Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation


 , , , and
, , , and 
Abstract
:1. Introduction
2. Big Data in Nephrology and Transplantation: Registries and Administrative Claims
3. Using Electronic Health Record Data in Nephrology
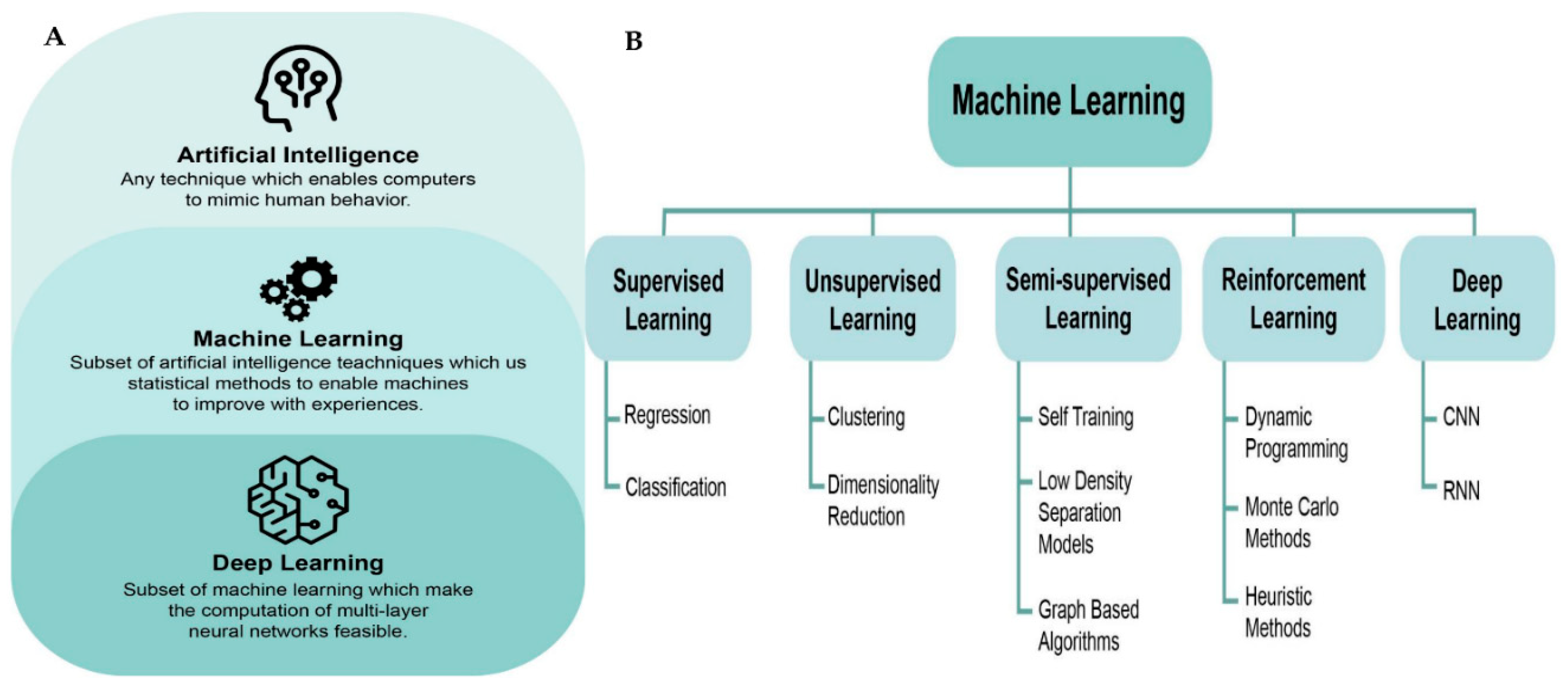
4. Artificial Intelligence in Nephrology and Transplantation
5. Potential Directions and Future Scope
6. Conclusions
Funding
Conflicts of Interest
References
- Sutherland, S.M.; Goldstein, S.L.; Bagshaw, S.M. Leveraging Big Data and Electronic Health Records to Enhance Novel Approaches to Acute Kidney Injury Research and Care. Blood Purif. 2017, 44, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Kashani, K.; Cheungpasitporn, W.; Ronco, C. Biomarkers of acute kidney injury: The pathway from discovery to clinical adoption. Clin. Chem. Lab. Med. 2017, 55, 1074–1089. [Google Scholar] [CrossRef] [PubMed]
- Srivali, N.; Thongprayoon, C.; Cheungpasitporn, W.; Ungprasert, P.; Caples, S.M. Unusual cause of pleural effusion: Ovarian hyperstimulation syndrome. QJM 2016, 109, 197–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanguankeo, A.; Upala, S.; Cheungpasitporn, W.; Ungprasert, P.; Knight, E.L. Effects of Statins on Renal Outcome in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0132970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Kittanamongkolchai, W.; Sakhuja, A.; Mao, M.A.; Erickson, S.B. Impact of admission serum potassium on mortality in patients with chronic kidney disease and cardiovascular disease. QJM 2017, 110, 713–739. [Google Scholar] [CrossRef]
- Jadlowiec, C.; Smith, M.; Neville, M.; Mao, S.; Abdelwahab, D.; Reddy, K.; Moss, A.; Aqel, B.; Taner, T. Acute Kidney Injury Patterns Following Transplantation of Steatotic Liver Allografts. J. Clin. Med. 2020, 9, 954. [Google Scholar] [CrossRef] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; O’Corragain, O.A.; Edmonds, P.J.; Kittanamongkolchai, W.; Erickson, S.B. Associations of sugar-sweetened and artificially sweetened soda with chronic kidney disease: A systematic review and meta-analysis. Nephrology 2014, 19, 791–797. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Chesdachai, S.; Panjawatanana, P.; Ungprasert, P.; Cheungpasitporn, W. Associations of Proton-Pump Inhibitors and H2 Receptor Antagonists with Chronic Kidney Disease: A Meta-Analysis. Dig. Dis. Sci. 2017, 62, 2821–2827. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Thamcharoen, N.; Panjawatanan, P.; Cheungpasitporn, W. Association of coffee consumption and chronic kidney disease: A meta-analysis. Int. J. Clin. Pr. 2017, 71. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Nissaisorakarn, P.; Jaruvongvanich, V.; Nakkala, K.; Rajapakse, R.; Cheungpasitporn, W. Association of Helicobacter pylori with Chronic Kidney Diseases: A Meta-Analysis. Dig. Dis. Sci. 2017, 62, 2045–2052. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Scribani, M.; Ungprasert, P.; Cheungpasitporn, W. Noninvasive fibrosis markers and chronic kidney disease among adults with nonalcoholic fatty liver in USA. Eur. J. Gastroenterol Hepatol. 2018, 30, 404–410. [Google Scholar] [CrossRef]
- Glassock, R.J.; Warnock, D.G.; Delanaye, P. The global burden of chronic kidney disease: Estimates, variability and pitfalls. Nat. Rev. Nephrol. 2017, 13, 104–114. [Google Scholar] [CrossRef]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.; Yang, C.W. Chronic kidney disease: global dimension and perspectives. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Kaewput, W.; Thongprayoon, C.; Rangsin, R.; Ruangkanchanasetr, P.; Bathini, T.; Mao, M.A.; Cheungpasitporn, W. Association between serum uric acid and chronic kidney disease in patients with hypertension: A multicenter nationwide cross-sectional study. J. Evid. Based Med. 2019, 12, 235–242. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Breuer, C.; Cabiddu, G.; Testa, A.; Jadeau, C.; Brunori, G. Where Are You Going, Nephrology? Considerations on Models of Care in an Evolving Discipline. J. Clin. Med. 2018, 7, 199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaewput, W.; Thongprayoon, C.; Chewcharat, A.; Rangsin, R.; Satirapoj, B.; Kaewput, C.; Suwannahitatorn, P.; Bathini, T.; Mao, M.A.; Cato, L.D.; et al. Rate of kidney function decline and factors predicting progression of kidney disease in type 2 diabetes mellitus patients with reduced kidney function: A nationwide retrospective cohort study. Ther. Apher. Dial. 2020. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Chen, T.; Li, Y.; Chen, T.; Li, X.; Liu, Z. Artificial Intelligence in Nephrology: How Can Artificial Intelligence Augment Nephrologists’ Intelligence? Kidney Dis. 2020, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Levin, A. Global challenges in kidney diseases. Nephrol Dial. Transpl. 2018, 33, 371–372. [Google Scholar] [CrossRef]
