Exercise-Based Interventions in Hemodialysis Patients: A Systematic Review with a Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
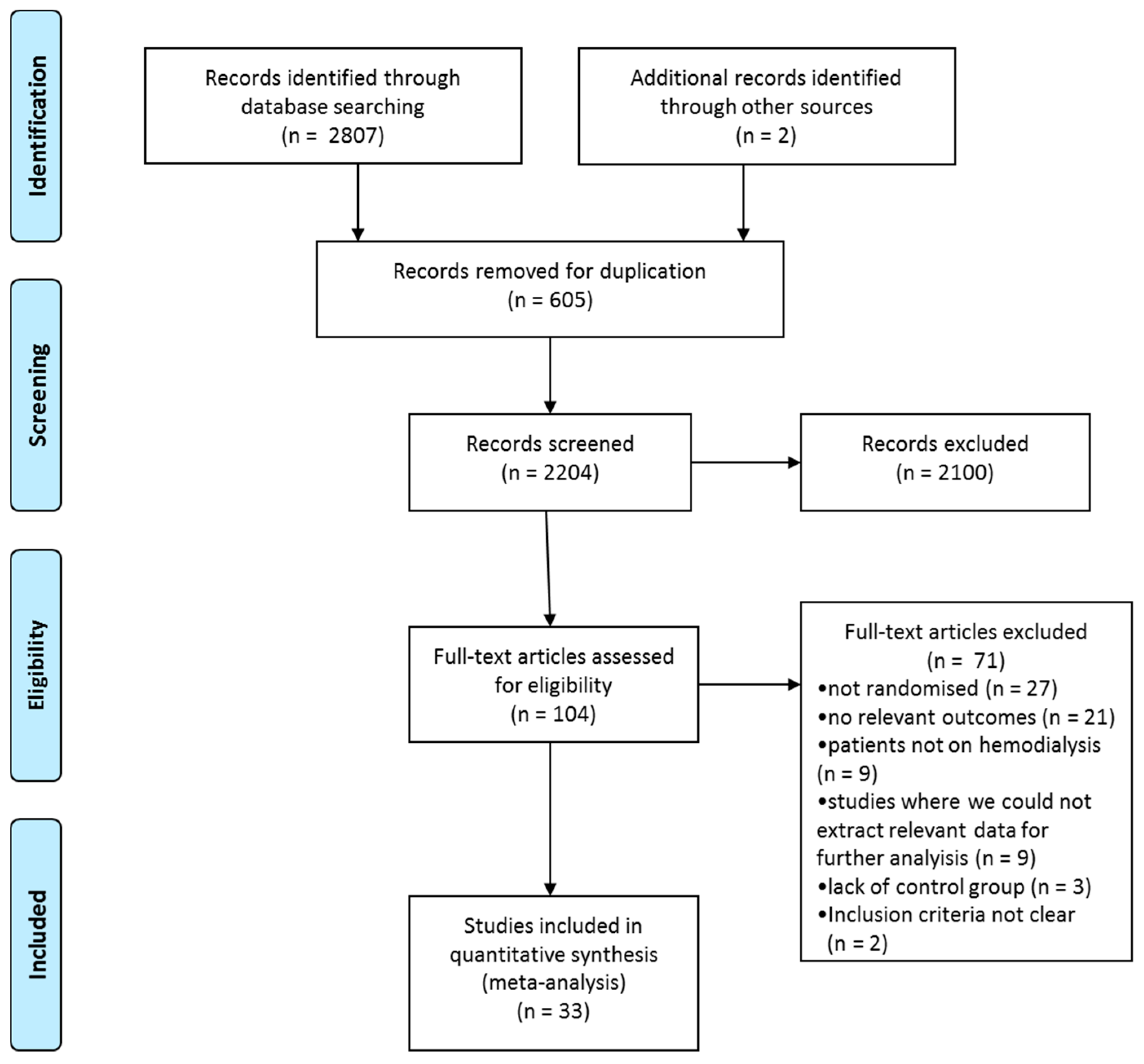
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Screening Strategy
2.4. Data Extraction
2.5. Quality Assessment
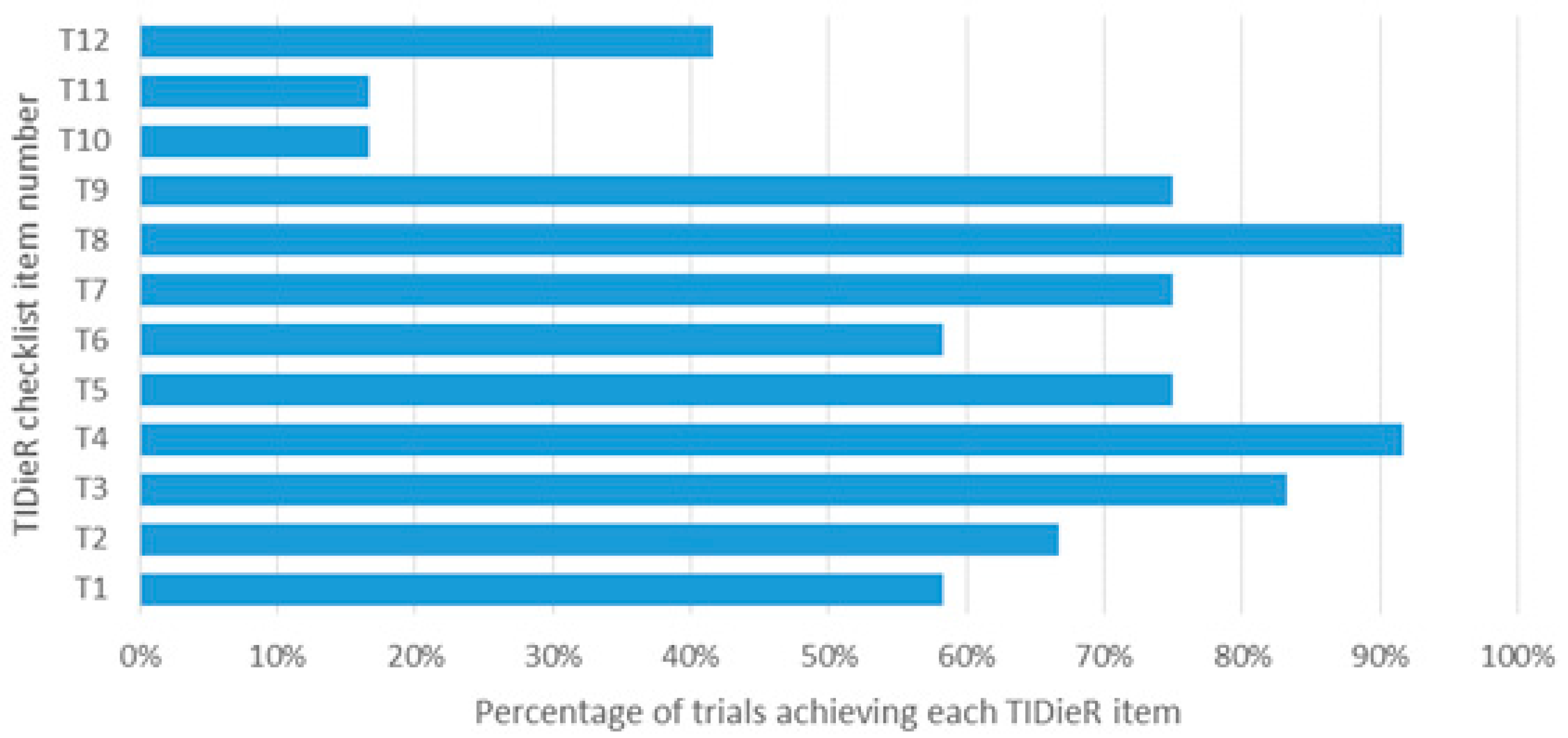
2.6. Completeness of Intervention Description
2.7. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Completeness of Intervention Description
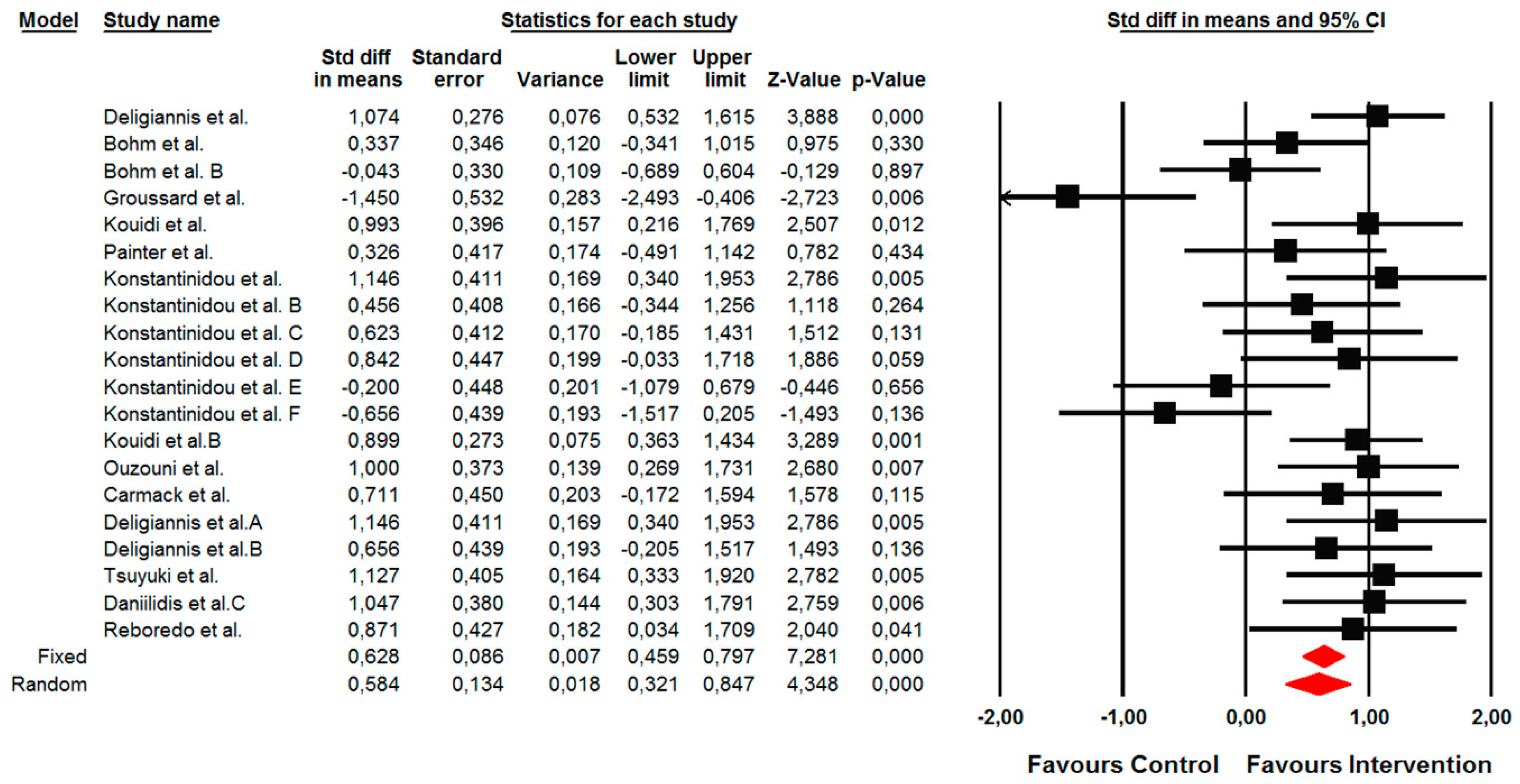
3.4. Effects of the Interventions on Measures of Functional Fitness/Capacities
3.4.1. Primary Outcome: Changes in Functional Capacity Measured by a 6-min Walk Test
3.4.2. Secondary Outcomes
Changes in Oxygen Consumption Measured by VO2max and peakVO2 Tests
Changes in Lower Limb Strength Endurance Assessed by 10 Repetition Sit-to-Stand Test
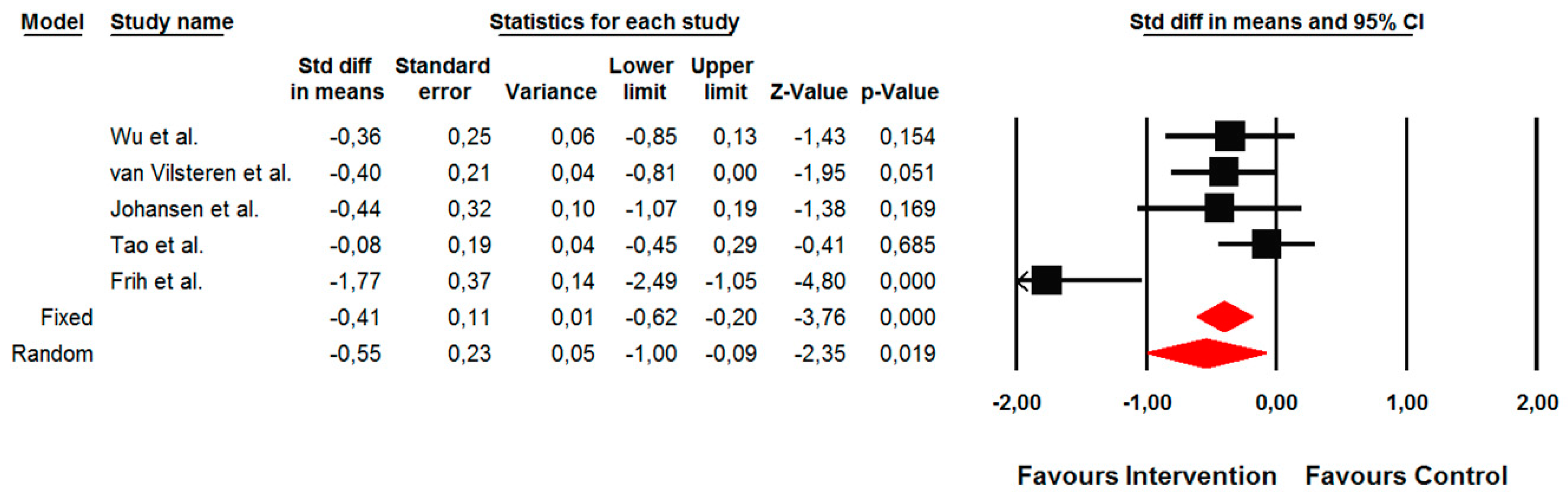
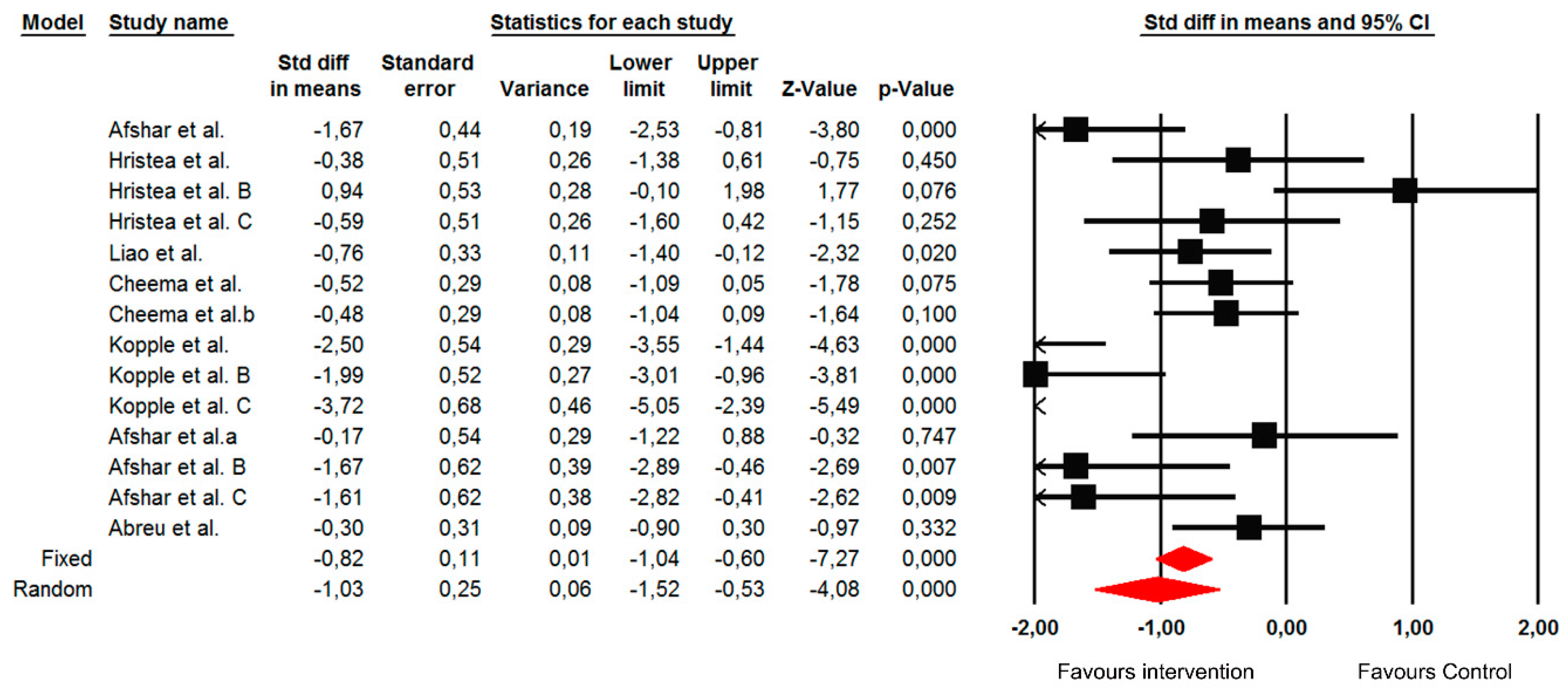
3.5. Effects of the Interventions on the Measures of Inflammation Biomarkers
Changes in the C-Reactive Protein (CRP)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global prevalence of chronic kidney disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- De Francisco, A. Future directions in therapy for chronic kidney disease. Nefrología 2010, 30, 1–9. [Google Scholar]
- United States Renal Data System. 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2018.
- Johansen, K.L.; Chertow, G.M.; Ng, A.V.; Mulligan, K.; Carey, S.; Schoenfeld, P.Y.; Kent-Braun, J.A. Physical activity levels in patients on hemodialysis and healthy sedentary controls. Kidney Int. 2000, 57, 2564–2570. [Google Scholar] [CrossRef] [Green Version]
- Bučar Pajek, M.; Pajek, J. Characterization of deficits across the spectrum of motor abilities in dialysis patients and the impact of sarcopenic overweight and obesity. Clin. Nutr. 2018, 37, 870–877. [Google Scholar] [CrossRef] [Green Version]
