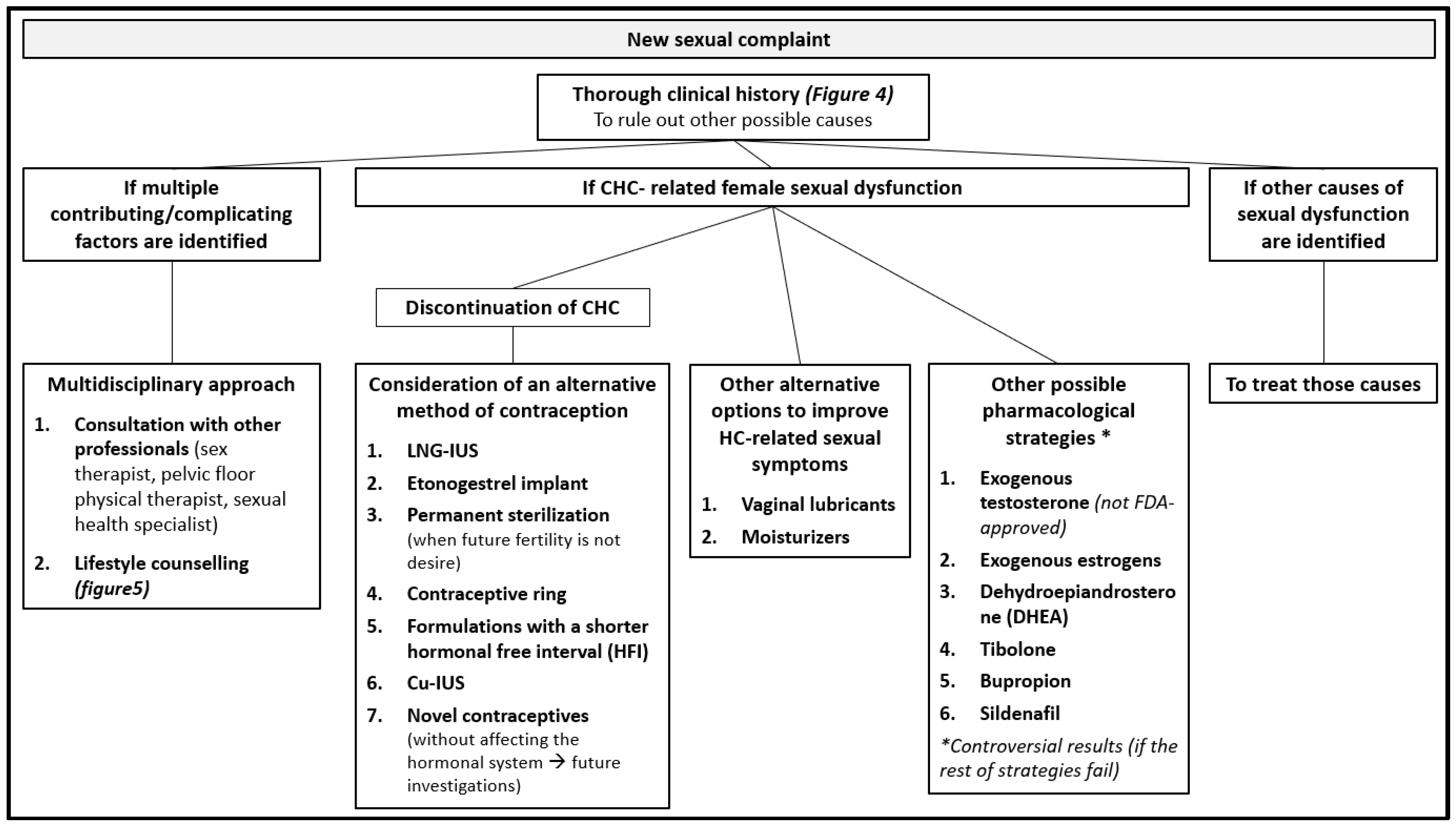
3.4. Management Strategies for Sexual Dysfunction Secondary to Hormonal Contraceptives
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Burrows, L.J.; Basha, M.; Goldstein, A.T. The Effects of Hormonal Contraceptives on Female Sexuality: A Review. J. Sex. Med. 2012, 9, 2213–2223. [Google Scholar] [CrossRef] [PubMed]
- Casey, P.M.; MacLaughlin, K.L.; Faubion, S.S. Impact of Contraception on Female Sexual Function. J. Women’s Heal. 2017, 26, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Champaneria, R.; D’Andrea, R.M.; Latthe, P.M. Hormonal contraception and pelvic floor function: a systematic review. Int. Urogynecol. J. 2016, 27, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Egarter, C.; Frey Tirri, B.; Bitzer, J.; Kaminskyy, V.; Oddens, B.J.; Prilepskaya, V.; Yeshaya, A.; Marintcheva-Petrova, M.; Weyers, S. Women’s perceptions and reasons for choosing the pill, patch, or ring in the CHOICE study: A cross-sectional survey of contraceptive method selection after counseling. BMC Womens. Health 2013, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Baird, D.T.; Castelo-Branco, C.; Collins, J.; Evers, J.L.H.; Glasier, A.; La Vecchia, C.; Leridon, H.; Mishell, D.R.; Wellings, K.; Arisi, E.; et al. Female contraception over 40. Hum. Reprod. Update 2009, 15, 599–612. [Google Scholar] [Green Version]
- Boozalis, A.; Tutlam, N.T.; Chrisman Robbins, C.; Peipert, J.F. Sexual Desire and Hormonal Contraception. Obstet. Gynecol. 2016, 127, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Skouby, S.O. Contraceptive use and behavior in the 21st century: a comprehensive study across five European countries. Eur. J. Contracept. Reprod. Heal. Care 2010, 15, S42–S53. [Google Scholar] [CrossRef] [PubMed]
- Oliveira Da Silva, M.; Albrecht, J.; Olsen, J.; Karro, H.; Temmerman, M.; Gissler, M.; Bloemenkamp, K.; Hannaford, P.; Fronteira, I. The Reproductive Health Report: The state of sexual and reproductive health within the European Union. Eur. J. Contracept. Reprod. Heal. Care 2011, 16, S1–S70. [Google Scholar]
- Hall, K.S.; Trussell, J. Types of combined oral contraceptives used by US women. Contraception 2012, 86, 659–665. [Google Scholar] [CrossRef] [Green Version]
- Black, A.; Guilbert, E.; Costescu, D.; Dunn, S.; Fisher, W.; Kives, S.; Mirosh, M.; Norman, W.V.; Pymar, H.; Reid, R.; et al. No. 329-Canadian Contraception Consensus Part 4 of 4 Chapter 9: Combined Hormonal Contraception. J. Obstet. Gynaecol. Canada 2017, 39, 229–268. [Google Scholar] [CrossRef]