- Yang, C.; Kong, G.; Wang, L.; Zhang, L.; Zhao, M.-H. Big data in nephrology: Are we ready for the change? Nephrology 2019, 24, 1097–1102. [Google Scholar] [CrossRef] [Green Version]
- Kolachalama, V.B.; Singh, P.; Lin, C.Q.; Mun, D.; Belghasem, M.E.; Henderson, J.M.; Francis, J.M.; Salant, D.J.; Chitalia, V.C. Association of Pathological Fibrosis With Renal Survival Using Deep Neural Networks. Kidney Int. Rep. 2018, 3, 464–475. [Google Scholar] [CrossRef] [Green Version]
- Bello, A.K.; Levin, A.; Tonelli, M.; Okpechi, I.G.; Feehally, J.; Harris, D.; Jindal, K.; Salako, B.L.; Rateb, A.; Osman, M.A.; et al. Assessment of Global Kidney Health Care Status. JAMA 2017, 317, 1864–1881. [Google Scholar] [CrossRef] [PubMed]
- Inrig, J.K.; Califf, R.M.; Tasneem, A.; Vegunta, R.K.; Molina, C.; Stanifer, J.W.; Chiswell, K.; Patel, U.D. The landscape of clinical trials in nephrology: A systematic review of Clinicaltrials.gov. Am. J. Kidney Dis. 2014, 63, 771–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulsen, T.; Jamuar, S.S.; Moody, A.R.; Karnes, J.H.; Varga, O.; Hedensted, S.; Spreafico, R.; Hafler, D.A.; McKinney, E.F. From Big Data to Precision Medicine. Front. Med. 2019, 6, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shilo, S.; Rossman, H.; Segal, E. Axes of a revolution: Challenges and promises of big data in healthcare. Nat. Med. 2020, 26, 29–38. [Google Scholar] [CrossRef]
- Gameiro, J.; Branco, T.; Lopes, J.A. Artificial Intelligence in Acute Kidney Injury Risk Prediction. J. Clin. Med. 2020, 9, 678. [Google Scholar]
- Gore, E.J.; Gomes-Neto, A.W.; Wang, L.; Bakker, S.; Niesters, H.; de Joode, A.; Verschuuren, E.; Westra, J.; Leer-Buter, C.V. Torquetenovirus Serum Load and Long-Term Outcomes in Renal Transplant Recipients. J. Clin. Med. 2020, 9, 440. [Google Scholar] [CrossRef] [Green Version]
- Swarte, J.C.; Douwes, R.M.; Hu, S.; Vich Vila, A.; Eisenga, M.F.; van Londen, M.; Gomes-Neto, A.W.; Weersma, R.K.; Harmsen, H.; Bakker, S. Characteristics and Dysbiosis of the Gut Microbiome in Renal Transplant Recipients. J. Clin. Med. 2020, 9, 386. [Google Scholar] [CrossRef] [Green Version]
- Thölking, G.; Gillhaus, N.H.; Schütte-Nütgen, K.; Pavenstädt, H.; Koch, R.; Suwelack, B.; Reuter, S. Conversion to Everolimus was Beneficial and Safe for Fast and Slow Tacrolimus Metabolizers After Renal Transplantation. J. Clin. Med. 2020, 9, 328. [Google Scholar] [CrossRef] [Green Version]
- Cheungpasitporn, W.; Kremers, W.K.; Lorenz, E.; Amer, H.; Cosio, F.G.; Stegall, M.D.; Gandhi, M.J.; Schinstock, C.A. De novo donor-specific antibody following BK nephropathy: The incidence and association with antibody-mediated rejection. Clin. Transpl. 2018, 32, e13194. [Google Scholar] [CrossRef]
- Chewcharat, A.; Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Thirunavukkarasu, S.; Kashani, K.B. Trajectories of Serum Sodium on In-Hospital and 1-Year Survival among Hospitalized Patients. Clin. J. Am. Soc. Nephrol. 2020. [Google Scholar] [CrossRef]
- Kaewput, W.; Thongprayoon, C.; Boonpheng, B.; Ungprasert, P.; Bathini, T.; Chewcharat, A.; Srivali, N.; Vallabhajosyula, S.; Cheungpasitporn, W. Inpatient Burden and Mortality of Goodpasture’s Syndrome in the United States: Nationwide Inpatient Sample 2003–2014. J. Clin. Med. 2020, 9, 455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Ungprasert, P.; Wijarnpreecha, K.; Kaewput, W.; Leeaphorn, N.; Bathini, T.; Chebib, F.T.; Kröner, P.T. Subarachnoid Hemorrhage in Hospitalized Renal Transplant Recipients with Autosomal Dominant Polycystic Kidney Disease: A Nationwide Analysis. J. Clin. Med. 2019, 8, 524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leeaphorn, N.; Thongprayoon, C.; Chon, W.J.; Cummings, L.S.; Mao, M.A.; Cheungpasitporn, W. Outcomes of kidney retransplantation after graft loss as a result of BK virus nephropathy in the era of newer immunosuppressant agents. Am. J. Transpl. 2019. [Google Scholar] [CrossRef] [PubMed]