- Sietsema, K.E.; Amato, A.; Adler, S.G.; Brass, E.P. Exercise capacity as a predictor of survival among ambulatory patients with end-stage renal disease. Kidney Int. 2004, 65, 719–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daratha, K.B.; Short, R.A.; Corbett, C.F.; Ring, M.E.; Alicic, R.; Choka, R.; Tuttle, K.R. Risks of subsequent hospitalization and death in patients with kidney disease. Clin. J. Am. Soc. Nephrol. 2012, 7, 409–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vecchi, A.F.; Colucci, P.; Salerno, F.; Scalamogna, A.; Ponticelli, C. Outcome of peritoneal dialysis in cirrhotic patients with chronic renal failure. Am. J. Kidney Dis. 2002, 40, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Fitts, S.S. Physical benefits and challenges of exercise for people with chronic renal disease. J. Ren. Nutr. 1997, 7, 123–128. [Google Scholar] [CrossRef]
- Goldberg, A.P.; Geltman, E.M.; Hagberg, J.M.; Gavin, J.R.; Delmez, J.A.; Carney, R.M.; Naumowicz, A.; Oldfield, M.H.; Harter, H.R. Therapeutic benefits of exercise training for hemodialysis patients. Kidney Int. Suppl. 1983, 16, S303–S309. [Google Scholar]
- Heidari, B. C-reactive protein and other markers of inflammation in hemodialysis patients. Casp. J. Intern. Med. 2013, 4, 611–616. [Google Scholar]
- Sheng, K.; Zhang, P.; Chen, L.; Cheng, J.; Wu, C.; Chen, J. Intradialytic exercise in hemodialysis patients: A systematic review and meta-analysis. Am. J. Nephrol. 2014, 40, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.; Steele, M. Exercise training in hemodialysis patients: A systematic review and meta-analysis. Nephrology 2011, 16, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L.; Chertow, G.M.; da Silva, M.; Carey, S.; Painter, P. Determinants of physical performance in ambulatory