- Imprialos, K.P.; Stavropoulos, K.; Doumas, M.; Tziomalos, K.; Karagiannis, A.; Athyros, V.G. Sexual Dysfunction, Cardiovascular Risk and Effects of Pharmacotherapy. Curr. Vasc. Pharmacol. 2018, 16, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Montejo, A.L.; Montejo, L.; Navarro-Cremades, F. Sexual side-effects of antidepressant and antipsychotic drugs. Curr. Opin. Psychiatry 2015, 28, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Montejo, A.L.; Montejo, L.; Baldwin, D.S. The impact of severe mental disorders and psychotropic medications on sexual health and its implications for clinical management. World Psychiatry 2018, 17, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montejo, A.L.; Majadas, S.; Rico-Villademoros, F.; Llorca, G.; De La Gándara, J.; Franco, M.; Martín-Carrasco, M.; Aguera, L.; Prieto, N.; Spanish Working Group for the Study of Psychotropic-Related Sexual Dysfunction. Frequency of sexual dysfunction in patients with a psychotic disorder receiving antipsychotics. J. Sex. Med. 2010, 7, 3404–3413. [Google Scholar] [CrossRef] [PubMed]
- Montejo, A.L.; Calama, J.; Rico-Villademoros, F.; Montejo, L.; González-García, N.; Pérez, J. A Real-World Study on Antidepressant-Associated Sexual Dysfunction in 2144 Outpatients: The SALSEX I Study. Arch. Sex. Behav. 2019, 48, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Bellastella, G.; Castaldo, F.; Petrizzo, M.; Giugliano, D.; Esposito, K. Sexual function in young women with type 1 diabetes: the METRO study. J. Endocrinol. Invest. 2017, 40, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Giugliano, D. Obesity, the metabolic syndrome, and sexual dysfunction. Int. J. Impot. Res. 2005, 17, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.N.; Thurston, R.C. A biopsychosocial approach to women’s sexual function and dysfunction at midlife: A narrative review. Maturitas 2016, 87, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Hughes, H. Management of postpartum loss of libido. J. Fam. Health Care 2008, 18, 123–135. [Google Scholar] [PubMed]
- FDA Office of Women’s Health Birth Control Guide. Available online: https://www.fda.gov/media/99605/download (accessed on 5 January 2019).
- Black, A.; Guilbert, E.; Costescu, D.; Dunn, S.; Fisher, W.; Kives, S.; Mirosh, M.; Norman, W.; Pymar, H.; Reid, R.; et al. Canadian Contraception Consensus (Part 3 of 4): Chapter 8-Progestin-Only Contraception. J. Obstet. Gynaecol. Canada 2016, 38, 279–300. [Google Scholar] [CrossRef]
- Black, A.; Guilbert, E.; Costescu, D.; Dunn, S.; Fisher, W.; Kives, S.; Mirosh, M.; Norman, W.; Pymar, H.; Reid, R.; et al. Canadian Contraception Consensus (Part 3 of 4): Chapter 7-Intrauterine Contraception. J. Obstet. Gynaecol. Canada 2016, 38, 182–222. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Recomendaciones sobre prácticas seleccionadas para el uso de anticonceptivos; World Health Organization: Geneva, Switzerland, 2018; ISBN 978-92-4-356540-8. [Google Scholar]
- Sánchez Borrego, R.; Martínez Pérez, Ó. Guía práctica de anticoncepción oral basada en la evidencia; Emisa: Madrid, Spain, 2003; ISBN 84-86917-66-2. [Google Scholar]