- Lertjitbanjong, P.; Thongprayoon, C.; Cheungpasitporn, W.; O’Corragain, O.A.; Srivali, N.; Bathini, T.; Watthanasuntorn, K.; Aeddula, N.R.; Salim, S.A.; Ungprasert, P.; et al. Acute Kidney Injury after Lung Transplantation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Salim, S.A.; Ungprasert, P.; Wijarnpreecha, K.; et al. Incidence and Impact of Acute Kidney Injury after Liver Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongboonsin, J.; Thongprayoon, C.; Bathini, T.; Ungprasert, P.; Aeddula, N.R.; Mao, M.A.; Cheungpasitporn, W. Acetazolamide Therapy in Patients with Heart Failure: A Meta-Analysis. J. Clin. Med. 2019, 8, 349. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez Suarez, M.L.; Thongprayoon, C.; Mao, M.A.; Leeaphorn, N.; Bathini, T.; Cheungpasitporn, W. Outcomes of Kidney Transplant Patients with Atypical Hemolytic Uremic Syndrome Treated with Eculizumab: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 919. [Google Scholar] [CrossRef] [Green Version]
- Chewcharat, A.; Thongprayoon, C.; Bathini, T.; Aeddula, N.R.; Boonpheng, B.; Kaewput, W.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Torres-Ortiz, A.; et al. Incidence and Mortality of Renal Cell Carcinoma after Kidney Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 530. [Google Scholar] [CrossRef] [Green Version]
- Cheungpasitporn, W.; Thongprayoon, C.; Craici, I.M.; Sharma, K.; Chesdachai, S.; Khoury, N.J.; Ettore, A.S. Reactivation of BK polyomavirus during pregnancy, vertical transmission, and clinical significance: A meta-analysis. J. Clin. Virol. 2018, 102, 56–62. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Cheungpasitporn, W.; Lertjitbanjong, P.; Aeddula, N.R.; Bathini, T.; Watthanasuntorn, K.; Srivali, N.; Mao, M.A.; Kashani, K. Incidence and Impact of Acute Kidney Injury in Patients Receiving Extracorporeal Membrane Oxygenation: A Meta-Analysis. J. Clin. Med. 2019, 8, 981. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Kaewput, W.; Thamcharoen, N.; Bathini, T.; Watthanasuntorn, K.; Salim, S.A.; Ungprasert, P.; Lertjitbanjong, P.; Aeddula, N.R.; Torres-Ortiz, A.; et al. Acute Kidney Injury in Patients Undergoing Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Kanduri, S.R.; Cheungpasitporn, W.; Thongprayoon, C.; Bathini, T.; Kovvuru, K.; Garla, V.; Medaura, J.; Vaitla, P.; Kashani, K.B. Incidence and Mortality of Acute Kidney Injury in Patients Undergoing Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-analysis. QJM 2020. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Sakhuja, A.; Erickson, S.B. Admission calcium levels and risk of acute kidney injury in hospitalised patients. Int. J. Clin. Pr. 2018, 72, e13057. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Khoury, N.J.; Bathini, T.; Aeddula, N.R.; Boonpheng, B.; Leeaphorn, N.; Ungprasert, P.; Bruminhent, J.; Lertjitbanjong, P.; Watthanasuntorn, K.; et al. BK polyomavirus genotypes in renal transplant recipients in the United States: A meta-analysis. J. Evid. Based Med. 2019, 12, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.Y.; Hsieh, M.H.; Lin, C.L.; Hsieh, M.J.; Hsu, W.H.; Lin, C.C.; Hsu, C.Y.; Kao, C.H. Artificial Intelligence Prediction Model for the Cost and Mortality of Renal Replacement Therapy in Aged and Super-Aged Populations in Taiwan. J. Clin. Med. 2019, 8, 995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díez-Sanmartín, C.; Sarasa Cabezuelo, A. Application of Artificial Intelligence Techniques to Predict Survival in Kidney Transplantation: A Review. J. Clin. Med. 2020, 9, 572. [Google Scholar] [CrossRef] [Green Version]
- Azuaje, F.; Kim, S.Y.; Perez Hernandez, D.; Dittmar, G. Connecting Histopathology Imaging and Proteomics in Kidney Cancer through Machine Learning. J. Clin. Med. 2019, 8, 1535. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, C.C.; Tu, H.T.; Lin, C.H.; Chen, K.H.; Yeh, Y.H.; See, L.C. Temporal Trends of Severe Hypoglycemia and Subsequent Mortality in Patients with Advanced Diabetic Kidney Diseases Transitioning to Dialysis. J. Clin. Med. 2019, 8, 420. [Google Scholar] [CrossRef] [Green Version]
- Gout, A.M.; Martin, N.C.; Brown, A.F.; Ravine, D. PKDB: Polycystic Kidney Disease Mutation Database—A gene variant database for autosomal dominant polycystic kidney disease. Hum. Mutat. 2007, 28, 654–659. [Google Scholar] [CrossRef]