patients on hemodialysis. Kidney Int. 2001, 60, 1586–1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, N.; McFarlane, J.; Cornelissen, V. The effect of exercise therapy on physical function, biochemistry and dialysis adequacy in haemodialysis patients: A systematic review and meta-analysis. Open J. Nephrol. 2013, 3, 25–36. [Google Scholar] [CrossRef] [Green Version]
- Scapini, K.B.; Bohlke, M.; Moraes, O.A.; Rodrigues, C.G.; Inácio, J.F.; Sbruzzi, G.; Leguisamo, C.P.; Sanches, I.C.; Tourinho Filho, H.; Irigoyen, M.C. Combined training is the most effective training modality to improve aerobic capacity and blood pressure control in people requiring haemodialysis for end-stage renal disease: Systematic review and network meta-analysis. J. Physiother. 2019, 65, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Do, J.Y.; Jeong, H.Y.; Lee, S.-Y.; Kim, J.C. The clinical significance of physical activity in maintenance dialysis patients. Kidney Blood Press. Res. 2017, 42, 575–586. [Google Scholar] [CrossRef] [Green Version]
- Shimoda, T.; Matsuzawa, R.; Hoshi, K.; Yoneki, K.; Harada, M.; Watanabe, T.; Matsunaga, A. Effects of supervised exercise on depressive symptoms in hemodialysis patients: A systematic review and meta-analysis of randomized controlled trials. Ren. Replace. Ther. 2017, 3, 56. [Google Scholar] [CrossRef] [Green Version]
- Parker, K. Intradialytic exercise is medicine for hemodialysis patients. Curr. Sports Med. Rep. 2016, 15, 269–275. [Google Scholar]
- Lu, Y.; Wang, Y.; Lu, Q. Effects of exercise on muscle fitness in dialysis patients: A systematic review and meta-analysis. Am. J. Nephrol. 2019, 50, 291–302. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Consumers and Communication Group Resources for Authors. Available online: https://cccrg.cochrane.org/author-resources (accessed on 7 January 2019).