- Roney, J.R.; Simmons, Z.L. Hormonal predictors of sexual motivation in natural menstrual cycles. Horm. Behav. 2013, 63, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Grøntvedt, T.V.; Grebe, N.M.; Kennair, L.E.O.; Gangestad, S.W. Estrogenic and progestogenic effects of hormonal contraceptives in relation to sexual behavior: insights into extended sexuality. Evol. Hum. Behav. 2017, 38, 283–292. [Google Scholar] [CrossRef]
- Grebe, N.M.; Gangestad, S.W.; Garver-Apgar, C.E.; Thornhill, R. Women’s luteal-phase sexual proceptivity and the functions of extended sexuality. Psychol. Sci. 2013, 24, 2106–2110. [Google Scholar] [CrossRef] [PubMed]
- Raudrant, D.; Rabe, T. Progestogens with antiandrogenic properties. Drugs 2003, 63, 463–492. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, A.; Kapamadzija, A.; Maticki-Sekulic, M. Hormones and female sexuality. Med. Pregl. 2003, 56, 446–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitruk-Ware, R. New progestagens for contraceptive use. Hum. Reprod. Update 2006, 12, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Espitia De La Hoz, F.J. O-08 Alteration of the Sexual Response Cycle in Women Using Combined Oral Contraceptives. J. Sex. Med. 2017, 14, e374. [Google Scholar] [CrossRef]
- Bahamondes, L.; Bahamondes, M.V. New and emerging contraceptives: a state-of-the-art review. Int. J. Womens. Health 2014, 6, 221. [Google Scholar] [CrossRef]
- Dennerstein, L.; Randolph, J.; Taffe, J.; Dudley, E.; Burger, H. Hormones, mood, sexuality, and the menopausal transition. Fertil. Steril. 2002, 77, 42–48. [Google Scholar] [CrossRef]
- Benedetto, C.; Cagnacci, A.; De Seta, F.; Genazzani, A.R.; Guida, M.; Michieli, R.; Moscarini, M.; Primiero, F.; Russo, N. Counseling on vaginal delivery of contraceptive hormones: Implications for women’s body knowledge and sexual health. Gynecol. Endocrinol. 2013, 29, 1015–1021. [Google Scholar]
- Scheele, D.; Plota, J.; Stoffel-Wagner, B.; Maier, W.; Hurlemann, R. Hormonal contraceptives suppress oxytocin-induced brain reward responses to the partner’s face. Soc. Cogn. Affect. Neurosci. 2016, 11, 767–774. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association, Ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9780890425558. [Google Scholar]
- World Health Organization. Defining Sexual Health: Report of a Technical Consultation on Sexual Health; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Mercer, C.H.; Fenton, K.A.; Johnson, A.M.; Wellings, K.; Macdowall, W.; McManus, S.; Nanchahal, K.; Erens, B. Sexual function problems and help seeking behaviour in Britain: national probability sample survey. BMJ 2003, 327, 426–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobecki, J.N.; Curlin, F.A.; Rasinski, K.A.; Lindau, S.T. What we don’t talk about when we don’t talk about sex: results of a national survey of U.S. obstetrician/gynecologists. J. Sex. Med. 2012, 9, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Sand, M.; Fisher, W.A. Women’s Endorsement of Models of Female Sexual Response: The Nurses’ Sexuality Study. J. Sex. Med. 2007, 4, 708–719. [Google Scholar] [CrossRef] [PubMed]