- Massie, A.B.; Kucirka, L.M.; Segev, D.L. Big data in organ transplantation: Registries and administrative claims. Am. J. Transpl. 2014, 14, 1723–1730. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulos, T.; Krochmal, M.; Cisek, K.; Fernandes, M.; Husi, H.; Stevens, R.; Bascands, J.L.; Schanstra, J.P.; Klein, J. Omics databases on kidney disease: Where they can be found and how to benefit from them. Clin. Kidney J. 2016, 9, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Port, F.K.; Held, P.J. The US Renal Data System at 30 Years: A Historical Perspective. Am. J. Kidney Dis. 2019, 73, 459–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stack, A.G.; Casserly, L.F.; Cronin, C.J.; Chernenko, T.; Cullen, W.; Hannigan, A.; Saran, R.; Johnson, H.; Browne, G.; Ferguson, J.P. Prevalence and variation of Chronic Kidney Disease in the Irish health system: Initial findings from the National Kidney Disease Surveillance Programme. Bmc Nephrol. 2014, 15, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bello, A.K.; Ronksley, P.E.; Tangri, N.; Singer, A.; Grill, A.; Nitsch, D.; Queenan, J.A.; Lindeman, C.; Soos, B.; Freiheit, E.; et al. A national surveillance project on chronic kidney disease management in Canadian primary care: A study protocol. BMJ Open 2017, 7, e016267. [Google Scholar] [CrossRef] [PubMed]
- Saran, R.; Steffick, D.; Bragg-Gresham, J. The China Kidney Disease Network (CK-NET): “Big Data-Big Dreams”. Am. J. Kidney Dis. 2017, 69, 713–716. [Google Scholar] [CrossRef] [Green Version]
- Dienemann, T.; Fujii, N.; Orlandi, P.; Nessel, L.; Furth, S.L.; Hoy, W.E.; Matsuo, S.; Mayer, G.; Methven, S.; Schaefer, F.; et al. International Network of Chronic Kidney Disease cohort studies (iNET-CKD): A global network of chronic kidney disease cohorts. BMC Nephrol. 2016, 17, 121. [Google Scholar] [CrossRef]
- Lv, J.; Zhang, H.; Wong, M.G.; Jardine, M.J.; Hladunewich, M.; Jha, V.; Monaghan, H.; Zhao, M.; Barbour, S.; Reich, H.; et al. Effect of Oral Methylprednisolone on Clinical Outcomes in Patients With IgA Nephropathy: The TESTING Randomized Clinical Trial. JAMA 2017, 318, 432–442. [Google Scholar] [CrossRef]
- Matsushita, K.; Ballew, S.H.; Astor, B.C.; Jong, P.E.d.; Gansevoort, R.T.; Hemmelgarn, B.R.; Levey, A.S.; Levin, A.; Wen, C.-P.; Woodward, M.; et al. Cohort profile: The chronic kidney disease prognosis consortium. Int. J. Epidemiol. 2013, 42, 1660–1668. [Google Scholar] [CrossRef] [Green Version]
- Levin, A.; Tonelli, M.; Bonventre, J.; Coresh, J.; Donner, J.-A.; Fogo, A.B.; Fox, C.S.; Gansevoort, R.T.; Heerspink, H.J.L.; Jardine, M.; et al. Global kidney health 2017 and beyond: A roadmap for closing gaps in care, research, and policy. Lancet 2017, 390, 1888–1917. [Google Scholar] [CrossRef]
- O’Seaghdha, C.M.; Fox, C.S. Genome-wide association studies of chronic kidney disease: What have we learned? Nat. Rev. Nephrol. 2011, 8, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Wuttke, M.; Köttgen, A. Insights into kidney diseases from genome-wide association studies. Nat. Rev. Nephrol. 2016, 12, 549–562. [Google Scholar] [CrossRef]
- Ahlqvist, E.; van Zuydam, N.R.; Groop, L.C.; McCarthy, M.I. The genetics of diabetic complications. Nat. Rev. Nephrol. 2015, 11, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Mohan, C.; Putterman, C. Genetics and pathogenesis of systemic lupus erythematosus and lupus nephritis. Nat. Rev. Nephrol. 2015, 11, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Lindenmeyer, M.T.; Kretzler, M. Renal biopsy-driven molecular target identification in glomerular disease. Pflug. Arch. 2017, 469, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Rumsfeld, J.S.; Joynt, K.E.; Maddox, T.M. Big data analytics to improve cardiovascular care: Promise and challenges. Nat. Rev. Cardiol. 2016, 13, 350–359. [Google Scholar] [CrossRef]
- Cheungpasitporn, W.; Thongprayoon, C.; Ungprasert, P.; Wijarnpreecha, K.; Raimondo, M.; Kroner, P.T. Acute pancreatitis in end-stage renal disease patients in the USA: A nationwide, propensity score-matched analysis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 968–972. [Google Scholar] [CrossRef]