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [PubMed] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sport. Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; He, Q.; Yin, X.; He, Q.; Cao, S.; Ying, G. Effect of individualized exercise during maintenance haemodialysis on exercise capacity and health-related quality of life in patients with uraemia. J. Int. Med. Res. 2014, 42, 718–727. [Google Scholar] [CrossRef]
- Bohm, C.; Stewart, K.; Onyskie-Marcus, J.; Esliger, D.; Kriellaars, D.; Rigatto, C. Effects of intradialytic cycling compared with pedometry on physical function in chronic outpatient hemodialysis: A prospective randomized trial. Nephrol. Dial. Transplant 2014, 29, 1947–1955. [Google Scholar] [CrossRef] [Green Version]
- Reboredo, M.M.; Neder, J.A.; Pinheiro, B.V.; Henrique, D.M.; Lovisi, J.C.; Paula, R.B. Intra-dialytic training accelerates oxygen uptake kinetics in hemodialysis patients. Eur. J. Prev. Cardiol. 2015, 22, 912–919. [Google Scholar] [CrossRef]
- Groussard, C.; Rouchon-Isnard, M.; Coutard, C.; Romain, F.; Malardé, L.; Lemoine-Morel, S.; Martin, B.; Pereira, B.; Boisseau, N. Beneficial effects of an intradialytic cycling training program in patients with end-stage kidney disease. Appl. Physiol. Nutr. Metab. 2015, 40, 550–556. [Google Scholar] [CrossRef]
- Liao, M.-T.; Liu, W.-C.; Lin, F.-H.; Huang, C.-F.; Chen, S.-Y.; Liu, C.-C.; Lin, S.-H.; Lu, K.-C.; Wu, C.-C. Intradialytic aerobic cycling exercise alleviates inflammation and improves endothelial progenitor cell count and bone density in hemodialysis patients. Medicine (Baltimore) 2016, 95, e4134. [Google Scholar] [CrossRef]
- Cheema, B.; Abas, H.; Smith, B.; O’Sullivan, A.; Chan, M.; Patwardhan, A.; Kelly, J.; Gillin, A.; Pang, G.; Lloyd, B.; et al. Randomized controlled trial of intradialytic resistance training to target muscle wasting in ESRD: The progressive exercise for anabolism in kidney disease (PEAK) study. Am. J. Kidney Dis. 2007, 50, 574–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkman, D.L.; Mullins, P.; Junglee, N.A.; Kumwenda, M.; Jibani, M.M.; Macdonald, J.H. Anabolic exercise in haemodialysis patients: A randomised controlled pilot study. J. Cachexia Sarcopenia Muscle 2014, 5, 199–207. [Google Scholar] [CrossRef] [PubMed]
- DePaul, V.; Moreland, J.; Eager, T.; Clase, C.M. The effectiveness of aerobic and muscle strength training in patients receiving hemodialysis and EPO: A randomized controlled trial. Am. J. Kidney Dis. 2002, 40, 1219–1229. [Google Scholar] [CrossRef] [PubMed]
- Abreu, C.C.; Cardozo, L.F.M.F.; Stockler-Pinto, M.B.; Esgalhado, M.; Barboza, J.E.; Frauches, R.; Mafra, D. Does resistance exercise performed during dialysis modulate Nrf2 and NF-κB in patients with chronic kidney disease? Life Sci. 2017, 188, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Van Vilsteren, M.C.B.A.; de Greef, M.H.G.; Huisman, R.M. The effects of a low-to-moderate intensity pre-conditioning exercise programme linked with exercise counselling for sedentary haemodialysis patients in The Netherlands: Results of a randomized clinical trial. Nephrol. Dial. Transplant. 2005, 20, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Johansen, K.L.; Painter, P.L.; Sakkas, G.K.; Gordon, P.; Doyle, J.; Shubert, T. Effects of resistance exercise training and nandrolone decanoate on body composition and muscle function among patients who receive hemodialysis: A randomized, controlled trial. J. Am. Soc. Nephrol. 2006, 17, 2307–2314. [Google Scholar] [CrossRef]
- Deligiannis, A.; Kouidi, E.; Tourkantonis, A. Effects of physical training on heart rate variability in patients on hemodialysis. Am. J. Cardiol. 1999, 84, 197–202. [Google Scholar] [CrossRef]
- Kouidi, E.J.; Grekas, D.M.; Deligiannis, A.P. Effects of exercise training on noninvasive cardiac measures in patients undergoing long-term hemodialysis: A randomized controlled trial. Am. J. Kidney Dis. 2009, 54, 511–521. [Google Scholar] [CrossRef]
- Ouzouni, S.; Kouidi, E.; Sioulis, A.; Grekas, D.; Deligiannis, A. Effects of intradialytic exercise training on health-related quality of life indices in haemodialysis patients. Clin. Rehabil. 2009, 23, 53–63. [Google Scholar] [CrossRef]
- Daniilidis, M.; Kouidi, E.; Giagoudaki, F.; Fleva, A.; Nikolaides, P.; Vasilaki, A.; Deligiannis, A.; Tourkantonis, A. The immune response in hemodialysis patients following physical training. Sport Sci. Health 2004, 1, 11–16. [Google Scholar] [CrossRef]
- Tao, X.; Chow, S.K.Y.; Wong, F.K.Y. A nurse-led case management program on home exercise training for hemodialysis patients: A randomized controlled trial. Int. J. Nurs. Stud. 2015, 52, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Frih, B.; Jaafar, H.; Mkacher, W.; Ben Salah, Z.; Hammami, M.; Frih, A. The effect of interdialytic combined resistance and aerobic exercise training on health related outcomes in chronic hemodialysis patients: The tunisian randomized controlled study. Front. Physiol. 2017, 8, 288. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, P.L.; de Alba, A.; Pedrero-Chamizo, R.; Morales, J.S.; Cobo, F.; Botella, A.; González-Gross, M.; Pérez, M.; Lucia, A.; Marín-López, M.T. Intradialytic exercise: One size doesn’t fit all. Front. Physiol. 2018, 9, 844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinidou, E.; Koukouvou, G.; Kouidi, E.; Deligiannis, A.; Tourkantonis, A. Exercise training in patients with end-stage renal disease on hemodialysis: Comparison of three rehabilitation programs. J. Rehabil. Med. 2002, 34, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Pellizzaro, C.O.; Thomé, F.S.; Veronese, F.V. Effect of peripheral and respiratory muscle training on the functional capacity of hemodialysis patients. Ren. Fail. 2013, 35, 189–197. [Google Scholar] [CrossRef]