- Wiegel, M.; Meston, C.; Rosen, R. The female sexual function index (FSFI): cross-validation and development of clinical cutoff scores. J. Sex Marital Ther. 2005, 31, 1–20. [Google Scholar] [CrossRef]
- Davis, A.R.; Castaño, P.M. Oral contraceptives and libido in women. Annu. Rev. Sex Res. 2004, 15, 297–320. [Google Scholar]
- Pastor, Z.; Holla, K.; Chmel, R. The influence of combined oral contraceptives on female sexual desire: a systematic review. Eur. J. Contracept. Reprod. Health Care 2013, 18, 27–43. [Google Scholar] [CrossRef]
- Graham, C.A.; Bancroft, J.; Doll, H.A.; Greco, T.; Tanner, A. Does oral contraceptive-induced reduction in free testosterone adversely affect the sexuality or mood of women? Psychoneuroendocrinology 2007, 32, 246–255. [Google Scholar] [CrossRef]
- Strufaldi, R.; Pompei, L.M.; Steiner, M.L.; Cunha, E.P.; Ferreira, J.A.S.; Peixoto, S.; Fernandes, C.E. Effects of two combined hormonal contraceptives with the same composition and different doses on female sexual function and plasma androgen levels. Contraception 2010, 82, 147–154. [Google Scholar] [CrossRef]
- Elaut, E.; Buysse, A.; De Sutter, P.; Gerris, J.; De Cuypere, G.; T’Sjoen, G. Cycle-Related Changes in Mood, Sexual Desire, and Sexual Activity in Oral Contraception-Using and Nonhormonal-Contraception-Using Couples. J. Sex Res. 2016, 53, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Enzlin, P.; Weyers, S.; Janssens, D.; Poppe, W.; Eelen, C.; Pazmany, E.; Elaut, E.; Amy, J. Sexual Functioning in Women Using Levonorgestrel-Releasing Intrauterine Systems as Compared to Copper Intrauterine Devices. J. Sex. Med. 2012, 9, 1065–1073. [Google Scholar] [CrossRef]
- Toorzani, Z.M.; Zahraei, R.H.; Ehsanpour, S.; Nasiri, M.; Shahidi, S.; Soleimani, B. A study on the relationship of sexual satisfaction and common contraceptive methods employed by the couples. Iran. J. Nurs. Midwifery Res. 2010, 15, 115–119. [Google Scholar] [PubMed]
- Reed, B.; Harlow, S.; Legocki, L.; Helmuth, M.; Haefner, H.; Gillespie, B.; Sen, A. Oral contraceptive use and risk of vulvodynia: a population-based longitudinal study. BJOG An Int. J. Obstet. Gynaecol. 2013, 120, 1678–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iliadou, A.; Milsom, I.; Pedersen, N.L.; Altman, D. Risk of urinary incontinence symptoms in oral contraceptive users: a national cohort study from the Swedish Twin Register. Fertil. Steril. 2009, 92, 428–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graziottin, A. The shorter, the better: A review of the evidence for a shorter contraceptive hormone-free interval. Eur. J. Contracept. Reprod. Heal. Care 2016, 21, 93–105. [Google Scholar] [CrossRef]