- Thongprayoon, C.; Kaewput, W.; Boonpheng, B.; Ungprasert, P.; Bathini, T.; Srivali, N.; Vallabhajosyula, S.; Castaneda, J.L.; Monga, D.; Kanduri, S.R.; et al. Impact of ANCA-Associated Vasculitis on Outcomes of Hospitalizations for Goodpasture’s Syndrome in the United States: Nationwide Inpatient Sample 2003-2014. Medicina 2020, 56, 103. [Google Scholar] [CrossRef] [Green Version]
- Ungprasert, P.; Koster, M.J.; Cheungpasitporn, W.; Wijarnpreecha, K.; Thongprayoon, C.; Kroner, P.T. Inpatient epidemiology and economic burden of granulomatosis with polyangiitis: A 10-year study of the national inpatient sample. Rheumatology 2020. [Google Scholar] [CrossRef]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb. Med. Inform. 2016, 25 (Suppl. 1), S48–S61. [Google Scholar] [CrossRef]
- Sutherland, S.M.; Goldstein, S.L.; Bagshaw, S.M. Acute Kidney Injury and Big Data. Contrib. Nephrol. 2018, 193, 55–67. [Google Scholar]
- Sutherland, S.M. Electronic Health Record-Enabled Big-Data Approaches to Nephrotoxin-Associated Acute Kidney Injury Risk Prediction. Pharmacotherapy 2018, 38, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, S.M. Big Data and Pediatric Acute Kidney Injury: The Promise of Electronic Health Record Systems. Front. Pediatr. 2019, 7, 536. [Google Scholar] [CrossRef] [PubMed]
- Shipp, M.A.; Ross, K.N.; Tamayo, P.; Weng, A.P.; Kutok, J.L.; Aguiar, R.C.; Gaasenbeek, M.; Angelo, M.; Reich, M.; Pinkus, G.S.; et al. Diffuse large B-cell lymphoma outcome prediction by gene-expression profiling and supervised machine learning. Nat. Med. 2002, 8, 68–74. [Google Scholar] [CrossRef]
- Saez-Rodriguez, J.; Rinschen, M.M.; Floege, J.; Kramann, R. Big science and big data in nephrology. Kidney Int. 2019, 95, 1326–1337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angermueller, C.; Pärnamaa, T.; Parts, L.; Stegle, O. Deep learning for computational biology. Mol. Syst Biol. 2016, 12, 878. [Google Scholar] [CrossRef] [PubMed]
- SGarcelon, N.; Burgun, A.; Salomon, R.; Neuraz, A. Electronic health records for the diagnosis of rare diseases. Kidney Int. 2020, 97, 676–686. [Google Scholar] [CrossRef] [Green Version]
- Stead, W.W. Clinical Implications and Challenges of Artificial Intelligence and Deep Learning. JAMA 2018, 320, 1107–1108. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Emanuel, E.J. Predicting the Future—Big Data, Machine Learning, and Clinical Medicine. N. Engl. J. Med. 2016, 375, 1216–1219. [Google Scholar] [CrossRef] [Green Version]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Pennington, J.; Socher, R.; Manning, C.D. (Eds.) Glove: Global vectors for word representation. In Proceedings of the 2014 Conference on Empirical Methods in Natural Language Processing (EMNLP), Doha, Qatar, 25–29 October 2014. [Google Scholar]
- Hermsen, M.; de Bel, T.; den Boer, M.; Steenbergen, E.J.; Kers, J.; Florquin, S.; Roelofs, J.; Stegall, M.D.; Alexander, M.P.; Smith, B.H.; et al. Deep Learning-Based Histopathologic Assessment of Kidney Tissue. J. Am. Soc. Nephrol. 2019, 30, 1968–1979. [Google Scholar] [CrossRef]
- Ginley, B.; Lutnick, B.; Jen, K.Y.; Fogo, A.B.; Jain, S.; Rosenberg, A.; Walavalkar, V.; Wilding, G.; Tomaszewski, J.E.; Yacoub, R.; et al. Computational Segmentation and Classification of Diabetic Glomerulosclerosis. J. Am. Soc. Nephrol. 2019, 30, 1953–1967. [Google Scholar] [CrossRef] [PubMed]
- Tomašev, N.; Glorot, X.; Rae, J.W.; Zielinski, M.; Askham, H.; Saraiva, A.; et al. A clinically applicable approach to continuous prediction of future acute kidney injury. Nature 2019, 572, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Escandell-Montero, P.; Chermisi, M.; Martínez-Martínez, J.M.; Gómez-Sanchis, J.; Barbieri, C.; Soria-Olivas, E.; Mari, F.; Vila-Francés, J.; Stopper, A.; Gatti, E.; et al. Optimization of anemia treatment in hemodialysis patients via reinforcement learning. Artif. Intell. Med. 2014, 62, 47–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbieri, C.; Molina, M.; Ponce, P.; Tothova, M.; Cattinelli, I.; Ion Titapiccolo, J.; Mari, F.; Amato, C.; Leipold, F.; Wehmeyer, W.; et al. An international observational study suggests that artificial intelligence for clinical decision support optimizes anemia management in hemodialysis patients. Kidney Int. 2016, 90, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Li, X.; Li, Y.; Xia, E.; Qin, Y.; Liang, S.; Xu, F.; Liang, D.; Zeng, C.; Liu, Z. Prediction and Risk Stratification of Kidney Outcomes in IgA Nephropathy. Am. J. Kidney Dis. 2019, 74, 300–309. [Google Scholar] [CrossRef]