- Segura-Ortí, E.; Kouidi, E.; Lisón, J.F. Effect of resistance exercise during hemodialysis on physical function and quality of life: Randomized controlled trial. Clin. Nephrol. 2009, 71, 527–537. [Google Scholar] [CrossRef]
- Kouidi, E.; Iacovides, A.; Iordanidis, P.; Vassiliou, S.; Deligiannis, A.; Ierodiakonou, C.; Tourkantonis, A. Exercise renal rehabilitation program: Psychosocial effects. Nephron 1997, 77, 152–158. [Google Scholar] [CrossRef]
- Afshar, R.; Emany, A.; Saremi, A.; Shavandi, N.; Sanavi, S. Effects of intradialytic aerobic training on sleep quality in hemodialysis patients. Iran. J. Kidney Dis. 2011, 5, 119–123. [Google Scholar]
- Hristea, D.; Deschamps, T.; Paris, A.; Lefrançois, G.; Collet, V.; Savoiu, C.; Ozenne, S.; Coupel, S.; Testa, A.; Magnard, J. Combining intra-dialytic exercise and nutritional supplementation in malnourished older haemodialysis patients: Towards better quality of life and autonomy. Nephrology 2016, 21, 785–790. [Google Scholar] [CrossRef]
- Painter, P.; Moore, G.; Carlson, L.; Paul, S.; Myll, J.; Phillips, W.; Haskell, W. Effects of exercise training plus normalization of hematocrit on exercise capacity and health-related quality of life. Am. J. Kidney Dis. 2002, 39, 257–265. [Google Scholar] [CrossRef]
- Kopple, J.D.; Wang, H.; Casaburi, R.; Fournier, M.; Lewis, M.I.; Taylor, W.; Storer, T.W. Exercise in maintenance hemodialysis patients induces transcriptional changes in genes favoring anabolic muscle. J. Am. Soc. Nephrol. 2007, 18, 2975–2986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, K.P.; Fassett, R.G.; Sharman, J.E.; Coombes, J.S.; Williams, A.D. Effect of intradialytic versus home-based aerobic exercise training on physical function and vascular parameters in hemodialysis patients: A randomized pilot study. Am. J. Kidney Dis. 2010, 55, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Afshar, R.; Shegarfy, L.; Shavandi, N.; Sanavi, S. Effects of aerobic exercise and resistance training on lipid profiles and inflammation status in patients on maintenance hemodialysis. Indian J. Nephrol. 2010, 20, 185–189. [Google Scholar] [PubMed]
- Orcy, R.B.; Dias, P.S.; Seus, T.L.; Barcellos, F.C.; Bohlke, M. Combined resistance and aerobic exercise is better than resistance training alone to improve functional performance of haemodialysis patients—Results of a randomized controlled trial. Physiother. Res. Int. 2012, 17, 235–243. [Google Scholar] [CrossRef]
- Carmack, C.L.; Amaral-Melendez, M.; Boudreaux, E.; Brantley, P.J.; Jones, G.N.; Franks, B.D.; McKnight, G.T. Exercise as a component of the physical and psychological rehabilitation of hemodialysis patients. Int. J. Rehabil. Health 1995, 1, 13–23. [Google Scholar] [CrossRef]
- Tsuyuki, K.; Kimura, Y.; Chiashi, K.; Matsushita, C.; Ninomiya, K.; Choh, K.; Hase, H.; Dohi, S. Oxygen uptake efficiency slope as monitoring tool for physical training in chronic hemodialysis patients. Ther. Apher. Dial. 2003, 7, 461–467. [Google Scholar] [CrossRef]
- Dobsak, P.; Homolka, P.; Svojanovsky, J.; Reichertova, A.; Soucek, M.; Novakova, M.; Dusek, L.; Vasku, J.; Eicher, J.-C.; Siegelova, J. Intra-dialytic electrostimulation of leg extensors may improve exercise tolerance and quality of life in hemodialyzed patients. Artif. Organs 2012, 36, 71–78. [Google Scholar] [CrossRef]
- Deligiannis, A.; Kouidi, E.; Tassoulas, E.; Gigis, P.; Tourkantonis, A.; Coats, A. Cardiac effects of exercise rehabilitation in hemodialysis patients. Int. J. Cardiol. 1999, 70, 253–266. [Google Scholar] [CrossRef]
- Heiwe, S.; Jacobson, S.H. Exercise training in adults with CKD: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 64, 383–393. [Google Scholar] [CrossRef]
- Matsuzawa, R.; Hoshi, K.; Yoneki, K.; Harada, M.; Watanabe, T.; Shimoda, T.; Yamamoto, S.; Matsunaga, A. Exercise training in elderly people undergoing hemodialysis: A systematic review and meta-analysis. Kidney Int. Rep. 2017, 2, 1096–1110. [Google Scholar] [CrossRef] [Green Version]
- Heresi, G.A.; Dweik, R.A. Strengths and limitations of the six-minute-walk test. Am. J. Respir. Crit. Care Med. 2011, 183, 1122–1124. [Google Scholar] [CrossRef] [PubMed]