- Guida, M.; Cibarelli, F.; Troisi, J.; Gallo, A.; Palumbo, A.R.; Di Spiezio Sardo, A. Sexual life impact evaluation of different hormonal contraceptives on the basis of their methods of administration. Arch. Gynecol. Obstet. 2014, 290, 1239–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrzypulec, V.; Drosdzol, A. Evaluation of quality of life and sexual functioning of women using levonorgestrel-releasing intrauterine contraceptive system--Mirena. Coll. Antropol. 2008, 32, 1059–1068. [Google Scholar]
- Smith, N.K.; Jozkowski, K.N.; Sanders, S.A. Hormonal contraception and female pain, orgasm and sexual pleasure. J. Sex. Med. 2014, 11, 462–470. [Google Scholar] [CrossRef]
- Li, D.; Wilcox, A.J.; Dunson, D.B. Benchmark pregnancy rates and the assessment of post-coital contraceptives: an update. Contraception 2015, 91, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Gracia, C.R.; Sammel, M.D.; Charlesworth, S.; Lin, H.; Barnhart, K.T.; Creinin, M.D. Sexual function in first-time contraceptive ring and contraceptive patch users. Fertil. Steril. 2010, 93, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.M.M.; El-Sherbiny, W.S.M.; Mostafa, W.A.I. Combined contraceptive ring versus combined oral contraceptive (30-μg ethinylestradiol and 3-mg drospirenone). Int. J. Gynaecol. Obstet. 2011, 114, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, C.; Morotti, E.; Persico, N.; Battaglia, B.; Busacchi, P.; Casadio, P.; Paradisi, R.; Venturoli, S. Clitoral vascularization and sexual behavior in young patients treated with drospirenone-ethinyl estradiol or contraceptive vaginal ring: a prospective, randomized, pilot study. J. Sex. Med. 2014, 11, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Guida, M.; Di Spiezio Sardo, A.; Bramante, S.; Sparice, S.; Acunzo, G.; Tommaselli, G.A.; Di Carlo, C.; Pellicano, M.; Greco, E.; Nappi, C. Effects of two types of hormonal contraception—oral versus intravaginal—on the sexual life of women and their partners. Hum. Reprod. 2005, 20, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Freeman, S. Nondaily hormonal contraception: considerations in contraceptive choice and patient counseling. J. Am. Acad. Nurse Pract. 2004, 16, 226–238. [Google Scholar] [CrossRef]
- Nappi, R.E. Association of E2v/DNG as contraceptive choice for a better quality of life of women. Minerva Ginecol. 2012, 64, 41–52. [Google Scholar] [PubMed]
- Jozkowski, K.N.; Herbenick, D.; Schick, V.; Reece, M.; Sanders, S.A.; Fortenberry, J.D. Women’s perceptions about lubricant use and vaginal wetness during sexual activities. J. Sex. Med. 2013, 10, 484–492. [Google Scholar] [CrossRef]
- Henzl, M.R.; Loomba, P.K. Transdermal delivery of sex steroids for hormone replacement therapy and contraception. A review of principles and practice. J. Reprod. Med. 2003, 48, 525–540. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Hormonal Contraceptives | Route of Administration | Dosing Frequency | Mechanism of Action | Sexual Effects |
|---|---|---|---|---|
| Levonorgesetrel-realising intrauterine systems (LNG-IUDs) | Intrauterine | Inserted by a healthcare provider. Lasts up to 3–5 years, depending on the type. LARC. |