- Samal, L.; D’Amore, J.D.; Bates, D.W.; Wright, A. Implementation of a scalable, web-based, automated clinical decision support risk-prediction tool for chronic kidney disease using C-CDA and application programming interfaces. J. Am. Med. Inf. Assoc. 2017, 24, 1111–1115. [Google Scholar] [CrossRef] [Green Version]
- Tangri, N.; Stevens, L.A.; Griffith, J.; Tighiouart, H.; Djurdjev, O.; Naimark, D.; Levin, A.; Levey, A.S. A predictive model for progression of chronic kidney disease to kidney failure. JAMA 2011, 305, 1553–1559. [Google Scholar] [CrossRef] [Green Version]
- Ravizza, S.; Huschto, T.; Adamov, A.; Böhm, L.; Büsser, A.; Flöther, F.F.; Hinzmann, R.; König, H.; McAhren, S.M.; Robertson, D.H.; et al. Predicting the early risk of chronic kidney disease in patients with diabetes using real-world data. Nat. Med. 2019, 25, 57–59. [Google Scholar] [CrossRef]
- Zhou, C.; Wang, R.; Jiang, W.; Zhu, J.; Liu, Y.; Zheng, J.; et al. Machine learning for the prediction of acute kidney injury and paraplegia after thoracoabdominal aortic aneurysm repair. J. Card. Surg. 2020, 35, 89–99. [Google Scholar] [CrossRef]
- Xu, Z.; Chou, J.; Zhang, X.S.; Luo, Y.; Isakova, T.; Adekkanattu, P.; Ancker, J.S.; Jiang, G.; Kiefer, R.C.; Pacheco, J.A.; et al. Identifying sub-phenotypes of acute kidney injury using structured and unstructured electronic health record data with memory networks. J. Biomed. Inform. 2020, 102, 103361. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Waitman, L.R.; Yu, A.S.; Robbins, D.C.; Hu, Y.; Liu, M. Longitudinal Risk Prediction of Chronic Kidney Disease in Diabetic Patients Using a Temporal-Enhanced Gradient Boosting Machine: Retrospective Cohort Study. JMIR Med. Inform. 2020, 8, e15510. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, H.H.; Sen, S.; Palmieri, T.L.; Blackmon, T.; Wajda, J.; Tran, N.K. Early Recognition of Burn- and Trauma-Related Acute Kidney Injury: A Pilot Comparison of Machine Learning Techniques. Sci. Rep. 2020, 10, 205. [Google Scholar] [CrossRef] [PubMed]
- Morid, M.A.; Sheng, O.R.L.; Del Fiol, G.; Facelli, J.C.; Bray, B.E.; Abdelrahman, S. Temporal Pattern Detection to Predict Adverse Events in Critical Care: Case Study With Acute Kidney Injury. JMIR Med. Inform. 2020, 8, e14272. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Tang, Z.; Hu, X.; Lu, S.; Miao, B.; Hong, S.; Bai, H.; Sun, C.; Qiu, J.; Liang, H.; et al. Machine learning for the prediction of severe pneumonia during posttransplant hospitalization in recipients of a deceased-donor kidney transplant. Ann. Transl. Med. 2020, 8, 82. [Google Scholar] [CrossRef]
- Li, N.; Huang, H.; Qian, H.-Z.; Liu, P.; Lu, H.; Liu, X. Improving accuracy of estimating glomerular filtration rate using artificial neural network: Model development and validation. J. Transl. Med. 2020, 18, 120. [Google Scholar] [CrossRef]
- Lei, L.; Wang, Y.; Xue, Q.; Tong, J.; Zhou, C.-M.; Yang, J.-J. A comparative study of machine learning algorithms for predicting acute kidney injury after liver cancer resection. PeerJ 2020, 8, e8583. [Google Scholar] [CrossRef]
- Kate, R.J.; Pearce, N.; Mazumdar, D.; Nilakantan, V. A continual prediction model for inpatient acute kidney injury. Comput. Biol. Med. 2020, 116, 103580. [Google Scholar] [CrossRef]
- Kang, M.W.; Kim, J.; Kim, D.K.; Oh, K.-H.; Joo, K.W.; Kim, Y.S.; Han, S.S. Machine learning algorithm to predict mortality in patients undergoing continuous renal replacement therapy. Crit. Care 2020, 24, 42. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, L.P.; Reyfman, P.A.; Smith, A.D.R.; Zeng, Z.; Kho, A.; Sanchez-Pinto, L.N.; Luo, Y. Early prediction of acute kidney injury following ICU admission using a multivariate panel of physiological measurements. Bmc Med. Inform. Decis. Mak. 2019, 19 (Suppl. 1), 16. [Google Scholar] [CrossRef]
- Zhang, Z.; Ho, K.M.; Hong, Y. Machine learning for the prediction of volume responsiveness in patients with oliguric acute kidney injury in critical care. Crit. Care 2019, 23, 112. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Luo, Y.; Adekkanattu, P.; Ancker, J.S.; Jiang, G.; Kiefer, R.C.; Pacheco, J.A.; Rasmussen, L.V.; Pathak, J.; Wang, F. Stratified Mortality Prediction of Patients with Acute Kidney Injury in Critical Care. Stud. Health Technol. Inform. 2019, 264, 462–466. [Google Scholar] [PubMed]