- Bučar Pajek, M.; Čuk, I.; Leskošek, B.; Mlinšek, G.; Buturović Ponikvar, J.; Pajek, J. Six-minute walk test in renal failure patients: Representative results, performance analysis and perceived dyspnea predictors. PLoS ONE 2016, 11, e0150414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, D.-C.; Kim, M.-J.; Lee, C.-M. Meta-analysis on the effect of combined exercise program intervention on Korean middle-aged women. J. Exerc. Rehabil. 2018, 14, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Bučar Pajek, M.; Leskošek, B.; Vivoda, T.; Svilan, K.; Čuk, I.; Pajek, J. Integrative examination of motor abilities in dialysis patients and selection of tests for a standardized physical function assessment. Ther. Apher. Dial. 2016, 20, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Puhan, M.A.; Siebeling, L.; Zoller, M.; Muggensturm, P.; ter Riet, G. Simple functional performance tests and mortality in COPD. Eur. Respir. J. 2013, 42, 956–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panichi, V.; Migliori, M.; De Pietro, S.; Taccola, D.; Bianchi, A.M.; Norpoth, M.; Metelli, M.R.; Giovannini, L.; Tetta, C.; Palla, R. C reactive protein in patients with chronic renal diseases. Ren. Fail. 2001, 23, 551–562. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, J.; Herrlinger, S.; Pruy, A.; Metzger, T.; Wanner, C. Inflammation enhances cardiovascular risk and mortality in hemodialysis patients. Kidney Int. 1999, 55, 648–658. [Google Scholar] [CrossRef] [Green Version]
- Fedewa, M.V.; Hathaway, E.D.; Ward-Ritacco, C.L. Effect of exercise training on C reactive protein: A systematic review and meta-analysis of randomised and non-randomised controlled trials. Br. J. Sports Med. 2017, 51, 670–676. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population Sex; Age (years) (mean ± SD) | Time on Dialysis (months) | Sample Size | Training Program | Outcome Measure | Results |
|---|---|---|---|---|---|---|
| Deligiannis 1999 [39] | M and F; Ex 48 ± 12 Con 48 ± 11 | Ex 75.6 ± 36.0 Con 74.4 ± 43.2 | Ex (n = 30) Con (n = 30) | Ex: AER; 6 months; 3 days/week; 90 min; 60%–70% HRmax Con: usual care | VO2max | Ex: 41.0% ↑ * Con: no changes |
| Afshar 2011 [50] | M; Ex 50.71 ± 21.06 Con 53 ± 19.4 | Ex 25.71 ± 7.61 Con 24.86 ± 15.44 | Ex (n = 14) Con (n = 14) | Ex: AER; 8 weeks; 3 days/week; 20 min; 12–15 RPE Con: usual care | CRP | Ex: 83.2% ↓ ** Con: 1.2% ↑ |
| Wu 2014 [28] | M and F; Ex 45 Con 44 | Ex 55.5 ± 37.3 Con 39.8 ± 29.7 | Ex (n = 34) Con (n = 35) | Ex: AER; 12 weeks; 3 days/week; 13 min; 12–16 RPE Con: stretching; 12 weeks; 3 days/week; 10–15 min | 6MWT STS-10 | Ex: 8.09% ↓ * Con: 4.77% ↓ Ex: 5.7% ↓ * Con: 5.0% ↓ |
| Bohm 2014 [29] | M and F; Ex 52 ± 14.5 Con 53 ± 16.9 | Ex 37 ± 69 Con 21 ± 30 | Ex (n = 27) Con (n = 26) | Ex: AER; 12 weeks; 3 days/week; 45 min; 13 RPE Con: walking program at home | peakVO2 6MWT | Ex: fter 12 weeks: 9.89% ↑ after 24 weeks: no change Con: after 12 weeks: 3.31% ↓ after 24 weeks: 1.66% ↑ Ex: after 12 weeks: 6.58% ↑ after 24 weeks: 3.96% ↑ Con: after 12 weeks: 1.67% ↑ after 24 weeks: 0.05% ↓ |
| Groussard 2015 [31] | M and F; Ex 66.5 ± 4.6 Con 68.4 ± 3.7 | Ex 36.6 ± 8.2 Con 41.2 ± 8.1 | Ex (n = 8) Con (n = 10) | Ex: AER; 3 months; 3 days/week; 30 min; 55%–60% peak power Con: usual care | 6MWT peakVO2 | Ex: 23.15% ↑ ** Con: 7.98% ↑ Ex: 2.72% ↓ Con: 14.18% ↑ |
| Hristea 2016 [51] | M and F; Ex 68.5 ± 13.97 Con 70.8 ± 15.18 | Ex 139 Con 96 | Ex (n = 10) Con (n = 11) | Ex: AER; 6 months; 3 days/week; 30 min; 3 RPE (modified Borg scale) Con: usual care | 6MWT CRP | Ex: 21.8% ↑ ** Con: 18.8% ↓ Ex: 30.6% ↓** Con: 19.8% ↓ |
| Liao 2016 [32] | M and F; Ex 62 ± 8 Con 62 ± 9 | Ex 71 ± 46 Con 83 ± 71 | Ex (n = 20) Con (n = 20) | Ex: AER; 3 months; 3 days/week; 20 min; 13–14 RPE Con: usual care | CRP 6MWT | Ex: 37.6% ↓ * Con: 0.81% ↓ Ex: 11.1% ↑ * Con: 1.1% ↓ |
| Cheema 2007 [33] | M and F; Ex 60.0 ± 15.3 Con 65.0 ± 12.9 | Ex 39.6 Con 19.2 | Ex (n = 24) Con (n = 25) | Ex: RT; 12 weeks; 3 days/week; 45 min; 15–17 RPE Con: usual care | 6MWT CRP | Ex: 3.36% ↑ Con: 0.74% ↓ Ex: 10.26% ↓ * Con: 33.33% ↑ * |
| Kirkman 2014 [34] | M and F; Ex 48 ± 18 Con 58 ± 15 | Ex 46 ± 54 Con 66 ± 47 | Ex (n = 9) Con (n = 10) | Ex: RT; 12 weeks; 2 days/week; 80% of their predicted 1 RM Con: stretching | 6MWT | Ex: 7.33% ↑ Con: 13.04% ↑ |
| Kouidi 1997 [49] | M and F; Ex 49.6 ± 12.1 Con 52.8 ± 10.2 | Ex 70.8 ± 58.8 Con 74.4 ± 64.8 | Ex (n = 20) Con (n = 11) | Ex: COMB; 6 months; 3 days/week; 90 min; 50%–60% VO2max Con: usual care | VO2max | Ex: 38.09% ↑ * Con: 1.24% ↓ |
| Painter 2002 [52] | M and F; Ex 55.9 ± 15.15 Con 52.8 ± 16.8 | Ex 33.7 ± 35.6 Con 40.2 ± 62.4 | Ex: AER; 5 months; 3 days/week; 30 min; 12–14 RPE Con: usual care | peak VO2 | Ex: 13.3% ↑ * Con: 0.5% ↑ | |
| DePaul 2002 [35] | M and F; Ex 55 ± 16 Con 54 ± 14 | Ex 50.4 ± 57.6 Con 55.2 ± 54.0 | Ex (n = 20) Con (n = 18) | Ex: COMB; 12 weeks; 3 days/week; 30 min; 13 RPE Con: range-of-motion exercises; 12 weeks; 3 days/week; 30 min | 6MWT | Ex: 0.87% ↑ Con: 0.94% ↑ |
| Konstantinidou 2002 [46] | M and F; group A 46.4 ± 13.9 group B 48.3 ± 12.1 group C 51.4 ± 12.5 group D 50.2 ± 7.9 | group A 78 ± 62 group B 72 ± 66 group C 62 ± 37 group D 79 ± 86 | group A (n = 16) group B (n = 10) group C (n = 10) group D (n = 12) | group A: COMB; 6 months; 3 days/week; 60 min; 60%–70% HRmax group B: COMB; 6 months; 3 days/week; 70% HRmax group C: AER 6 months; 5 days/week; 50%–60% HRmax group D: usual care | peakVO2 | group A: 42.77 % ↑ * group B: 23.93% ↑ * group C: 17.28% ↑ * group D: 3.07% ↓ |
| van Vilsteren 2005 [37] | M and F; Ex 52 ± 15 Con 58 ± 16 | Ex 38.6 ± 48.9 Con 46.8 ± 52.9 | Ex (n = 53) Con (n = 43) | Ex: COMB; 12 weeks; 2–3 days/week; 60 min; 12–16 RPE Con: usual care | STS-10 peakVO2 | Ex: 22.36% ↓ * Con: 0.25% ↓ Ex: 10.14% ↑ Con: 0.46% ↑ |