| Positive effects. However, more studies are needed |
| “The implant”. Etonorgestrel implant. | Subdermal | Inserted by a healthcare provider. Lasts up to 3 years. LARC. |
| Negative effects. However, more studies are needed. |
| Depot Medroxyprogesterone Acetate (DMPA) | Intramuscularly | Every three months. SARC/LARC. |
| Mixed results. More studies are needed. |
| “The Pill”. Combined oral contraceptive | Oral | Must swallow a pill every day. |
| Mixed results. More studies are needed. |
| “The Mini pill”. Progestin-Only Pills (POPs) | Oral | Must swallow a pill at the same time every day. |
| Mixed results. More studies are needed. |
| Contraceptive Patch | Dermal. Is placed on 1 of 4 sites: the buttocks, upper outer arm, lower abdomen, or upper torso, excluding the breast. | Put on a new patch each week for 3 weeks (21 total days). Do not put on a patch during the fourth week. |
| Positive effects. Slight increases in sexual function scores were noted with contraceptive patch, but not clinically significant. |
| Vaginal Contraceptive Ring | Vaginal | Put the ring into the vagina yourself. Keep the ring in you r vagina for 3 weeks |
| Mixed results. More studies are needed. |
| Emergency contraceptives | Route of administration | Dosing frequency | ||
| Levonorgestrel 1.5 mg | Oral | Swallow the pills as soon as possible within 3 days after having unprotected sex. | ||
| Ulipristal Acetate | Oral | Swallow the pills within 5 days after having unprotected sex. | ||
| Most Androgenic | Less Androgenic | The Least Androgenic | Antiandrogenic |
|---|---|---|---|
| Norgestrel levonorgestrel | Norethindrone Norethindrone acetate Ethynodiol diacetate | Desogestrel Etonogestrel Norgestimate | Cyproterona acetato Drospirenona Dienogest |
| Information that should be collected in the medical record by health providers in response to a complaint of sexual dysfunction: |
|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casado-Espada, N.M.; de Alarcón, R.; de la Iglesia-Larrad, J.I.; Bote-Bonaechea, B.; Montejo, Á.L. Hormonal Contraceptives, Female Sexual Dysfunction, and Managing Strategies: A Review. J. Clin. Med. 2019, 8, 908. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060908
Casado-Espada NM, de Alarcón R, de la Iglesia-Larrad JI, Bote-Bonaechea B, Montejo ÁL. Hormonal Contraceptives, Female Sexual Dysfunction, and Managing Strategies: A Review. Journal of Clinical Medicine. 2019; 8(6):908. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060908
Chicago/Turabian StyleCasado-Espada, Nerea M., Rubén de Alarcón, Javier I. de la Iglesia-Larrad, Berta Bote-Bonaechea, and Ángel L. Montejo. 2019. "Hormonal Contraceptives, Female Sexual Dysfunction, and Managing Strategies: A Review" Journal of Clinical Medicine 8, no. 6: 908. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8060908