- Xiao, J.; Ding, R.; Xu, X.; Guan, H.; Feng, X.; Sun, T.; Zhu, S.; Ye, Z. Comparison and development of machine learning tools in the prediction of chronic kidney disease progression. J. Transl. Med. 2019, 17, 119. [Google Scholar] [CrossRef] [Green Version]
- Mark, E.; Goldsman, D.; Gurbaxani, B.; Keskinocak, P.; Sokol, J. Using machine learning and an ensemble of methods to predict kidney transplant survival. PLoS ONE 2019, 14, e0209068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, S.; Massie, A.B.; Thomas, A.G.; Bahn, G.; Luo, X.; Jackson, K.R.; Ottmann, S.E.; Brennan, D.C.; Desai, N.M.; Coresh, J.; et al. Who can tolerate a marginal kidney? Predicting survival after deceased donor kidney transplant by donor-recipient combination. Am. J. Transpl. 2019, 19, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.D.; Noh, J.; Lee, H.; Kim, D.K.; Lim, C.S.; Kim, Y.H.; Lee, J.P.; Kim, G.; Kim, Y.S. A Machine Learning Approach Using Survival Statistics to Predict Graft Survival in Kidney Transplant Recipients: A Multicenter Cohort Study. Sci. Rep. 2017, 7, 8904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niel, O.; Bastard, P. Artificial Intelligence in Nephrology: Core Concepts, Clinical Applications, and Perspectives. Am. J. Kidney Dis. 2019, 74, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Improta, G.; Mazzella, V.; Vecchione, D.; Santini, S.; Triassi, M. Fuzzy logic-based clinical decision support system for the evaluation of renal function in post-Transplant Patients [published online ahead of print, 2019 Nov 12]. J. Eval. Clin. Pract. 2019. [Google Scholar] [CrossRef] [Green Version]
- Atallah, D.M.; Badawy, M.; El-Sayed, A.; Ghoneim, M.A. Predicting kidney transplantation outcome based on hybrid feature selection and KNN classifier. Multimed. Tools Appl. 2019, 78, 20383–20407. [Google Scholar] [CrossRef]
- Nematollahi, M.; Akbari, R.; Nikeghbalian, S.; Salehnasab, C. Classification Models to Predict Survival of Kidney Transplant Recipients Using Two Intelligent Techniques of Data Mining and Logistic Regression. Int. J. Organ. Transpl. Med. 2017, 8, 119–122. [Google Scholar]
- Tapak, L.; Hamidi, O.; Amini, P.; Poorolajal, J. Prediction of Kidney Graft Rejection Using Artificial Neural Network. Healthc Inf. Res. 2017, 23, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Shahmoradi, L.; Langarizadeh, M.; Pourmand, G.; Fard, Z.A.; Borhani, A. Comparing Three Data Mining Methods to Predict Kidney Transplant Survival. Acta Inf. Med. 2016, 24, 322–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luck, M.; Sylvain, T.; Cardinal, H.; Lodi, A.; Bengio, Y. Deep learning for patient-specific kidney graft survival analysis. arXiv 2017, arXiv:170510245. [Google Scholar]
- Topuz, K.; Zengul, F.D.; Dag, A.; Almehmi, A.; Yildirim, M.B. Predicting graft survival among kidney transplant recipients: A Bayesian decision support model. Decis. Support. Syst. 2018, 106, 97–109. [Google Scholar] [CrossRef]
- Lyell, D.; Coiera, E. Automation bias and verification complexity: A systematic review. J. Am. Med. Inf. Assoc. 2017, 24, 423–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Sinha, A.D. Big data in nephrology-a time to rethink. Nephrol. Dial. Transpl. 2018, 33, 1–3. [Google Scholar] [CrossRef]
- Lee, C.H.; Yoon, H.-J. Medical big data: Promise and challenges. Kidney Res. Clin. Pr. 2017, 36, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Calvert, J.; Saber, N.; Hoffman, J.; Das, R. Machine-Learning-Based Laboratory Developed Test for the Diagnosis of Sepsis in High-Risk Patients. Diagnostics 2019, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Lim, E.-C.; Park, J.H.; Jeon, H.J.; Kim, H.-J.; Lee, H.-J.; Song, C.-G.; Hong, S.K. Developing a Diagnostic Decision Support System for Benign Paroxysmal Positional Vertigo Using a Deep-Learning Model. J. Clin. Med. 2019, 8, 633. [Google Scholar] [CrossRef] [Green Version]
- Heo, S.-J.; Kim, Y.; Yun, S.; Lim, S.-S.; Kim, J.; Nam, C.-M.; Park, E.-C.; Jung, I.; Yoon, J.-H. Deep Learning Algorithms with Demographic Information Help to Detect Tuberculosis in Chest Radiographs in Annual Workers’ Health Examination Data. Int. J. Env. Res. Public Health 2019, 16, 250. [Google Scholar] [CrossRef] [Green Version]