| Kopple 2007 [53] | M and F; group 1 45.9 ± 4.1 group 2 46.0 ± 2.7 group 3 42.7 ± 3.8 group 4 41.3 ± 3.3 | group 1 45.9 ± 14.1 group 2 51.9 ± 12.4 group 3 38.3 ± 5.8 group 4 51.4 ± 21.0 | group 1 (n = 10) group 2 (n = 15) group 3 (n = 12) group 4 (n = 14) | Group 1: AER; 5 months; 3 days/week; 30 min; 50% peakVO2 Group 2: RT; 5 months; 3 days/week; 5% of the 5 RM Group 3: COMB;5 months; 3 days/week Group 4: usual care | CRP | group 1: 44.44% ↓ group 2: 20.00% ↑ group 3: 26.09% ↑ group 4: 33.33% ↑ |
| Kouidi 2009 [40] | M and F; Ex 54.6 ± 8.9 Con 53.2 ± 6.1 | Ex 75.6 ± 44.4 Con 74.4 ± 46.8 | Ex (n = 30) Con (n = 29) | Ex: COMB; 10 months; 3 days/week; 90 min; 13 RPE Con: usual care | peakVO2 | Ex: 30.49% ↑ ** Con: 1.19% ↓ |
| Koh 2010 [54] | M and F; group 1 52.3 ± 10.9 group 2 52.1 ± 13.6 group 3 51.3 ± 14.4 | group 1 32.1 ± 26.7 group 2 37.0 ± 31.1 group 3 25.8 ± 22.2 | group 1 (n = 15) group 2 (n = 15) group 3 (n = 16) | group 1: AER; 6 months; 3 days/week; 30 min; 13–14 RPE group 2: walking; 6 months; 3 days/week; 30 min; 13–14 RPE group 3: usual care | 6MWT | group 1: 13.61% ↑ group 2: 11.04% ↑ group 3: 4.87% ↑ |
| Afshar 2010 [55] | M; group 1 50.7 ± 21.06 group 2 51 ± 16.4 group 3 53 ± 19.4 | group 1 25.71 ± 7.61 group 2 24.86 ± 18.69 group 3 24.86 ± 15.44 | group 1 (n = 7) group 2 (n = 7) group 3 (n = 7) | group 1: AER; 8 weeks; 3 days/week; 30 min; 12–16 RPE group 2: RT; 8 weeks; 3 days/week; 30 min; 15–17 RPE group 3: usual care | CRP | group 1: 83.85% ↓ ** group 2: 67.89% ↓ * group 3: 1.47% ↑ |
| Ouzouni 2009 [41] | M and F; Ex 47.4 ± 15.7 Con 50.5 ± 11.7 | Ex 92.4 ± 84 Con 103.2 ± 72 | Ex (n = 19) Con (n = 14) | Ex: COMB; 10 months; 3 days/week; 60–90 min 13–14 RPE Con: usual care | peakVO2 | Ex: 21.05% ↑* Con: 0.99% ↓ |
| Orcy 2012 [56] | M and F; group 1 56.9 ± 14.8 group 2 55.8 ± 18.3 | group 1 22.5 group 2 23 | group 1 (n = 13) group 2 (n = 13) | group 1: COMB; 10 weeks; 3 days/week; 13–14 RPE group 2: RT; 10 weeks; 3 days/week; 13–14 RPE | 6MWT | group 1: 9.01% ↑ * group 2: 4.48% ↓ |
| Tao 2015 [43] | M and F; Ex 53.02 ± 11.62 Con 56.68 ± 9.67 | Ex 83.46 ± 61.37 Con 84.70 ± 70.55 | Ex (n = 57) Con (n = 56) | Ex: RT; 6 weeks; 1 day/week; 20 min; RPE 12–13 + home exercise; 1 day/week; 20 min Con: RT; 6 weeks; 1 day/week; 20 min; RPE 12–13 | STS-10 | Ex: 21.03% ↓ ** Con: 16.24% ↓* |
| Carmack 1995 [57] | M and F; All subjects 44.09 | All subjects 29.52 | Ex (n = 10) Con (n = 11) | Ex: AER; 10 weeks; 3 days/week; 25 min Con: usual care | peakVO2 | Ex: 34.58% ↑ * Con: 9.0% ↑ |
| Deligiannis 1999 [39] | M and F; group 1 46.4 ± 13.9 group 2 51.4 ± 12.5 group 3 50.2 ± 1.9 | group 1 78 ± 62 group 2 62 ± 37 group 3 79 ± 86 | group 1 (n = 16) group 2 (n = 10) group 3 (n = 12) | group 1: COMB; 6 months; 3 days/week; 90 min; 60%–70% HRmax group 2: AER; 6 months; 5 days/week; 30 min; 50%–60% HRmax + simple flexibility and muscular extension exercises group 3: usual care | VO2max | group 1: 42.8% ↑** group 2: 17.3% ↑* group 3: 3.07% ↓ |
| Tsuyuki 2003 [58] | M and F; Ex 40.1 ± 11.9 Con 39.7 ± 10.7 | Ex 25.2 Con 32.4 | Ex (n = 17) Con (n = 12) | Ex: AER; 20 weeks; 2–3 days/week; 30 min; 50%–60% of the peak heart rate Con: usual care | peakVO2 | Ex: 25.58% ↑ ** Con: 2.25% ↓ |
| Segura-Ortí 2009 [48] | M and F; group 1 53.5 ± 18.0 group 2 60.1 ± 16.9 | group 1 37.3 ± 34.9 group 2 53.7 ± 42.0 | group 1 (n = 17) group 2 (n = 18) | group 1: RT; 6 months; 3 days/week; 25 min; 12–14 RPE group 2: AER; 6 months; 3 days/week; 25 min; 11 RPE | STS-10 6MWT | group 1: 22.31% ↓ ** group 2: 6.37% ↓ group 1: 11.21% ↑ ** group 2: 8.95% ↑ |
| Johansen 2006 [38] | M and F; Ex 54.4 ± 13.6 Con 56.8 ± 13.8 | Ex 33.0 Con 25.5 | Ex (n = 20) Con (n = 20) | Ex: RT; 12 weeks; 3 days/week Con: usual care | STS-10 | Ex: 16.11% ↓ Con: 0.66% ↓ |
| Daniilidis 2004 [42] | M and F; Ex 46.7 ± 13.8 Con 53.7 ± 7.1 | Ex 78 ± 62.4 Con 72 ± 81.8 | Ex (n = 18) Con (n = 14) | Ex: COMB; 6 months; 3 days/week; 60 min; 75%–85% of the estimated peak heart rate Con: usual care | peakVO2 | Ex: 42.77% ↑ * Con: 2.45% ↓ |
| Pellizzaro 2013 [47] | M and F; Ex 48.9 ± 10.1 Con 51.9 ± 11.6 | Ex 54 Con 54 | Ex (n = 14) Con (n = 14) | Ex: RT 10 weeks; 3 days/week; 50% of 1 RM Con: usual care | 6MWT | Ex: 6.84% ↑ * Con: 0.07% ↑ |
| Dobsak 2012 [59] | M and F; Ex 58.2 ± 7.2 Con 60.1 ± 8.2 | Ex 49.2 ± 25.2 Con 49.2 ± 27.6 | Ex (n = 11) Con (n = 10) | Ex: AER; 20 weeks; 3 days/week; 20–40 min; 60% peak workload Con: usual care | 6MWT | Ex: 15.02% ↑ ** Con: 3.32% ↓ |
| Reboredo 2015 [30] | M and F; Ex 50.7 ± 10.7 Con 42.2 ± 13.0 | Ex 39.6 ± 40.8 Con 57.6 ± 52.8 | Ex (n = 12) Con (n = 12) | Ex: AER; 12 weeks; 3 days/week; 43 min; 4–6 RPE Con: usual care | peakVO2 | Ex: 12.4% ↑ * Con: 9.2% ↓ |
| Frih 2017 [44] | M; Ex 64.2 ± 3.4 Con 65.2 ± 3.1 | Ex 72.7 ± 12.7 Con 73.6 ± 13.4 | Ex (n = 21) Con (n = 20) | Ex: COMB; 16 weeks; 4 days/week; 40 min; 5–6 RPE (Borg 10 grade scale); 60% of 1 RMCon: usual care | 6MWT STS-10 | Ex: 15.94% ↑ * Con: 1.56% ↓ Ex: 16.2% ↓ * Con: 0.95% ↑ |
| Valenzuela 2018 [45] | M and F; Ex 68 ± 13 Con 68 ± 11 | Ex 84 ± 60 Con 60 ± 48 | Ex (n = 27) Con (n = 40) | Ex: COMB; 14 weeks; 3 days/week; 50 min; RPE 13 Con: usual care | 6MWT STS-10 | Ex: 11.05% ↑ ** Con: 3.23% ↓ Ex: 22% ↓ ** Con: 6% ↑ |
| Abreu 2017 [36] | M and F; All subjects 46.4 ± 14.6 | ND | Ex (n = 25) Con (n = 19) | Ex: COMB; 12 weeks; 3 days/week; 30 min; 60% of 1 RM Con: usual care | CRP | Ex: 24.68% ↓ Con: 1.64% ↓ |