- Kooman, J.P.; Wieringa, F.P.; Han, M.; Chaudhuri, S.; van der Sande, F.M.; Usvyat, L.A.; Kotanko, P. Wearable health devices and personal area networks: can they improve outcomes in haemodialysis patients? Nephrol. Dial. Transplant. 2020, 35 (Suppl. 2), ii43–ii50. [Google Scholar] [CrossRef]
- Shortliffe, E.H.; Sepúlveda, M.J. Clinical Decision Support in the Era of Artificial Intelligence. JAMA 2018, 320, 2199–2200. [Google Scholar] [CrossRef] [PubMed]
- Santo, B.A.; Rosenberg, A.Z.; Sarder, P. Artificial intelligence driven next-generation renal histomorphometry. Curr. Opin. Nephrol. Hypertens. 2020, 29, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Na, L.; Yang, C.; Lo, C.C.; Zhao, F.; Fukuoka, Y.; Aswani, A. Feasibility of Reidentifying Individuals in Large National Physical Activity Data Sets From Which Protected Health Information Has Been Removed With Use of Machine Learning. JAMA Netw. Open 2018, 1, e186040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermeyer, Z.; Lee, T.H. Lost in Thought—The Limits of the Human Mind and the Future of Medicine. N. Engl. J. Med. 2017, 377, 1209–1211. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Renal and Transplant Databases | Organizations |
|---|---|
|
|
| Study | Country | Study Type | N | Subjects | Intervention |
|---|---|---|---|---|---|
| Zhou, 2020 [90] | China | R | 212 | Prediction of ARF and paraplegia after TAAAR | Machine learning classification models |
| Xu, 2020 [91] | USA | R | 37,486 | Identification the sub-phenotypes of AKI | Memory network-based deep learning approach |
| Song, 2020 [92] | USA | R | 14,039 | Longitudinal Risk Prediction of CKD in Diabetic Patients | Temporal-enhanced gradient boosting machine |
| Rashidi, 2020 [93] | USA | P, R | 101 | Early recognition of burn- and trauma-related AKI | Artificial intelligence /machine learning algorithms |
| Morid, 2020 [94] | USA | R | 22,542 | Prediction of adverse events in critical patients with AKI | Temporal pattern detection |
| Luo, 2020 [95] | China | R | 519 | Prediction of severe pneumonia during post-transplant hospitalization in recipients of a deceased-donor kidney transplant | Machine learning |
| Li, 2020 [96] | China | P | 1952 | Accuracy improvement of GFR estimation | Artificial neural network |
| Lei, 2020 [97] | China | R | 1173 | Prediction of AKI after liver cancer resection | Machine learning algorithms |
| Kate, 2020 [98] | USA | R | 44,691 | Prediction of AKI in hospitalized patients | Machine learning predictive models |
| Kang, 2020 [99] | South Korea | R | 1571 | Prediction of mortality in CRRT patients | Machine learning algorithms |
| Zimmerman, 2019 [100] | USA | R | 23,950 | Prediction of AKI following ICU admission | Machine learning models |
| Zhang, 2019 [101] | China | R | 2456 | Prediction of volume responsiveness in oliguric AKI | Machine learning models |
| Xu, 2019 [102] | USA | R | 58,976 | Prediction of mortality in patients with AKI in the ICU | Machine learning models |
| Xiao, 2019 [103] | China | R | 551 | Prediction of CKD progression | Machine learning tools |
| Mark, 2019 [104] | USA | R | 100,000 | Prediction of survival of kidney transplant recipients from UNOS | Machine learning models |
| Bae, 2019 [105] | USA | R | 120,818 | Prediction of survival after deceased donor kidney transplant from OPTN database | Machine learning methods |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Kaewput, W.; Kovvuru, K.; Hansrivijit, P.; Kanduri, S.R.; Bathini, T.; Chewcharat, A.; Leeaphorn, N.; Gonzalez-Suarez, M.L.; Cheungpasitporn, W. Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation. J. Clin. Med. 2020, 9, 1107. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041107
Thongprayoon C, Kaewput W, Kovvuru K, Hansrivijit P, Kanduri SR, Bathini T, Chewcharat A, Leeaphorn N, Gonzalez-Suarez ML, Cheungpasitporn W. Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation. Journal of Clinical Medicine. 2020; 9(4):1107. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041107
Chicago/Turabian StyleThongprayoon, Charat, Wisit Kaewput, Karthik Kovvuru, Panupong Hansrivijit, Swetha R. Kanduri, Tarun Bathini, Api Chewcharat, Napat Leeaphorn, Maria L. Gonzalez-Suarez, and Wisit Cheungpasitporn. 2020. "Promises of Big Data and Artificial Intelligence in Nephrology and Transplantation" Journal of Clinical Medicine 9, no. 4: 1107. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041107