| Study | Criterion 1 | Criterion 2 | Criterion 3 | Criterion 4 | Criterion 5 | Criterion 6 | Criterion 7 | Criterion 8 | Criterion 9 | Criterion 10 | Criterion 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DePaul et al. [35] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Konstantinidou et al. [46] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| van Vilsteren et al. [37] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 6 |
| Johansen et al. [38] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Cheema et al. [33] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Wu et al. [28] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Bohm et al. [29] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Groussard et al. [31] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Hristea et al. [51] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Liao et al. [32] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Kirkman et al. [34] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 6 |
| Koh et al. [54] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 5 |
| Orcy et al. [56] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Segura-Orti et al. [48] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Pellizzaro et al. [47] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Dobsak et al. [59] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Frih et al. [44] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6 |
| Valenzuela et al. [45] | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Afshar et al. [50] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Kopple et al. [53] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Afshar et al. [55] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Abreu et al. [36] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Tao et al. [43] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Deligiannis et al. [60] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 4 |
| Kouidi et al. [49] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Painter et al. [52] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Kouidi et al. [40] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 6 |
| Ouzouni et al. [41] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Carmack et al. [57] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 3 |
| Deligiannis et al. [39] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 3 |
| Tsuyuki et al. [58] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 5 |
| Daniilidis et al. [42] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 4 |
| Reboredo et al. [30] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Coefficient | Standard Error | 95% Lower CI | 95% Upper CI | z Value | p Value | |
|---|---|---|---|---|---|---|
| 6-min walk test | ||||||
| Age of patients | 0.034 | 0.015 | 0.004 | 0.063 | 2.243 | 0.025 * |
| Time on dialysis | 0.005 | 0.003 | −0.002 | 0.012 | 1.382 | 0.167 |
| Duration of intervention (weeks) | −0.011 | 0.019 | −0.048 | 0.026 | −0.576 | 0.556 |
| Weekly frequency | 1.631 | 0.398 | 0.852 | 2.410 | 4.102 | <0.001 ** |
| Duration of single training session | 0.006 | 0.010 | −0.014 | 0.026 | 0.561 | 0.575 |
| Total number of training sessions | 0.000 | 0.006 | −0.012 | 0.013 | 0.013 | 0.989 |
| Total training volume | 0.000 | 0.000 | 0.000 | 0.000 | 0.319 | 0.750 |
| Oxygen consumption | ||||||
| Age of patients | −0.013 | 0.013 | −0.039 | 0.013 | −0.970 | 0.332 |
| Time on dialysis | 0.011 | 0.006 | −0.001 | 0.023 | 1.760 | 0.078 |
| Duration of intervention (weeks) | 0.024 | 0.017 | −0.009 | 0.057 | 1.447 | 0.148 |
| Weekly frequency | −0.322 | 0.227 | −0.768 | 0.124 | −1.417 | 0.157 |
| Duration of single training session | 0.017 | 0.008 | 0.002 | 0.032 | 2.248 | 0.025 * |
| Total number of training sessions | 0.003 | 0.005 | −0.007 | 0.012 | 0.520 | 0.603 |
| Total training volume | 0.000 | 0.000 | 0.000 | 0.000 | 1.730 | 0.084 |
| C-reactive protein | ||||||
| Age of patients | 0.077 | 0.024 | 0.031 | 0.124 | 3.272 | 0.001 ** |
| Time on dialysis | 0.013 | 0.006 | 0.001 | 0.024 | 2.113 | 0.035 * |
| Duration of intervention (weeks) | −0.035 | 0.043 | −0.119 | 0.049 | −0.822 | 0.411 |
| Weekly frequency | NA | NA | NA | NA | NA | NA |
| Duration of single training session | 0.000 | 0.036 | −0.071 | 0.071 | −0.001 | 0.999 |
| Total number of training sessions | −0.012 | 0.014 | −0.040 | 0.016 | −0.822 | 0.411 |
| Total training volume | 0.000 | 0.000 | −0.001 | 0.000 | −0.654 | 0.513 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogataj, Š.; Pajek, M.; Pajek, J.; Buturović Ponikvar, J.; Paravlic, A.H. Exercise-Based Interventions in Hemodialysis Patients: A Systematic Review with a Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010043
Bogataj Š, Pajek M, Pajek J, Buturović Ponikvar J, Paravlic AH. Exercise-Based Interventions in Hemodialysis Patients: A Systematic Review with a Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2020; 9(1):43. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010043
Chicago/Turabian StyleBogataj, Špela, Maja Pajek, Jernej Pajek, Jadranka Buturović Ponikvar, and Armin H. Paravlic. 2020. "Exercise-Based Interventions in Hemodialysis Patients: A Systematic Review with a Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 9, no. 1: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9010043